

Fostering Civil Discourse in Academic Medicine
Fostering Civil Discourse and Collaboration in Academic Medicine: A Comprehensive Intervention Approach
Jessica Bunin, MD, MHPE ¹; Ryan Landoll, PhD ¹; Jeanmarie Rey, MD ¹; Lisa Harris, DO ¹; Gayle Haischer-Rollo, MD ¹
- Uniformed Services University, 4301 Jones Bridge Road, Bethesda MD, 20814
OPEN ACCESS
PUBLISHED: 31 August 2025
CITATION: Bunin, J., Landoll, R., et al., 2025. Fostering Civil Discourse and Collaboration in Academic Medicine: A Comprehensive Intervention Approach. Medical Research Archives, [online] 13(8). https://doi.org/10.18103/mra.v13i8.6893
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i8.6893
ISSN 2375-1924
Abstract
Introduction: Rising global political polarization and distrust are impacting academic medicine. Intensified by events like COVID-19 and social unrest, these factors are leading to incivility, communication breakdowns, and compromised patient care. Restorative practice and civil discourse offer potential solutions by emphasizing community building and communication. This article describes a novel faculty development curriculum integrating Restorative Practice and civil discourse to enhance communication and conflict resolution.
Methods: We developed “Community Building for Civil Discourse,” a curriculum designed as a series of full-day, off-campus faculty development retreats. These retreats blended restorative practice principles with civil discourse models, aiming to enhance communication skills and foster connections among staff and faculty. We used pre- and post-surveys to assess knowledge acquisition, retreat effectiveness, and sense of belonging/hope, supplemented by qualitative data on experiences and challenges.
Results: Two hundred ninety-four interprofessional individuals participated, demonstrating broad engagement. Post-retreat, 81% reported increased understanding of both reflective practice and civil discourse, 72.3% felt confident in applying community building skills, and 64% were confident in conducting civil discourse. Notably, 54% reported a high increase in belonging, and 74.9% expressed high levels of hope for the institution’s future. An overwhelming 88% deemed the retreat an effective use of time.
Conclusion: The challenges of polarization in academic medicine necessitate proactive interventions. Our findings emphasize the value of integrating Tier 1 Restorative Practice and civil discourse in fostering dialogue and belonging. This faculty development curriculum provides an evidence-based foundation for navigating contemporary academic complexities, enabling institutions to prevent harm, foster healing, and cultivate a more collaborative environment.
Keywords
Restorative Practice, Civil Discourse, Academic Medicine, Faculty Development, Communication Skills
Introduction
Political polarization and erosion of trust are increasing globally and academic medicine is not immune. These challenges in conjunction with the isolating effects of COVID-19, racial violence, and political unrest threaten the foundation of mutual respect and collaboration in medical education. This has resulted in incivility and a decrease in effective communication and collaboration, an increase in verbal abuse and harassment, and a decrease in the quality of patient care. Recent articles exploring the experiences during COVID-19 surrounding issues such as vaccination reveal that civil discourse was replaced by identity attacks, insults, profanity, threats, and severe toxicity. The resulting deep divide, especially among scientists and clinicians, underscores the need for proactive interventions within academic institutions. The practice of civil discourse is lacking and offers a potential solution to the current atmosphere. Civil discourse necessitates a foundation of mindfulness, active listening, critical thinking, open communication, and psychological safety. It involves respecting others’ identities and beliefs while seeking common ground and listening beyond preconceptions. Civil discourse is not possible, however, in the absence of strong relationships and a strong community. To build community and to address this deep divide in academia, calls to action have arisen to explore ways of resolving conflicts and mending harms within the academic community. One such paradigm shift in conflict resolution is the application of restorative practice in academic settings.
Restorative practice is a social science focused on strengthening and repairing relationships within communities. Its core purpose is to build healthy social connections, resolve conflicts, and address harm. The principles, which originated from indigenous communities, prioritize healing and reconciliation over punishment. In academic medicine, a field that thrives on collaboration and innovation, restorative practice offers a promising frame that is proactive and reactive. For instance, Tier one proactive practices, such as community-building circles, can foster interpersonal skills and mutual understanding. Tier two practices, which are used reactively to respond to conflict and harm are centered around restorative conferences. Finally, Tier 3 practices, including circles of support and accountability, help navigate challenging reintegration processes. By adopting restorative practice principles, most notably building and strengthening relationships (Tier 1), academic institutions can transform conflicts into opportunities for growth and understanding. Capitalizing on the strong foundation of community building allows for the tenets of civil discourse to be utilized to address disagreements among student groups, faculty members, and interdisciplinary teams. Moreover, when weaving together restorative practice and civil discourse we can put into practice the core values of academic medicine, such as collaboration, empathy, and social responsibility.
This article aims to describe a novel staff and faculty development curriculum utilizing both restorative practice and civil discourse to improve communication and conflict resolution within an institution. We hypothesized that this curriculum would increase a sense of belonging, confidence in communicating across differences and hopefulness regarding the future of the institution.
Methods
We developed a curriculum centered around a series of monthly faculty and staff retreats under the banner of “Community Building for Civil Discourse” (CBCD) to incorporate restorative practice community building into the fabric of our School of Medicine and to allow for a climate in which civil discourse might thrive. These retreats blend restorative practice principles with civil discourse models tailored to the dynamics of academic medicine. The overarching aims of this curriculum are to build communication skills among our staff and faculty, begin to consider the many ways in which restorative practice might be implemented within our community, and to allow staff and faculty to make more intimate connections with each other.
The structure of each retreat is designed to foster active engagement and learning. The full-day retreats are held at a site away from our university campus.
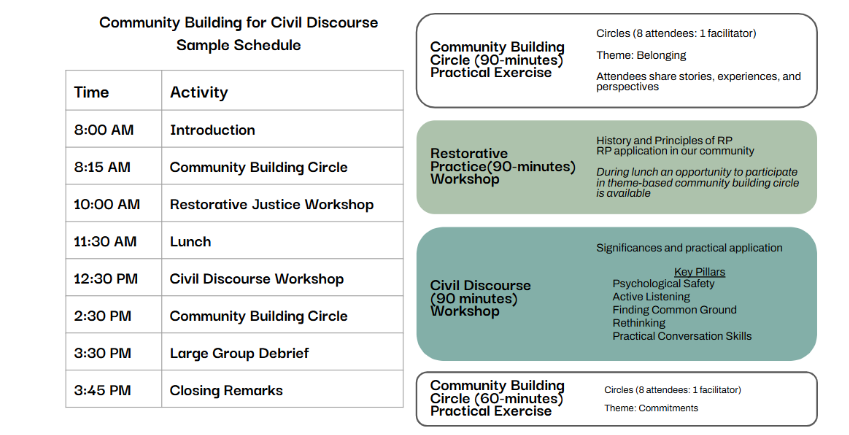
The day begins with a community-building circle (five circles of eight attendees and one facilitator per circle) centered on the theme of belonging, providing participants with a safe space to share stories, experiences, and perspectives. Following this, a 90-minute educational session delves into the history and principles of restorative practice, offering insights into its application within our community. Over lunch, there is an opportunity to either network and reflect or participate in a theme-based community building circle, allowing participants to delve deeper into specific topics of interest.
In the afternoon, attention shifts to civil discourse, with a 90-minute session dedicated to exploring its significance and practical application. Key pillars of civil discourse, including psychological safety, active listening, finding common ground, rethinking, and practicing conversational skills, are discussed and practiced in a variety of interactive activities. The day culminates in another community-building circle aimed at generating commitments for ongoing community activism within the university.
The team invited senior leadership from the School of Medicine to the inaugural retreat, believing that the deliberate selection of participants would emphasize the institutional commitment to fostering a culture of open dialogue and collaboration from the highest echelons of leadership.
Evaluating the impact of these interventions requires a comprehensive evaluation framework that encompasses both quantitative and qualitative measures. Pre- and post-surveys were completed on the day of each retreat, capturing participants’ perceptions of the content and subjective knowledge gained during the retreat. Questions pertained to the acquisition of knowledge about restorative practice and civil discourse, the effectiveness of the retreats, and the sense of belonging and hope among attendees and were scored on a 5-point Likert scale.
Results
To date, 294 individuals representing interprofessional sectors of the academic community have participated in the CBCD retreats, showcasing a broad cross-section of engagement. This breadth of participation highlights the widespread acknowledgment within academic medicine of the significance of fostering open dialogue and collaboration across the institution. The first retreat was attended by department chairs, members of the Dean’s staff, and the Dean of the School of Medicine.
The pre-course survey had a response rate of 88% (259/294), and the post-course survey had a response rate of 90.8% (267/297). Pre-course survey responses showed that less than 45% (117/259) of participants found their departments to be quite or extremely effective at community building, and 38% (98/259) found their departments to be quite or extremely effective at communicating across differences. Additionally, most participants had heard of restorative practice and civil discourse but had varying levels of understanding.
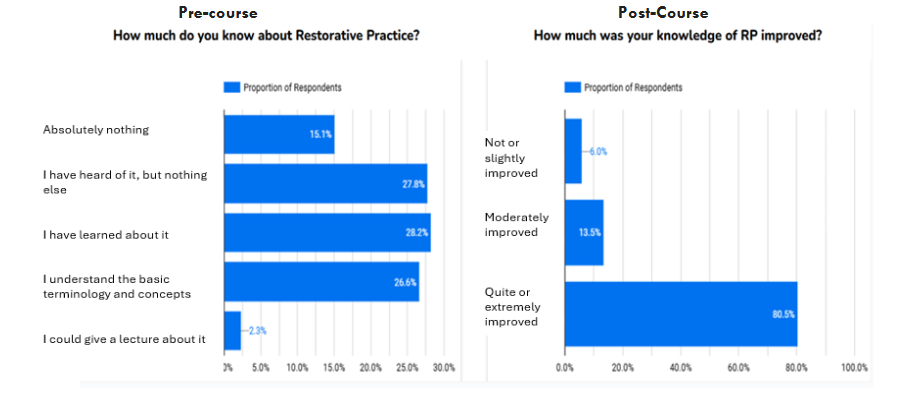
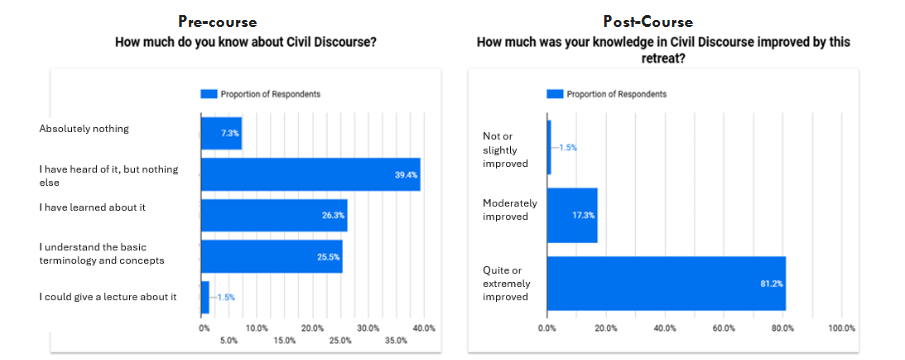
Figure 2: Knowledge before and after CBCD curriculum
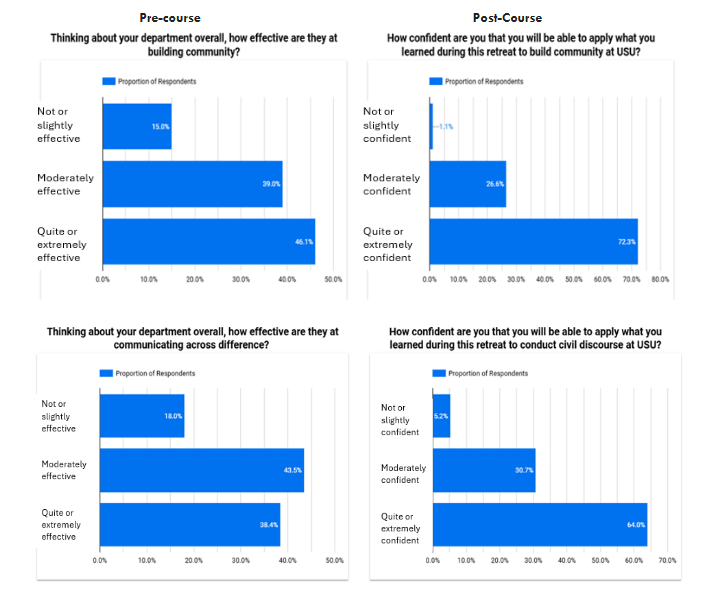
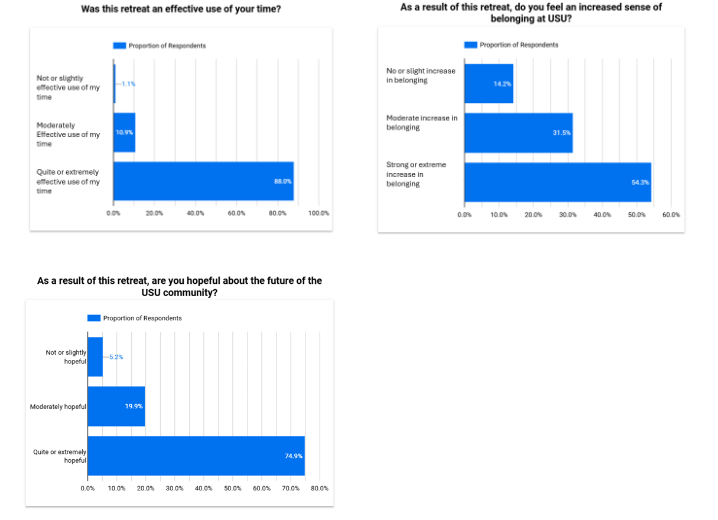
Figure 4: Use of time, belonging and hope after CBCD curriculum
Post-survey responses revealed significant positive feedback. Participants felt that their knowledge had been quite or extremely improved, with 81% (215/267 for RP and 216/267 for CD) reporting an increasing understanding of both restorative practice and civil discourse. Seventy-two-point three percent (193/267) of respondents expressed moderate to extreme confidence in applying what they learned to community building, and 64% (171/267) were quite or extremely confident in their ability to conduct civil discourse. Additionally, 54% (145/267) expressed a strong or extreme increase in their sense of belonging and 74.9% (200/267) felt extreme or high levels of hope for the future of the community. Finally, 88% (235/267) deemed the retreat an extremely or quite effective use of time.
Throughout these retreats, common themes emerged regarding lessons learned and commitments made. Participants collectively pledged to implement restorative practices and civil discourse, utilizing conversational tools and employing circles to facilitate dialogue. The participants also committed to enhancing listening and communication skills, emphasizing active listening, questioning, and patience. Promoting community building and engagement was another key commitment, with a focus on increasing opportunities for meetings to foster trust and respect. Furthermore, participants committed to personal and professional growth, remaining open to alternate perspectives and questioning assumptions. They emphasized the importance of action and accountability, pledging to actively utilize the tools learned during the workshop to drive meaningful change.
As barriers to incorporating what they learned, attendees reported that resistance to change, lack of a common framework and understanding, time constraints, competing priorities, generational and cultural disconnects, fear of negative outcomes, and limited opportunities to practice were the most concerning issues. When asked what they needed to apply their learning, attendees reported they needed several key elements: access to resources and materials, ongoing education and training, practice opportunities, support from facilitators and experts, and leadership and departmental backing.
Discussion
This article describes a successful staff and faculty development curriculum utilizing both restorative practice and civil discourse to improve communication and conflict resolution within an institution. We demonstrated an increase in sense of belonging, confidence in communicating across differences, and hopefulness regarding the future of the institution. The fact that busy staff and faculty members, leaders, and academicians found value in dedicating eight hours to this retreat speaks volumes about its impact and relevance. Participants explored the tiers of restorative practice and the necessity of rethinking traditional conflict resolution approaches. Embracing difference emerged as a fundamental principle, emphasizing the value of communication across difference in fostering a more cohesive and collaborative academic community.
The key lessons learned from these retreats were both impactful and reflected a true understanding of the purposes of the retreat. Participants gained a deeper understanding of restorative practice and civil discourse, along with practical frameworks and techniques for engaging in difficult conversations and active listening. They recognized the significance of community and relationships, developing empathy and valuing the importance of engaging in challenging discussions. The overall results from the faculty surveys highlight the importance of leadership commitment and peer support in driving cultural change.
Building on the key lessons learned, we next delve deeper into the Restorative Practice and Civil Discourse principles that formed a cornerstone of our curriculum, outlining their integration and impact within academic medicine.
Restorative Practice
The integration of restorative practice (RP) principles into academic medicine represents a paradigm shift from hierarchical, punitive approaches to those grounded in community, mutual understanding, and shared accountability. While the predominant application of RP in healthcare settings has centered on its Tier 2 response-to-harm framework, our initiative focused intentionally on Tier 1 community building as a proactive, culture-shaping strategy. This foundational tier offers an underutilized but crucial approach to fostering trust, psychological safety, and authentic relationships among faculty and staff, which are prerequisites for civil discourse and meaningful collaboration.
The promising outcomes of our retreats highlight the relevance and utility of RP as a potential preventative tool in academic institutions. Participants not only reported increased understanding of RP and civil discourse principles but also expressed a strengthened sense of belonging and optimism about their institutional community. These findings align with the broader literature regarding the use of circles outside of medical education, suggesting that RP, particularly through community-building circles, cultivates environments where dialogue can flourish and where individuals feel seen, heard, and valued. This approach also holds particular significance in a post-pandemic landscape, where isolation and incivility have compounded long-standing issues such as mistreatment, marginalization, and structural challenges within medical education.
Despite these successes, implementation challenges remain. Participants voiced concerns about the time and structural support required to embed RP principles into daily practice. There is also the risk that RP, when misunderstood or superficially applied, may be reduced to a tool for managing conflict rather than a framework for reimagining institutional culture. As such, institutions must commit to sustained investment—not only in facilitator training and resource development but also in aligning leadership values with restorative principles. This commitment is essential to moving RP beyond isolated events and toward institutional transformation.
To address these challenges and sustain community building beyond structured retreats, we’ve initiated and will continue monthly lunch and learn events and community building circles. These informal gatherings will offer continuous opportunities for learning, dialogue, and relationship building among faculty, staff, and students, aiming to reduce silos and mitigate hierarchical structures across the university. We also plan to deliver continued faculty development sessions focused on both Tier 1 (community building) and Tier 2 (response to harm) restorative practices to serve as refreshers and enhance faculty capacity.
Civil Discourse
While the integration of restorative practices demonstrates clear benefits, the literature reveals a notable gap in studies specifically examining the outcomes of utilizing civil discourse within medical education. A recent article, “Civil Discourse as a Teaching Strategy in Nursing,” highlights the potential of civil discourse to cultivate competencies in person-centered care and interprofessional partnerships. The potential benefits, such as promoting diverse perspectives, addressing social determinants of health, and fostering empathy and professionalism, are highly relevant to medical training. However, as the nursing article itself points out, direct outcome data demonstrating these benefits within a medical curriculum is largely absent. The current scarcity of peer-reviewed research directly exploring the impact of civil discourse interventions and their subsequent influence uncovers a critical area for future investigation.
Our initiative provided a unique opportunity to explore this gap, as individuals from across the academic community participated in our retreats and demonstrated improvement in both understanding and value of communication across differences. Prior to the retreat, a minority of participants found their departments effective at communicating across differences. Post-survey responses indicated a substantial increase in participants’ understanding of civil discourse and their confidence in applying it. These findings suggest that structured interventions can significantly enhance individuals’ capacity for civil discourse. This is particularly relevant given that promoting community building and engagement, along with enhancing listening and communication skills, were key commitments participants pledged to implement.
This limited evidence, beyond isolated discussions or blog posts, indicates a significant need for rigorous empirical studies to understand how civil discourse can be effectively integrated and assessed within medical education to achieve measurable improvements in communication, empathy, and ultimately, clinical practice.
Conclusion
The challenges posed by political polarization and social isolation demand proactive and innovative interventions within academic medicine. By embracing restorative practice principles and civil discourse models, academic institutions can cultivate environments conducive to open dialogue, collaboration, and belonging. Our findings highlight the value of Tier 1 restorative practices in fostering conditions for civil discourse, repairing fractured relationships, and building academic communities. CBCD is not a panacea, but it provides a powerful, evidence-informed foundation for responding to the complexity of contemporary academic medicine. By investing in community-building approaches and enhanced dialogue, institutions can not only prevent future harm but also begin to heal past wounds and cultivate a more humane and collaborative learning and working environment.
Biographical Notes
- Jessica Bunin, MD, MHPE is a Professor of Medicine and Health Professions Education at the Uniformed Services University in Bethesda, MD.
- Ryan Landoll, PhD is the Assistant Dean of Preclinical Science at the Uniformed Services University in Bethesda, MD. He is an Associate Professor in the Department of Family Medicine.
- Jeanmarie Rey, MD is an Associate Professor of Family Medicine at the Uniformed Services University in Bethesda, MD.
- Lisa Harris, DO is the Assistant Dean for Pathways and Recruitment at the Uniformed Services University in Bethesda, MD. She is an Associate Professor of Family Medicine.
- Gayle “Hava” Haischer-Rollo, MD is the Assistant Dean of Faculty Development at the Uniformed Services University in Bethesda, MD. She is an Associate Professor of Pediatrics.
References
- Weber Shandwick. Civility in America: Solutions for Tomorrow 2019. Weber Shandwick; 2019. Accessed May 24, 2025. https://cms.webershandwick.com/wp-content/uploads/2023/01/CivilityInAmerica2019SolutionsforTomorrow-1.pdf.
- Caravaca F, González-Cabañas J, Cuevas Á, Cuevas R. Estimating ideology and polarization in European countries using Facebook data. EPJ Data Sci. 2022;11(1):56.
- Lane SR, Loya N, LeClere M. Collective response to the 2020 COVID-19, racial injustice, and political polarization triad: case studies for social work education. J Prog Hum Serv. 2024:1-23. doi:10.1080/10428232.2024.2323049.
- Abate LE, Greenberg L. Incivility in medical education: a scoping review. BMC Med Educ. 2023;23(1):24.
- Lewis C. The impact of interprofessional incivility on medical performance, service and patient care: a systematic review. Future Healthc J. 2023;10(1):69-77.
- Stevens H, Rasul ME, Oh YJ. Emotions and incivility in vaccine mandate discourse: natural language processing insights. JMIR Infodemiol. 2022;2(2):e37635.
- Stearns S, Mangan-Friel J, Cushman J. Cultivating Civil Discourse: A Guide for Adults and Youth. University of Connecticut Extension; 2024. Accessed July 23, 2025. https://publications.extension.uconn.edu/publication/civil-discourse/.
- Sheffield SLM, Timmermans JA. Creating a collaborative community spirit for the future of academic development. Int J Acad Dev. 2021;26(2):117-120.
- Sawin G, Sawin V, Wachtel T, et al. Scoping review of restorative justice in academics and medicine: a powerful tool for justice equity diversity and inclusion. Health Equity. 2023;7(1):663-675.
- Acosta D, Karp DR. Restorative justice as the Rx for mistreatment in academic medicine: applications to consider for learners, faculty, and staff. Acad Med. 2018;93(3):354-356.
- Wachtel T. Defining Restorative. International Institute for Restorative Practices; 2012. Accessed August 11, 2025. https://rpforschools.net/articles/Theory/Wachtel%202012%20Defining%20Restorative.pdf.
- Karp DR. Restorative Justice for College and University. Good Books; 2019.
- Shetty N, Fakhoury J, Lopez S, et al. Building a trauma-informed community: applying community building circles to an academic health research setting. Acad Med. 2024;99(2):164-168.
- Donovan EC. Civil discourse as a teaching strategy in nursing. Nurse Educ. 2024;49(4):230-231.