






Evaluating APMs for Oncology Care Access in the U.S.
From Fee-for-Service to Value: Evaluating Alternative Payment Models for Novel Oncology Care Access
Rayan K. Salih, PharmD¹˒³; Reyna Jash, PharmD, MBA¹˒³; Dhaval Patel, PharmD¹˒³; Emily Wong, PharmD, MBA¹˒³; Vanessa Quintero, PharmD¹˒³; Tim Jurasik, PharmD¹˒³; John M. York, PharmD, MBA, PhD¹˒²˒³
- Rutgers University, Ernest Mario School of Pharmacy (New Brunswick, NJ)
- Institute of Global Entrepreneur and Rady School of Management, University of California, San Diego (San Diego, CA)
- Rutgers Institute for Pharmaceutical Industry Fellowships, Rutgers, the State University of New Jersey (Piscataway, NJ)
OPEN ACCESS
PUBLISHED:31 October 2025
CITATION: SALIH, Rayan K. et al. From Fee-for-Service to Value: Evaluating Alternative Payment Models for Novel Oncology Care Access. Medical Research Archives, [S.l.], v. 13, n. 10, oct. 2025. Available at: <https://esmed.org/MRA/mra/article/view/7000>. Date accessed: 07 nov. 2025. doi: https://doi.org/10.18103/mra.v13i10.7000.
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i10.7000
ISSN 2375-1924
Abstract
As cancer treatments become more complex and costly, traditional reimbursement models that reward volume rather than value create significant challenges for patients, providers, and health systems. In response, alternative payment models have emerged to better align financial incentives with quality care, affordability, and outcomes. However, their adoption in oncology remains uneven, especially for innovative therapies such as gene-based treatments and immunotherapies. This systematic review examines two questions: (1) What is the current status of oncology-focused alternative payment models in the United States? and (2) How do these models influence patient access to novel treatments? A structured literature review was conducted using three major databases and guided by a five-dimensional access framework that includes availability, accessibility, accommodation, affordability, and acceptability. Forty eligible studies were thematically analyzed. The results identified four dominant themes: clinical pathways, value-based care, quality measurement, and barriers to implementation. While models such as the Oncology Care Model and the Enhancing Oncology Model show promise in improving coordination and lowering costs, they often fall short in addressing access gaps, particularly in underserved communities. This review offers a new stakeholder-informed process model and highlights the need for proactive planning, standardized metrics, and cross-sector collaboration to ensure that future models are equitable, scalable, and capable of supporting continued innovation in oncology care.
Keywords
- Oncology
- Alternative Payment Models
- Value-Based Care
- Patient Access
- Healthcare Systems
Introduction
The fee-for-service (FFS) payment model has long dominated the United States (U.S.) healthcare system, incentivizing volume over value and increasing healthcare costs. In the FFS model, providers are reimbursed for each service or procedure performed, regardless of the quality or outcome of care. While this approach ensures payment for rendered services, it often leads to fragmented care delivery and provides little emphasis on patient outcomes. This misalignment becomes particularly pronounced in oncology, where treatment regimens often involve innovative and expensive therapies. Traditional payment structures fail to address the complexity of managing cancer patients, leading to significant financial strain on healthcare systems and patients. The growth of innovative oncology treatments (e.g., immune, gene, and CAR-T therapies) represents a significant advancement in cancer care. However, high cost poses a challenge, with price tags often exceeding hundreds of thousands per patient. For novel oncology therapies, the challenges posed by FFS may be exacerbated by higher price tags, leaving patients to navigate significant financial burdens and access barriers.
Alternative payment models (APMs) are emerging as a potential solution. Alternative payment models aim to align financial incentives with delivering high-quality, cost-effective care by linking reimbursement to quality and outcomes rather than service volume. Specific models, such as the Oncology Care Model (OCM) and its successor, the Enhancing Oncology Model (EOM), as well as Bundled Payments for Care Improvement (BPCI), represent tailored efforts to improve the value of oncology care. While APMs have grown in oncology since the passage of the Affordable Care Act (ACA), there is limited research and evidence to evaluate their efficacy once implemented. These gaps raise critical questions about the adaptability of APMs to novel oncology innovations and their ability to address key barriers to patient access, including affordability, insurance coverage, and continuity of care. Current literature on APMs primarily focuses on their general implementation in healthcare. However, there is a lack of comprehensive analysis of their impact on oncology, particularly concerning novel therapies.
This paper addresses the following research questions: 1) What is the current status of APMs in the U.S. healthcare system? and 2) How do these models improve patient access? Through a comprehensive, systematic literature review and thematic analysis, this work provides insights into the administrative, clinical, and economic impacts of APMs, focusing on their potential to support equitable access to novel oncology therapies. This paper begins with a literature review to contextualize the gap and questions. It segues to relevant methodology. Next, the results provide both descriptive and thematic analyses. The paper concludes with a comprehensive discussion, highlighting contributions, their alignment with existing literature, study limitations, and a proposed agenda for future research.
Literature Review
Implementation of APMs
The literature widely discusses implementation of APMs, with most studies focusing on the potential to reduce costs while improving patient care. Many healthcare settings are implementing models like the BPCI, showing promising results in improving efficiency and patient satisfaction. While the evidence for the broader effectiveness of APMs is strong, limited literature focuses specifically on novel therapies within oncology.
The application of APMs in oncology treatment is a subject of growing interest, with the OCM and EOM identified as the most prominent in oncology care. These models aim to enhance quality of care by reimbursing providers based on patient outcomes rather than the volume of services delivered. The Enhancing Oncology Model (EOM) builds on the foundation of the OCM by offering enhanced financial incentives, targeted support for underserved populations, and additional resources for oncology practices. The goal is to improve patient outcomes, enhance patient experience, and reduce costs for Medicare beneficiaries receiving chemotherapy. Studies have demonstrated that OCM participants have improved care coordination and better-quality outcomes compared to FFS models. However, integrating APMs in novel oncology care is slow despite these improvements.
Patient Access
The central focus of APMs is to enhance patient access to care. Implementing APMs has shown promise in improving financial accessibility for patients, reducing out-of-pocket costs, and ensuring more equitable care distribution. However, many studies have pointed out significant barriers, particularly for newer, high-cost treatments such as immunotherapies and gene therapies, which remain underrepresented in APM discussions. Additionally, contributions have not fully explored the impact of APMs on those with limited access to specialized cancer care. This observation may suggest a gap in the literature regarding APMs’ ability to address the needs of these underserved populations.
Maximize Outcomes, Minimize Costs
New, innovative therapies allow patients and healthcare providers to choose treatment options, but they also carry uncertainty that complicates the reimbursement process. Before health plans decide on reimbursement, providers must provide data to address essential complexities and nuances of the new, novel therapy. Alternative payment models aim to maximize outcomes and minimize costs in response to rising healthcare costs. In a disease state like oncology with high-cost treatments, APMs are appropriately suited to make substantial differences in patient care. However, application of APMs and the goals of incentivizing improved clinical outcomes are not always delivered appropriately. The healthcare system’s stakeholders have conflicting goals, including access, cost containment, and high-quality care. These differences can lead to challenges in achieving high-value care, as the focus may result in suboptimal care and lower long-term value for patients.
Paucity of Literature
There is a limited amount of published literature regarding the efficacy of APMs, which slows the uptake of these innovative models. There continues to be a need for both payers and providers to participate in APMs and voice the components that matter most in patient care. Incorporating value-based payment models requires incentives for the plan sponsors and providers to participate, in addition to data availability and performance metrics. Much of the evidence from APM implementation has not convinced stakeholders. However, Navathe and colleagues argue that it is not the model that has failed; it is the misalignment of expectations, evaluation standards, and outcomes.
A significant gap exists in understanding how healthcare stakeholders can optimize APMs for the unique challenges of oncology treatments. There is a notable lack of studies exploring these models’ specific administrative, economic, and clinical impacts in oncology. This study aims to fill these gaps by analyzing the current status of APMs in oncology, assessing their effectiveness in improving patient access and exploring the barriers to the adoption of novel cancer therapies. This study will provide insights to inform policy and healthcare practice by identifying key barriers to adopting APMs in novel oncology therapies. Furthermore, it will contribute to the growing knowledge of value-based care, particularly in oncology.
Materials and Methods
This review utilized systematic and snowball approaches to investigate the status of APMs on access to novel oncology therapeutics. The systematic approach drew upon Tranfield, colleagues, and Moher and collaborators’ methods. The analysis involved content assessment of the pulled studies to code key themes and identify APMs’ impact on treatment access.
This systematic review engaged three research databases (PubMed, Embase, and Scopus) to capture relevant citations. Search strings (Table 1) captured two research questions: 1) What is the current status of alternative payment models in the U.S. healthcare system? and 2) How do these models improve patient access? It also considered the inclusion and exclusion criteria (Table 1). Each search string utilized “OR” and “AND” operators for a broad capture of citations. The systematic search protocol ran each string set ((“alternative payment model*” OR “alternative payment system*”) individually and together using the “AND” operator for additional parameters (“oncology*” OR “cancer*”)).
| Area (Abbreviation) | Use String |
|---|---|
| Oncology | (oncolog* OR cancer* OR tumor) |
| Alternative Payment Models (APM) | ((“alternative payment system*” OR APS OR “alternative payment model* OR AMP)) |
| Inclusion | Exclusion |
|---|---|
| 1. Language: English | 1. Document Types: Non-peer review materials, including non-academic books, newspapers, letters, editorial materials, commentaries, magazines, book reviews, editorials, letters to the editor, proceedings, health service research |
| 2. Period: 2017-2024 | 2. Setting: Outside the U.S. |
| 3. Document Types: Peer-reviewed articles, systematic reviews, reviews, conference papers, studies, white papers | |
| 4. Research Focus: Oncology, alternative payment models, inpatient and outpatient, and patient access to covered medication(s) within the U.S. payer system. |
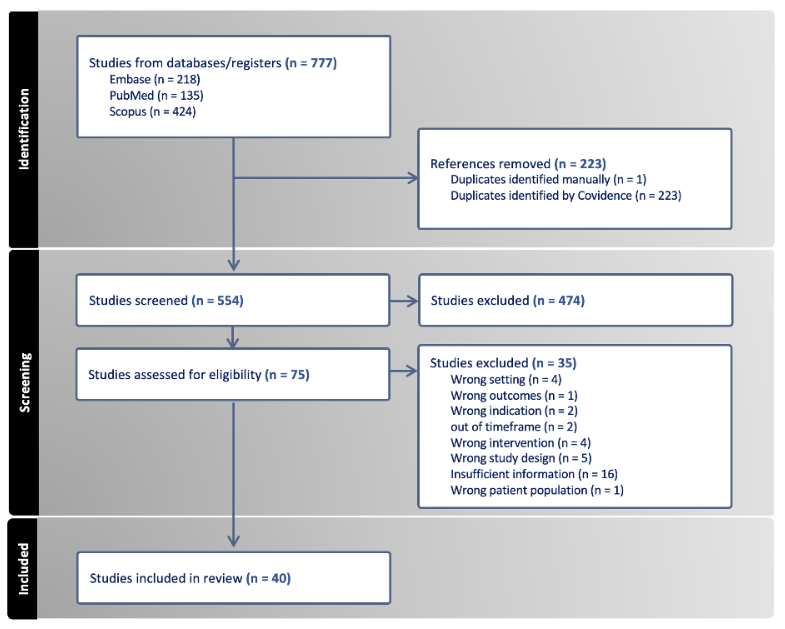
This effort utilized predefined screening criteria for reviewing titles, abstracts, and research articles using the Preferred Reporting Items for Systematic and Meta-Analyses (PRISMA) guidelines. The snowball search followed the guidance of Wohlin, which identified relevant publications from the systematic review. This initial screen led to 776 citations. Deduplication reduced this list to 554 citations. Study eligibility further narrowed this list to 80 sources, and screening each title and abstract resulted in a final analysis of 40 publications.
The literature review utilized the conceptual framework of access to care defined by Penchansky and Thomas, which captures access as a multidimensional framework composed of five key dimensions: Availability, Accessibility, Accommodation, Affordability, and Acceptability (Table 2). The review aimed to identify and synthesize relevant literature about these dimensions across various healthcare settings. Each dimension captures different aspects of access, including provider-to-population ratios, travel time to healthcare facilities, appointment flexibility, patient-reported out-of-pocket costs, and patient satisfaction surveys.
| Dimension | Definition |
|---|---|
| Availability | Physical presence of services or resources |
| Accessibility | Geographic and logistical ease of obtaining services |
| Affordability | Financial capability to use healthcare services |
| Acceptability | Cultural and social acceptance of the services |
| Accommodation | The fit between services and patients’ needs |
Quality assessment of the final analysis articles drew upon PRISMA. Such considerations included 1) the relevance of study abstracts towards providing key findings effectively, 2) the robustness of the study methods, 3) the reliability of the references, 4) the structure of results presented, and 5) the validity of the study conclusions about the research questions in focus.
Final analysis used descriptive and thematic analysis techniques. Descriptive analysis systematically encompassed key study characteristics, such as study type, design, geographic distribution, and publication year. This process also examined methodological aspects, including research design, data collection, and analysis techniques. Meanwhile, the thematic analysis identified and categorized recurring patterns and themes associated with broader themes about the research questions.
The review addressed the first research question and identified four themes derived from the literature: 1) Clinical Pathways, 2) Value-Based Care, 3) Quality Measurement and Improvement, and 4) Barriers to Implementation. This process began by identifying and extracting access-related information from each article and summarizing key points relevant to the thematic domains. The next effort focused on the second research question. It aligned each summary with one or more of the five access dimensions defined by Penchansky and Thomas: A1) Availability, A2) Accessibility, A3) Accommodation, A4) Affordability, and A5) Acceptability. The basis for choosing this framework involved the ability to capture patient access through multiple factors and not a rigid definition. The review used consistent criteria to guide alignment and held regular discussions to address interpretive differences and refine definitions. The review tracked recurring themes and marked the point when additional studies no longer introduced new concepts. Each summary described how the APM addressed specific access dimensions and provided contextual insights relevant to implementation. These findings informed the final analysis of access-related patterns across the literature.
Results
Descriptive Summary
The 40 studies in this systematic literature review offer fresh perspectives on the evolving landscape of APMs in the U.S. healthcare system, particularly for novel oncology therapies. Between 2017-2024, most of these studies appear in 2018 and 2021 (n = 8 each), highlighting a noticeable surge in scholarly interest. Regarding methodology, cohort studies (n = 8) and claims-based analyses (n = 8) emerge as the most common approaches, while systematic reviews (n = 5) provide comprehensive syntheses that further enrich the discussion.
These studies span a range of practice settings. Most focus on a mixed oncology setting (n = 29), while nine concentrate on outpatient settings, and only two focus on inpatient care. Although many cite a mixed oncology approach, they often lack clarity regarding what this “mixed” context entails, underscoring a persistent gap in the level of detail provided. The researchers identify “mixed” oncology settings as those incorporating inpatient and outpatient settings.
The literature also identifies four primary areas of oncology treatments. When analyzing treatment types, most fall under Cancer Treatment Modalities (n = 15), followed by Specialized Cancer Types and Treatments (n = 10), Oncology Care Services (n = 9), and Supportive and Palliative Care (n = 8). Commonly cited therapies include cetuximab, trastuzumab, gefitinib, pembrolizumab, and ALK inhibitors. Breast, ovarian, lung, and colorectal cancers emerge as the most frequently discussed tumor types.
When examining the studies by journal source, it becomes clear that most fall under the “Other” category—encompassing JAMA, Health Affairs, Implementation Science, and similar outlets—totaling 18 publications. In addition, a notable cluster appears in the Journal of Oncology Practice (n = 8), while the Journal of Managed Care & Specialty Pharmacy accounts for five studies (n = 5).
Of the 40 studies included, 24 list authors with specific advanced credentials, primarily PharmDs, PhDs, and MD/DO degrees. Authors classified under “master’s level” or “N/A” indicate no relevant qualifications. Among those with documented advanced degrees, most are medical doctors (n = 20), followed by a diverse “Other” group—including MA, MS, MHS, MBA, JD, and similar backgrounds—and finally, those who do not meet any credential category (n = 19).
These findings reveal that although APMs in oncology continue to garner growing attention, research exploring their integration with novel therapies—beyond a cost or utilization lens—remains limited. This gap underscores the need for more targeted inquiries that evaluate economic and administrative feasibility, real-world clinical outcomes, and the impact of the models on equitable patient access.
Thematic Analysis
Key themes emerging from the literature include perceived value of precision oncology therapies, need for robust comparative evidence against standard-of-care treatments, and the impact of diagnostic testing on clinical utility and overall value assessment. To address the first research question involving the current status of APMs in oncology care, this review conducts a thematic analysis to identify common patterns, challenges, and opportunities across the literature. This analysis offers insight into how APMs are currently designed, implemented, and evaluated within the oncology space in U.S. healthcare.
| Theme | Citation (First Author, Publication Year) | Supportive Evidence |
|---|---|---|
| Clinical Pathways | Abrahams et al. (2017), Nejati et al. (2019), Wen et al. (2018), Panchal et al. (2023) | Oncology clinical pathways are “multidisciplinary care plans that translate evidence into specific guidance on the sequencing of care and the timeline of interventions for patients with specific diagnoses and characteristics.” Adoption of clinical pathways was consistently associated with reductions in resource use and costs for various cancer types. |
| Value-Based Care | Abrahams et al. (2017), Aviki et al. (2018), Brooks et al. (2022), Frois et al. (2019), Reitblat et al. (2021), Panchal et al. (2023), Oderda et al. (2024) | Economic pressures from payers are the foremost leading factor in the oncology provider landscape. Few studies have critically assessed the actual or simulated implementation of value-based healthcare in urology. However, the available literature suggests promising early results. |
| Quality Measurement & Improvement | Pai et al. (2020), Seymour et al. (2020), Ems et al. (2018), Nejati et al. (2019) | Quality measures are necessary because they can help improve and standardize cancer care delivery among healthcare providers and across tumor types. Emphasizing decreased use of unnecessary imaging, testing, treatment, and surgeries. Use of patient-reported outcome measures (PROM). |
| Barriers to Implementation | Panchal et al. (2023), Reitblat et al. (2021), Oderda et al. (2024) | Substantial cost associated with implementing a clinical care pathway program. Adopting innovations in healthcare services and therapies adds to the site’s financial risk. Structural barriers pose a significant challenge to piloting these principles in general, including a lack of consensus around the best-operationalized value measurement, limited IT infrastructure to enable integrated care, and the complexity of financial risk sharing. |
Key Themes Highlighting the Current Status of APMs in the U.S. Healthcare System
Clinical Pathways
Clinical pathways highlight the current shift to value-based frameworks that enhance care quality and cost efficiency. Clinical pathways represent a practical tool promoting VBC by standardizing treatments and improving efficiency. Clinical pathways incorporate transparency, evidence-based decisions, and regular updates reflecting current scientific evidence and clinical advances for proper implementation. The current status of APMs continues to try to address additional cost savings for institutions that warrant the cost of implementation. For example, the Centers for Medicare & Medicaid Services (CMS) actively promotes APMs through initiatives like the Quality Payment Program (QPP), which includes tracks such as the Merit-based Incentive Payment System (MIPS) and Advanced APMs. These models incentivize providers to deliver high-quality, coordinated care, which can lead to cost savings. Clinical pathways are a step towards that goal due to their associations with reductions in resource use and costs for various cancer types. One study adopting a clinical pathway across 46 cancer settings was associated with a 75% reduction in hospitalization costs per patient over three years. However, the success of these pathways depends on continuous updates to reflect the latest advancements.
While the financial efficacy of clinical pathways may be evident, a patient-centric approach must address health equity. A current challenge is maintaining transparency in creating clinical pathways. There is minimal transparency on how the creation of pathways keeps the patient as the primary focus. Whether that is how payers or developers consider the cost to determine treatment on the pathway, this issue aligns with the current status of APMs in the healthcare system as new models and new incentives continue to address the shortfalls of previous models.
Value-Based Care (VBC)
Value-based care (VBC) in the U.S. represents a strategic shift from the traditional FFS model, which rewards providers based on volume rather than quality of care. Value-based care prioritizes delivering better health outcomes relative to cost and urges providers to focus on safety, efficacy, patient-centeredness, timeliness, efficiency, and equity. This approach first gained traction in oncology, where rising costs, inconsistent care quality, and rapid innovation highlight the need for more accountable, coordinated care delivery. To translate VBC into practice, stakeholders must implement APMs, including ACOs, bundled payments, Patient-Centered Medical Home (PCMH), and OCMs. These APMs link reimbursement performance to cost-efficiency metrics and aim to improve care delivery through tools like clinical pathways and care coordination infrastructure.
Despite growing adoption, the implementation of APMs remains uneven across the U.S. Providers continue to face barriers such as limited IT infrastructure, misaligned incentives, administrative burdens, and unclear definitions of value. Clinical pathways, a key mechanism for operationalizing VBC, often lack transparency and rarely include patient input during development, limiting flexibility and access to newer therapies. Many cancer centers also struggle to incorporate patient experience and outcomes into their value frameworks, with 50% reporting using real-world data to support such efforts. Providers frequently rely on internal consensus or National Comprehensive Cancer Network (NCCN) guidelines over value frameworks, citing limited integration into reimbursement systems and a lack of actionable guidance.
Despite these limitations, evidence from other specialties shows that value-based strategies can succeed with proper infrastructure support. Reitblat et al. demonstrate that guideline adherence, outcome measurement, and integrated team-based care models in urology improve survival, reduce hospitalizations, and lower costs.
Quality Measurement & Improvement
Advancing APMs within oncology care involves developing and applying quality measurement strategies to standardize and improve care delivery. Both Pai et al. and Seymour et al. highlight that robust quality metrics must ensure payment models do not inadvertently incentivize under-treatment or compromise clinical outcomes. Instead, these measures must enhance consistency and the value providers deliver.
One central focus area is reducing low-value or unnecessary services, such as redundant imaging, excessive laboratory testing, and inappropriate surgical interventions. Pai et al. underscore that grounding APMs in quality metrics discourages unnecessary practices and reinforces evidence-based clinical guidelines. Such measures help reduce costs and mitigate potential patient harm from overtreatment or overuse of diagnostic procedures.
Another emerging dimension within quality measurement is integrating patient-reported outcome measures (PROMs). Patient-reported outcome measures capture critical dimensions of the patient experience, including treatment-related burdens, functional status, and financial strain, which clinical endpoints often overlook. Pai et al. advocate for PROMs in evaluating immunotherapy outcomes, particularly identifying functional decline associated with immune-related adverse events and elevating patient-defined priorities like cognitive, emotional, and financial well-being. Patient-reported outcome measures also call for patient involvement in measure development to ensure relevance and impact. Similarly, Seymour et al. argue that VBC insurance design should prioritize interventions that improve PROMs, emphasizing the need for validated tools to assess the financial burden and align patient cost-sharing with treatment value rather than price alone.
Barriers to Implementation
Current literature supports theoretical benefits of APMs in oncology while highlighting several practical and structural barriers to real-world implementation. These challenges reflect the complexity of translating VBC principles into the fragmented and high-stakes environment of cancer care delivery, highlighting the evolving implementation of APMs.
Panchal et al. identify a prominent barrier as the substantial requirement of cost and resource investments to operationalize APMs, particularly when implementing clinical pathways. These programs require significant upfront investment to build infrastructure, train staff, and align workflows with VBC objectives. Effective APMs often require integrated electronic health records, real-time data sharing, and analytic capabilities to track outcomes and costs. These requirements disproportionately affect smaller practices and community oncology centers, as they lack the infrastructure to scale and absorb expenses without jeopardizing financial sustainability.
Financial risk is a recurring challenge in adopting innovative therapies and services. In oncology, where treatments are expensive and outcomes often uncertain, providers face significant concerns regarding reimbursement and potential financial losses. Reitblat et al. suggest that this risk aversion exacerbates the existing FFS model, which may discourage experimentation with APMs and limit participation. Additionally, the complexity of financial risk-sharing agreements also deters adoption.
While quality metrics exist, operationalization varies widely across payers, programs, and institutions. Poor operationalization creates confusion and undermines the need for standardization in the widespread implementation and execution of APMs.
APMs and Patient Access
This systematic literature review analyzes access through Penchansky and Thomas’ definition, which consists of five dimensions: Availability, Accessibility, Accommodation, Affordability, and Acceptability. Penchansky and Thomas’ work inspired a set of specific dimensions that fit between the patient and the health care system. Other definitions of patient access highlight the need to include and consider multiple factors.
| A1 – Availability | Study (First Author, Year) | Key Insight | Net Impact |
|---|---|---|---|
| Abrahams et al., 2017 | Clinical pathways may narrow treatment options by limiting shared decision-making. | Mixed | |
| Baumgardner et al., 2018 | APMs such as the Oncology Care Model incentivize coordinated resource use. | Positive | |
| Nejati et al., 2019 | Pathways reduce low-value services and resource use but may restrict access if not updated regularly. | Mixed | |
| Seymour et al., 2020 | APMs enhance availability via 24/7 access, triage systems, and evidence-based practice redesign. | Positive | |
| Oderda et al., 2024 | Reimbursement strategies must balance cost, actionability, and clinical relevance. | Mixed |
| A2 – Accessibility | Study (First Author, Year) | Key Insight | Net Impact |
|---|---|---|---|
| Panchal et al., 2023 | APMs more commonly adopted in outpatient settings; increase access to high-value care. | Positive | |
| Segel et al., 2021 | Rural and safety-net hospitals face barriers in meeting APM benchmarks. | Negative | |
| Reitblat et al., 2021 | Structural barriers, such as weak coordination and IT limitations, hinder accessibility. | Negative | |
| Polson et al., 2019 | Many patients fail to meet episode criteria, limiting access to bundled-payment benefits. | Negative |
| A3 – Accommodation | Study (First Author, Year) | Key Insight | Net Impact |
|---|---|---|---|
| ASCO Policy Statement, 2016 | Clinical pathway development lacks transparency and burdens providers administratively. | Negative | |
| Kocher & Adashi, 2023 | Models like EOM improve care alignment with patient needs but require infrastructure investment. | Mixed | |
| Kline et al., 2021 | Practices using APMs more likely to offer extended hours and symptom management. | Positive |
| A4 – Affordability | Study (First Author, Year) | Key Insight | Net Impact |
|---|---|---|---|
| Trombley et al., 2024 | OCM reduced total cost per episode by minimizing hospitalizations and unnecessary care. | Positive | |
| Chambers et al., 2018 | Specialty drug coverage varies widely across health plans. | Negative | |
| Segel et al., 2021 | Rural hospitals often fail to meet risk benchmarks, increasing costs and reducing sustainability. | Negative | |
| Seymour et al., 2020 | APMs reduce out-of-pocket burden through more efficient care pathways. | Positive |
| A5 – Acceptability | Study (First Author, Year) | Key Insight | Net Impact |
|---|---|---|---|
| Zafar, 2015 | Financial toxicity reduces treatment adherence and trust in system. | Negative | |
| Reitblat et al., 2021 | High-cost therapies require cultural readiness and patient trust for effective shared decision-making. | Mixed | |
| Seymour et al., 2020 | APMs must prioritize culturally competent communication to foster trust and satisfaction. | Mixed |
Legend:
- Positive: Supports access
- Mixed: Some evidence of improvement, but with limitations
- Negative: Barriers or reduced access observed
A1 – Availability
The first A stands for “Availability.” Penchansky and Thomas define “Availability” as “the physical presence of services or resources.” Researchers code availability whenever a study presents patients and healthcare providers sharing a decision-making experience with novel oncology treatments. Abrahams et al. identify clinical pathways as narrowing treatment availability because some pathways undergo development without meaningful patient involvement. Another example by Baumgardner et al. speaks to APMs like the OCM, incentivizing efficient resource use and care coordination to positively influence a patient’s access to care. However, Nejati et al. conclude that adopting clinical pathways demonstrates reductions in resource use, reduction of low-value services, and lower cancer care costs. This inconsistency of conclusions highlights the need for additional data on APMs to distinguish which models positively impact patient access and which do not.
Seymour et al. highlight how APMs enhance access to oncology care by redesigning practices. Providers can set up a practice that includes around-the-clock clinical availability, care coordination, and care focused on evidence-based guidelines. Alternative payment models reduce low-value care and high cost while increasing access to high-value therapies and care by making providers and resources more readily available.
Much of the available literature on APMs and implementation does not include the payer perspective. Payers are essential in determining the availability of treatments to patients. In Table 4, Oderda et al. emphasize how vital the financial aspect of reimbursement is to establish APMs. The authors underscore prioritizing clinical relevance, actionability, and cost savings for payer decision-making. Runyan et al. observe that only a few payers use APMs, with slightly more planning to adopt them in the next few years. Without the widespread implementation of APMs, the availability of innovative treatments will continue to be in battle with traditional utilization management tools like step therapy.
A2 – Accessibility
The second “A” in the five dimensions of access stands for Accessibility. Penchansky and Thomas define this as “geographic and logistical ease of obtaining services.” Often, innovative treatments for cancer care involve specialists who may be far from a patient’s home. During the 2023 National Comprehensive Cancer Network (NCCN) policy summit, Cancer Across Geography, panelists emphasized that “where you live should not determine whether you live.” Alternative payment models help facilitate receiving care by involving closer-to-home care in outpatient settings.
The literature reveals that outpatient cancer centers are more likely to adopt APMs than academic centers. Adoption of APMs allows the centers to transition to VBC models with minimal institutional barriers easily. That same study highlights how implementing APMs improves accessibility to innovative therapies, care coordination, and patient-centered services while identifying financial barriers and administrative burdens as key challenges to broad and equitable adoption across different settings.
Of the 40 studies analyzed in this paper, 29 (72.5%) focus on patients in a mixed oncology setting (inpatient and outpatient). Rural hospitals and clinics often treat the most vulnerable patient populations and frequently experience high volumes of reduced patient outcomes, high mortality percentages, and emergency room visits. These factors severely mitigate an institution’s ability to meet risk-adjusted benchmarks, preventing full participation in APMs. However, APMs are not uniform; where one model may not work well for a patient population, care setting (e.g., outpatient vs. inpatient), or disease state, it may facilitate care in other scenarios.
Another accessibility component is care coordination. Reitblat et al. highlight the structural barriers—such as care coordination—that limit broad implementation and equitable access to VBC models. Patients, caregivers, providers, manufacturers, and payers contribute significantly to care coordination. For example, Polson et al. explain how episode-based payment models apply to Medicare and commercial health plans, encouraging broader payer participation in oncology care. Conversely, the same study finds that many cancer patients fail to meet the criteria for qualifying episodes, leading to reduced access to the model. A significant challenge in developing an APM lies in the details, especially metrics, for ensuring efficient and cost-effective implementation.
A3 – Accommodation
Payers represent one of the most significant unknowns when understanding the prioritization of components for coverage and reimbursement. Moreover, in novel oncology treatments, the typical and well-validated randomized controlled trial—the industry gold standard—is not readily achievable with smaller patient populations and unique disease settings.
Organizations such as the American Society of Clinical Oncology (ASCO) apply a multistakeholder perspective when utilizing clinical pathways, a form of APM, to enhance quality and value. ASCO raises concerns about a lack of transparency in pathway development, administrative burdens on oncology practices, and difficulty understanding the actual value of pathways on patient outcomes. Variations among payers in oncology care management and APM adoption hinder access to evidence-based frameworks and cost-effective care. Models like the OCM have limited uptake since their rollout, leaving patients reliant on traditional management tools such as step edits and formulary blocks. Additionally, APMs require adequate care teams and scheduling systems, particularly within models like the OCM. These models aim to reduce unnecessary hospitalizations and emergency department visits by increasing access to outpatient care and proactive symptom management. Many studies highlight how APMs incentivize practices to offer extended hours, same-day appointments, and 24/7 access to clinicians, improving the flexibility and responsiveness of care for patients experiencing urgent side effects or complications. Care coordination and navigation—often supported by APM funding—emerge as central components, emphasizing roles like nurse navigators and care coordinators. One example is the EOM, which builds on the previous OCM by focusing more on patient needs and preferences.
The literature suggests that APMs in oncology drive meaningful innovation in care structure and delivery, with promising implications for improving accommodation. However, the extent to which these changes benefit patients depends on the practice setting. Larger clinical and academic programs demonstrate greater sustainability in accommodating patient needs, partly due to their superior resources and infrastructure compared to smaller community-based practices.
A4 – Affordability
The development of APMs improves patient care and reduces costs through value-based incentives. These incentives motivate stakeholders to adopt new care delivery approaches without exposing them to unmanageable administrative, financial, and clinical risks. In contrast, FFS models prioritize volume-based financial incentives, which lead to the overuse of low-value services and suboptimal care. Alternative Payment Models increase accountability for quality and total care cost and promote high-value therapies. This shift reshapes financial reforms that reduce patient cost burdens by lowering out-of-pocket expenses for essential treatments.
Alternative Payment Models, such as bundled payments, episode-based payments, and the OCM, create downward pressure on overall costs, aiming to eliminate unnecessary and duplicative services. Theoretically, these models incentivize high-quality, cost-effective care by shifting from volume-based to value-based reimbursement, which improves patient affordability. The Oncology Care Model, for example, reports reductions in total cost of care per episode, primarily due to fewer hospital admissions and better symptom management through triage teams.
However, some APMs inadvertently contribute to disparities in access by disadvantaging certain hospitals, particularly rural facilities and those unaffiliated with academic medical centers. These equity concerns highlight uneven distribution of affordability. Using Medicare-linked data from 2007 to 2015 for breast or prostate cancer patients, researchers observe higher-than-expected mortality rates at for-profit hospitals, hospitals unaffiliated with medical schools, and rural hospitals. The results also show that hospitals serving underserved or high-risk populations struggle to meet risk-adjusted performance benchmarks, limiting their success within the OCM and challenging their ongoing participation.
A5 – Acceptability
The final A in the five dimensions of access stands for “Acceptability.” Acceptability, as conceptualized by Penchansky and Thomas, refers to the degree of congruence between patients’ attitudes and the characteristics of healthcare providers, including their values, communication style, and perceived responsiveness. In oncology, acceptability is a crucial yet often underexplored factor affecting access to care. As APMs attempt to improve care quality while controlling costs, they may inadvertently neglect cultural, linguistic, and psychosocial considerations that influence how patients perceive care. This issue is particularly salient for novel cancer therapies, which often require complex treatment regimens and a high level of trust between patient and provider. For patients from underserved or historically marginalized communities, a lack of cultural competence, miscommunication, or perceived bias may lead to discomfort, distrust, or disengagement from the treatment process. Thus, APMs that fail to integrate patient-centered strategies—such as culturally appropriate communication and shared decision-making—risk undermining treatment adherence and overall care effectiveness.
The Acceptability dimension also reflects how patient engagement, informed consent, and shared decision-making contribute to the success of innovative oncology treatments under APMs. Models like the EOM aim to improve patient outcomes by emphasizing value and experience; however, they lose impact when providers and patients fail to align in communication or mutual understanding. High-cost therapies such as CAR-T or gene-based treatments require patients to have technical comprehension and emotional and cultural readiness. When APMs prioritize performance metrics or administrative efficiency without addressing these softer dimensions of care, they risk alienating patients or fostering treatment hesitancy.
Discussion
The purpose of this paper is to address two specific questions. The first focuses on the current status of APMs in the U.S. healthcare system—a detailed thematic analysis identifies and explores multiple areas to characterize the current status, addressing this question. Themes include Clinical Pathways, Value-Based Care, Quality Measurement and Improvement, and Barriers to Implementation. The second research question relates to how APMs improve patient access. Using the lens of the 5As, this analysis highlights critical elements that enable this work to engage with the literature and the nuances relevant to Affordability, Availability, Accessibility, Accommodation, and Acceptability. The most significant dimension within the literature revolves around affordability. The second most frequent dimension within the analysis involves multiple As. This observation suggests that the literature identifies access as a multidimensional phenomenon. Further discussion of these considerations relevant to the two research questions, as well as their importance and implications for practice and policy, follows in this discussion section. This dialogue presents an explanatory model and research agenda with relevant questions. This section then closes by highlighting contributions to knowledge and practice, implications, limits of this research, strategies to address potential concerns, and future research questions.
Alternative Payment Models in U.S. Healthcare
The current status of APMs in the U.S. healthcare system has significantly evolved since inception. Initially, FFS models dominated the healthcare landscape, incentivizing priority volume over value, leading to fragmented care and escalating costs. Recently, implementing APMs aims to address these insufficiencies, stressing the importance of quality and outcomes. To put VBC into action, APM implementation includes models such as Accountable Care Organizations (ACOs), bundled payments, Patient-Centered Medical Homes (PCMHs), and Oncology Care Model (OCM). This current research displays that, while the adoption of APMs is on the rise, barriers still exist that limit consensus uptake by institutions.
This work’s findings show that through appropriate implementation with supporting infrastructure, APMs are successful in both patient outcomes and cost. The lack of consensus adoption can primarily be due to switching from FFS to APMs, which demands considerable financial and resource investment. Establishing APMs requires substantial investment to develop infrastructure, educate personnel, and synchronize workflows with value-based goals. This point underscores that adopting APM involves financial risk; stakeholders must address concerns about reimbursement and potential economic loss to support the continued growth of these models.
Value-based care (VBC) principles, specifically in oncology, help drive the implementation of APMs. Value-based care’s purpose is to deliver high-quality care that is personalized, efficient, and affordable. Our findings show that principles of APMs that focus on VBC include patient-centered care, evidence-based practices, care coordination, and quality and safety. Alternative Payment Models incentivize stakeholders like manufacturers, payers, and providers to collaborate to pave the way for patient access to novel oncology therapies. Examples in the literature include ACOs, bundled payments, PCMHs, and OCMs. These instances of APM implementation call attention to the importance of creating reimbursement models as up-to-date as the novel therapies they cover.
Despite promising initiatives, there is a limit to the real-world uptake of APMs in oncology, with notable constraints by systemic misalignments among stakeholders. Provider, patient, and payer resistance often reflects more profound inconsistency in incentives, infrastructure, and capacity. For providers, especially those in community settings, high administrative burdens and data infrastructure demands serve as barriers to participation and sustainability. Additionally, smaller practices and community centers often lack the infrastructure to scale and absorb such expenses. Patients, meanwhile, may distrust value-based models that appear to prioritize cost containment over personalized care, revealing a gap between theoretical patient-centeredness and actual perceptions. Payers remain skeptical of APM return on investment, citing a lack of standardized metrics, outcome variability, and operational complexity. Their hesitation also reflects a broader challenge in oncology in defining and measuring “value” amid rapid innovation and rising costs. While APMs offer a blueprint for aligning cost and quality, current models often layer into a system that does not have the infrastructure to support them.
This hurdle suggests that the future success of APMs in oncology depends on refining the model design and rethinking the underlying health system conditions in these models’ functions. Policymakers and stakeholders must address technical barriers and relational and infrastructural deficits that hinder trust and collaboration across these stakeholders.
Factors of Patient Access and APMs
The paper’s second objective focuses on identifying patient access within APMs. Access is central to health policy and healthcare. Although access is an important concept, it does not have a widely used standardized definition. Government agencies and the private sector attempt to define patient access to care using combinations of components like coverage, timeliness, and seamless data exchange between patients, providers, and payers.
Proposals for access-focused value assessment frameworks are also more common in complex oncology and immune-mediated inflammatory diseases. These frameworks use core components to measure patient access and care improvements, much like APMs. As medicines become more innovative and novel, the usual reimbursement models that cover heart failure and high cholesterol medicines cannot appropriately apply to novel drugs that only treat a fraction of the world’s population.
Alternative Payment Models in oncology influence patient access through multiple dimensions, as defined by Penchansky and Thomas’s 5As framework. Alternative Payment Models, such as the OCM, affect availability, incentivizing providers to offer more coordinated, guideline-concordant services and increasing access to evidence-based treatments. Accessibility, defined as the geographical and logistical ease of obtaining care, may improve through enhanced care coordination. Yet, disparities remain for rural and underserved populations with scarce oncology services. Accommodation, referring to how health services meet patients’ needs, often improves under APMs due to greater emphasis on patient navigation and after-hours care. Nonetheless, some providers may lack the infrastructure to implement these changes fully. Reducing unnecessary spending and lowering out-of-pocket costs through better-managed care pathways addresses affordability, although the effects on individual patient financial burdens remain uneven.
Lastly, patient satisfaction and alignment with expectations may improve acceptability by incentivizing providers to focus on patient-centered outcomes. However, concerns about a reduction in treatment choices can affect trust in the system. Overall, APMs promise to improve access to oncology care, but their impact is variable across the five dimensions and warrants ongoing evaluation to ensure equity and effectiveness.
This work’s findings highlight affordability as the most frequent dimension of the 5As. This finding is no surprise due to the worldwide attention the U.S. healthcare system draws. Alternative Payment Models move payment models away from FFS to increase accountability for quality and total cost of care and emphasize population health management in place of specific services. Specifically, regarding oncology therapies, novel treatments routinely replace more immediate lines of treatment options. Often, they present as first-line treatment options or, in the cases of rare cancers, as the only treatment option.
Payers represent one of the biggest unknowns when understanding the prioritized components for coverage and reimbursement. Especially in novel oncology treatments, where the well-validated randomized control trials, an industry gold standard, are not easily achieved with the smaller patient populations and unique disease settings. The variation among different payers regarding oncology care emphasizes the importance of patient-centered outcomes and APMs. Organizations like ASCO take a multistakeholder perspective when using clinical pathways, a form of APM, as tools for enhancing quality and value. The concerns that ASCO issues recommendations for include pathway development, administrative burdens on oncology practices, and understanding the actual value of the pathways on patient outcomes. Since the adoption and implementation of APMs are in early development compared to traditional reimbursement processes, these recommendations are part of an ongoing iterative process.
Health Policy Implications
Key opinion leaders and influencers in the U.S. healthcare ecosystem include payers, employers, policymakers, and providers. Patients, caregivers, and patient advocates should have the ability to collaborate with these key opinion leaders to create clear patient access options. To that end, health policy must evolve to ensure that APMs meaningfully address the multidimensional aspects of access, particularly for populations with limited availability of specialized services or affordability barriers. Adopting APMs creates an opportunity for more equitable and sustainable access to novel oncology products, but without deliberate policy design, these models risk reinforcing existing disparities. Policymakers must take a proactive role in facilitating multistakeholder collaboration, including regulators, manufacturers, payers, and patient advocacy groups, to define what success looks like for access within APMs.
Contributions
This review contributes to both academic knowledge and real-world APM implementation.
Contributions to Theory
This paper proposes a novel stakeholder-driven explanatory model around APM development, process, and outputs. This input-moderator-process cycle-output (IMPO) model reflects critical elements emerging from the literature. It depicts relevant inputs and influences on the process cycle involving APM development and implementation as a central point, leading to appropriate outputs. It starts with collaboration among manufacturers, payers, providers, and patients as critical inputs to the successful design and implementation of APMs. The model begins with these critical stakeholders because barriers to patient access must begin with stakeholders who impact care delivery.
Manufacturers, payers, providers, and patients provide data that help create clinical pathways, value-based care models, and quality measures that drive improvements. Manufacturers have clinical trial data, real-world data, and patient-reported outcomes later in the life cycle. Payers have claims data that tell the stories of hundreds of patients and their care, from office visits to treatment administration. Providers and care teams frequently have hands-on experiences with patients and treatment administration. By starting the process with manufacturers and considering barriers to implementation, the development of APMs can limit hiccups from FDA approval to patient use. Including patients at the beginning of this model is key because, through their stories and experiences, patients identify barriers and help create solutions to increase access to novel oncology products.
The moderators in the model reflect barriers to implementing APMs, which this review identified in the literature in addressing the first research question. These included provider-to-population ratios, travel time to care, appointment flexibility, out-of-pocket (OOP) costs, and patient satisfaction as barriers to APM implementation. The literature also noted a negative impact on patient access for providers with limited IT infrastructure, administrative burdens, and unclear definitions of value patient access to novel oncology care. Payers presented several barriers to APM implementation, including limited integration into existing reimbursement systems and a lack of actionable guidance. Additionally, patients reflected a lack of care coordination and frustrations over the parity of patient voice in developing APMs.
Figure 2. Theoretical IMPO Model Highlighting Components of Alternative Payment Model (APM) Development
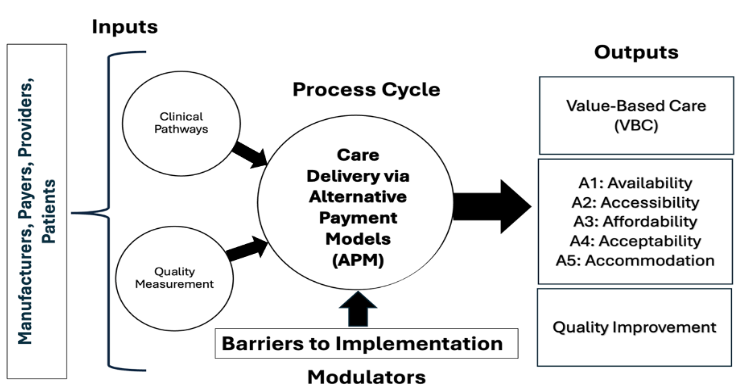
The process cycle describes delivering care through an APM. This process cycle considers the inputs (relevant stakeholders) and the moderators (barriers to implementation) to denote the development of APMs in novel oncology care. The outputs – value-based care (VBC), the 5As, and Quality Improvement- emerge at the end of the model, as previously discussed in this paper. These three outputs result from the process cycle using the inputs and moderators to develop innovative APMs to match the most recent innovative oncology products.
This paper also contributes to the existing knowledge available by advancing the theoretical understanding of access to novel oncology care by applying the Penchansky and Thomas five-dimension access model—Availability, Accessibility, Affordability, Accommodation, and Acceptability—to evaluate the effectiveness of APMs. Using the framework provides a structured, multi-faceted view of patient access that enriches current value-based care literature. This work provides a comprehensive systematic review of 40 peer-reviewed articles, thematically organized to highlight the current status of APMs in oncology care and impact on patient access to novel oncology care. It offers insights into clinical pathways, quality measurement and improvement, implementation barriers, and value-based care principles as these components relate to the current status of APMs in the U.S. healthcare system.
Contributions to Practice
Regarding contributions to practice, this paper provides actionable insights for oncology providers, particularly those in community settings. The findings highlight the infrastructure and care coordination requirements of successful APMs and identify practical limitations such as administrative burdens, financial risk, and technology constraints. Addressing the barriers to implementation practices can help evaluate the capabilities and investments needed for adoption. Highlighting the diversity of settings (inpatient/outpatient) in APMs plays a role in facilitating increased awareness and evaluation toward implementation. For healthcare administrators and policymakers, the findings of this paper outline best practices and shortcomings of current APMs, including a need for patient-centered design, the importance of standardized metrics and real-world evidence, as well as the risks of excluding smaller and rural practices from innovation due to infrastructure or financial challenges. The analysis directly supports health equity efforts by exposing disparities in access to novel oncology treatments across underserved populations and geography. The findings identify ways APMs may reduce or exacerbate inequities, informing payers and providers on how to build and implement models more equitably. Lastly, the work emphasizes the necessity of cross-sector collaboration—including policymakers, manufacturers, payers, and providers—to define success criteria and enhance trust and alignment in oncology APMs. Notable contributions of this research to the existing literature lie in the novel IMPO model, assessing APMs through the lens of 5As, a thematic analysis focused on components that apply to oncology and other therapeutic areas.
The paper’s second objective focuses on identifying patient access within APMs. Access is central to health policy and healthcare. Although access is an important concept, it does not have a widely used standardized definition. Government agencies and the private sector attempt to define patient access to care using combinations of components like coverage, timeliness, and seamless data exchange between patients, providers, and payers.
Proposals for access-focused value assessment frameworks are also more common in complex oncology and immune-mediated inflammatory diseases. These frameworks use core components to measure patient access and care improvements, much like APMs. As medicines become more innovative and novel, the usual reimbursement models that cover heart failure and high cholesterol medicines cannot appropriately apply to novel drugs that only treat a fraction of the world’s population.
Alternative Payment Models in oncology influence patient access through multiple dimensions, as defined by Penchansky and Thomas’s 5As framework. Alternative Payment Models, such as the OCM, affect availability, incentivizing providers to offer more coordinated, guideline-concordant services and increasing access to evidence-based treatments. Accessibility, defined as the geographical and logistical ease of obtaining care, may improve with better care coordination. Yet, disparities remain for rural and underserved populations with scarce oncology services. Accommodation, referring to how health services meet patients’ needs, often improves under APMs due to greater emphasis on patient navigation and after-hours care. Nonetheless, some providers may lack the infrastructure to implement these changes fully. Reducing unnecessary spending and lowering out-of-pocket costs through better-managed care pathways addresses affordability, although the effects on individual patient financial burdens remain uneven.
Lastly, patient satisfaction and alignment with expectations may improve acceptability by incentivizing providers to focus on patient-centered outcomes. However, concerns about a reduction in treatment choices can affect trust in the system. Overall, APMs promise to improve access to oncology care, but their impact is variable across the five dimensions and warrants ongoing evaluation to ensure equity and effectiveness.
This work’s findings highlight affordability as the most frequent dimension of the 5As (Figure 3). This finding is no surprise due to the worldwide attention the U.S. healthcare system draws. Alternative Payment Models move payment models away from FFS to increase accountability for quality and total cost of care and emphasize population health management in place of specific services. Specifically, regarding oncology therapies, novel treatments routinely replace more immediate lines of treatment options. Often, they present as first-line treatment options or, in the cases of rare cancers, as the only treatment option
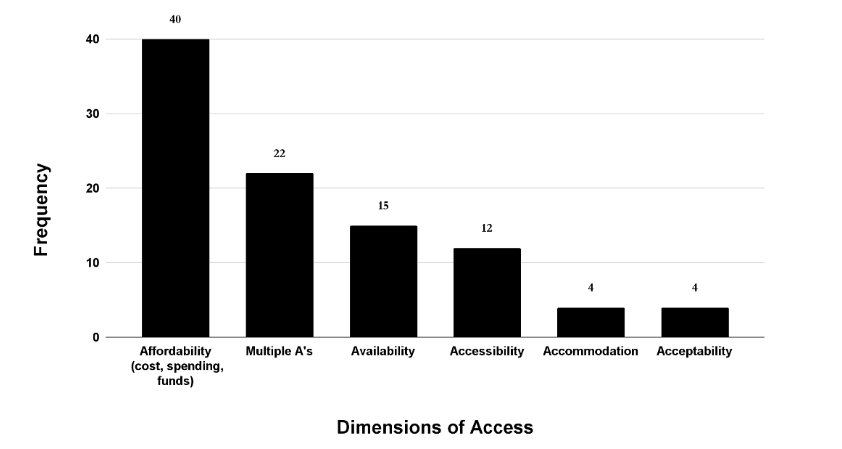
Figure 3. Frequency of Penchansky and Thomas’ 5As in the Literature Examined
Payers represent one of the biggest unknowns when understanding the prioritized components for coverage and reimbursement. Especially in novel oncology treatments, where the well-validated randomized control trials, an industry gold standard, are not easily achieved with the smaller patient populations and unique disease settings.
The variation among different payers regarding oncology care emphasizes the importance of patient-centered outcomes and APMs. Organizations like ASCO take a multistakeholder perspective when using clinical pathways, a form of APM, as tools for enhancing quality and value. The concerns that ASCO issues recommendations
Limitations
This review identifies some limitations. Firstly, there is limited generalizability. Studies are often based on specific populations or limited geographic regions, meaning the findings may not be generalizable to other areas or different types of health plans. Analyses on particular cancer types may not apply to others. Small sample sizes in some studies or specific analyses (e.g., practice-level analyses) further limit generalizability. Studies based on hypothetical simulations rather than real-world implementation may also lack generalizability.
Secondly, some studies note challenges regarding implementation and stakeholder involvement. Information asymmetry exists between payers and providers, and payers often consider payment models proprietary. Providers may resist sharing actual costs. Additional challenges include the complexity and burden of implementing APMs. A key barrier for providers is the financial risk of adopting innovations within APMs before formal adoption. Providers need more explicit guidance on assessing value within these changing payment environments. The lack of strong links between public and private stakeholders is a general barrier to APM financing and reimbursement.
Thirdly, more research is needed on how financing strategies influence evidence-based implementation. Additional factors that would benefit from additional research are those associated with the sustainability of support programs, such as patient navigation, under APMs. Furthermore, evidence is insufficient regarding the impact of APMs on patient outcomes, such as survival, recurrence, and quality of life, especially in integrating novel therapies, particularly the lack of real-world data linking APM participation with clinical outcomes (e.g., survival, recurrence).
Lastly, this research involves a systematic literature review, and there are limits to the depth of the sources pulled. Additionally, because the review relied on individual reviewers, the review is subjective. Most papers had one reviewer, and having multiple reviewers would end up giving a less subjective view.
Research Agenda
Providers are increasingly forced to incorporate value-based considerations in therapy decisions as the landscape shifts from volume to value. Future research is needed to understand how providers define and assess the value of novel therapies under different APMs and what evidence they need to make value-based decisions. Another vital research area in this space is evaluating financial risk by quantifying tradeoffs between shared savings opportunities and economic uncertainty for providers when including drug costs in bundled or capitated payments. As APMs expand, it is critical to understand which types of hospitals or practices might be disproportionately advantaged or disadvantaged, affecting the delivery and availability of novel therapies that may be concentrated in specific settings and centers. Similarly, when it comes to patient access, research is needed to determine the administrative impact of APMs, which includes the sustainability of support programs, such as patient navigation, which are essential for coordinating care, especially for patients receiving complex novel treatments.
Conclusion
This systematic review evaluated the role of alternative payment models in expanding access to novel oncology therapies within the United States. The findings underscore the growing interest in payment reform and reveal four recurring themes shaping the current landscape: clinical pathways, value-based care implementation, quality improvement strategies, and persistent barriers to adoption. While these models aim to balance cost control with improved outcomes, their real-world application remains inconsistent due to infrastructure challenges, administrative burdens, and misaligned incentives across stakeholders.
By applying a five-dimensional (5A) access framework, this review demonstrates that alternative payment models can enhance affordability, availability, and accommodation. However, significant disparities persist—particularly for rural, smaller, or underserved care settings—where such models are harder to implement. Acceptability and accessibility dimensions are often overlooked, especially regarding cultural responsiveness and care coordination. To achieve equitable access, future models must adopt a more inclusive, patient-centered design.
Ultimately, success will require collaborative leadership from payers, policymakers, manufacturers, providers, and patients. A refined stakeholder-driven process model introduced in this review offers a practical roadmap for designing payment innovations that support sustainable, high-value oncology care in an era of personalized medicine.
Funding: No funding was received for this work.
Conflict of Interest: At the time of research, Dr. Salih reported being a contract employee with the National Pharmaceutical Council as a sponsor for the Rutgers Pharmaceutical Industry Fellowship Program. Drs. Jash and Wong reported being contract employees with Sanofi as a sponsor for the Rutgers Pharmaceutical Industry Fellowship Program. Dr. Patel reported being a contract employee with Johnson and Johnson as a sponsor for the Rutgers Pharmaceutical Industry Fellowship Program. Dr. Quintero reported being a contract employee with Bayer as a sponsor for the Rutgers Pharmaceutical Industry Fellowship Program. Dr. Jurasik reported being a contract employee with Bristol Myers Squibb as a sponsor for the Rutgers Pharmaceutical Industry Fellowship Program. Dr. York reported no competing interests for this work.
Acknowledgements: The authors would like to thank Santos Torres, Jr., MBA for his guidance and insights throughout this project. We used the generative AI tool Google NotebookLM to query citations, which were further reviewed and revised by the authors.
References
- Wang Y, Hou W, Wang X, Zhang H, Wang J. Bad to all? A novel way to analyze the effects of fee-for-service on multiple grades hospitals’ operation outcomes. Int J Environ Res Public Health. 2021; 18(23):12723. doi:10.3390/ijerph182312723
- Fainman EZ, Kucukyazici B. Design of financial incentives and payment schemes in healthcare systems: a review. Socioecon Plann Sci. 2020;72:100901. doi:10.1016/j.seps.2020.100901
- Darves-Bornoz AL, Resnick MJ. The evolution of financial incentives in the US healthcare system. Urol Oncol. 2017;35(1):1-4. doi:10.1016/j.urolonc.2016.09.011
- Fiorenza S, Ritchie DS, Ramsey SD, Turtle CJ, Roth JA. Value and affordability of CAR T-cell therapy in the United States. Bone Marrow Transplant. 2020;55(9):1706-1715. doi:10.1038/s41409-020-0909-6
- AAPC Editorial Team. Alternative Payment Models (APMs). Accessed January 21, 2025. https://www.aapc.com/resources/alternative-payment-models-apms
- Aviki EM, Schleicher SM, Mullangi S, Matsoukas K, Korenstein D. Alternative payment and care-delivery models in oncology: a systematic review. Cancer. 2018;124(16):3293-3306. doi:10.1002/cncr.31546
- National Association of Insurance Commissioners. Alternative payment methods: recent developments and trends. 2022. Accessed January 2025. https://content.naic.org/sites/default/files/cipr-report-alternative-payment-methods.pdf
- Howard SW, Bradford N, Belue R, Henning M, Qian Z, Ahaus K, Reindersma T. Building alternative payment models in health care. Front Health Serv. 2024;4:1235913. doi:10.3389/frhs.2024.1235913
- Nussbaum S, McClellan M, Metlay G. Principles for a framework for alternative payment models. JAMA. 2018;319(7):653-654. doi:10.1001/jama.2017.20226
- American Medical Association. Alternative Payment Models and Vulnerable Populations (Report 10 of the Council on Medical Service A-19). American Medical Association; 2019. Accessed January 2025. https://www.ama-assn.org/system/files/2019-07/a19-cms-report-10.pdf
- American Medical Association. Medicare Basics series: advancing value-based care with alternative payment models. American Medical Association; 2024. Accessed January 2025. https://www.ama-assn.org/practice-management/medicare-medicaid/medicare-basics-series-advancing-value-based-care-alternative
- Liao JM, Navathe AS, Werner RM. The impact of Medicare’s alternative payment models on the value of care. Annu Rev Public Health. 2020;41:551-565. doi:10.1146/annurev-publhealth-040119-094327
- Navathe AS, Liao JM, Wang E, et al. Association of patient outcomes with bundled payments among hospitalized patients attributed to accountable care organizations. JAMA Health Forum. 2021;2(8):e212131. doi:10.1001/jamahealthforum.2021.2131
- Zafar SY. Financial toxicity of cancer care: it’s time to intervene. J Natl Cancer Inst. 2015;108(5):djv370. doi:10.1093/jnci/djv370
- Jiao B, Hsieh YL, Li M, Verguet S. Value-based pricing for drugs with uncertain clinical benefits. Health Econ. Published online 2025. doi:10.1002/hec.4932
- Porter ME. What is value in health care? N Engl J Med. 2010;363(26):2477-2481. doi:10.1056/NEJMp1011024
- Thornton RLJ, Wilding KM, Gratale D, Walker KO. Alternative payment models and working with payers: key considerations for advancing population health goals and achieving child health equity. Pediatr Clin North Am. 2023;70(4):667-682. doi:10.1016/j.pcl.2023.04.008
- Patel KK. Can alternative payment models save primary care?: lessons from Hawaii for the nation. JAMA. 2019;322(1):35-36. doi:10.1001/jama.2019.6025
- Tranfield D, Denyer D, Smart P. Towards a methodology for developing evidence-informed management knowledge by means of systematic review. Br J Manag. 2003;14(3):207-222. doi:10.1111/1467-8551.00375
- van Haastrecht M, Sarhan I, Yigit Ozkan B, Brinkhuis M, Spruit M. SYMBALS: a systematic review methodology blending active learning and snowballing. Front Res Metr Anal. 2021;6:685591. doi:10.3389/frma.2021.685591
- Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
- Wohlin C. Guidelines for snowballing in systematic literature studies and a replication in software engineering. In: Proceedings of the 18th International Conference on Evaluation and Assessment in Software Engineering (EASE ’14). ACM; 2014:1-10. doi:10.1145/2601248.2601268
- Penchansky R, Thomas JW. The concept of access: definition and relationship to consumer satisfaction. Med Care. 1981;19(2):127-140. doi:10.1097/00005650-198102000-00001
- Johnston KJ, Wen H, Joynt Maddox KE. Lack of access to specialists associated with mortality and preventable hospitalizations of rural Medicare beneficiaries. Health Aff (Millwood). 2019;38(12):1993-2002. doi:10.1377/hlthaff.2019.00838
- Counts NZ, Smith JD, Crowley DM. (Expected) value-based payment: from total cost of care to net present value of care. Healthc (Amst). 2019;7(1):1-3. doi:10.1016/j.hjdsi.2018.10.001
- Sawar K, Sawar L, Chen K. Call for specialty-specific benchmarks for cross-specialty quality measures in the Quality Payment Program. Cureus. 2024;16(6):e61618. doi:10.7759/cureus.61618
- Nejati M, Razavi M, Harirchi I, Zendehdel K, Nejati P. The impact of provider payment reforms and associated care delivery models on cost and quality in cancer care: a systematic literature review. PLoS One. 2019;14(4):e0214382. doi:10.1371/journal.pone.0214382
- Howard SW, Bradford N, Belue R, et al. Building alternative payment models in health care. Front Health Serv. 2024;4:1235913. doi:10.3389/frhs.2024.1235913
- Abrahams E, Balch A, Goldsmith P, et al. Clinical pathways: recommendations for putting patients at the center of value-based care. Clin Cancer Res. 2017;23(16):4545-4549. doi:10.1158/1078-0432.CCR-17-1609
- Teisberg E, Wallace S, O’Hara S. Defining and implementing value-based health care: a strategic framework. Acad Med. 2020;95(5):682-685. doi:10.1097/ACM.0000000000003122
- Seymour EK, Loy B, Fontenot J. Incorporating value-based care into oncology. Cancer J. 2020;26(4):292-300. doi:10.1097/PPO.0000000000000455
- Bauder N, Cabrera Chien L. Enhancing mobility in oncology: evidence-based practices across the care continuum. Semin Oncol Nurs. 2024;40(4):151677. doi:10.1016/j.soncn.2024.151677
- Chung H, Hyatt A, Webber K, Kosmider S, Krishnasamy M. Value in care: the contribution of supportive care to value-based lung cancer services—a qualitative semistructured interview study. Health Expect. 2024;27(3):e14089. doi:10.1111/hex.14089
- Ouayogodé MH, Fraze T, Rich EC, Colla CH. Association of organizational factors and physician practices’ participation in alternative payment models. JAMA Netw Open. 2020;3(4):e202019. doi:10.1001/jamanetworkopen.2020.2019
- Miller BF, Ross KM, Davis MM, Melek SP, Kathol R, Gordon P. Payment reform in the patient-centered medical home: enabling and sustaining integrated behavioral health care. Am Psychol. 2017;72(1):55-68. doi:10.1037/a0040358
- Panchal A, Brendle K, Ilham N, et al. The implementation of value-based frameworks, clinical care pathways, and alternative payment models for cancer care in the United States. J Manag Care Spec Pharm. 2023;29(9):999-1008. doi:10.18553/jmcp.2023.29.9.999
- Frois C, Jarvis J, Grice K, et al. Drug treatment value in a changing oncology landscape: a literature and provider perspective. J Manag Care Spec Pharm. 2019;25(3):246-259. doi:10.18553/jmcp.2019.25.3.246
- Reitblat C, Bain PA, Porter ME, et al. Value-based healthcare in urology: a collaborative review. Eur Urol. 2021;79(5):572-585. doi:10.1016/j.eururo.2020.12.008
- Kaufman HL, Pai T, Nardi E, et al. Defining current gaps in quality measures for cancer immunotherapy: consensus report from the Society for Immunotherapy of Cancer (SITC) 2019 Quality Summit. J Immunother Cancer. 2020;8(1