






Evaluating P16, P53, and Ki-67 in Cervical Cancer
Comparative evaluation of P16, P53, and KI-67 expression in cervical intraepithelial neoplasia and invasive cervical carcinoma: a prospective histopathological and immunohistochemical study
Dr. Shikha Sachan MD (Pathology)1, Dr. Lubna Khan MD (Pathology)2*, Dr. Anjali Kumari3, Dr. Sunaina Singh3
- Senior Resident KGMU Lucknow
- Professor Department of Pathology, GSVM Medical College Kanpur
- Junior Resident, Department of Pathology, GSVM Medical College Kanpur
OPEN ACCESS
PUBLISHED 31 October 2025
CITATION Sachan, S., Khan, L., et al., 2025. Comparative evaluation of P16, P53, and KI-67 expression in cervical intraepithelial neoplasia and invasive cervical carcinoma: a prospective histopathological and immunohistochemical study. Medical Research Archives, [online] 13(10). https://doi.org/10.18103/mra.v13i10.6991
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i10.6991
ISSN 2375-1924
ABSTRACT
Introduction: Cervical cancer remains a leading cause of cancer-related mortality among women worldwide, particularly in developing countries. Persistent infection with high-risk human papillomavirus types, mainly 16 and 18, plays a pivotal role in the transformation from cervical intraepithelial neoplasia to invasive squamous cell carcinoma. Immunohistochemical markers including p16, p53, and Ki-67 are valuable in improving diagnostic precision and grading disease severity.
Objective: This study aimed to evaluate and compare the expression patterns of p16, p53, and Ki-67 in precancerous and malignant cervical lesions and to correlate these markers with histopathological grades.
Methods: A prospective observational study was carried out over fifteen months in a tertiary care hospital in northern India, analyzing one hundred cervical biopsy samples. Each specimen underwent hematoxylin and eosin staining and immunohistochemical testing for p16, p53, and Ki-67. Marker expression was scored according to staining intensity and distribution, and statistical associations were examined using chi-square tests and correlation analysis.
Results: A significant progressive increase in p16, p53, and Ki-67 expression was observed with higher grades of cervical lesions (p < 0.0001 for all). Ki-67 positivity rose from 5 percent in low-grade lesions to 57 percent in severe dysplasia, reflecting enhanced proliferative activity. p53 expression increased from 10 percent in mild dysplasia to 65 percent in severe lesions, indicating progressive alteration of tumor suppressor pathways. p16 expression rose from 12 percent in early lesions to 59 percent in advanced grades, consistent with oncogenic human papillomavirus integration.
Conclusion: Immunohistochemical evaluation of p16, p53, and Ki-67 provides a reliable adjunct for diagnosis and grading of cervical precancer and cancer. Their combined use enhances accuracy, supports early identification of high-risk cases, and guides individualized clinical management for better patient outcomes.
Keywords: Cervical cancer; cervical intraepithelial neoplasia; squamous cell carcinoma; p16; p53; Ki-67; immunohistochemistry.
Introduction
Cervical cancer represents a major global public health burden, ranking as the fourth most common cancer among women worldwide and a leading cause of mortality in low- and middle-income countries (LMICs)[1,2]. According to the World Health Organization (WHO), there were approximately 604,000 new cases and 342,000 deaths globally in 2020, with nearly 90% of these occurring in resource-constrained settings where screening and vaccination coverage remain suboptimal[2]. The global strategy to eliminate cervical cancer emphasizes HPV vaccination, early detection, and timely treatment as key interventions to achieve a target incidence rate below 4 per 100,000 women[2].
The etiopathogenesis of cervical cancer is intricately linked to persistent infection with high-risk human papillomavirus (HPV) types, particularly HPV-16 and HPV-18, which together account for over 70% of cases worldwide[3,4]. HPV infects the basal epithelial cells of the transformation zone of the cervix, and through integration of viral oncogenes E6 and E7, leads to the inactivation of tumor suppressor proteins p53 and retinoblastoma protein (pRb), respectively[5-7]. This results in loss of normal cell-cycle regulation, genomic instability, and progressive dysplasia that may culminate in invasive carcinoma if left untreated[7-9].
Cervical carcinogenesis is a multistep process, typically beginning with low-grade squamous intraepithelial lesions (LSIL/CIN1), progressing to high-grade lesions (HSIL/CIN2–CIN3), and ultimately to invasive squamous cell carcinoma (SCC)[10-12]. Although histopathological examination using hematoxylin and eosin (H&E) remains the diagnostic gold standard, morphological overlap between reactive atypia, metaplastic changes, and early neoplastic transformation can pose diagnostic challenges[10,13]. Hence, adjunctive immunohistochemical (IHC) biomarkers such as p16, p53, and Ki-67 have become invaluable tools for improving diagnostic accuracy and lesion stratification[8,14-16].
A cyclin-dependent kinase inhibitor, p16, is encoded by the CDKN2A gene and functions as a key regulator of the G1/S cell cycle checkpoint. Overexpression of p16 occurs as a compensatory response to HPV E7-mediated inactivation of pRb, resulting in uncontrolled cell proliferation[8,11,13]. Consequently, diffuse “block-positive” p16 staining is a hallmark of high-grade HPV-associated lesions and a reliable surrogate marker for oncogenic HPV activity[11-13,16].
A nuclear proliferation marker Ki-67 is expressed during all active phases of the cell cycle (G1, S, G2, and M), but absent in quiescent (G0) cells. Its expression correlates strongly with the grade of dysplasia and tumor aggressiveness[14,15]. A progressive increase in Ki-67 labeling index from CIN1 to CIN3 has been consistently reported, reflecting enhanced proliferative activity with advancing lesion severity[15,16].
The “guardian of the genome,” p53, plays a pivotal role in maintaining genomic stability by inducing cell-cycle arrest, DNA repair, or apoptosis following DNA damage[6,7]. In HPV-related lesions, the E6 oncoprotein mediates ubiquitin-dependent degradation of p53, leading to loss of its tumor-suppressive functions. In high-grade lesions and invasive carcinoma, however, p53 overexpression may be detected due to accumulation of mutant, dysfunctional protein[6,7].
The combined use of p16, p53, and Ki-67 provides complementary diagnostic and prognostic insights. Dual immunostaining for p16/Ki-67 enhances the sensitivity and specificity for detecting high-grade lesions, whereas p53 evaluation assists in differentiating HPV-dependent from HPV-independent neoplasia[17-19]. According to the Lower Anogenital Squamous Terminology (LAST) guidelines, p16 immunostaining is now recommended as an ancillary test in morphologically equivocal cases of CIN[19].
Given these considerations, the present study was designed to evaluate and compare the expression of p16, p53, and Ki-67 in cervical intraepithelial neoplasia (CIN) and invasive squamous cell carcinoma (SCC), and to explore their correlation with histological grades. Understanding these biomarker expression patterns can refine diagnostic precision, guide clinical management, and potentially identify lesions at higher risk of malignant transformation—thereby contributing to the broader goal of reducing cervical cancer burden through early and accurate detection. This study aims to evaluate the expression patterns of p16, p53, and Ki-67 in cervical biopsy specimens, correlate these patterns with the histological grades of CIN and invasive carcinoma, and explore their diagnostic and prognostic significance. The findings from this study may help enhance diagnostic accuracy, facilitate better risk stratification, and contribute to more effective clinical management strategies for cervical neoplasia.
Material and Methods
This prospective observational, non-randomized study was conducted from June 2023 to December 2024 at a tertiary centre in North India. The objective of the study was to assess and correlate the expression of p16, p53, and Ki-67 with the histological grades of cervical intraepithelial neoplasia (CIN) and invasive cervical carcinoma. A total of 100 women, aged ≥18 years, with confirmed cervical lesions, were enrolled following informed consent. Ethical approval was obtained, and the study adhered to the principles of the Declaration of Helsinki.
Inclusion criteria required participants to have confirmed CIN or squamous cell carcinoma (SCC) and suitable biopsy specimens. Exclusion criteria included prior treatment, recurrent or non-epithelial malignancies, and inadequate biopsy samples.
SAMPLE COLLECTION AND PROCESSING:
Cervical biopsy specimens were collected aseptically and fixed in 10% buffered formalin. The samples were processed, embedded in paraffin, and sectioned into 4–5 μm slices. Hematoxylin and eosin (H&E) staining was performed for histopathological grading according to WHO guidelines. For immunohistochemistry (IHC), unstained sections were mounted on poly-L-lysine slides and processed using the avidin-biotin complex method. Primary antibodies against p16, p53, and Ki-67 were applied, with appropriate controls. Expression of p16 was assessed for cytoplasmic/nuclear staining intensity and extent, Ki-67 for the percentage of nuclear positivity, and p53 for normal, reduced, or aberrant expression patterns. This comprehensive approach facilitated accurate histological and immunohistochemical characterization of the cervical lesions.
DATA COLLECTION AND STATISTICAL ANALYSIS:
Demographic details, clinical features, histopathological diagnoses, and IHC scores were systematically recorded using a structured proforma. The data were entered into Microsoft Excel, and statistical analysis was performed using IBM SPSS version 20. The Chi-square test was employed to assess associations between biomarker expression and histological grades. A p-value of <0.05 was considered statistically significant. Spearman’s rank correlation was used to determine the strength of association between biomarker expression and lesion severity. This methodology enabled a thorough and objective evaluation of biomarkers in the diagnosis and prognosis of cervical neoplasia.
Results
| CIN Grading | Ki-67 Positive Cases | p53 Positive Cases | p16 Positive Cases |
|---|---|---|---|
| CIN1 | 5% | 10% | 12% |
| CIN2 | 38% | 25% | 29% |
| CIN3 | 57% | 65% | 59% |
p- value p<0.0001 p<0.0001 p<0.0001
Table 1 presents the comparative evaluation of Ki-67, p53, and P16 expression across different grades of cervical intraepithelial neoplasia (CIN1, CIN2, and CIN3). The findings demonstrate a significant progressive increase in the proportion of positive cases for all three markers with advancing CIN grade. Ki-67 positivity increased from 5% in CIN1 to 57% in CIN3, indicating heightened cellular proliferation in higher-grade lesions. Similarly, p53 expression rose from 10% in CIN1 to 65% in CIN3, reflecting increased tumor suppressor pathway alterations in severe dysplasia. P16 positivity also showed a consistent upward trend, from 12% in CIN1 to 59% in CIN3, signifying its role in high-grade cervical lesions. All associations between marker expression and CIN grade were statistically significant (p < 0.001), underscoring their potential diagnostic and prognostic relevance in cervical pathology.
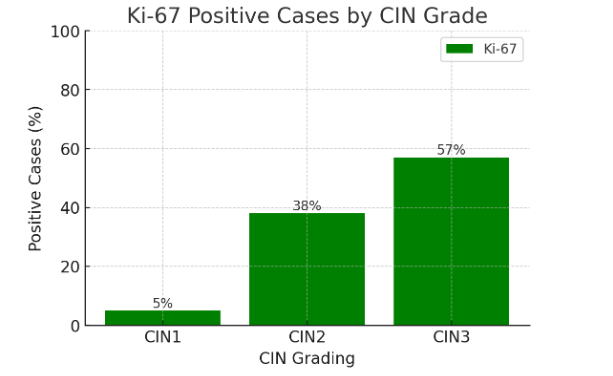
Figure 1 shows the percentage of Ki-67 positive cases across CIN grades (CIN1, CIN2, CIN3). Ki-67 expression increases markedly with CIN severity, from 5% in CIN1 to 57% in CIN3. Ki-67 is a well-established marker of cellular proliferation. The observed progressive increase reflects enhanced proliferative activity in higher-grade lesions, aiding in distinguishing low-grade from high-grade cervical neoplasia and predicting progression risk.
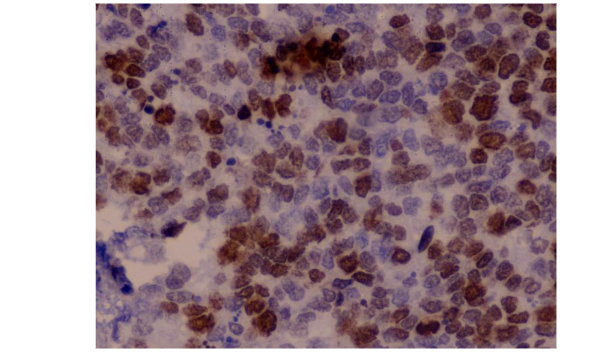
Figure 2 shows an immunohistochemical staining of cervical tissue, demonstrating strong nuclear positivity in numerous epithelial cells. The brown chromogen deposits indicate positive expression of the target biomarker Ki-67, while the background tissue is counterstained in blue with hematoxylin to visualize nuclei of negative cells. The distribution of staining is widespread, with high labeling density, consistent with a high-grade lesion showing marked proliferative or dysplastic activity.
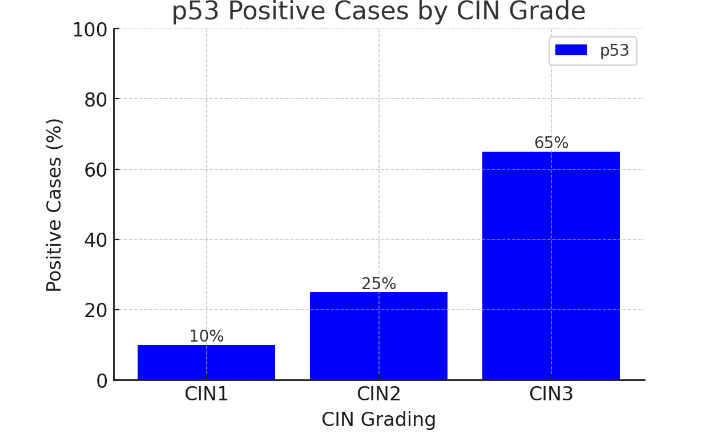
Figure 3 illustrates the percentage of p53 positive cases across CIN grades. p53 expression increases from 10% in CIN1 to 65% in CIN3, with a sharp rise in CIN3 lesions. p53 plays a key role in regulating cell cycle arrest and apoptosis. Overexpression in higher CIN grades suggests accumulation of genetic alterations and impaired tumor suppressor pathways, which can help identify lesions at higher risk for invasive transformation.
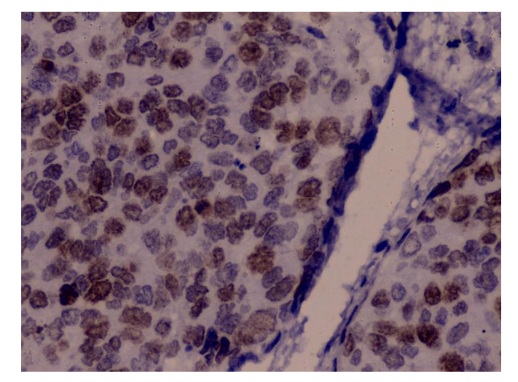
Figure 4 depicts an immunohistochemically stained section of cervical tissue showing diffuse nuclear positivity. Brown chromogen deposits within the nuclei indicate expression of p53 biomarker, while the blue counterstain (hematoxylin) highlights the nuclei of negative or unstained cells and background tissue architecture. The staining appears strong and widespread across the epithelial cell layers, suggesting high biomarker expression consistent with advanced dysplasia or high-grade cervical intraepithelial neoplasia.
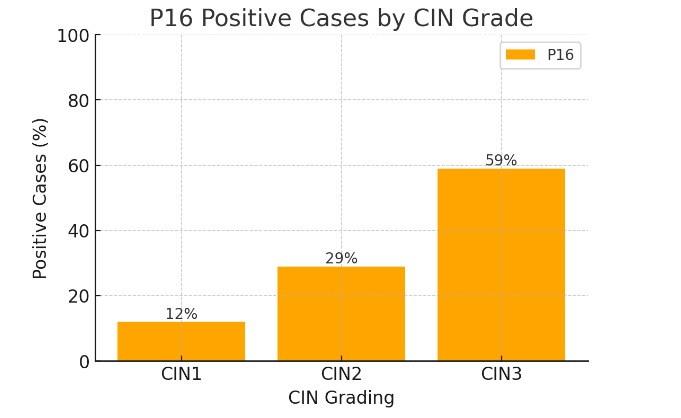
This bar chart shows the percentage of p16 positive cases across CIN grades, with positivity increasing from 12% in CIN1 to 59% in CIN3. P16 is a surrogate biomarker for oncogenic HPV activity. Its marked expression in higher-grade CIN reflects HPV-mediated disruption of cell cycle regulation, making it a valuable tool in identifying high-grade lesions and improving diagnostic accuracy.
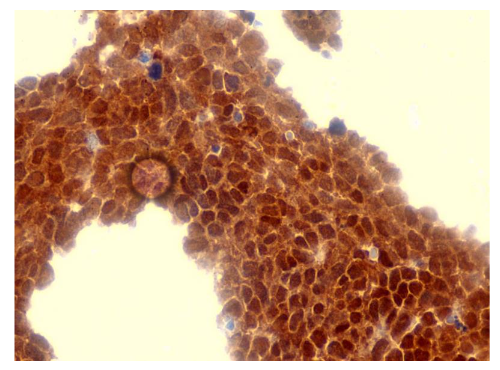
Figure 6 shows an immunohistochemically stained section of cervical epithelium demonstrating intense and diffuse nuclear and cytoplasmic brown staining throughout almost all epithelial cells, indicating strong positivity for p16. The staining pattern is continuous and block-like, extending across the full epithelial thickness, a characteristic feature associated with high-grade cervical intraepithelial neoplasia (CIN2/CIN3).
Discussion
Cervical cancer remains a major global health challenge, particularly in low- and middle-income countries (LMICs), where the implementation of effective screening programs and HPV vaccination remains insufficient. According to the World Health Organization (WHO)[1][2], this disparity contributes to higher incidence and mortality rates in these regions. Recent global epidemiological estimates by Arbyn et al.[20] further emphasize that more than 600,000 new cases and over 340,000 deaths occur annually, with the majority reported from resource-limited settings, underscoring persistent inequities in prevention and early detection. Persistent infection with high-risk human papillomavirus (HPV) types, especially HPV-16 and HPV-18, is well-established as the primary cause of cervical carcinogenesis. The pioneering work of zur Hausen[21] conclusively demonstrated the oncogenic role of HPV, laying the foundation for molecular understanding, biomarker development, and preventive vaccine strategies. The disease typically progresses through a defined sequence: initial HPV infection leads to cervical intraepithelial neoplasia (CIN), which can evolve into invasive carcinoma if left untreated[3].
The present study evaluated the expression patterns of Ki-67, p53, and p16 across various grades of cervical intraepithelial neoplasia (CIN) and demonstrated a statistically significant increase in the proportion of positive cases with advancing lesion severity. Among these markers, Ki-67 showed a progressive rise in positivity, from only 5% in CIN1 to 38% in CIN2 and reaching 57% in CIN3. This trend reflects the heightened proliferative activity that accompanies neoplastic progression, consistent with Ki-67’s established role as a nuclear protein expressed during active phases of the cell cycle (G1, S, G2, and M phases) but absent in quiescent (G0) cells. The increasing labelling index with higher CIN grade suggests that as lesions become more dysplastic, there is a greater proportion of cells engaged in active division, indicative of loss of normal cell cycle regulation. Our findings are in agreement with previous work[14], which demonstrated a strong correlation between Ki-67 expression and histological grade of cervical lesions, emphasizing its utility as an adjunctive marker for differentiating low-grade squamous intraepithelial lesions (LSIL) from high-grade squamous intraepithelial lesions (HSIL). Similarly, a study[15] reported significantly higher Ki-67 expression in CIN3 and invasive squamous cell carcinoma compared to CIN1 and CIN2, underscoring its prognostic significance. Comparable evidence has been reported by Kanthiya et al.[22], who showed that p16 and Ki-67 expression levels correlated directly with lesion severity, achieving sensitivities and specificities of 84.5% and 90.5% for p16 and 82.1% and 88.6% for Ki-67 in detecting CIN2+ lesions. Wentzensen et al.[24] validated these findings in a large multicentric cohort, showing that dual-stain p16/Ki-67 cytology offered superior sensitivity to Pap cytology for detecting CIN2+ while maintaining comparable specificity.
In our study, p53 expression increased steadily with CIN grade, from 10% in CIN1 to 25% in CIN2 and 65% in CIN3. This upward trend suggests that as cervical lesions progress, there is greater disruption of tumor suppressor pathways, likely due to genomic instability and mutation-associated protein accumulation. p53, often referred to as the “guardian of the genome,” plays a critical role in cell cycle arrest, DNA repair, and apoptosis in response to genomic damage. In HPV-associated neoplasia, the E6 oncoprotein typically targets p53 for proteasomal degradation, leading to reduced or absent protein levels. However, in high-grade lesions, p53 overexpression may occur due to mutations in the TP53 gene that result in a stable but dysfunctional protein. Our findings are consistent with available data from previous work[6], that found a similar pattern of increased p53 positivity in high-grade CIN and invasive carcinoma, and with reports[7], which showed a significant association between p53 expression and lesion severity. These results are further supported by Zhou et al.[24], whose meta-analysis demonstrated that p53 overexpression was associated with poorer overall survival (hazard ratio ≈ 1.67) in cervical cancer. Haensgen et al.[25] also highlighted that tumor hypoxia may favor selection of p53-defective clones, providing a mechanistic link between p53 aberration and aggressive tumor behavior.
In our series, p16 immunoexpression increased from 12% in CIN1 to 29% in CIN2 and 59% in CIN3, with high-grade lesions exhibiting intense, diffuse, block-type nuclear and cytoplasmic staining involving the full epithelial thickness. This pattern is characteristic of oncogenic HPV activity, in which the viral E7 oncoprotein inactivates the retinoblastoma protein (pRb), releasing E2F transcription factors and driving uncontrolled cell cycle progression. The resulting feedback leads to overexpression of p16, making it a sensitive surrogate marker for high-risk HPV infection. These results are in line with studies[11], which demonstrated that p16 overexpression is consistently present in HSIL and carcinoma, but absent or focal in low-grade lesions. A meta-analysis[12] confirmed that p16 immunostaining improves diagnostic accuracy, particularly in differentiating reactive atypia from true high-grade dysplasia. More recent studies[13,16] have highlighted the prognostic value of p16 in predicting the progression of low-grade lesions. Collectively, these international findings reinforce the combined diagnostic power of p16 and Ki-67 demonstrated in the present study, underscoring their clinical value for triaging HPV-positive women and guiding treatment decisions.
The combined evaluation of Ki-67, p53, and p16 enhances diagnostic accuracy. HSIL can be confirmed with Ki-67 and p16 together, while p53 may provide additional insight into tumor suppressor pathway disruption. Previous reports[18] demonstrated that dual immunostaining for p16 and Ki-67 significantly improves interobserver reproducibility in CIN diagnosis. The Lower Anogenital Squamous Terminology (LAST) guidelines[19] also recommend incorporating p16 into diagnostic algorithms for ambiguous cases. The highly significant p-values (<0.0001) for all three markers in our study underscore their strong association with CIN grade, supporting their inclusion in routine histopathological evaluation.
Overall, our findings corroborate existing literature and highlight the complementary diagnostic and prognostic utility of Ki-67, p53, and p16 in cervical pathology. Future studies with larger sample sizes and long-term follow-up could further clarify their predictive value for progression to invasive carcinoma and their role in tailoring patient surveillance and treatment strategies.
Conclusion
The present study demonstrates that Ki-67, p53, and p16 expression significantly increase with the histological severity of cervical intraepithelial neoplasia. Ki-67 reliably reflects proliferative activity, p53 indicates tumor suppressor pathway disruption, and p16 serves as a sensitive surrogate marker for high-risk HPV-mediated oncogenesis. When used together, these biomarkers substantially enhance diagnostic accuracy, facilitate differentiation between low- and high-grade lesions, and support prognostication. Incorporating their evaluation into routine histopathological practice can improve early detection, guide clinical decision-making, and potentially reduce progression to invasive carcinoma through timely intervention.
Conflict of Interest Statement: None.
Funding Statement: None.
Acknowledgements: None.
References:
- Vu M, Yu J, Awolude OA, Chuang L. Cervical cancer worldwide. Curr Probl Cancer. 2018; 42(5):457–465.
- World Health Organization. Global strategy to accelerate the elimination of cervical cancer as a public health problem. Geneva: WHO; 2020.
- Bosch FX, Lorincz A, Muñoz N, Meijer CJ, Shah KV. The causal relation between human papillomavirus and cervical cancer. J Clin Pathol. 2002;55(4):244–265.
- Castle PE, Maza M. Prophylactic HPV vaccination: past, present, and future. Epidemiol Infect. 2016;144(3):449–468.
- Yang X, Lu L. Expression of HPV-16 E6 protein and p53 inactivation increases cervical cancer invasion. Diagn Pathol. 2015;65(2):70–73.
- Sousa R, Carvalho L, Catarino R, Medeiros R. p53 expression in cervical intraepithelial neoplasia: correlation with lesion grade and HPV infection. Diagn Cytopathol. 2018;46(1):22–28.
- Shukla S, Mahata S, Shishodia G, et al. Aberrant expression of p53 in precancerous lesions of the uterine cervix: correlation with progression and HPV infection. Int J Gynecol Pathol. 2017;36(2):117–125.
- Luttmer R, Dijkstra MG, Snijders PJ, Berkhof J, van Kemenade FJ, Rozendaal L, et al. p16/Ki-67 dual-stained cytology for detecting cervical (pre)cancer in HPV-positive women. Mod Pathol. 2016;29(8):870–878.
- Mitra S, Shriwas D, Mondal M, Kamilya G, Manna AK. Role of Ki-67 and hormone receptors in cervical epithelial lesions. J Clin Diagn Res. 2025;19(2).
- Hunter K, Thavaraj S, Bal M. Diagnosis and histopathological reporting. In: Stell & Maran’s Textbook of Head and Neck Surgery and Oncology. 6th ed. 2024.
- Klaes R, Friedrich T, Spitkovsky D, et al. Overexpression of p16(INK4A) as a specific marker for dysplastic and neoplastic epithelial cells of the cervix uteri. Int J Cancer. 2001;92(2):276–284.
- Tsoumpou I, Arbyn M, Kyrgiou M, et al. p16(INK4a) immunostaining in cytological and histological specimens from the uterine cervix: a systematic review and meta-analysis. Cancer Treat Rev. 2009;35(3):210–220.
- Bergeron C, Ordi J, Schmidt D, et al. Conjunctive p16INK4a testing significantly increases accuracy in diagnosing high-grade CIN. Am J Clin Pathol. 2010;133(3):395–406.
- Keating JT, Cviko A, Riethdorf S, et al. Ki-67, cyclin E, and p16INK4 are complementary surrogate biomarkers for HPV-related cervical neoplasia. Am J Surg Pathol. 2001;25(7):884–891.
- Badr RE, Badria FA, Abdelfatah RM. Immunohistochemical expression of Ki-67 in premalignant and malignant cervical lesions. Egypt J Pathol. 2014;34(1):39–47.
- Negri G, Rigo A, Vittadello F, et al. p16INK4a expression and progression risk of low-grade squamous intraepithelial lesion: a 5-year follow-up study. Int J Gynecol Pathol. 2010;29(4):343–350.
- Gustinucci D, Rossi PG, Cesarini E, Broccolini M, Bulletti S, Carlani A, et al. Use of cytology, E6/E7 mRNA, and p16INK4a–Ki-67 to define the management of HPV-positive women. Cancer Cytopathol. 2016;145(1):35–45.
- Schmitt M, Dondog B, Waterboer T, Pawlita M. Homogeneous amplification of genital human alpha papillomaviruses by PCR using novel GP5+ and GP6+ primers. J Clin Microbiol. 2011;49(7):2625–2631.
- Darragh TM, Colgan TJ, Cox JT, et al. The Lower Anogenital Squamous Terminology (LAST) Project for HPV-associated lesions: background and consensus recommendations. Arch Pathol Lab Med. 2012;136(10):1266–1297.
- Arbyn M, Weiderpass E, Bruni L, de Sanjosé S, Saraiya M, Ferlay J, Bray F. Estimates of incidence and mortality of cervical cancer in 2018: a worldwide analysis. The Lancet Global Health. 2020 Feb 1;8(2):e191-203.
- Zur Hausen H. Papillomaviruses and cancer: from basic studies to clinical application. Nature reviews cancer. 2002 May 1;2(5):342-50.
- Kanthiya K, Khunnarong J, Tangjitgamol S, Puripat N, Tanvanich S. Expression of the p16 and Ki67 in cervical squamous intraepithelial lesions and cancer. Asian Pacific Journal of Cancer Prevention. 2016 Jul 1;17(7):3201-6.
- Wentzensen N, Fetterman B, Castle PE, Schiffman M, Wood SN, Stiemerling E, Tokugawa D, Bodelon C, Poitras N, Lorey T, Kinney W. p16/Ki-67 dual stain cytology for detection of cervical precancer in HPV-positive women. Journal of the National Cancer Institute. 2015 Dec 1;107(12):djv257.
- Zhou R, Wei C, Liu J, Luo Y, Tang W. The prognostic value of p53 expression for patients with cervical cancer: a meta analysis. Eur J Obstet Gynecol Reprod Biol. 2015 Dec;195:210-213.
- Haensgen G, Krause U, Becker A, Stadler P, Lautenschlaeger C, Wohlrab W, Rath FW, Molls M, Dunst J. Tumor hypoxia, p53, and prognosis in cervical cancers. Int J Radiat Oncol Biol Phys. 2001 Jul 15;50(4):865-72. doi: 10.1016/s0360-3016(01)01523-1. PMID: 11429213.