

Free Colon vs. Jejunum Flap for Xerostomia Treatment
Comparison of Free Colon Flap versus Free Jejunum Flap in the Treatment of Xerostomia
Hung-Chi Chen, MD, PhD, FACS 1; Shih-Heng Chen, MD, PHD 2; Yueh-Bih Tang, MD, PhD 3; Katie Lin, MD1
- Department of Plastic Surgery, China Medical University and China Medical University Hospital
- Department of Plastic and Reconstructive Surgery, Chang Gung Memorial Hospital, Chang Gung University and Medical College, Taoyuan, Taiwan
- Department of Plastic Surgery, Far Eastern Memorial Hospital
OPEN ACCESS
PUBLISHED: 30 November 2024
CITATION: Chen, H., Chen, S., et al., 2024. Comparison of Free Colon Flap versus Free Jejunum Flap in the Treatment of Xerostomia. Medical Research Archives, (online) 12(11).
https://doi.org/10.18103/mra.v12i11.5881
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i11.5881
ISSN 2375-1924
Abstract
After radiation or multiple surgeries for oral cancers the patients may develop various degree of xerostomia. They have difficulty in swallowing and speech, also tend to develop inflammation of mucosa, dental caries and even trismus. When the xerostomia is mild, it can be treated with medication or just by frequent hydration with water. When the xerostomia is more severe surgical correction may be an option, namely using free jejunum or colon flap to provide lubrication. However, in the literature there was no comparison between free colon and free jejunum flap for surgical treatment of xerostomia.
Our hospital receives a large number of oral cancers due to consumption of betel nuts which causes 3000 new cases of oral cancers per year in our country. Among our patients 34 had xerostomia treated with surgery. For patients who had no family history of colon cancer and colonoscopy showed no abnormal findings, a free colon flap was selected for reconstruction of xerostomia. When the family history was not clear and the patients were old with polyps during previous colonoscopy, free jejunum flap was used.
Technically the free jejunum flap was harvested from the second portion of jejunum. For colon flap a segment was harvested from right colon. The postoperative results were compared regarding easiness of surgery, bacteria count of the flap, amount and quality of lubrication, comfort of the mouth (including flavor of secretion), requirement of secondary debulking procedures, complications of surgery, infection of lung during follow-ups, etc. The patients reported different responses to the spontaneous movement of jejunum flap inside the mouth. The bad smell of colon flap disappeared after 3 months. The results regarding subjective issue were obtained in the outpatient clinic with questionnaire using 5-point likert scale. The objective data such as requirement of secondary debulking procedures, complications of surgery, and infection of lung during follow-ups were analyzed.
Conclusion: In terms of quality of lubrication, both groups showed similar results. So far there are no patients who develop cancer from the flaps in either group, but jejunum flap seems to be a safer consideration for patients with long life expectancy.
Keywords:
Xerostomia, free colon flap, free jejunum flap, lubrication, odor of flap, bacteria, spontaneous movement of flap
Introduction
Oral cancers are often treated with surgical excision and reconstruction, followed by adjuvant radiation therapy and/or chemotherapy. Regardless of these treatments, the patients may still have multiple recurrences. After radiation or multiple surgeries the patients may develop various degree of xerostomia. They may have difficulty in swallowing and speech. A common complaint is that they could not speak continuously for few minutes, and difficulty to eat dry food. They may also tend to develop inflammation of mucosa, caries and even trismus. When the xerostomia is mild, it can be treated with medication or just by frequent hydration with water. Medical treatments include lozenges and saliva production stimulators which only have temporary effect. When the xerostomia is more severe which seriously affect quality of life or jobs (such as working as a teacher or tour guide), surgical reconstruction can be considered, namely using free jejunum or colon flap to provide lubrication of the oral cavity.
Free colon flap transfer had been reported for the reconstruction of circumferential defect of hypopharynx and esophagus, also used for intraoral reconstruction. It is split longitudinally along its anti-mesenteric border. Free jejunum flap has been used more widely and also can restore lubrication. However, in the literature there was no comparison between free colon and free jejunum flap for treatment of xerostomia.
Patients and Methods:
Our hospital receives a large number of oral cancers due to special culture of chewing betel nut which causes 3000 new cases in our country, an incidence much higher than other countries. Among our patients 34 had xerostomia treated with surgery. For patients having no family history of colon cancer and colonoscopy showed no abnormal findings, a free colon flap was selected for reconstruction of xerostomia. When the family history was not clear and the patients were old with past history of polyps found during colonoscopy, a free jejunum flap was used. Twelve patients received free colon transfer for the reconstruction of their oral mucosal defect following release of trismus, and 22 patients underwent free jejunum flap transfer.
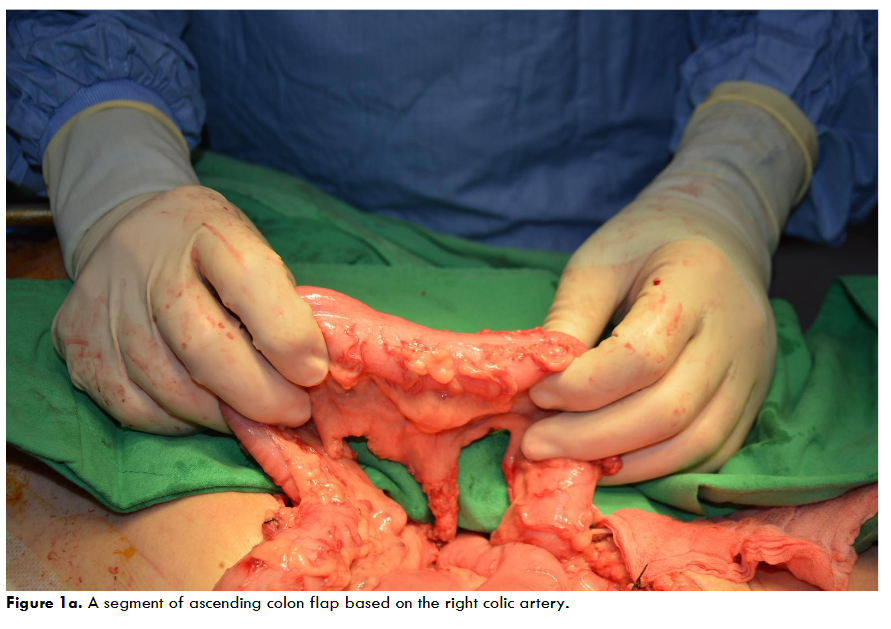
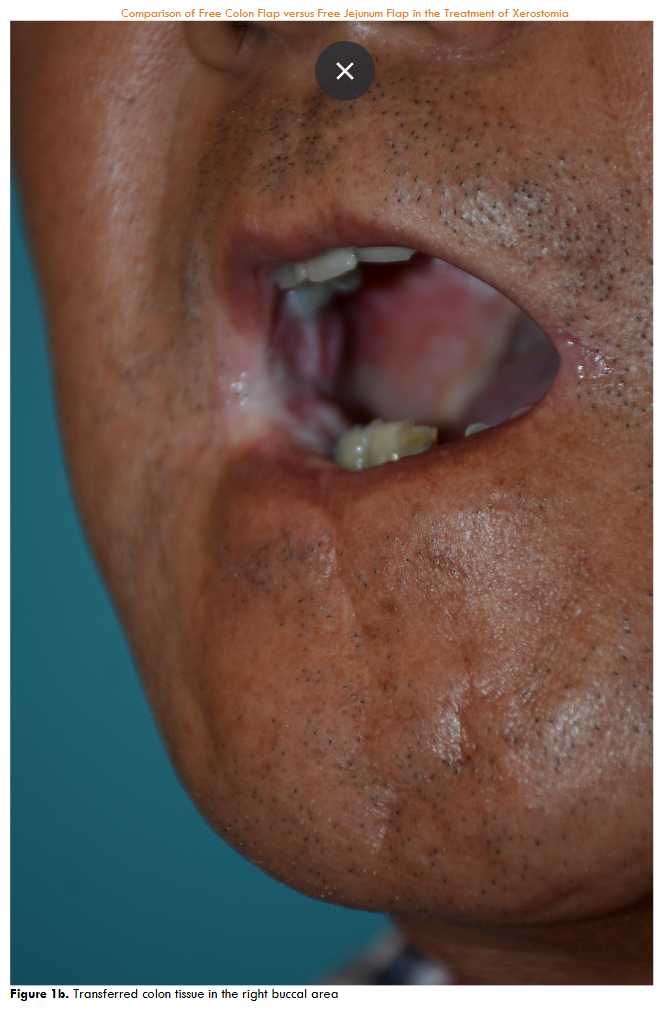
Regarding surgical methods, 12 patients received free colon flap transfer after the release of trismus. The transferred colon flap, harvested via laparotomy approach, consisted of a segment of the ascending colon based on the right colic artery.
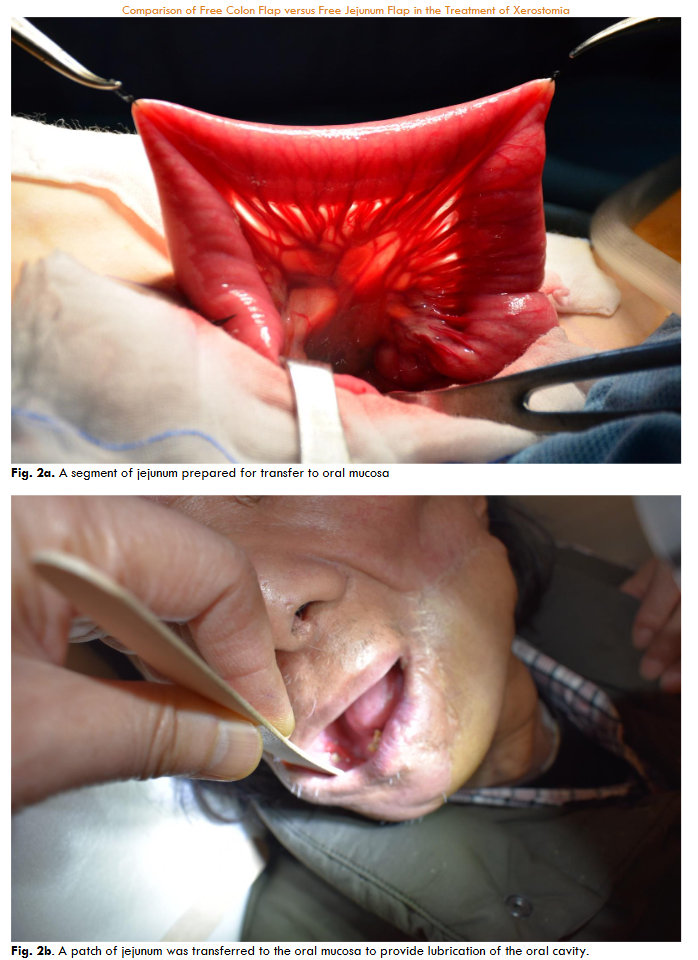
Free jejunum flap was harvested from the second portion of jejunum with second jejunal artery as its vascular pedicle. The harvested jejunum or colon segment was split along its anti-mesenteric border for reconstruction of the oral mucosal defect. It was best indicated when there was no tooth at one side of the mouth so that the flap would not be chewed between the teeth after reconstruction.
Results
In terms of the perioperative evaluation of xerostomia, we followed the “Symptom Management Guidelines: XEROSTOMIA NCI GRADE AND MANAGEMENT,” which graded patients’ severity of xerostomia on a scale of 0 to 4, with grade 0 being normal, and grade 4 being life-threatening.
The postoperative results were compared in 2 aspects:
- objective data: hours of surgery, bacteria count of the flap cultured during surgery, requirement of secondary debulking procedures, complications of surgery, infection of lung during follow-up, etc. These data were analyzed.
- Subjective data: including whether there was spontaneous movement of flap inside the mouth, the quality of lubrication, comfort of the mouth (including flavor of secretion) and the time for disappearance of uncomfortable smell of the flap. The results regarding subjective issue were obtained in the outpatient clinic with questionnaire using 5-point Likert scale.
Table 1: Comparison between free colon flap and free jejunum flap in the reconstruction of xerostomia
| Free colon flap | Free jejunum flap |
|---|---|
| Quality of secretion | More watery (more comfortable to the tongue) |
| More tenacious (slightly less comfortable to the tongue) | |
| Easiness in technique | Tolerates longer ischemia time due to less oxygen demand |
| Tolerates short ischemia time due to high oxygen demand | |
| Intestinal segment harvested | Right colon |
| Second portion of jejunum | |
| Bacterial count during transfer | G-negative and anaerobic bacteria, fungus |
| G-positive and G-negative bacilli | |
| Preoperative bowel preparation | Colon preparation |
| Not needed | |
| Postoperative use of antibiotics | Covering G-negative and anaerobic bacteria, antifungal agents |
| Covering G-positive and G-negative bacteria | |
| Operation time | 6-9 hours (average 7.3 hours) |
| 6-8 hours (average 6.8 hours) | |
| Bad smell | Disappears within 1-3 months |
| No bad smell | |
| Complications | Failure (1/12) |
| No failure | |
| Re-exploration (2/12) | Re-exploration (2/22) |
| Wound infection (2/12) treated conservatively | Wound infection (1/22) |
| Hematoma (1/12) | Hematoma (1/22) |
| Intestinal adhesion (0/12) | Intestinal adhesion (0/22) |
| Pneumonia (0/12) | Pneumonia (0/22) |
| Minimal spontaneous movement in the mouth | Spontaneous movement in the mouth, should not be used to reconstruct part of the lip |
| Requiring revision | 0/12 |
| 3/22 revised due to redundancy of flap | |
| Development of cancer in the flap after transfer | Possible, but not seen in our series |
| None |
Discussion:
Saliva plays an important role for the health of the oral cavity. The functions of saliva provide antimicrobial proteins, enzyme for initial digestion of the food, and lubrication of oral mucosa. The loss of saliva would cause inflammation of oral cavity, dental caries, as well as difficulty in swallowing and speech. Oral cancer patients are often treated with surgery and radiation therapy/chemotherapy. They may develop a moderate to severe xerostomia. Conventional treatment of xerostomia is using saliva stimulant to increase secretion by the remaining salivary glands, which usually has minimal and transient effect after radiation therapy. Other methods include proper hydration and avoidance of hard foods. Surgical reconstruction with intestinal tissue to restore oral lubrication is an option.
In the oral cavity the normal pH is maintained at 6.7-7.3 (near neutrality) by saliva. Tooth decay will develop when pH falls below 5.5. In this situation the patients start to suffer from gingivitis and periodontitis, dental caries, and fungus infection especially candidiasis. After we transfer free jejunum flap, the pH of mouth was slightly alkaline (7-7.5), and nearly neutral (6.5-7.3) after transfer of colon flap. The pH of oral cavity also depends on the function of the residual salivary glands and the size of the transferred jejunum or colon flap.
The microbial composition of the human gut microbiota varies with the gastrointestinal tract:
- In the stomach and small intestine, relatively few species of bacteria are present. However, colon contains the highest microbial density. From proximal to distal gastrointestinal tract, the microbiota have increased in number and diversity. Like in duodenum and jejunum, the composition of microorganisms are Bacilli, Streptococcaceae, Actinobacteria, Actinomycinaeae, Corynebacteriaceae. The small intestine contains small amount of microorganisms due to the proximity to the stomach. Gram-positive cocci and rod-shaped bacteria are the predominant microorganisms found in the jejunum. The bacterial flora of the small intestine aid in a wide range of intestinal functions. After transfer of jejunum we do not need to use antibiotics to cover anaerobic bacteria.
- In the colon, most bacteria are Lachnospiraceae and Bacteroidetes. However, the colon contains a densely-populated microbial ecosystem. The modification in the composition and function of the gut microbiota can change intestinal permeability, digestion and metabolism as well as immune responses. The colon contains the largest bacterial ecosystem in the human body. About 99% of the colon and feces flora are made up of obligate anaerobes such as Bacteroides and Bifidobacterium. Factors that disrupt the microorganism population of the large intestine include antibiotics, stress, and parasites. After transfer of colon flap we need antibiotics to cover anaerobic bacteria.
The lifetime risk of developing colorectal cancer is about 1 in 25. However, a person’s risk might also depend on other risk factors for colorectal cancer, such as diet, obesity, lack of exercise, tobacco and alcohol use as well as environmental impacts such as exposure to chemicals. Family history may also play a role. In our series none of the patients were found to develop colon cancers in the flap with the longest follow-up of 29 years. The incidence of jejunum cancer is much less in general population.
Skin flap (radial forearm flap or anterolateral thigh flap) is often used for reconstruction of oral mucosa defect after excision of oral cancer, which cannot provide lubrication. Free jejunum flap was first done in 1959. Since then, other enteric flaps had been used in the reconstruction of the aero-digestive tract due to good tissue pliability and natural mucus production. Gastro-omental flap is also able to secrete mucus. However, it may develop ulceration due to high acidity of its secretion. In our opinion the gastro-omental flap is not suitable to provide lubrication of oral cavity because it may create an acidic condition with a pH lower than 5.5 which would cause inflammation of oral cavity as well as dental caries.
Regarding to colon flap, in addition to having a better tolerance to ischemia time than jejunum flap, the secretion of colon flap is more watery similar to saliva. In our experience, the bad smell of colon flap usually faded away in 1-3 months postoperatively. In a previous study, Escherichia Coli is the organism cultured most frequently. In this study, the disappearance of originally bad smell was noted because there was no food residue to be metabolized by E. Coli to produce hydrogen sulphide and methanethiol. In our clinical case series, it did not cause infection of the oral cavity, esophagus, or the lung. The intestinal bacteria are not extinguished even after a long period of time, and intestinal flap transfer to the oral cavity or pharynx is safe for the patients.
In the previous studies the transverse colon segment based on the middle colic artery was the donor site. However, the middle colic artery is usually more dominant in blood supply for the colon system. Therefore, we preferred to harvest the ascending colon flap based on the right colic artery to preserve the major blood supply of the colon system.
To prevent future trismus and to maximize the capability of secretion, the ischemia time during flap transfer should be minimized. Several methods have been proposed, such as preparation of recipient vessels before ligation of the vascular pedicle, vessel anastomosis before definitive flap inset, or mastering the “airborne” suture tying technique to shorten vascular anastomosis time.
In earlier animal studies, the tolerance of ischemic time was shorter for the ileum than for the jejunum, and ischemic time of less than 1 hour was suggested for microvascular transfer of the ileum. It was believed that there are more bacteria in the ileum than in the jejunum, and therefore autolysis will be triggered sooner after the initiation of ischemia. However, some animal experiments conducted by Nakao showed that ischemic time of jejunum and ileum had no significant differences. The study by Chen et al in 2013 was to identify the ischemic tolerance of the ileum, and the study showed ischemic time of more than 1 hour is compatible with good survival of ileum and colon. Therefore, in the future, ileum transfer can be another option for treatment of xerostomia.
Some might concern about the risk of colon flap harvest by laparotomy, which might outweigh the benefit of treating trismus and xerostomia with colon or jejunum flap. However, in the study addressing the donor-site morbidity after free ileocolon flap transfer, the most frequent complication is only transient diarrhea. Therefore, the donor-site morbidity would be reasonably less.
There are other salivary gland disorders leading to xerostomia, such as salivary gland tumors, Sjogren’s syndrome and infections. Some promising new methods are being developed to treat the xerostomia with the regeneration of the salivary gland, such as stem cell therapy and bioengineered artificial salivary gland organ.
Conclusion:
In terms of quality of lubrication, both groups showed similar results. Regardless of the high incidence of colon cancer, so far in our series there were no patients who develop cancer in either group, but jejunum seems to be a safer consideration for patients with long life expectancy. Free colon or jejunum flap transfer could safely provide lubrication in patients with severe xerostomia. After release of trismus, either free colon or jejunum flap could repair oral mucosa defect with simultaneous relief of xerostomia.
References:
- Dirix P, Nuyts S, Van den Bogaert W. Radiation‐induced xerostomia in patients with head and neck cancer: a literature review. Cancer: Interdisciplinary International Journal of the American Cancer Society 2006; 107:2525-34.
- Wijers OB, Levendag PC, Braaksma MM, Boonzaaijer M, Visch LL, Schmitz PI. Patients with head and neck cancer cured by radiation therapy: A survey of the dry mouth syndrome in long‐term survivors. Head & neck 2002; 24:737-47.
- Wu AJ. Optimizing dry mouth treatment for individuals with Sjögren’s syndrome. Rheumatic Disease Clinics of North America 2008; 34:1001-10.
- Ying-Sheng Lin, Seyed Abolghasem Mousavi, Hung-Chi Chen. Free colon tissue for the management of xerostomia in head and neck cancer patients: A bacteriological study and clinical case series. J Plast Reconstr and Aesthetic Surg 2022; 75 : 2676-2683.
- Braakhuis BJM, Visser O, Leemans CR). Oral and oropharyngeal cancer in the Netherlands between 1989 and 2006: increasing incidence, but not in young adults. Oral Oncology 2009; 45: e85-e89.
- Jung KW, Park S, Kong HJ, Won YJ, Lee JY, Park EC, Lee JS. Cancer statistics in Korea: incidence, mortality, survival and prevalence in 2008. Cancer Res Treat 2011; 43(1): 1-11.
- Agency BC. Symptom Management Guidelines: XEROSTOMIA NCI GRADE AND MANAGEMENT.
- Porcheri C, Mitsiadis TA. Physiology, Pathology and Regeneration of Salivary Glands. Cells 2019; 8:976.
- Soutar DS, McGregor I. The radial forearm flap in intraoral reconstruction: the experience of 60 consecutive cases. Plast Reconstr Surg. 1986;78:1-8.
- Koshima I, Fukuda H, Yamamoto H, Moriguchi T, Soeda S, Ohta S. Free anterolateral thigh flaps for reconstruction of head and neck defects. Plast Reconstr Surg 1993; 92:421-8; discussion 9-30.
- Kadota H, Fukushima J, Nakashima T, Kumamoto Y, Yoshida S,Yasumatsu R, Shiratsuchi H, Morita M. Comparison of salvage and planned pharyngolaryngectomy with jejunal transfer for hypopharyngeal carcinoma after chemoradiotherapy. Laryngoscope 2010; 120: 1103-1107.
- Wada T, et al. ICG fluorescence imaging for quantitative evaluation of colonic perfusion in laparoscopic colorectal surgery. Surg Endosc 2017; 31(10):4184–4193.
- Seidenberg B, Rosenak SS, Hurwitt ES, Som ML. Immediate reconstruction of the cervical esophagus by a revascularized isolated jejunal segment. Ann Surg 1959; 149:162.
- Lorenz RR, Alam DS. The increasing use of enteral flaps in reconstruction for the upper aerodigestive tract. Current opinion in otolaryngology & head and neck surgery 2003; 11:230-5.
- Gallagher J, Webb A, Ilankovan V. Gastro-omental free flaps in oral and oropharyngeal reconstruction: surgical anatomy, complications, outcomes. The British journal of oral & maxillofacial surgery 2002; 40:32-6.
- Chen HC, Ciudad P, Chen SH, Agko M. Thirty‐five years of single surgeon experience in the reconstruction of esophagus and voice with free ileocolon flap following total pharyngolaryngectomy. Journal of surgical oncology 2018; 117:459-68.
- Flynn M, Acland R. Free intestinal autografts for reconstruction following pharyngolaryngoesophagectomy. Surgery, gynecology & obstetrics 1979; 149:858-62.
- Nakatsuka T, Harii K, Ebihara S, Hirano K, Haneda T, Hayashi R, et al. Free colon transfer: a versatile method for reconstruction of pharyngoesophageal defects with a large pharyngostoma. Ann Plast Surg 1996; 37:596-603.
- Wei F-C, Carver N, Chen H-C, Tsai M-H, Wang J-Y. Free colon transfer for pharyngo-oesophageal reconstruction. British journal of plastic surgery 2000; 53:12-6.
- Jones TR, Lee G, Emami B, Strasberg S. Free colon transfer for resurfacing large oral cavity defects. Plast Reconstr Surg 1995; 96:1092-9.
- Wei F-C, Lutz BS, Chen H-C, Tsai M-H, Lin P-Y. Free transverse colon transplantation for functional reconstruction of intra-oral lining: a clinical and histologic study. Plast Reconstr Surg 1998; 102:2346-51.
- Rampazzo A, Gharb BB, di Spilimbergo SS, Chung K-P, Chen H-C. Voice reconstruction with free ileocolon flap transfer: implications for the lower respiratory tract. Plast Reconstr Surg 2011; 127:1916-24.
- Rampazzo A, Salgado CJ, Gharb BB, Mardini S, Di Spilimbergo SS, Chen H-C. Donor-site morbidity after free ileocolon flap transfer for esophageal and voice reconstruction. Plast Reconstr Surg 2008; 122:186e-94e.
- Leung HW, Chan AL. Glutamine in alleviation of radiation-induced severe oral mucositis: A meta-analysis. Nutrition and cancer 2016; 68:734-42.
- Suarez F, Springfield J, Levitt M. Identification of gases responsible for the odour of human flatus and evaluation of a device purported to reduce this odour. Gut. 1998; 43:100-4.
- Chen H-C, Mardini S, Tsai F-C. “Airborne” suture tying technique for the microvascular anastomosis. Plast Reconstr Surg 2004; 113:1225-8.
- Agko M, Ciudad P, Chen HC. “Airborne” suture tying technique: Simple steps to make it easy. Head & neck 2017; 558-61.
- Nakao M, Taguchi T, Yanai K, et al. Energy metabolism during cold ischemia and reperfusion in rat small intestinal transplantation: comparison of jejunal and ileal grafts. J Pediatr Surg 1997; 5e1678.
- Chen SH, Tang YB, Chen HC. Survival of transferred ileum after ischemia time longer than 1 hour: a clinical result different from animal studies. J Am Coll Surg. Aug 2013, 217; (2):300-5. doi: 10.1016/j.jamcollsurg.2013.03.018. Epub 2013 Jun 5. PMID: 23755932.
- Coppes R, Stokman M. Stem cells and the repair of radiation‐induced salivary gland damage. Oral diseases 2011; 17:143-53.
- Kojima T, Kanemaru Si, Hirano S, Tateya I, Ohno S, Nakamura T, et al. Regeneration of radiation damaged salivary glands with adipose‐derived stromal cells. The Laryngoscope 2011; 121:1864-9.