





Expert vs. AI in Interpreting Fetal Heart Monitoring
Agreement between an Expert in Physiological Interpretation of Cardiotocographs (CTG) and the Tweris Mini CTG
Mareva Gillon¹, Luka Velemir², Nemanja Kovacev³, Nikola Zivkovic⁴, Edwin Chandrahara⁵
- Hospital Centre of Antibes-Juan-Les-Pins
- Gynecology Institute of Nice, 5 rue Cronstadt 06000 Nice, France
- Polyclinic OrtoMD, Futoska 117, 21000 Novi Sad, Serbia
- Rubix’s Code, Berlin, Germany
- Global Academy of Medical Education and Training Ltd, London, UK.
OPEN ACCESS
PUBLISHED: 30 April 2025
CITATION: Gillon, M., et al., 2025. Agreement between an Expert in Physiological Interpretation of Cardiotocographs (CTG) and the Tweris Mini CTG Artificial Intelligence (AI) App in recognizing and managing different types of fetal hypoxic stress and abnormal CTG patterns. Medical Research Archives, (online) 13(4).
https://doi.org/10.18103/mra.v13i4.5684
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i4.5684
ISSN 2375-1924
ABSTRACT
Introduction:
Tweris Mini is a visual analysis Artificial Intelligence (AI) application designed to detect different types of fetal hypoxic stress, and common abnormal fetal heart rate patterns on Cardiotocograph (CTG) images. It is based on the classification system recommended by the International Expert Consensus Guidelines on Physiological Interpretation of Cardiotograph published by over 50 CTG experts from more than 20 countries.
Objective:
This study aims to evaluate the degree of agreement between the expert who pioneered the physiological interpretation of Cardiotocograph in 2006, and was on the editorial board of the international expert consensus guidelines, and the Tweris Mini App in classifying different types of fetal hypoxic stress and abnormal Cardiotocograph patterns, along with their proposed management.
Materials & Methods:
A total of 100 anonymized CTG traces were randomly selected, representing no hypoxia (NH) and various types of fetal hypoxic stress: chronic (C), gradually evolving compensated (GC), gradually evolving decompensated (GD), subacute (S), and acute (A). Specific abnormal CTG patterns, including atypical sinusoidal (AS), typical sinusoidal (TS), and Zigzag (ZZ) patterns. The expert classified the traces and provided the following management recommendations: continue labour (CO), induce stress (IS), or expedite birth (EB). Two independent obstetricians used the Tweris Mini App to classify the same CTG traces and the recommended management by the Tweris Mini AI App. The Cohen Kappa was used for statistical analysis to determine the level of agreement.
Results:
The overall degree of agreement between the Tweris Mini App and the expert was 94%, with complete (100%) agreement relating to acute hypoxic stress, Zigzag and atypical sinusoidal (Poole Shwartz test) patterns. The Cohen Kappa statistic for diagnostic agreement was 0.92 (95% CI: 0.83–0.99, p<.001). The agreement between the Tweris Mini App and the expert regarding the recommended management reached 98%. The Cohen Kappa statistic for management was 0.96 (95% CI: 0.94–0.98, p<.001).
Conclusion:
There was excellent agreement (>90%) between the Tweris Mini App and the expert, who pioneered Physiological Interpretation of CTG in both diagnosing different types of fetal hypoxic stress and recommending optimum management. Our findings suggest that Tweris AI Mini App has a high reliability to be used as a diagnosis & decision support tool in clinical practice.
Keywords: cardiotocograph (CTG); physiological CTG interpretation; artificial intelligence (AI); types of hypoxic stress; Tweris Mini App (TMA); Zigzag pattern.
Introduction
Cardiotocograph (CTG) is ubiquitously used in obstetric practice to recognise fetal heart rate changes in response to ongoing uterine contractions. If the features of decompensation of fetal central organs are timely recognised on the CTG trace, then, immediate and appropriate actions could be taken to reduce the stress and/or expedite birth to improve perinatal outcomes without increasing unnecessary intrapartum interventions such as emergency caesarean sections and operative vaginal births to the mother. In order to avoid hypoxic-ischaemic encephalopathy (HIE) and its long term sequelae such as cerebral palsy, learning difficulties and/or intrapartum-related perinatal deaths on one hand, and to avoid complications of unnecessary intrapartum operative interventions to the mother, accurate diagnosis of different types of fetal hypoxic stress and abnormal patterns that indicate an underlying pathology is crucial. Unlike other branches in clinical medicine where new technology is only introduced into clinical practice as routine standard of care following rigorous research, very unfortunately, CTG was directly introduced into clinical practice in 1960s without any prior robust scientific research or randomised controlled trials. Lack of sound scientific foundation and knowledge to differentiate features of fetal compensation from decompensation on the CTG trace, opened the doors to confusion, anxiety and over-reaction. The large void of knowledge of fetal physiology leading to iatrogenic anxiety due to the failure to conduct robust research prior to introducing technology was soon filled by the erroneous opinions CTG “experts” in advanced economies. Presumption of knowledge led to the features which were normal physiological cardioprotective reflex responses to reduce fetal myocardial workload (fetal heart rate decelerations), being illogically considered as “reassuring” or “non-reassuring” or abnormal based on the apparent morphology or arbitrarily predetermined time limits. These gross errors were perpetuated by several CTG guidelines, leading to an overall classification of CTG traces into “Normal, Suspicious, Pathological”¹².
False positive rate of traditional “Normal, Suspicious, Pathological” CTG Classifications
It is now well recognised by systematic reviews and metanalysis that randomly grouping different features of the fetal heart rate into pre-defined categories, due to lack of understanding of basic fetal pathophysiology has a high false positive rate of 98%³, which corroborates the findings of Karin Nelson et al, in 1996 who analysed >150,000 CTG traces and their resultant perinatal outcomes. They reported that, even in the presence of repetitive late decelerations and reduced baseline fetal heart rate variability, 99.8% of neonates were born with normal umbilical cord pH⁴. Therefore, contemporary scientific evidence suggests that performing unnecessary operative interventions due to “obstetrician’s distress” following the observation of “concerning” CTG patterns are totally unnecessary as these “concerning features” are not associated with neonatal metabolic acidosis in >99.8% of cases. This may explain the exponential increase in the rate of caesarean sections since the introduction of CTG into routine clinical practice in 1968 without any concomitant reduction in the rates of cerebral palsy or perinatal deaths⁷.
Fallacies of morphology of fetal heart rate (FHR) decelerations
National and International Guidelines which have been erroneously advising frontline midwives, obstetricians and nurses to illogically focus on the morphology of fetal heart rate decelerations, and to classify them into “early, variable, late, typical, atypical, complicated, uncomplicated, reassuring, non-reassuring” had failed to appreciate the inherent flaws of relying on pattern recognition. It should have been obvious to those who produced these guidelines that focusing on pattern recognition isolated FHR changes to classify CTG traces into “Normal, Suspicious, Pathological” without incorporating the knowledge of fetal pathophysiology, to differentiate features suggestive of compensatory stress response from the onset of decompensation, would lead to human errors in both classification and management resulting in poor maternal and neonatal outcomes.
Poor inter and intra-observer agreements with traditional (“Normal, Suspicious, Pathological”) Classification systems.
It is not surprising that several scientific publications have highlighted both inter and intra-observer disagreements in recognition of fetal heart rate changes, especially morphology of decelerations with the range of agreements between very poor to modest (Kappa 0.3–0.6)⁸–¹¹. It is obvious that if frontline clinicians do not agree on the observed patterns, this will lead to a different classification resulting in variation in their interventions and outcomes. It was erroneously presumed that the variation in outcomes and increasing unnecessary emergency caesarean sections were due to the lack of knowledge and skills of frontline clinicians in recognising CTG patterns. However, scientific evidence has illustrated that even the presumed “CTG experts” and those who had assumed themselves as “experts” in CTG interpretation, including those appeared as expert witnesses in courts to provide medico-legal opinions due to such presumed expertise on CTG interpretation experienced the same pitfalls of pattern recognition¹⁴–¹⁶. In fact, these presumed experts, changed their own CTG classification they had provided earlier, once the knowledge of neonatal outcomes were revealed to them¹⁶. This illustrates the simple fact that reliance on clinicians with presumed expertise on CTG interpretation without the knowledge of fetal pathophysiology but have the benefit of hindsight to provide medico-legal opinions, may lead to injustice to both the parents of the damaged or deceased children and frontline clinicians¹⁷–¹⁹.
It is not surprising that the effectiveness of electronic fetal heart rate monitoring has been recently questioned by some authors²⁰–²². However, it appears that many authors have failed to appreciate that the CTG technology per se has no problems, but its introduction into clinical practice without robust scientific evidence, and perpetuation of historical errors by some CTG Guidelines which focus on the morphology of fetal heart rate decelerations without incorporating the knowledge of fetal pathophysiology, is the underlying “root cause” of the perceived ineffectiveness of electronic fetal heart rate monitoring¹⁷–¹⁹.
Therefore, there is an urgent need to move away from focussing on the morphology of decelerations and on classifying individual CTG features in isolation, to avoid the flaws of pattern recognition to reduce the inter and intra-observer disagreements and the resultant variation in management.
Physiological Interpretation of CTG: a new concept in 2006, born out of a crisis
Physiological interpretation of CTG involves application of the knowledge of fetal pathophysiology whilst interpreting CTG traces and classifying CTG traces based on the features of suggestive of different types of hypoxic stress and recognising features of non-hypoxic causes of fetal compromise, and differentiating features of fetal compensation from decompensation²³–²⁵. This was in response to an intrapartum fetal monitoring crisis at a leading teaching hospital in London, UK where several babies had sustained hypoxic-ischaemic encephalopathy (HIE) due to the use of “normal, suspicious, pathological” classification system and resultant CTG misinterpretation²³. One of the authors (EC) was appointed as the labour ward lead consultant in 2005 following this iatrogenic intrapartum fiasco to help train the staff on the basics of CTG interpretation and to help improve perinatal outcomes²³. A subsequent publication by the team from this hospital had admitted that lack of knowledge and lack of training contributed 13 out of 14 babies who had sustained a severe hypoxic-ischaemic encephalopathy (HIE)²⁶–²⁷. Therefore, out of this crisis, the concept of physiological interpretation of CTG, was born in 2006 to prevent avoidable hypoxic-ischaemic encephalopathy (HIE) and its long term sequelae such as cerebral palsy and learning difficulties and perinatal deaths as well as to reduce unnecessary intrapartum operative interventions.
There have been several publications since its inception to confirm the proof of concept²⁸–³⁶. Hospitals which had implemented the concepts of physiological interpretation of CTG had shown approximately a 50% reduction in the rate of HIE and emergency caesarean sections after the introduction of physiological interpretation of CTG²⁴,³⁵,⁴⁶. More than 150 Physiological CTG Masterclasses were conducted in over 20 countries from 2006 to 2025 to disseminate knowledge and to prevent avoidable harm to mothers and babies. The first International Expert Consensus Guidelines on Physiological Interpretation of CTG was published in 2016⁴⁴, which was revised in 2024 in response to emerging scientific evidence⁴⁵.
Tweris CTG Mini App (AI): A decision and management Support Tool
There have been several attempts to incorporate artificial intelligence (AI) solutions in clinical medicine, especially in areas which involve pattern recognition such as radiology and histopathology. CTG interpretation also involves pattern recognition and therefore, teams from France, UK, Serbia and Germany collaborated to develop the Tweris CTG Mini App (named after Tweroues, a protective goddess of childbirth and fertility in Ancient Egyptian Religion). The aim was twofold: to protect the inherent intelligent potential of human fetuses from CTG misinterpretation and to protect their mothers from unnecessary intrapartum operative interventions due to overtreatment due to lack of knowledge (https://tweris.com/our-solution/).
Tweris Mini CTG AI App is based on the classification recommended by the latest international expert consensus statement on physiological interpretation of CTG⁴⁵, and the Tweris CTG AI Mini App (TMA) is being continuously upgraded based on submission of data from clinicians and several hospitals from in Europe, Asia, China, and the Middle East to continuously improve its accuracy. Recent publication has suggested a significant improvement in inter-observer agreement as compared to traditional classification systems⁴⁶.
Objective
Our objective was to evaluate the degree of agreement between the expert who pioneered the physiological interpretation of CTG in 2006, and was on the editorial board of the international expert consensus guidelines, and the Tweris Mini CTG AI App in classifying different types of fetal hypoxic stress and abnormal CTG patterns, along with their proposed management.
Materials & Methods
ALGORITHM DEVELOPMENT
The dataset comprises CTG photos classified by 2 experts in physiological CTG analysis into 9 different categories including no hypoxia (NH), various types of fetal hypoxic stress: chronic (C), gradually evolving compensated (GC), gradually evolving decompensated (GD), subacute (S), and acute (A), and specific abnormal CTG patterns, including atypical sinusoidal (AS), typical sinusoidal (TS), and ZigZag (ZZ) patterns.
The dataset contains a total of 5724 images, with 2061 images representing NH and 3663 images representing the other conditions.
To classify fetal heart rate (FHR) conditions based on Cardiotocography (CTG) images, we developed a Convolutional Recurrent Neural Network (CRNN) model designed to extract both deep and temporal features. The images were resized to 448×224 pixels, pre-processed through adaptive thresholding, background normalization, and standard augmentation techniques to enhance robustness. The model architecture integrates stacked convolutional layers with batch normalization and
max-pooling, followed by three bidirectional LSTM layers to capture sequential dependencies. A series of fully connected layers concludes the model, with softmax output for multi-class classification across nine FHR conditions. The model was trained using 5-fold cross-validation, with weighted categorical crossentropy loss to address class imbalance. Optimization was performed using the Adam optimizer (learning rate = 0.0001), and dropout regularization was applied to mitigate overfitting. Training was conducted on an NVIDIA GeForce RTX 2070 GPU using CUDA acceleration.
For each prediction made, the model provided a recommendation for appropriate clinical management, based on the International Expert Consensus Guidelines on Physiological CTG Interpretation.
A total of 100 anonymized CTG trace segments, each lasting 15 to 20 minutes, were randomly selected and compiled into a new set of images, distinct from those used to train the algorithm. The classification table recommended by the latest International Expert Consensus Guidelines on Physiological Interpretation of CTG produced by > 50 CTG Experts from > 20 countries in October 2024⁴⁵ was used in the study. The expert, who pioneered Physiological Interpretation of CTG in 2006 classified the traces using the above guideline and also provided the following management recommendations: continue labour (CO), reduce stress (RS), or expedite birth (EB). This expert was a member of the CTG guideline produced by the International Federation of Gynecology and Obstetrics (FIGO) in 2015, and International Expert Consensus Guidelines on Physiological Interpretation of CTG in 2018 and 2024. He was a course co-ordinator of the Intrapartum Fetal Surveillance Course of the Royal College of Obstetricians & Gynaecologists (RCOG) from 2014 to 2019, and he has conducted over 100 physiological CTG Masterclasses in over 20 countries. Moreover, he has authored four textbooks, and edited two textbooks on Physiological Interpretation of CTGs.
Two independent obstetricians (MG & NK) used the Tweris Mini CTG AI App to classify the same CTG traces and the recommended management by the Tweris Mini CTG AI App. The Cohen Kappa was used for statistical analysis to determine the level of agreement. Ethics approval was not required because this was a retrospective study with no patient identifiable data, and with no interventions.
Results
The overall degree of agreement between the Tweris Mini App and the expert was 94%, with complete (100%) agreement relating to acute hypoxic stress, ZigZag and atypical sinusoidal (Poole Shartz Tech) patterns. The agreement for the recognition of features of both chronic hypoxia and subacute hypoxia was 93%. One case, which was classified as chronic hypoxia by the expert was classified as decompensated gradually evolving hypoxia by the Tweris Mini App (Figure 1). There was 66% agreement for the classification of decompensated gradually evolving hypoxia, as the Tweris Mini CTG AI App classified one case as compensated gradually evolving hypoxia (Figure 2), and the second CTG classified as subacute hypoxia (Figure 3). The agreement for true sinusoidal pattern secondary to chronic fetal anaemia and acidosis was only 50%, as the Tweris Mini CTG AI App classified 50% of cases of typical sinusoidal patterns as chronic hypoxia. However, when it was re-tested on a segment of the CTG trace without ongoing shallow decelerations, Tweris Mini CTG AI App correctly identified the “Typical sinusoidal Pattern” (Figure 4). The Cohen Kappa statistic for diagnostic agreement was 0.92 (95% CI: 0.83–0.99, p<.001).
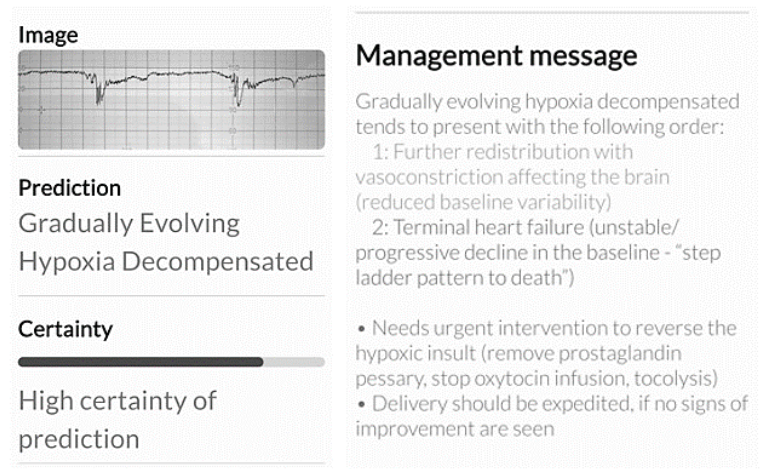
Figure 1.
CTG trace classified as “chronic hypoxia” by the expert, was classified as a “decompensated gradually evolving hypoxia” by the Tweris Mini CTG AI App. Note the management message is similar to the expert’s management plan.
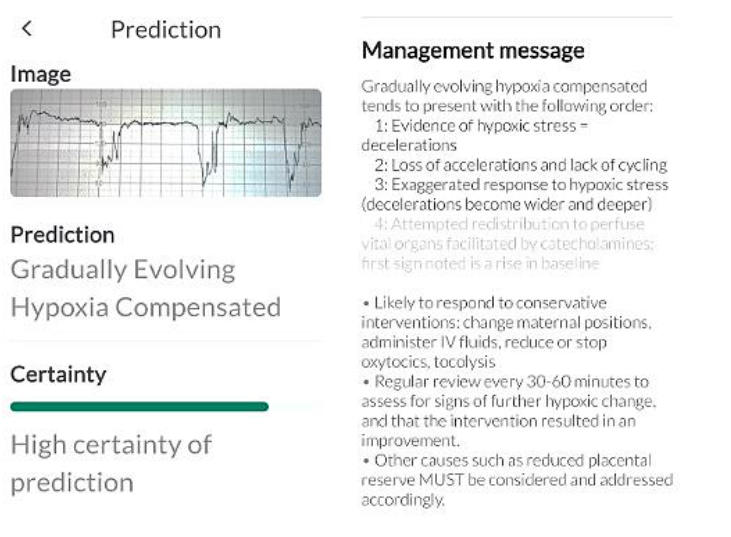
CTG trace which was classified as “decompensated gradually evolving hypoxia” by the expert was classified as “compensated gradually evolving hypoxia” by the Tweris Mini CTG AI App. However, the management message is to reduce the ongoing stress as that of the expert.
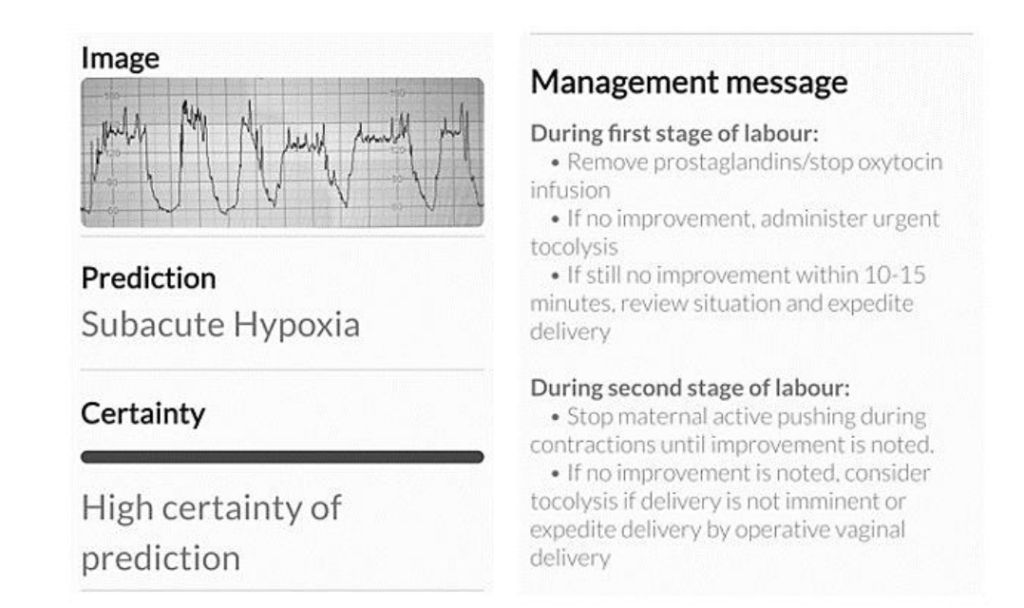
Figure 3.
CTG trace which shows a combination of features suggestive of gradually evolving hypoxia and subacute hypoxic stress. The Tweris Mini CTG AI App diagnosed this as “subacute hypoxia”. However, the management message was similar to the expert.
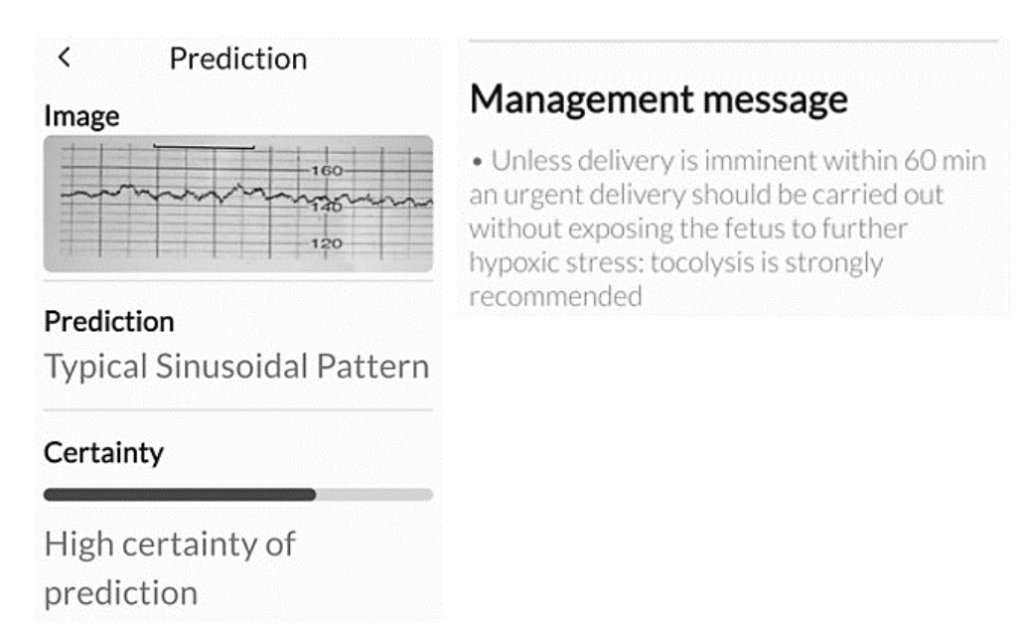
Figure 4.
CTG trace which was classified as “typical sinusoidal pattern” by the expert. This was initially classified as “chronic hypoxia” by the Tweris Mini CTG AI App, with similar management message. However, when the CTG segment devoid of shallow decelerations were presented, the Tweris Mini CTG AI App correctly classified it as “Typical Sinusoidal Pattern”.
The agreement between the Tweris Mini App and the expert regarding the recommended management reached 98%. The discrepancy was observed only in two cases where the Tweris Mini CTG AI App recommended “reduction of stress” instead of expediting birth, and to continue observation instead of reducing stress. The Cohen Kappa statistic for management was 0.96 (95% CI: 0.94–0.98, p<.001).
Discussion
To our best knowledge, this is the first study which analysed the diagnostic agreement and management plan between the expert who pioneered the concepts of physiological interpretation in their daily clinical practice, as well as the Tweris Mini CTG AI App (TMA), which has been exclusively trained on the principles of physiological interpretation of CTG.
Among the 6 cases of diagnostic disagreement, the TMA had under-classified 2 cases: one case as a decompensated gradually evolving hypoxia (GD) instead of chronic hypoxia (C), and another case as a compensated gradually evolving hypoxia (GC) instead of decompensated gradually evolving hypoxia (GD). The under-classification of chronic hypoxia (C) as decompensated gradually evolving hypoxia may have resulted in the reduction in stress instead of expediting birth. However, in the absence of improvement after reduction of stress (i.e., administration of tocolytics), delivery would have been accomplished, albeit approximately 30 minutes later. It is very likely that the TMA “under-classified” due to the recognition of ongoing shallow decelerations as “tardy” decelerations and increase in the baseline with reduced variability as compensated gradually evolving hypoxia.
In all other remaining cases of disagreement between the TMA and the expert (TMA diagnosing GD and S instead of GC, ZZ instead of S, C instead of TS, S instead of GD, and GD instead of C), the recommended management by the expert and the TMA would have remained the same. This includes expediting birth for cases of C or TS, and reduction of hypoxic stress for ZZ, S, and GD, followed by either continuation of labour if improvement occurred or expedited birth if there was no improvement. Therefore, the ultimate management plan would not have altered, resulting in consistent maternal and perinatal outcomes.
Our earlier study concluded that instead of grouping random features of fetal heart rate into different categories and focussing on morphology of decelerations, using a combination of features (chronic hypoxia, subacute hypoxia and chorioamnionitis or a sequence of features (gradually evolving hypoxia – compensated or decompensated) by the application of the knowledge of fetal pathophysiology significantly increased the inter-observer agreement between midwives and obstetricians²³. This study confirms that high level of agreements between the expert who pioneered the concept of physiological interpretation of CTG and the Tweris Mini CTG AI App could be achieved for both diagnosis and recommended management (94% and 98%, respectively), by programming the AI based on the principles of international expert consensus guidelines on physiological interpretation of CTG. Consistent diagnosis and appropriate management is likely to contribute to improvements in maternal and perinatal outcomes.
The strengths of the study include being the first in scientific literature which compared the performance of the Tweris Mini CTG AI App with the pioneer who developed the concepts of physiological interpretation of CTG. The CTG traces were randomly selected consisting of different types of fetal hypoxic stress and abnormal fetal heart rate patterns of clinical significance (Figure 5). Moreover, the traces were independently analysed by two obstetricians (MG and NK) using the TMA to ensure objectivity and to avoid any bias. We acknowledge that our study has some limitations. It is a retrospective study and therefore, it has all the drawbacks of retrospective studies. However, all the studies performed to assess inter-observer variability in CTG interpretations were retrospective. We included management decisions to further improve the clinical relevance of our study.
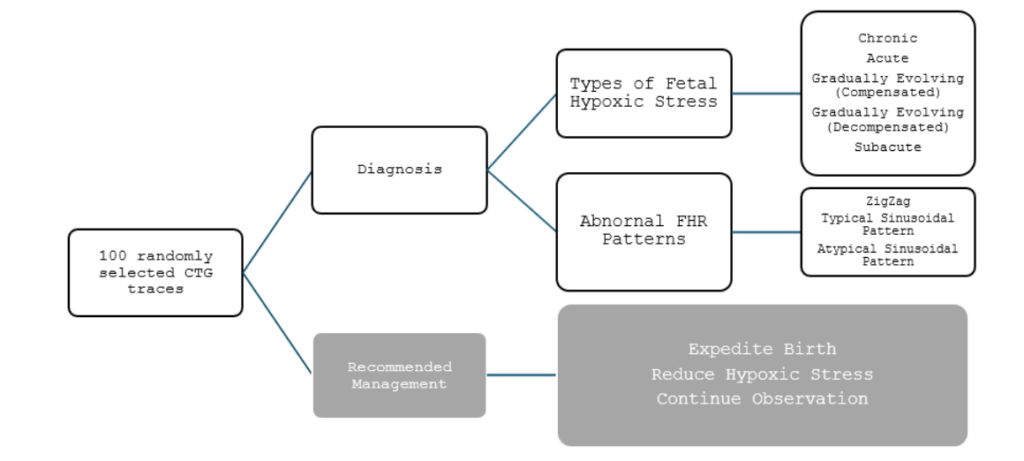
Figure 5.
Types of Hypoxic Stress and Abnormal Fetal Heart Rate (FHR) patterns and Recommended management presented to both the expert and the Tweris Mini CTG AI App.
Several studies have highlighted significant inter and intra-observer variability in the classification of CTG traces¹⁴–¹⁶. It has been reported from several countries which use “normal, suspicious, pathological” classification system that CTG misinterpretation has contributed to significant harm (severe hypoxic-ischaemic brain injuries and perinatal deaths) to babies in > 50% of cases⁷,⁸. More recently, four consecutive “Each Baby Counts” Reports have highlighted that CTG misinterpretation contributed to > 50% of all cases on severe hypoxic-ischaemic brain injuries as well as intrapartum stillbirths and early neonatal deaths in the UK⁷,⁸. The medico-legal costs relating to CTG misinterpretation alone, have been reported as £6.7 million/day in the United Kingdom by the NHS Resolution, which is a body which has been set up to indemnify the NHS against litigation²². Therefore, it is hoped that by significant eliminating significant inter and intra-observer variations reported with visual interpretation of CTG traces, the Tweris CTG AI App will reduce both human and financial costs of CTG Misinterpretation.
It may be argued that the use of computerised analysis of intrapartum cardiotocographs have been shown to be ineffective in improving perinatal outcomes or reducing emergency caesarean sections by randomised controlled trials. However, this argument is deeply flawed because both the INFANT Trial³⁹ and the FM-Alert Trial⁴⁰ were both based on illogical CTG guidelines which grouped random features into different categories (Normal, Suspicious, Pathological and Normal, Intermediate, Abnormal, respectively)³⁸. They did not include considering the principles of physiological interpretation of CTG and did not consider different types of hypoxic stress or fetal responses to stress. Moreover, both the INFANT Trial and FM-Alert Trial did not exclude pre-existing fetal compromise such as chronic hypoxia. Therefore, due to these inherent flaws from the outset, it was not surprising that the INFANT Trial and the FM-Alert Trial reported absence of any benefit with computerised analysis of intrapartum cardiotocographs.
In contrast, the Tweris Mini CTG AI App is based on the principles of physiological interpretation of CTG, and the algorithm is trained to recognise a combination of features (chronic hypoxia and subacute hypoxia) and sequence of changes (compensated or decompensated gradually evolving hypoxia). Moreover, the Tweris Mini CTG AI App has also been trained on recognising abnormal patterns such as the ZigZag and the Poole Shartz Teeth
Patterns. Therefore, the authors believe that by significantly eliminating significant inter and intra-observer variations reported with visual interpretation of CTG traces, and being based on the sound principles of physiological interpretation of CTG, the Tweris CTG AI App will help reduce both human and financial costs of CTG misinterpretation.
Conclusion
There was excellent agreement between the Tweris Mini App and the expert who pioneered the concepts of physiological interpretation of CTG in both diagnosing different types of fetal hypoxic stress and recommending labour management (Figure 6). This suggests that the Tweris Mini CTG AI App has a high reliability in clinical practice to function as both diagnostic and management support tool for frontline clinicians.
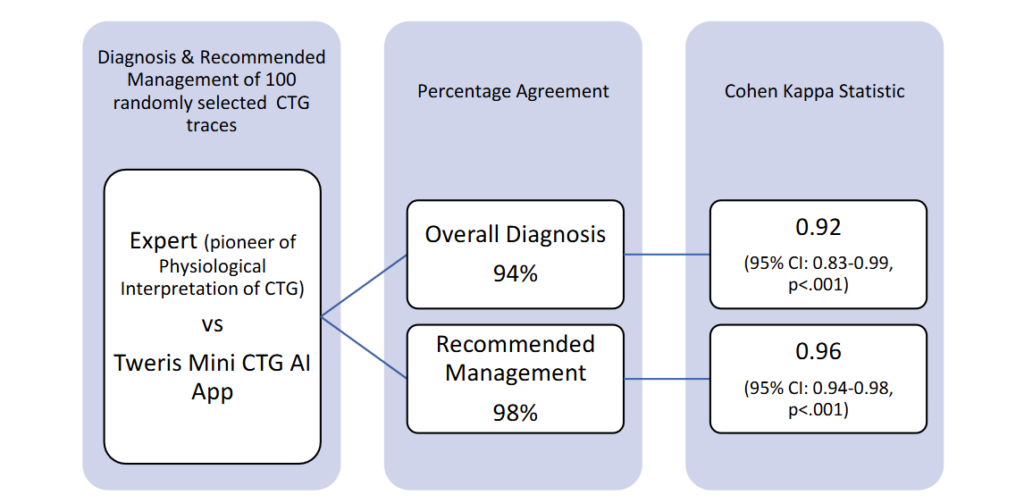
Figure 6 Diagnosis & Recommended Management of 100 randomly selected CTG traces
Contribution to Authorship
EC conceptualized the project, and LV and EC designed the study. EC classified the CTG traces. NK and MG independently analyzed the CTG traces using the Tweris Mini App. LV analyzed the data, and NZ was involved in the technical development of the Tweris Mini App. All authors contributed to the writing of the manuscript and reviewed and approved the final manuscript.
Conflict of Interest
EC is a member of the Editorial Board, and LV is a member of the International Expert Panel for the International Expert Consensus Statement on Physiological Interpretation of CTG. LV, EC and NK are the co-founders of the Tweris AI Project which is hosted and supported by Start-up Incubator Paca Est, France. Tweris Mini App has been currently made available free of charge in Apple and Android Stores for midwives and obstetricians with its aim to improve perinatal outcomes and to reduce unnecessary intrapartum operative interventions due to CTG misinterpretation.
(https://tweris.com/our-solution/)
References
2. Ayres-De-Campos D, Spong CY, Chandraharan E. FIGO Intrapartum Fetal Monitoring Expert Consensus Panel. FIGO consensus guidelines on intrapartum fetal monitoring: cardiotocography. Int J Gynaecol Obstet 2015;131:13–24.
3. American College of Obstetricians and Gynecologists ACOG practice bulletin No 106: intrapartum fetal heart rate monitoring: nomenclature, interpretation, and general management principles. Obstet Gynecol 2009;114:192-202.
4. Alfirevic Z, Devane D, Gyte GM, Cuthbert A. Continuous cardiotocography (CTG) as a form of electronic fetal monitoring (EFM) for fetal assessment during labour. Cochrane Database Syst Rev 2017; 2:CD006066.
5. Zullo F, Di Mascio D, Raghuraman N, Wagner S, Brunelli R, Giancotti A, Mendez-Figueroa H, Cahill AG, Gupta M, Berghella V, Blackwell SC, Chauhan SP. Three-tiered fetal heart rate interpretation system and adverse neonatal and maternal outcomes: a systematic review and meta-analysis. Am J Obstet Gynecol. 2023 Oct;229 (4):377-387.
6. Clark SL, Hankins GD. Temporal and demographic trends in cerebral palsy—fact and fiction. Am J Obstet Gynecol 2003;188:628-33.
7. Nelson KB, Dambrosia JM, Ting TY, Grether JK. Uncertain value of electronic fetal monitoring in predicting cerebral palsy. N Engl J Med 1996;334: 613-8.
8. Bernardes J, Costa-Pereira A, Ayres-de-Campos D, van Geijn HP, Pereira-Leite L. Evaluation of interobserver agreement of cardiotocograms. Int J Gynaecol Obstet 1997;57:33–7.
9. Blackwell SC, Grobman WA, Antoniewicz L, Hutchinson M, Gyamfi Bannerman C. Interobserver and intraobserver reliability of the NICHD 3-tier fetal heart rate interpretation system. Am J Obstet Gynecol 2011;205:378.e1–5.
10. Rei M, Tavares S, Pinto P, et al. Interobserver agreement in CTG interpretation using the 2015 FIGO guidelines for intrapartum fetal monitoring. Eur J Obstet Gynecol Reprod Biol 2016;205:27–31.
11. Beaulieu MD, Fabia J, Leduc B, et al. The reproducibility of intrapartum cardiotocogram assessments. Can Med Assoc J 1982;127: 214–6.
12. Santo S, Ayres-de-Campos D, Costa-Santos C, et al. Agreement and accuracy using the FIGO, ACOG and NICE cardiotocography interpretation guidelines. Acta Obstet Gynecol Scand 2017;96: 166–75.
13. Santo S, Ayres-de-Campos D. Human factors affecting the interpretation of fetal heart rate tracings: an update. Curr Opin Obstet Gynecol 2012;24:84–8.
14. Hruban L, Spilka J, Chudacek V, et al. Agreement on intrapartum cardiotocogram recordings between expert obstetricians. J Eval Clin Pract 2015; 21: 694–702.
15. Sabiani L, Le Dû R, Loundou A, et al. Intra- and interobserver agreement among obstetric experts in court regarding the review of abnormal fetal heart rate tracings and obstetrical management. Am J Obstet Gynecol 2015;213:856.e1-8.
16. Ayres-de-Campos D, Arteiro D, Costa-Santos C, Bernardes J. Knowledge of adverse neonatal outcome alters clinicians’ interpretation of the intrapartum cardiotocograph. BJOG 2011;118: 978-84.
17. Chandraharan E Intrapartum care: An urgent need to question historical practices and ‘non-evidence’-based, illogical foetal monitoring guidelines to avoid patient harm. Journal of Patient Safety and Risk Management. 2019; 24(5): 210-217.
18. Chandraharan E, Tahan ME, Pereira S. Each fetus matters: an urgent paradigm shift is needed to move away from the rigid “CTG Guideline Stickers” so as to individualize intrapartum fetal heart rate monitoring and to improve perinatal outcomes. Obstet Gynecol Int J 2016;5:00168.
19. Chandraharan E. Updated NICE Cardiotocograph (CTG) guideline: Is it suspicious or
pathological?. J Clin Med Surgery. 2023; 3(2): 1129.
20. Clark SL, Hamilton EF, Garite TJ, et al. The limits of electronic fetal heart rate monitoring in the prevention of neonatal metabolic acidemia. Am J Obstet Gynocol 2017; 216: 163.e1–163.e6.
21. Sartwelle TP, Johnston JC, Arda B, Zebenigus M. Cerebral palsy, cesarean sections, and electronic fetal monitoring: All the light we cannot see. Clinical Ethics. 2019;14(3):107-114.
22. Nelson KB, Sartwelle TP, Rouse DJ. Electronic fetal monitoring, cerebral palsy, and caesarean section: assumptions versus evidence. BMJ. 2016 Dec 1;355:i6405.
23. Chandraharan E. Physiological Interpretation of Cardiotocograph: Does the Emerging Scientific Evidence Suggest a Reversal in the “Thunder and Lightning” Phenomenon?. J Clin Med Surgery. 2023; 3(1): 1098.
24. Jia YJ, Ghi T, Pereira S, Gracia Perez-Bonfils A, Chandraharan E. Pathophysiological interpretation of fetal heart rate tracings in clinical practice. Am J Obstet Gynecol. 2023 Jun;228(6):622-644.
25. Chandraharan E. Handbook of CTG interpretation: from patterns to physiology. Cambridge, United Kingdom: Cambridge University Press; 2017.
26. Doria V, Papageorghiou AT, Gustafsson A, Ugwumadu A, Farrer K, Arulkumaran S. Review of the first 1502 cases of ECG-ST waveform analysis during labour in a teaching hospital. BJOG. 2007 Oct; 114(10): 1202-1207.
27. Chandraharan E. Fetal Electrocardiograph (ST-Analyser or STAN): Is it time for the Requiem?. J Clin Med Surgery. 2023; 3(2): 1111.
28. Chandraharan E, Arulkumaran S. Prevention of birth asphyxia: responding appropriately to cardiotocograph (CTG) traces. Best Pract Res Clin Obstet Gynaecol 2007;21:609–24.
29. Chandraharan E. Rational Approach to electronic fetal monitoring in all resource settings. SL J Obst & Gynaecol 2010; 32: 77-84
30. McDonnell S, Chandraharan E, The Pathophysiology of CTGs and Types of Intrapartum Hypoxia, Current Women`s Health Reviews 2013; 9(3).
31. Pinas A, Chandraharan E. Continuous cardiotocography during labour: analysis, classification and management. Best Pract Res Clin Obstet Gynaecol 2016;30:33–47.
32. Chandraharan E, Preti M, Lowe V, Archer A, Ugwumadu A, Arulkumaran S. Effectiveness of ‘George’s Intrapartum Monitoring Strategy’ on Operative Delivery and Perinatal Outcomes at a Teaching Hospital in London: a 5 Year Experience. Book of Abstracts. COGI Conference, Vienna, 2013.
33. Pereira S, Chandraharan E. Recognition of chronic hypoxia and pre-existing foetal injury on the cardiotocograph (CTG): urgent need to think beyond the guidelines. Porto Biomed J 2017;2: 124–9.
34. Oikonomou M, Chandraharan E. Fetal heart rate monitoring in labor: from pattern recognition to fetal physiology. Minerva Obstet Gynecol 2021; 73:19–33.
35. Griffiths K, Gupta N, Chandraharan E. Intrapartum fetal surveillance: a physiological approach,Obstetrics, Gynaecology & Reproductive Medicine, Volume 32, Issue 8, 2022,Pages 179-187.
36. Bolten M, Chandraharan E. The Significance of ‘Non-Significant’ Meconium Stained Amniotic Fluid (MSAF): Colour versus Contents. J Adv Med Med Res. 2019. doi:10.9734/jammr/2019/v30i530192
37. Physiological interpretation of CTG: From Knowledge to Practice. Volumes 1-3. Glob Acad Med Edu Train, London, UK. KDP. 2022 (https://www.amazon.co.uk/s?k=chandraharan&crid=1VKO4VCPZJ5IV&sprefix=chandraharan%2Caps%2C310&ref=nb_sb_noss_1)
38. Yanamandra N, Chandraharan E. Saltatory and sinusoidal fetal heart rate (FHR) patterns and significance of FHR ‘overshoots’. Curr Wom Health Rev. 2013;9:1e8
39. Al Fahdi B & Chandraharan E. True vs Spurious Intrapartum Fetal Heart Rate Accelerations on the Cardiotocograph (CTG): An Urgent Need for Caution. Glob J Reprod Med. 2020; 7 (5): 5556 722. DOI: 10.19080/GJORM.2019.07.555722.
40. Afors K, Chandraharan E. Use of continuous electronic fetal monitoring in a preterm fetus: clinical dilemmas and recommendations for practice. J Pregnancy. 2011;2011:848794.
41. Saeed F, Abeysuriya S, Chandraharan E. Erroneous Recording of Maternal Heart Rate as Fetal Heart Rate During Second Stage of Labour: Isn’t it Time to Stop this? J Biomed Res Environ Sci. 2021 May 11; 2(5): 315-319. doi: 10.37871/jbres1233.
42. Nurani R, Chandraharan E, Lowe V, Ugwumadu A, Arulkumaran S. Misidentification of maternal heart rate as fetal on cardiotocography during the second stage of labor: the role of the fetal electrocardiograph. Acta Obstet Gynecol Scand. 2012 Dec;91(12):1428-32. doi: 10.1111/j.1600-0412.2012.01511.x. Epub 2012 Sep 18.
43. Ingram C, Gupta N, Mustafa S, Singh M, Chandraharan E. Impact of Physiological CTG Guidelines on Intrapartum Hypoxic injuries and brain cooling. World Congress of the Royal College of Obstetricians and Gynaecologists (RCOG) 2021.
44. Jia YJ, Ghi T, Pereira S, Gracia Perez-Bonfils A, Chandraharan E. Pathophysiological interpretation of fetal heart rate tracings in clinical practice. Am J Obstet Gynecol. 2023 Jun;228(6): 622-644.
45. Reeves K, Scully R, Dutta A, Bullen-Bull R, Singh M, Chandraharan E. Training and support on Physiological CTG Interpretation: Does it reduce the hypoxic encephalopathy (HIE) rate? European Congress on Intrapartum Care. 2021.
46. Chandraharan E, Evans SA, Krueger D, Pereira S, Skivens S, et al. (2018) Physiological CTG interpretation. Intrapartum Fetal Monitoring Guideline. https://physiological-ctg.com/guideline.html.
47. Zamora Del Pozo C, Chóliz Ezquerro M, Mejía I, Díaz de Terán Martínez-Berganza E, Esteban LM, Rivero Alonso A, Castán Larraz B, Andeyro García M, Savirón Cornudella R. Diagnostic capacity and interobserver variability in FIGO, ACOG, NICE and Chandraharan cardiotocographic guidelines to predict neonatal acidemia. J Matern Fetal Neonatal Med. 2022 Dec;35(25):8498-8506.
48. Ghi T, Di Pasquo E, Dall’Asta A, et al. Intrapartum fetal heart rate between 150 and 160 bpm at or after 40 weeks and labor outcome. Acta Obstet Gynecol Scand 2021;100:548–54.
49. Preti M, Chandraharan E. Importance of fetal heart rate cycling during the interpretation of the cardiotocograph (CTG). Int J Gynecol Reprod Sci 2018;1:10–2.
50. Pereira S, Lau K, Modestini C, Wertheim D, Chandraharan E. Absence of fetal heart rate cycling on the intrapartum cardiotocograph (CTG) is associated with intrapartum pyrexia and lower Apgar scores. J Matern Fetal Neonatal Med. 2021 Jun 22:1-6.
51. Gracia-Perez-Bonfils A, Martinez-Perez O, Llurba E, Chandraharan E. Fetal heart rate changes on the cardiotocograph trace secondary to maternal COVID-19 infection. Eur J Obstet Gynecol Reprod Biol. 2020 Sep;252:286-293.
52. di Pasquo E, Commare A, Masturzo B, Paolucci S, Cromi A, Montersino B, Germano CM, Attini R, Perrone S, Pisani F, Dall’Asta A, Fieni S, Frusca T, Ghi T. Short-term morbidity and types of intrapartum hypoxia in the newborn with metabolic acidaemia: a retrospective cohort study. BJOG. 2022 Oct;129(11):1916-1925.
53. Descourvieres L, Ghesquiere L, Drumez E, Martin C, Sauvage A, Subtil D, Houfflin-Debarge V, Garabedian C. Types of intrapartum hypoxia in the newborn at term with metabolic acidemia: A retrospective study. Acta Obstet Gynecol Scand. 2022 Nov;101(11):1276-1281.
54. Yatham SS, Whelehan V, Archer A, Chandraharan E. Types of intrapartum hypoxia on the cardiotocograph (CTG): do they have any relationship with the type of brain injury in the MRI scan in term babies? J Obstet Gynaecol. 2020 Jul; 40(5):688-693.
55. Pereira S, Patel R, Zaima A, Tvarozkova K, Chisholm P, Kappelou O, Evanson J, Chandraharan E, Wertheim D, Shah DK. Physiological CTG categorization in types of hypoxia compared with MRI and neurodevelopmental outcome in infants with HIE. J Matern Fetal Neonatal Med. 2022 Dec; 35(25):9675-9683.
56. Chandraharan E. Physiological Interpretation of Cardiotocograph: Does the Emerging Scientific Evidence Suggest a Reversal in the “Thunder and Lightning” Phenomenon?. J Clin Med Surgery. 2023; 3(1): 1098.
57. Jia YJ, Chen X, Cui HY, Whelehan V, Archer A, Chandraharan E. Physiological CTG interpretation: the significance of baseline fetal heart rate changes after the onset of decelerations and associated perinatal outcomes. J Matern Fetal Neonatal Med. 2021 Jul;34(14):2349-2354.
58. Gracia-Perez-Bonfils A, Vigneswaran K, Cuadras D, Chandraharan E. Does the saltatory pattern on cardiotocograph (CTG) trace really exist? The ZigZag pattern as an alternative definition and its correlation with perinatal outcomes. J Matern Fetal Neonatal Med. 2019 Nov 13:1-9.
59. Galli L, Dall’Asta A, Whelehan V, Archer A, Chandraharan E. Intrapartum cardiotocography patterns observed in suspected clinical and subclinical chorioamnionitis in term fetuses. J Obstet Gynaecol Res. 2019 Dec;45(12):2343-2350. doi: 10.1111/jog.14133. Epub 2019 Oct 16.
60. Sukumaran S, Pereira V, Mallur S, Chandraharan E. Cardiotocograph (CTG) changes and maternal and neonatal outcomes in chorioamnionitis and/or funisitis confirmed on histopathology. Eur J Obstet Gynecol Reprod Biol. 2021 May;260:183-188. doi: 10.1016/j.ejogrb.20 21.03.029. Epub 2021 Mar 30.
61. di Pasquo E, Fieni S, Chandraharan E, Dall’Asta A, Morganelli G, Spinelli M, Bettinelli ML, Aloe R, Russo A, Galli L, Perrone S, Ghi T. Correlation between intrapartum CTG findings and interleukin-6 levels in the umbilical cord arterial blood: A prospective cohort study. Eur J Obstet Gynecol Reprod Biol. 2024 Mar;294:128-134.
62. Ghi T, Fieni S, Ramirez Zegarra R, Pereira S, Dall’Asta A, Chandraharan E. Relative uteroplacental insufficiency of labor. Acta Obstet Gynecol Scand. 2024 Oct;103(10):1910-1918.
63. Chandraharan E, Kahar Y, Pereira S, Fieni S, Ghi T. Rational approach to fetal heart rate monitoring and management during the second stage of labor. Eur J Obstet Gynecol Reprod Biol. 2025 Feb;305:159-169.
64. Chandraharan E, Evans SA, Krueger D, Pereira S, Skivens S, et al. (2018) Physiological CTG interpretation. Intrapartum Fetal Monitoring Guideline. https://physiological-ctg.com/guideline.html.
65. Chandraharan E, Pereira S, Ghi T, Gracia Perez-Bonfils A, Fieni S, Jia YJ, Griffiths K, Sukumaran S, Ingram C, Reeves K, Bolten M, Loser K, Carreras E, Suy A, Garcia-Ruiz I, Galli L, Zaima A. International expert consensus statement on physiological interpretation of cardiotocograph (CTG): First revision (2024). Eur J Obstet Gynecol Reprod Biol. 2024 Oct 2;302:346-355.
66. Chandraharan E, Griffiths K, Edmonsdon M, et al. Physiological interpretation of cardiotocograph (CTG): Inter-observer and “Observer-AI” agreements in recognising types of fetal hypoxic stress. Medical Research Archives, [S.l.], v. 12, n. 11, nov. 2024. ISSN 2375-1924.
67. Figueras F, Albela S, Bonino S, et al. Visual analysis of antepartum fetal heart rate tracings: inter- and intra-observer agreement and impact of knowledge of neonatal outcome. J Perinat Med 2005;33:241–5.
68. Reif P, Schott S, Boyon C, et al. Does knowledge of fetal outcome influence the interpretation of intrapartum cardiotocography and subsequent clinical management? A multicentre European study. BJOG 2016.
69. Zain HA, Wright JW, Parrish GE, Diehl SJ. Interpreting the fetal heart rate tracing. Effect of knowledge of neonatal outcome. J Reprod Med 1998;43:367–70.
70. Berglund S, Grunewald C, Pettersson H, Cnattingius S. Severe asphyxia due to delivery-related malpractice in Sweden 1990-2005. BJOG. 2008 Feb;115(3):316-23.
71. Jonsson M, Nordén SL, Hanson U. Analysis of malpractice claims with a focus on oxytocin use in labour. Acta Obstet Gynecol Scand. 2007;86(3): 315-9.
72. Andreasen S, Backe B, Øian P. Claims for compensation after alleged birth asphyxia: a nationwide study covering 15 years. Acta Obstet Gynecol Scand. 2014 Feb;93(2):152-8.
73. Evers AC, Brouwers HA, Nikkels PG, Boon J, VAN Egmond-Linden A, Groenendaal F, Hart C, Hillegersberg J, Snuif YS, Sterken-Hooisma S, Bisschop CN, Westerhuis ME, Bruinse HW, Kwee A. Substandard care in delivery-related asphyxia among term infants: prospective cohort study. Acta Obstet Gynecol Scand. 2013 Jan;92(1):85-93.
74. Anderson A. Ten years of maternity claims: an analysis of the NHS Litigation Authority data—key findings. Clin Risk 2013;19:24-31 10.1177/135 6262213486434.
75. Wise J. Litigation in maternity care is rising, says National Audit Office. BMJ 2013;347:f6737.
76. Donn SM, Chiswick ML, Fanaroff JM. Medico-legal implications of hypoxic-ischemic birth injury. Semin Fetal Neonatal Med 2014;19:317-21.
77. The Early Notification scheme progress report: collaboration and improved experience for families. NHS Resolution, September 2019. https://resolution.nhs.uk/wp-content/uploads/2019/09/NHS-Resolution-Early-Notification-report.pdf
78. Royal College of Obstetricans and Gynaecologists. Each baby Counts: key messages from 2015. London: RCOG. 2016. (https://www.rcog.org.uk/media/3fopwy41/each-baby-counts-2015-full-report.pdf).
79. Royal College of Obstetricians and Gynaecologists. Each Baby Counts: 2018 Progress Report. London: RCOG. 2018. (https://www.rcog.org.uk/media/dswjqyin/each-baby-counts-re¬port-2018-11-12.pdf).
80. Royal College of Obstetricians and Gynaecologists. Each Baby Counts: 2019 Progress Report. London: RCOG. 2020. (https://www.rcog.org.uk/media/qhzlelnc/each-baby-counts-2019-progress-report.pdf).
81. Royal College of Obstetricians and Gynaecologists. Each Baby Counts: 2020 Final Progress Report. London: RCOG. 2021.
82. NHS Resolution. Annual Report & Accounts 2023/24. Published on 23 July 2024.
https://resolution.nhs.uk/wp-content/uploads/2024/07/NHS-Resolution-Annual-report-and-accounts_23-24_Access.pdf
83. INFANT Collaborative Group. Computerised interpretation of fetal heart rate during labour (INFANT): a randomised controlled trial. Lancet 2017 Apr 29;389(10080):1719-29.
84. Nunes I, Ayres-de-Campos D, Ugwumadu A, et al. Fetal monitoring and alert (FM-ALERT) study group. Central fetal monitoring with and without computer analysis: A randomized controlled trial. Obstet Gynecol 2017 Jan;129(1):83-90.