






Fatigue and Injury Risks in Paramedics: Key Findings
Self-Reported Fatigue and Injury in Paramedics
Graham Marvin, DPhty1*, Robin Orr, PhD1, Elisa F.D. Canetti, PhD1, and Ben Schram, PhD1
1. Tactical Research Unit, Bond Institute of Health and Sport, Bond University, Robina, Queensland, Australia.
OPEN ACCESS
PUBLISHED: 30 June 2025
CITATION: Marvin, G., Orr, R., et al., 2025. Self-Reported Fatigue and Injury in Paramedics. Medical Research Archives, [online] 13(6). https://doi.org/10.18103/mra.v13i6.6669
COPYRIGHT © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i6.6669
ISSN 2375-1924
ABSTRACT
Introduction: The high rates of fatigue among paramedics, particularly cognitive and physical fatigue, necessitate research to understand its impact on performance and safety.
Aims: This study aimed to identify paramedics’ self-perceived demands of cognitive and physical tasks, along with fatigue and fatigue-related injuries within the profession.
Methods: An online cross-sectional survey was distributed to all paramedics within the Emergency Service Agency (ESA) of a state agency. The survey included questions on the most cognitively and physically demanding tasks and personal injuries. The Occupational Fatigue Exhaustion Recovery Scale (OFERS) was used to assess acute and chronic fatigue levels and intershift recovery.
Results: A total of 35 responses were collected, with 22 completed surveys utilised for data analysis. The most cognitively demanding tasks were reported to be clinical decision-making and patient care tasks while the most physically demanding tasks were manual handling and carrying the responder bag. Most respondents (73%) reported feeling cognitively and physically fatigued at the end of their shift, while all (100%) reported fatigue was still felt on their days off. Notably, nearly a third (32%) of respondents reported having suffered an injury within the last six months, with the majority of those reporting injuries (86.5%) stating that they believed fatigue contributed to their injuries. These subjective reports aligned with the OFERS results that indicated moderate/high levels of chronic fatigue, elevated acute fatigue, and low recovery levels between shifts.
Conclusion: This research highlights the significant levels of fatigue, both cognitive and physical among paramedics and the connection between fatigue and injury risk. Strategies to reduce fatigue, both cognitive and physical, and improve recovery must be developed for this population to minimise the harmful effects of fatigue on performance and its contribution to injury risk.
Keywords: paramedics, injury, fatigue, cognitive, physical
INTRODUCTION
Paramedics are known to have high rates of fatigue with contributions from many individual subtypes of fatigue. Of the several types of fatigue identified, cognitive and physical fatigue are reported to be the most common in paramedics. One reason these types of fatigue are prevalent in this population is the occupational demand of shift work, which causes poor sleep quality and sleep deprivation. Cognitive fatigue can manifest as near misses, such as dropping patients, careless driving, or treatment/procedure errors, stemming from problems sustaining attention. Meanwhile, physical fatigue typically arises as physical exhaustion, most commonly reported by the cumulative effect of physical activity during a night shift. When combined, cognitive and physical fatigue are thought to contribute to an elevated injury risk.
In Australia, the risk of injury within the paramedic population is higher than in many other professions, with injury rates higher than those of the general workforce. In part, this may be due to the physical demands of the occupation, as many injuries are reported during patient care tasks or other manual handling tasks such as lifting, carrying, or putting down objects. A proposed reason for this risk during these tasks is that a paramedic is primarily sought for their clinical skills, not their physical fitness, and research suggests that those with lower levels of physical fitness are more susceptible to injury. Furthermore, paramedics who rate their health as poor or fair are more likely to have poor recovery, with recovery being influenced by sleep quality, which directly contributes to fatigue. Mental or physical fatigue can lead to an increased risk of injury, error, and safety-compromising behaviours by 1.9, 2.2, and 3.6 times, respectively, compared to those who are not fatigued. In combination, data from two studies totalling 1288 paramedics found that 89-95% of paramedic reported safety-compromising behaviours in the last three months were due to fatigue. Additionally, a further 50-76% of those surveyed reported adverse events or medication errors within the previous three months due to fatigue. Finally, 80% of paramedics reported that they had suffered an injury that they deemed to be due to their fatigue levels. Evidently, fatigue is a major burden that can come at great cost to both the paramedics and the public they serve.
Understanding paramedics’ perceptions of cognitive and physical fatigue and their relationship to injury is an important first step in mitigating their deleterious effects. Once a greater understanding of occupational fatigue is developed, recommendations can be made to enhance paramedic safety. Therefore, this study aimed to identify paramedics’ self-perceived cognitive and physically demanding tasks, along with their perceptions of fatigue and fatigue-related injuries within the profession.
METHODS
An online, cross-sectional survey was distributed via email to all metro paramedic members of a state Emergency Services Agency (ESA). Online surveys are cost-effective and enable access to varied populations. The Qualtrics (Qualtrics, Provo, UT) platform was utilised for ease of statistical analysis and data security. During the survey’s development, piloting was conducted with the ESA management to ensure the questions’ appropriateness, the content’s comprehensiveness, and the lack of an excessive time burden. As time-effective measurements are essential in the occupational environment, the completion time was designed to be less than 10 minutes, which has been suggested as the maximum time for a survey. Early piloting amongst ESA management ensured that the survey was reliable and valid regarding face, content, internal, and external validity.
Inclusion criteria to participate in the survey were: a) participants were over 18 years of age, b) be working part- or full-time as paramedics, c) had at least six months of experience. The single exclusion criterion was individuals with a known sleep disorder (insomnia, sleep apnoea, narcolepsy) diagnosed by a registered medical provider, as this may have confounded the findings. The survey was open for two months to provide adequate time for participants to complete it.
At the front end of the survey, demographic information such as age, height, weight, and sex were collected along with other job characteristics, such as years in service and typical shift length. Body Mass Index (BMI) was calculated for each individual response and grouped according to BMI categories. Questions contained within the body of the survey revolved around the individual’s perception of their most physically and cognitively demanding occupational tasks and enquired about any current or previous recovery strategies they utilised as part of their routine. Further questions probed whether the participants had suffered a work-related injury and whether they believed that fatigue contributed to this injury. A free text narrative for some question was allowed to clarify or to add comments. In addition to the survey, the Occupational Fatigue Exhaustion Recovery Scale (OFERS) was added to the back end of the online survey. The OFERS has a moderate test-retest reliability with scores of 0.61, 0.64, and 0.62 for chronic fatigue (CF), acute fatigue (AF), and intershift recovery (IR), respectively. The OFERS has previously been validated in paramedics for CF, AF, and IR. The OFERS has 15 questions relating to acute and chronic fatigue along with intershift recovery which captures the construct of mental and physical fatigue rated on a 0 (strongly agree) to 6 (strongly disagree) Likert scale. Each section of the OFERS is out of 30 total points, with CF and AF of 30 points denoting the highest level of fatigue, while IR of 0 out of 30 denotes inability to recover. Although the OFERS was based on a 0-6 Likert scale, total scores were normalized between 0 and 100 by the formula [sum (scale scores)/(n items in scale x 6)] x 100. For comparative purposes, the quartiles distribution scale was used for cut-offs with low, low/moderate, moderate/high and high for each subscale based on the OFERS manual. Positive and negative statements were scored in all dimensions, with questions on intershift recovery being reversed-scored. A high score of acute and chronic fatigue, coupled with poor intershift recovery, can be warning signs the workplace is unsustainable. A sample of the survey can be found in Supplement A. Ethics approval for this project was granted by the University Human Research Committee, and gatekeeper approvals were provided by the Commissioner of the ESA.
STATISTICS
Qualitative data were analysed based on the overarching themes in the short answer responses. A thematic content analysis was created to identify themes and contend frequency of responses. Quantitative data arising from the OFERS was downloaded from Qualtrics and uploaded to the Statistical Package for the Social Sciences computer software (SPSS for Mac, Version 29.0). An ANOVA was used to explore differences in the OFERS subcategories scores (CF, AF, IR) between BMI groups (healthy, overweight, and obese).
RESULTS
A total of 35 responses were collected with 26 of these being completed in full. Four more were excluded after not being from the paramedic department, resulting in 22 completed surveys. Of the 22 completed surveys, 16 were female (72.7%), five were male (22.7%), while one person (4.6%) preferred not to say. Within the paramedic department, shift length was relatively consistent with 20 paramedics (91%) having an 11-15 hour shift regularly while another two (9%) had 7-10 hour shifts. Most respondents (n=9, 41%) had been employed as paramedics for 1-3 years, followed by more senior clinicians with greater than 10 years (n=5, 23%) experience. The remaining respondents had 3-5 (n=3, 13.5%), 5-7 (n=3, 13.5%), and 7-9 (n=2, 9%) years of service. A breakdown of the demographic information captured can be found in Table 1.
| Age (n) | Weight (n) | Height (n) | Body Mass Index (n) |
|---|---|---|---|
| 20-25 years (5) | <50kg (1) | <160cm (3) | Healthy weight 18.5-24.9 (12) |
| 26-30 years (4) | 50-60kg (5) | 161-170cm (6) | Overweight 25-29.5 (6) |
| 31-35 years (8) | 61-70kg (4) | 171-180cm (13) | Obese 30+ (4) |
| 36-40 years (1) | 71-80kg (3) | ||
| 41-45 years (1) | 81-90kg (6) | ||
| 46-50 years (1) | 91-100kg (2) | ||
| 51-55 years (2) | 101-110kg (1) |
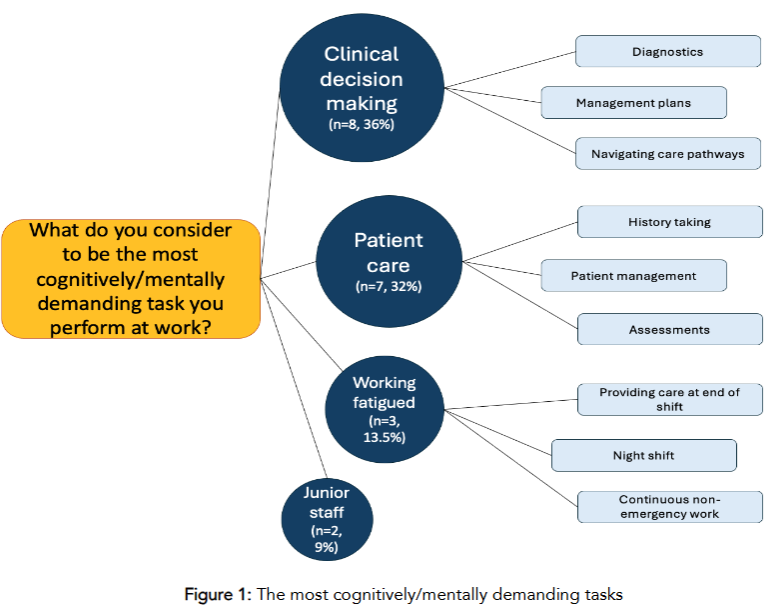
Qualitative answers were analysed to identify themes based on the overarching concepts that they reported. Within all free text narrative responses, multiple answers were identified. Of note, many respondents wrote multiple answers within all free-text narrative responses spanning multiple themes. For the question “what do you consider to be the most cognitively/mentally demanding task you perform at work?”, clinical decision-making was the most common response (n=8, 36%), with diagnostics, management plans, and navigating care pathways being most prevalent. Patient care (n=7, 32%) was the second most common response in relation to history taking, patient management, and assessments. Working under fatigue (n=3, 13.5%) was the third most common aspect, with difficulties in providing care at the end of a shift, night shift, and continuous non-emergency work. Interestingly, themes mentioned more than once were having to work with junior staff (n=2, 9%) and, difficulties with medication calculations (n=2, 9%).
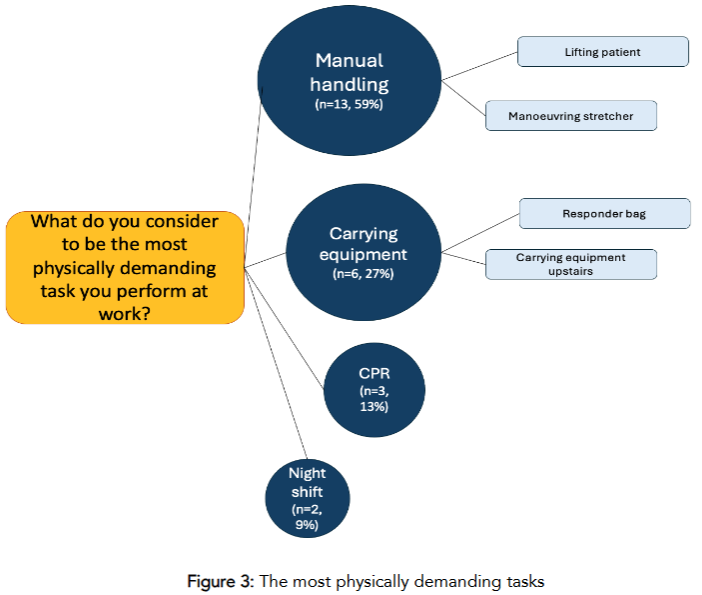
When asked “What do you consider to be the most physically demanding task you perform at work?” manual handling (n=13, 59%) was the most common response, with the main theme arising being patient lifting. The second most common response was carrying equipment (n=6, 27%), relaying concepts of generally carrying the heavily weighed responder bag for an extended period. Another physical challenge was performing cardiopulmonary resuscitation (CPR) (n=3, 13%). Lastly, a physically demanding topic mentioned on more than one occasion was ‘working the night shift’ (n=2, 9%).
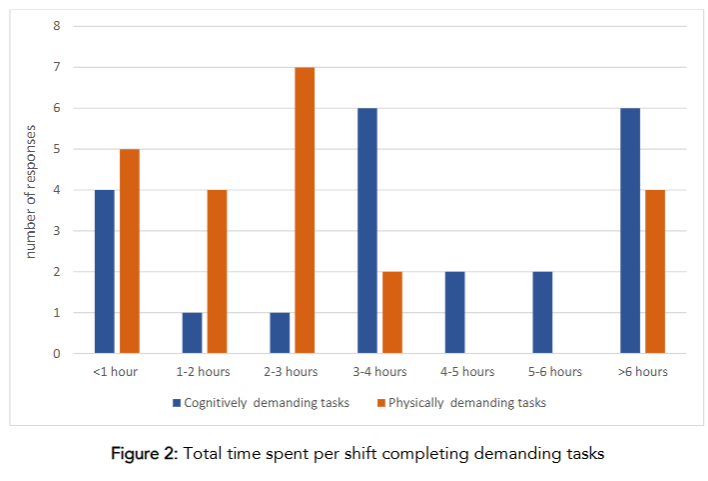
The cognitively demanding tasks were reported by 81% to be performed for 3-6 hours a day while the physically demanding tasks were reported (n=16, 72%) to be performed for 1-3 hours per day.
When paramedics were asked about how they felt after work (e.g., if they were cognitively fatigued, physically fatigued, or both), 73% stated feeling both cognitively and physically fatigued after work. Another 18% stated only feeling cognitively fatigued while 9% wrote in the other category. One respondent stated feeling “Emotionally and physically fatigued.” Another wrote “Depends on the shift. After yesterday’s 9-9 that turned into a 9-11 and we got no meal from 12 noon on, I was trashed and that has persisted through to my next shift.” Of the entire sample, 32% of respondents reported suffering an injury within the last six months, with each person stating that they reported the injury. When respondents were asked whether fatigue contributed to injury, 59% reported that they believed it ‘sometimes’ did, while another 23% stated ‘most of the time’, and 4.5% reported they believed it to be a contributing factor ‘every time’. Only 13.5% of respondents believed that fatigue was rarely the cause of an injury. Fatigue also featured as the most common reported risk factor for injury with 50% of respondents believing that to be the case.
The largest self-perceived subjective risk factor for injury while on duty was mostly stated as fatigue, with the second most being movement-related challenges. Themes of fatigue related to injury were inattention and feeling the pressure of the demands by the community with low staff numbers. Movement-related challenges were manual handling, fast and sudden movements, and time pressures with critical patients. The respondents conveyed that they believed that the effects of fatigue were not limited to their work, with all respondents reporting feeling fatigued during their days off. When rating this level of fatigue during days off, 45% reported that they ‘sometimes’ feel fatigued during their off days, while 36% stated ‘most of the time’ and 18% all the time. When the respondents were asked how this fatigue affects their ability to enjoy their day, three main themes were identified. The most common was a negative impact on leisure activities (n=7, 31%), such as not having energy for recreational activities or playing sports. This was followed by being fatigued on days off (n=5, 22%) and needing one to two days of rest before feeling recovered. All of these negatively affected relationships (n=5, 22%), with fatigue limiting patience for family and for feelings of not wanting to leave the house. The themes encapsulate the multifaceted impact of fatigue on personal well-being, social interactions, and the ability to engage in leisure activities.
When asked how they could reduce these feelings of fatigue, several themes emerged, with the most common being improvements of sleep and rest (n=8, 36%). Most suggestions included prioritising self-care, including sleep, resting before a night shift, and proper nutrition. Workload management (n=7, 31%) emerged as another recognised theme, suggesting working fewer hours and establishing stricter work/life boundaries. Several additional suggestions were noted; however, they focused on the workplace rather than the individual as per the question.
When asked how the workplace could assist in reducing fatigue levels, several suggestions were provided. Call appropriateness (n=7, 31%) emerged as a strong theme, focusing on avoiding dispatching crews to non-emergencies while handling low-priority jobs towards the end of the shift. Resource allocation (n=6, 27%) aimed to enhance both the total number and the quality of staff through improved training and education. Breaks and leave (n=5, 22%) appeared straightforward as the participants desired to have their annual leave approved and have their meal time breaks enforced. Another suggestion involved improving shift structures (n=4, 18%), which would allow for a reduction in shift length.
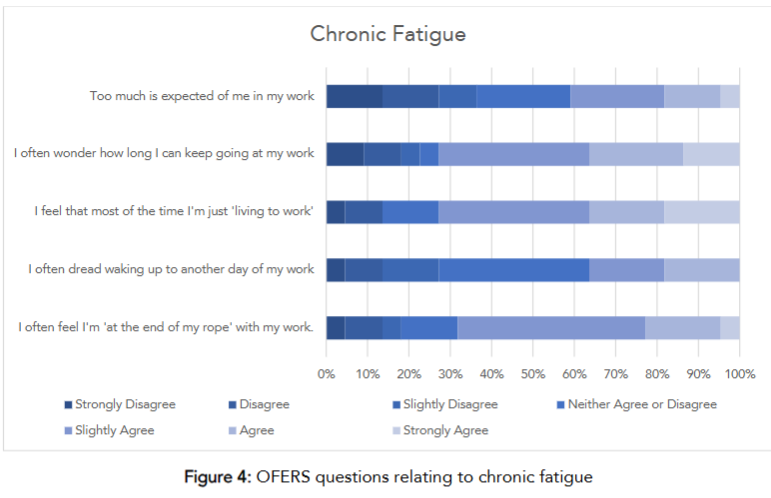
The fatigue survey captured ideas, feelings, and concerns related to fatigue within the occupation; however, the survey was purpose built and has not validated. As such, the OFERS was used to support the findings of the survey. The mean OFERS score for chronic fatigue (CF) was 57.6 ± 22 (Mean ± SD range; 15-100) out of 100 total points while acute fatigue scored 77 ± 18.3 (36.6-100) and intershift recovery 24.3 ± 18.3 (0-69).
Within the CF questions, 45% ‘slightly agreed’ that they often felt at the end of their rope with work. Meanwhile, 25% ‘agree’ that they wonder how long they can keep going at work. The breakdown of the CF section can be viewed in Figure 4.
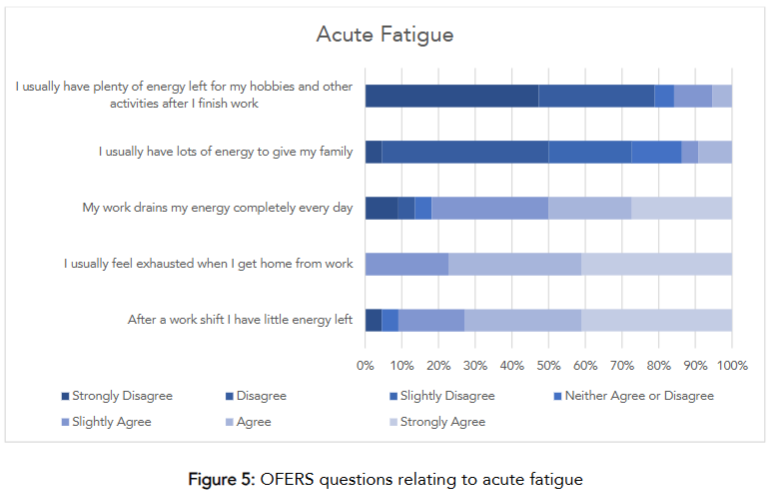
Within the AF questions, 48% of respondents ‘strongly disagree’ that they have energy left for hobbies after finishing work. Similarly, 45% ‘disagree’ that they have energy to give their families after work. The complete breakdown of AF section can be viewed in Figures 5.
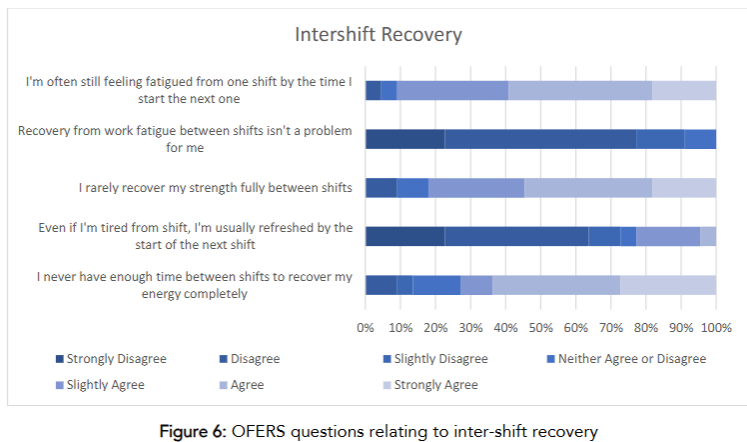
Regarding the IR questions, 50% ‘disagree’ that recovery from work fatigue isn’t a problem. Meanwhile, 40% ‘disagree’ that they are usually refreshed by the start of the next shift. The complete breakdown of IR section can be viewed in Figures 6.
There were no significant differences between BMI status and CF, AF, or IR. Table 2 presents a breakdown of the descriptive statistics.
| CF | AF | IR |
|---|---|---|
| Normal | Overweight | Obese |
| n= total people 12 6 4 | n= total people 12 6 4 | n= total people 12 6 4 |
| Mean 16.6 18 18.2 | Mean 22.6 24.6 22.5 | Mean 6.4 6.6 11 |
| Std. Deviation 7.7 2.5 8.1 | Std. Deviation 6.2 3.3 6.5 | Std. Deviation 5.5 5.1 5.7 |
| Minimum 5 15 7 | Minimum 11 20 14 | Minimum 0 0 6 |
| Maximum 30 21 26 | Maximum 29 29 30 | Maximum 21 15 19 |
DISCUSSION
The aim of this study was to identify paramedics’ self-perceived cognitive and physically demanding tasks, along with their perceptions of fatigue and fatigue-related injuries within the profession. The most cognitively demanding tasks for paramedics were clinical decision-making, patient care, and working under fatigue, typically occurring for 3-6 hours per shift. Meanwhile, the most physically demanding tasks were manual handling and carrying equipment, reported to be performed for 1-3 hours per shift. Regardless of the tasks being completed, 73% of the respondents experienced cognitive and physical fatigue after their shift and 86.5% believed that fatigue influenced previous injuries on some level. All respondents reported feeling fatigued once their shift cycle had finished, persisting into their days off, which negatively affected leisure activities and socialization. This was confirmed through the OFERS scores, which suggest that paramedics have a moderate to high amount of chronic fatigue, high levels of acute fatigue, and low levels of recovery between shifts.
Paramedics found clinical decision-making, patient care, and working under fatigue to be the most cognitively demanding tasks. To make sound clinical decisions, gathering as much information as possible while filtering out irrelevant information is needed. The higher the task complexity, the higher the cognitive load, which can be linked to poorer performance, particularly under fatigue. Paramedics report that fatigue is exacerbated by having to continuously respond to non-emergency calls; deemed highly demanding and frustrating.
Engaging in cognitively demanding tasks for over 3-6 hours a day can be a concern since cognitive fatigue will impair tasks requiring sustained attention in paramedics. Unfortunately, many paramedics are regularly fatigued, placing them at increased risk of safety-compromising behaviours with patients and themselves.
The most physically demanding task found in this study were manual handling, carrying equipment, and performing CPR. The findings align with recent research which found stretcher manipulation to be the most physically demanding task for paramedics. While manipulating a large stretcher can contribute to physical fatigue, so too can carrying the general vital equipment paramedics rely on, such as an airway bag, a vital signs monitor/defibrillator, a medication bag, and oxygen tank, which can weigh 3.4kg, 6.5kg, 9.3kg, and 3.2kg, respectively. Equipment carriage alone has been attributed to 28% of injuries in Australian paramedics. In addition to equipment-related physical demands, performing CPR can be considered vigorous activity measured at 6 metabolic equivalents, the same as jogging or bicycling at 10 miles per hour. This is of concern as these physically demanding tasks were performed for 1-3 hours a day. Given the prolonged exposure to these physically demanding tasks, and the high levels of fatigue reported in this study, the associated increase in risk of injury in this population is understandable. The findings align with previous studies whereby paramedics who are fatigued are at increased risk of injury and safety-compromising behaviours which may be due to paramedics having low fitness levels. Those who are less fit, fatigue at a lower relative working intensity, increasing the risk of injury more rapidly, and highlighting the need for fitness promotion strategies within this population.
Interestingly, 32% of paramedics reported sustaining an injury within the last six months. Recent research has shown that paramedics sustain injuries at a rate of up to 333.8 per 1,000 full time equivalent (FTE), with a lost time to injury of 93 per 1,000 FTE per year. Although most respondents did not report an injury within the last six months, 86.5% reported that they believed fatigue influenced an injury at some stage of their career. Other research investigations have highlighted the association between fatigue and injury risk in paramedics, with greater self-reported fatigue leading to greater injury risk.
The connection between fatigue is not only evident within the workplace but extends beyond it, influencing paramedics’ personal lives. Every respondent reported that their fatigue extended into their days off. Fatigue can affect the ability to enjoy the day off by limiting leisure activities and contributing to social isolation which may be why paramedics report higher levels of anxiety and depression than in the general population. The latent effect of fatigue has been reported to be a barrier to exercise in paramedics, contributing to decreased willpower and lack of energy. Within the present study, some suggested ways to combat fatigue such as prioritising self-care and increasing sleep. These suggests are in line with current research whereby paramedics that sleep less are purported to have increased fatigue and stress levels. Some other suggestions within the population were trying to work less or having stricter work/life boundaries as the profession’s nature can strain family relationships. However, no specific suggestions were given as to how this could be achieved.
Improving the workplace environment may help reduce fatigue by improving the training and education of the staff. The suggestion likely stems from some paramedics feeling ill-equipped to perform their normal duties based on their existing workloads and feeling overwhelmed. Another suggestion was to stop patient transfers after midnight and only respond to emergency calls after 0200. Stopping paramedics from heavy lifting late at night may be a helpful strategy. In Australia, during a five year span of 7,591 injuries, 36% of the injuries happened from 2000-0800, while 21% were reported during the first night shift with fatigue being a major contributor.
The OFERS scores encapsulate the responses from the open-ended answers, where paramedics described feeling overworked and under-recovered. The present study showed moderate/high, high, and low levels of chronic fatigue, acute fatigue, and intershift recovery, respectively. Research using the OFERS to assess fatigue in shift workers has surveyed nurses, and identified similar scores for chronic fatigue, acute fatigue, and inter-shift recovery. Patterson et al., surveyed paramedics, who reported low/moderate, moderate, and low/moderate levels of chronic fatigue, acute fatigue, and intershift recovery, lower levels than those reported in the present study. A potential reason for the difference may lie in the type of emergency medical services used within Patterson et al., with the authors using a variety of ground based, air based, intensive care unit, and emergency department staff used. Meanwhile, all respondents within this current study were ground-based.
LIMITATIONS
A primary limitation of this study is the small sample size, which makes generalizing to paramedics at large difficult. However, a larger sample is unlikely to change the results, as the findings are consistent with the literature. Another limitation can be the use of subjective outcome measures of recounted past events which may contribute to recall bias.
CONCLUSIONS
The present study emphasises the significant cognitive and physical demands placed on paramedics and the connection between fatigue, diminished recovery, and injury risk. Furthermore, fatigue is associated with previous injuries and should be considered as a factor when reporting an injury. Additionally, the fatigue experienced extends beyond the workplace, adversely affecting leisure and social interactions during off days. Agencies should seek feedback from their paramedics regarding how they feel best to optimise workplace conditions and reduce the negative impact of fatigue. Strategies aimed at mitigating fatigue and enhancing recovery must be developed for this population to minimise detrimental effects on performance and to help reduce injury risk.
CONFLICT OF INTERESTS
The present study was funded by an Australian state ESA as part of the lead author’s PhD, but they were not involved in the study design, questions, or writing process. No other conflicts of interest are noted.
REFERENCES
- Donnelly EA, Bradford P, Davis M, Hedges C, Socha D, Morassutti P, Pichika SC. What influences safety in paramedicine? Understanding the impact of stress and fatigue on safety outcomes. Journal of the American College of Emergency Physicians Open. Aug 2020;1(4):460-473. doi:10.1002/emp2.12123
- Lin MH, Huang YC, Chen WK, Wang JY. Sleepiness and injury risk in emergency medical service workers in Taiwan. PLoS One. 2020;15(2):e0229202. doi:10.1371/journal.pone.0229202
- Patterson PD, Weaver MD, Frank RC, et al. Association between poor sleep, fatigue, and safety outcomes in emergency medical services providers. Prehosp Emerg Care. 2012;16(1):86-97. doi:10.3109/10903127.2011.616261
- Donnelly EA, Bradford P, Davis M, Hedges C, Socha D, Morassutti P. Fatigue and Safety in Paramedicine. Article. Canadian Journal of Emergency Medicine. 2019;21(6):762-765. doi:10.1017/cem.2019.380
- Marvin G, Schram B, Orr R, Canetti FDE. Types and Contributors to Occupational Fatigue. Strength & Conditioning Journal. 2024;46(4):500-509.
- Patterson PD, Suffoletto BP, Kupas DF, Weaver MD, Hostler D. Sleep quality and fatigue among prehospital providers. Prehosp Emerg Care. Apr-Jun 2010;14(2):187-93. doi:10.3109/10903120903524971
- Paterson JL, Sofianopoulos S, Williams B. What paramedics think about when they think about fatigue: Contributing factors. Emerg Med Australas. 2014;26(2):139-144. doi:10.1111/1742-6723.12216
- Sofianopoulos S, Williams B, Archer F, Thompson B. The exploration of physical fatigue, sleep and depression in paramedics: a pilot study. Journal of Emergency Primary Health Care. 2011;9(1):1-33.
- Toyokuni Y, Ishimaru T, Honno K, Kubo T, Matsuda S, Fujino Y. Near-miss incidents owing to fatigue and irregular lifestyles in ambulance personnel. Arch Environ Occup Health. 2022;77(1):46-50. doi:10.1080/19338244.2020.1842312
- Suminska S, Nowak K, Lukomska B, Cygan HB. Cognitive functions of shift workers: paramedics and firefighters – an electroencephalography study. Int J Occup Saf Ergon. Sep 2021;27(3):686-697. doi:10.1080/10803548.2020.1773117
- Khan WAA, Jackson ML, Kennedy GA, Conduit R. A field investigation of the relationship between rotating shifts, sleep, mental health and physical activity of Australian paramedics. Article. Sci Rep. 2021;11(1):866. doi:10.1038/s41598-020-79093-5
- Marvin G, Schram B, Orr R, Canetti EFD. Occupation-Induced Fatigue and Impacts on Emergency First Responders: A Systematic Review. Int J Environ Res Public Health. 2023;20(7055) doi:10.3390/ijerph20227055
- Reichard AA, Marsh SM, Tonozzi TR, Konda S, Gormley MA. Occupational Injuries and Exposures among Emergency Medical Services Workers. Prehosp Emerg Care. 2017;21(4):420-431. doi:10.1080/10903127.2016.1274350
- Kearney J, Muir C, Smith K. Occupational injury among paramedics: a systematic review. Inj Prev. Apr 2022;28(2):175-184. doi:10.1136/injuryprev-2021-044405
- Lošonczi P. HJ. Analysis Of Occupational Risks In The Profession Of A Paramedic. Annals of Burns and Fire Disasters. 2022;38(1)
- Maguire BJ, O’Meara PF, Brightwell RF, O’Neill BJ, Fitzgerald GJ. Occupational injury risk among Australian paramedics: an analysis of national data. Med J Aust. May 5 2014;200(8):477-80. doi:10.5694/mja13.10941
- Bentley MA, Levine R. A National Assessment of the Health and Safety of Emergency Medical Services Professionals. Prehosp Disaster Med. Dec 2016;31(S1):S96-S104. doi:10.1017/S1049023X16001102
- Patterson PD, Buysse DJ, Weaver MD, Callaway CW, Yealy DM. Recovery between Work Shifts among Emergency Medical Services Clinicians. Prehosp Emerg Care. Jul-Sep 2015;19(3):365-75. doi:10.3109/10903127.2014.995847
- Regmi PR WE, Paudyal A, Simkhada P, van Teijlingen E. Guide to the design and application of online questionnaire surveys. Nepal Journal of Epidemiology. 2016;6(4):640-644.
- Revilla M, Ochoa C. Ideal and maximum length for a web survey. International Journal of Market Research. 2017;59(5)doi:10.2501/IJMR-2017-039
- Ball HL. Conducting Online Surveys. J Hum Lact. 2019;35(3):413-417.
- Control CfD. Adult BMI Categories. 2025. https://www.cdc.gov/bmi/adult-calculator/bmi-categories.html
- Winwood PC, Lushington K, Winefield AH. Further development and validation of the Occupational Fatigue Exhaustion Recovery (OFER) scale. J Occup Environ Med. Apr 2006;48(4):381-9. doi:10.1097/01.jom.0000194164.14081.06
- Winwood PC, Winefield AH, Dawson D, Lushington K. Development and validation of a scale to measure work-related fatigue and recovery: the Occupational Fatigue Exhaustion/Recovery Scale (OFER). J Occup Environ Med. Jun 2005;47(6):594-606. doi:10.1097/01.jom.0000161740.71049.c4
- Moosavian Hiaq SS, Jabbarzadeh Tabrizi F, Parvan K, Sarbakhsh P, Dickens G. Relationship between burnout and occupational fatigue exhaustion and recovery among orthopaedic nurses in Tabriz, Iran: a cross-sectional survey. BMJ Open. Aug 25 2024;14(8):e084522. doi:10.1136/bmjopen-2024-084522
- Rahman HA, Naing L, Abdul-Mumin K. Validation Of The Occupational Fatigue Exhaustion Recovery (Ofer) Scale Among Emergency Nurses In A Brunei Public Hospital. The Malaysian Journal of Nursing. 2017;8(3)
- Perona M, Rahman MA, O’Meara P. Paramedic Judgement, Decision-Making and Cognitive Processing: A Review of the Literature. Australasian Journal of Paramedicine. 2019;16:1-12. doi:10.33151/ajp.16.586
- Zaphir JS, Murphy KA, MacQuarrie AJ, Stainer MJ. Understanding The Role of Cognitive Load In Paramedical Contexts: A Systematic Review. Prehosp Emerg Care. Jun 26 2024:1-23. doi:10.1080/10903127.2024.2370491
- Ericsson CR, Lindstrom V, Rudman A, Nordquist H. Paramedics’ perceptions of job demands and resources in Finnish emergency medical services: a qualitative study. BMC Health Serv Res. Dec 2 2022;22(1):1469. doi:10.1186/s12913-022-08856-9
- Fischer SL, Sinden KE, MacPhee RS, Ottawa Paramedic Service Research T. Identifying the critical physical demanding tasks of paramedic work: Towards the development of a physical employment standard. Appl Ergon. Nov 2017;65:233-239. doi:10.1016/j.apergo.2017.06.021
- Harari Y, Riemer R, Jaffe E, Wacht O, Bitan Y. Paramedic equipment bags: How their position during out-of-hospital cardiopulmonary resuscitation (CPR) affect paramedic ergonomics and performance. Appl Ergon. Jan 2020;82:102977. doi:10.1016/j.apergo.2019.102977
- Kearney J, Muir C, Smith K. Factors Associated with Lost Time Injury among Paramedics in Victoria, Australia. Prehosp Emerg Care. 2024;28(2):297-307. doi:10.1080/10903127.2023.2168095
- Kwak SJ, Kim YM, Baek HJ, Kim SH, Yim HW. Chest compression quality, exercise intensity, and energy expenditure during cardiopulmonary resuscitation using compression-to-ventilation ratios of 15:1 or 30:2 or chest compression only: a randomized, crossover manikin study. Clin Exp Emerg Med. Sep 2016;3(3):148-157. doi:10.15441/ceem.15.105
- Ainsworth BE, et al. Compendium of physical activities: classification of energy costs of human physical activities. Med Sci Sports Exerc. 1993;25:71-80.
- Sheridan S. Paramedic health status, fitness and physical tasks: A review of the literature. Australasian Journal of Paramedicine. 2019;16 doi:10.33151/ajp.16.580
- Kirby K. The Impact of Working Shifts: Exploring the Views of UK Paramedics. Journal Of Paramedic Practice. 2016;8(5)
- Khan WAA, Conduit R, Kennedy GA, Jackson ML. The relationship between shift-work, sleep, and mental health among paramedics in Australia. Article. Sleep Health. 2020;6(3):330-337. doi:10.1016/j.sleh.2019.12.002
- Supples MW, Rivard MK, Cash RE, Chrzan K, Panchal AR, McGinnis HD. Barriers to Physical Activity Among Emergency Medical Services Professionals. J Phys Act Health. Mar 1 2021;18(3):304-309. doi:10.1123/jpah.2020-0305
- Australian Capital Territory Government. About us. https://esa.act.gov.au/about-us#:~:text=The%20ESA%20comprises%20the%20ACT,emergency%20management%20in%20the%20ACT%22.
- Althubaiti A. Information bias in health research: definition, pitfalls, and adjustment methods. J Multidiscip Healthc. 2016;9:211-7. doi:10.2147/JMDH.S104807