Funding and Organization of Child Abuse Teams in the USA
Organization and Funding of Medically-Oriented Child Abuse and Neglect Teams in the USA: Key Issues to Consider
Angelo P. Giardino, MD, PhD, MPH
Wilma T. Gibson Presidential Professor
Chair, Department of Pediatrics
University of Utah School of Medicine
Chief Medical Officer, Intermountain Primary Children’s Hospital
295 Chipeta Way, STE #9
Salt Lake City, UT 84108
801.587.7415
[email protected]
OPEN ACCESS
PUBLISHED: 31 March 2025
CITATION: Giardino, A., P., 2025. Organization and Funding of Medically-Oriented Child Abuse and Neglect Teams in the USA: Key Issues to Consider. Medical Research Archives, [online] 13(3). https://doi.org/10.18103/mra.v13i3.6298
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i3.6298
ISSN 2375-1924
ABSTRACT
Ideally, children reported for potential abuse and/or neglect would receive an evaluation by a medically-oriented child maltreatment team composed of an interdisciplinary team of health care professionals who collaborate with the community’s child protection and law enforcement professionals who then conduct an investigation to potentially substantiate the abuse and/or neglect. Each year, approximately 3 million reports for potential child abuse and neglect are received by authorities in the USA, and after investigation in 2022, over 558,000 children under 18 years of age were determined to be victims of some form of child maltreatment. This topical review explores the literature that has emerged over the past 25 years describing the systematic study of the organization and funding of medically-oriented child abuse and neglect teams in the USA. Several national surveys are summarized and compared regarding the organization and funding of such teams and programs. The majority of these teams are housed in the nation’s children’s hospitals, and child maltreatment programs vary widely in terms of 1) the professionals who staff the team, 2) the range of services each team provides, and 3) the manner in which they are funded and financially managed. Local factors are key to how teams are staffed and sustained, and, while the services provided are essential to the care of the children involved, the institutions housing the child abuse and neglect teams uniformly shoulder a significant portion of the financial responsibility to operate the programs on an annual basis.
Keywords: child abuse, neglect, funding, child maltreatment teams, interdisciplinary teams
Introduction
Ideally, children reported for concerns of abuse and neglect would receive a multi-disciplinary evaluation, and if child maltreatment is suspected, then a report would be made and a broader investigation would be conducted by child protection services and/or law enforcement. A medically-oriented child maltreatment evaluation team would be one that has at least one physician or advanced practice provider (i.e., nurse practitioner or physician’s assistant) serving on the team who participates in the child’s evaluation. This topical review will explore the relevant selected literature regarding medically-oriented child abuse and neglect or child maltreatment evaluation teams, many of which are housed at or associated with the nation’s approximately 220 children’s hospitals across the USA. See Appendix 1. Specifically, the review will highlight 1) the composition of the teams, 2) the services typically provided by these teams, and 3) the range of issues related to the finances that support the teams and their various activities.
Background
In 2022, the year with the most current national statistics for child maltreatment, authorities in the US received 3,096,101 reports of possible abuse and/or neglect, and after investigation by child protection law enforcement, 558,899 children under 18 years of age were determined (i.e., substantiated) to be victims of child maltreatment. Approximately three quarters of victims experienced neglect, nearly a fifth experienced physical abuse, about 10% experienced sexual abuse, another 7% experienced psychological abuse, and an estimated 1,990 children died as a result of their maltreatment.
In addition to the trauma experienced by the child who is abused and/or neglected, maltreatment also is known to have a tremendous financial impact on the child and their community as well. Using a lifetime of incurred cost type model, Klika, Rosenzweig and Merrick from a leading child advocacy national organization, Prevent Child Abuse America, estimated that for the 677,529 children substantiated in 2018 the total economic burden for these cases of child maltreatment that year would be approximately 563 billion dollars over their entire life course. Note this is a total lifetime cost projected forward from the year of their maltreatment and not the cost in that year alone when the case was substantiated.
Almost from the inception of child abuse and neglect as a field, the value of using a multi-disciplinary or interdisciplinary approach to patients referred for evaluation has been widely embraced. Multi- or interdisciplinary teams who evaluate possible cases of child maltreatment are composed of professionals from a variety of child-serving professions, typically address complex medical and psychosocial aspects of child maltreatment, and typically conduct lengthy evaluations that often require interfacing with other sectors outside of health care who then conduct the investigation such as child protective services law enforcement as well as the courts. Specific to child abuse and neglect evaluations, multi-disciplinary teams are defined as “a group of professionals who work together in a coordinated and collaborative manner to ensure an effective response to reports of child abuse and neglect.” The positive aspects to using this multidisciplinary approach in the evaluation of potential child maltreatment are generally seen as improved information sharing among professionals involved, promoting joint decision making and care planning, opportunity for shared and collaborative training and education, and the capacity to provide mutual support to team members doing this challenging work. Additionally, comprehensive evaluations that utilize the skills and expertise of a variety of disciplines are more likely to increase accuracy of the evaluations and decrease inappropriate referrals to child protective services. Early on, however, it was recognized that many of these labor-intensive, shared activities are not readily billable in the traditional fee-for-service health care financing environment omnipresent in the US health care system. As such, concerns about the financial viability of medically-oriented child maltreatment teams are longstanding and date back to the 1990s.
Method/Approach to topical review:
A number of surveys and program descriptions have been reported in the child abuse medical literature over the past 25 years which describe child maltreatment teams in the USA and which address: 1) the range of staffing and team composition models for medically-oriented child maltreatment teams, 2) the array of services and activities in which these teams engage, and 3) the variety of fiscally-related issues such as budget size, billing and reimbursement issues, and various sources of funding. Over this approximately 25-year period of time covered by this relevant selected literature, what has become clear is that multi-disciplinary child maltreatment teams, despite having a common mission of providing high quality diagnostic evaluations to children suspected of having been maltreated, manifest a great deal of variation in how they organize and fund themselves and this is described in the ensuing topical review. In fact, variation, mostly driven by local factors at each institution, is more the rule than the exception. To date, a number of successful approaches or models have been described, some state-wide, some regional in nature, and others, institution or program specific. Over time, program leaders have become more aware of the fiscal issues that underpin their team’s functioning and sustainability, and most remain concerned about the relative mismatch between the activities that must be supported to provide high quality evaluations and service to those children suspected of having been maltreated and the financial support available to sustain these efforts.
The Children’s Hospital Association (CHA) and its predecessor, the National Association of Children’s Hospitals and Related Institutions (NACRHI), defined a three-tiered description of the types of programs that could be available at member children’s hospitals that may be called upon to provide care, service, and support to children and families confronting concerns of possible child abuse and neglect.
| Basic | Advanced | Centers of Excellence |
|---|---|---|
| The three functions essential to a child protection response are: medical leadership, administrative coordination, and social work services. Each essential function need not be performed by a separate, dedicated staff person. | Advanced level, in addition to meeting all recommendations for the basic level, the child protection team is led by a full-time medical director who is board certified in child abuse pediatrics (with few exceptions). | Centers of excellence are distinguished by additional educational and research capabilities. In general, in addition to meeting all recommendations for the basic and advanced levels, a center of excellence features larger child protection teams whose members include additional professionals in the hospital, such as psychologists. |
| Staffing may be limited but includes, at minimum, a physician who provides medical leadership and administrative coordination, and social work services provided by staff trained in the field of child abuse. | Generally, has additional staff. Is an administrative unit of the children’s hospital with centralized management and administrative functions. | Offers advanced diagnostic and treatment services that often require consultation with hospital medical and surgical subspecialists. |
| Representatives of community agencies routinely participate in child protection meetings. | Meets regularly to present and review child abuse cases. Coordinates, as appropriate, with community agencies involved in child protection. | Is likely to offer an accredited fellowship. May sponsor multicenter trials. |
| If mental health professionals are not assigned to child protection, they should be available from other hospital departments or via referral. | Is more likely to serve a broader catchment area, receiving referrals from outlying communities. | Is a regional and national leader in child maltreatment and related family violence intervention and prevention. |
Topical Review
Staffing Composition and Services Provided:
For over 25 years, investigators have explored the types of professionals included on medically-oriented child maltreatment teams along with the range of services and activities in which these professionals participate. In a 1993 survey of child abuse teams drawn from a list of programs known to the Executive Committee of the American Academy of Pediatrics and published in 1999, 90% of 72 responding teams reported being staffed with a physician, 90% with social workers, 49% with nurses, and 67% had clerical support. Later, in a 1998 survey modeled after this 1993 survey, which was sent to a much larger list of programs drawn from the registries available from several large national organizations, of the 153 usable responses, 95% were staffed with physicians, 81% with social workers, 52% with nurses, 58% with psychologists or mental health professionals, and 56% with clerical or administrative staff. In a 2001 survey to child abuse programs specifically at children’s hospitals that sought to describe the “system of care” that served children suspected of having been maltreated, Tien and colleagues reported that of 122 respondents, 94% were staffed with physicians, 92% with social workers, 73% with nurses, and 53% had other health care professionals such as nurse practitioners, psychologists, psychiatrists or child life specialists.
Beginning in 2005, NACHRI, and then later its successor organization, CHA, conducted a series of 3 surveys of the hospital-based child abuse teams and programs in children’s hospitals across the US which were repeated approximately every three to four years until 2012. In the 2012 survey, of the 145 responses and using the tiered framework described above in Table 1, 27% of programs were Basic programs, 38% were Advanced, and 27% were at the Center of Excellence level, with 6% reporting no child abuse services. Of the 111 respondents in the 2012 CHA survey which answered the staffing question, 96% reported a physician medical director, 77% with social work, 71% with administrative support, 54% with nurse practitioners or physicians assistants, 44% with behavioral health professionals including psychologists, and 37% with nurses.
Most recently, with the support of CHA, the American Academy of Pediatrics and the Helfer Society (a physician organization of board certified Child Abuse Pediatricians), Bachim and colleagues reported on a 2017 survey that asked for data from calendar year 2015 and which built upon the 2012 CHA survey, and these authors provided a comparison to the CHA 2012 survey data. Of the 113 respondents, 19% were Basic programs (down from 27% in 2012), 45% were Advanced (increased from 38% in 2012) and 27% were at the Center of Excellence level (unchanged from 2012), with 8% reporting no child abuse services. Of the 100 respondents who provided staffing data for the year 2015, 72% reported increased staff time since 2012 with 16% reporting no change and 12% reporting less. Physicians were reported as staff on the team at 74%, social workers at 77%, administrative support at 74%, nurse practitioners and/or physicians assistants at 59%, behavioral health professionals at 63%, and staff nurses at 59%. Bachim and colleagues also provided a table that displays the full time equivalent (FTE) staffing average for each profession, for programs based on the tiered framework.
Services Provided:
In addition to the types of professionals who staff the teams and programs, the range of services provided by these professionals serving on the interdisciplinary child abuse and neglect teams also received attention in the literature. In the 1993 survey, 63 respondents described the physician time on the medically-oriented team as being allocated to patient care (60%), teaching (~17%), research (~9%), community service (~9%), and other activities such as administrative tasks or providing court testimony (~6%). Fifty-eight respondents listed other activities in which the interdisciplinary team engaged which included: inpatient consultations, outpatient evaluations, telephone consultations, crisis intervention, mental health services, and home visits.
In the 2001 survey conducted by Tien and colleagues, of the 88 respondents reporting on services provided, child maltreatment teams consulted on cases (89%), functioned as a liaison with child protective services (85%), tracked cases of maltreatment (70%), conducted quality assurance (63%), and made reports to child protective services (61%). Finally, in the 2012 CHA survey, 112 programs reported upon services provided, and these are listed in Table 3 below:
| Service | % of Programs Providing |
|---|---|
| Medical examinations | 99 |
| Court testimony | 98 |
| Inpatient medical care | 97 |
| Phone consultation | 96 |
| Written expert reports | 95 |
| 2nd opinion medical consultations | 88 |
| Psychosocial assessments | 76 |
| Mental health services | 59 |
| Forensic Interview | 49 |
| Telemedicine 2nd opinion | 43 |
Team Finances:
Regardless of team composition or in what activities teams engaged, the issue of how the team found financial support for their work and how the team managed its finances were of keen interest to child abuse and neglect professionals and health care administrators alike. Harkening back to Sister Irene Kravis, former CEO of the Catholic Hospital Association, and her now infamous quip about fiscal affairs, namely, “no margin, no mission,” it is paramount to understand the financial reality of how best to balance offering a specific health care service with a funding approach that sustains it over the long run. A sustainable business model is essential to keep the team adequately staffed and resourced which then allows it to function in an operationally stable manner, providing access to those services for the population currently and into the future. With this in mind, as a project for the special interest group of the Ambulatory Pediatric Association, Giardino and colleagues conducted an early survey in 1993 that sought out information on annual budgeting, funding sources, and funding stability related to the operation of medically-oriented child abuse and neglect evaluation teams in the US.
The initial 1993 survey collected data that suggested remarkably variable approaches to fiscal management among responding child abuse teams, most of which were at academic centers and housed within their associated children’s hospitals. Among the 51 respondents who disclosed an annual budget, the median total budget was $245,000, and budgets ranged from zero dollars, which indicated that the child abuse team was intertwined and embedded in other programs so respondents could not disaggregate their own program’s budget, to a high of $1,467,000. Approximately 55% of responses indicated a budget of zero to $250,000, another 25% indicated a budget above $250,000 to $500,000, and 20% reported budgets greater than $500,000.
Information collected on funding sources from 67 respondents varied widely and the most common revenue source was generated by patient care at over 34%, state and local government support at nearly 29%, and hospital or medical school intramural support at 18% which was then followed by single digit percentages for other which included grants, research grants, donations, honoraria, and training grants. Finally, 67 respondents also provided their assessment of funding stability for their program with 30% rating their child abuse and neglect program’s funding as very unstable, 34% rating it as stable and, 36% as very stable. Additionally, 69 respondents provided their opinion about the importance of funding to their child abuse and neglect team/program with 57% indicating that funding was important, another 29% indicating it was moderately important, and 14% indicating that funding was not important to the program.
In a similar 1998 survey among a broader sample of programs, the mean annual budget reported by 127 respondents was up to a median total budget of $300,000, and the reported range for budgets was from zero (no separate budget) to $6,000,000; 25% of programs reported a budget between zero and $125,000, 25% reported a budget figure greater than $125,000 to $300,000, 25% reported budgets greater than $300,000 to $610,000, and 25% reported an annual budget of greater than $610,000. Funding sources continued to vary widely, and among the 153 programs responding, state and local government funding was at 30% and patient care revenue was at 20% with a long list of other sources being reported including donations, victim funds, other grants, hospital or organizational intramural support, expert fees, and research. As a further drill down in the data, the broader survey in the 1998 study allowed the categorization of programs as hospital-based or community-based, and through this lens the 91 hospital-based programs reported patient care revenue at 27.5% compared to the 62 community-based programs at only 10%, whereas government funding was reported at 54% for community-based programs compared to only 20% for the hospital-based programs. Finally, of the 99 respondents who rated their opinion on funding stability, 17% rated funding stability for the program as very unstable, 49% rated it as stable, and 34% as very stable. Additionally, 49% indicated that funding was very important, 42% indicated it was moderately important, and only 9% indicated it was not important for their program. In the Tien and colleagues 2001 survey which collected limited financial information on child maltreatment programs at children’s hospitals, of the 122 respondents, 52% had a budget of $500,000 or less. In the 2012 CHA survey, 51 respondents reported the amount of direct expenses attributed to the child abuse program, regardless of whether they had an individual budget or not, and the reported direct expenses had a median of $800,000 and ranged from $20,893 to $9,599,410, with the mean for the 51 responding hospitals equal to $1,113,703. CHA reported that 47% of the direct expenses were covered on average by the hospital via intramural funding or subsidy, ranging from 5 hospitals where no direct expenses are covered to 9 hospitals where all of the direct expenses are covered. Regarding revenue, 55 hospitals reported an average revenue of $722,174, with a median of $450,000 and a range of $1,662 to $8,373,197. Revenue sources with the percentage of hospitals reporting each source are displayed in Table 4 below:
| Revenue Source | % of Hospitals Reporting (n = 104) |
|---|---|
| Medicaid | 87 |
| Private insurance | 77 |
| Payment for services | 69 |
| Victims of crime compensation | 48 |
| Donations | 38 |
| Hospital foundation | 36 |
| Court fees | 27 |
| Other foundations | 24 |
| National Children’s Alliance | 22 |
| SCHIP | 20 |
| TRICARE | 19 |
| State budget line item | 17 |
| State Attorney General or DOJ | <15 |
In addition to the budget numbers, 35 programs in 2015 provided direct expense data similar to CHA’s 2012 survey data and, in 2015, the mean direct expenses were $1,823,945 and 30 programs reported that on average their hospital covered 25% of those expenses, down from 47% in 2012.
Discussion
Medically-oriented child abuse and neglect teams and programs demonstrate considerable variation in the ways they serve their patients and staff and finance themselves. The one commonality that medically-oriented teams share is based on the way they are defined as including at a minimum a physician or an advanced practice provider such as a nurse practitioner or physician assistant. Outside of this shared element, teams clearly vary in how often they include staff nurses, social workers, and administrative personnel. Even more variation exists when it comes to including mental health professionals. Beyond differences in staffing, substantial variation is demonstrated in the services offered by these teams across programs in the US. While clinical care appears to be a common core element to many teams, a great deal of variation exists in terms of consultations, record review, court testimony and community involvement. Perhaps the greatest variation exists in the fiscal realms, especially how these teams fund themselves as well as how they manage their finances, budgets, revenues and expenses. Over the approximately 3-decade period of time covered by the relevant literature reviewed above, the size of the teams has grown, the types of professionals have increased, the sources of funding have broadened, the size of the budgets have increased and the recognition of the importance of finances to the sustainability of the programs among programs have increased as well. In the conclusion to the first survey reported upon in this topical review, the 1993 survey (published in 1999), the authors commented about the importance of grappling with the fiscal affairs of the child maltreatment teams, namely:
“In summary child abuse teams may be at risk in an era of limited resources and increasing financial pressures. This is only worsened by limited knowledge and awareness of the financial issues related to the management of the child abuse program, including budgets, costs, and reimbursement especially when coupled with the ever-present competing responsibilities of the team’s members. Clearly, program leaders view financial issues as important and great diversity exists among program strategies to address these issues.”
However, in the most recent article published 30 years later, the concern about finances remain even though decades have passed, with those authors raising concerns about unfunded care and potentially precarious funding for the teams and the professionals who staff them, namely:
“Child maltreatment teams within pediatric hospitals provide services that are largely unfunded and are currently unrecognized by healthcare payment models. Consistently, these specialists perform a variety of important clinical and non-clinical services that are critical to the medical and legal care of this population while relying on a diversity of funding sources to support their efforts. This study is part of an ongoing effort to collect and share data related to the risk that child abuse pediatric programs face since their services are so highly needed, but also so poorly funded. Efforts should continue to collect this data periodically to track if the fiscal situation for teams changes, particularly over the next survey period which includes the coronavirus pandemic.”
Conclusion
Medically-oriented multidisciplinary teams mostly housed at children’s hospitals have a variety of staffing models, are engaged in a broad range of services and supports surrounding the evaluation and treatment of children suspected of having been abused or neglected, and have a complicated financial picture to deal with including multiple sources of revenue and the need for a significant amount of institutional support. Not unexpectedly, the annual budgets for these teams have grown over the past three decades and the children’s hospitals that choose to host these programs take on a significant financial responsibility. In addition to the aforementioned hospital support, patient care revenue and local state government funding have consistently remained major sources of revenue. The majority of leaders for these medically-oriented child maltreatment teams indicate that financial issues are important to the sustainability of the program, and these leaders vary in their perception of their funding’s stability. The approach to operational and fiscal management appears to be widely variable, presumably responsive to local conditions that face each team in their own environment. The adaptability displayed by these teams and their leadership provides reason for optimism, however; the multi-disciplinary medically-oriented teams appear agile and responsive to local conditions which suggests they are well positioned to address challenges as they emerge in the future since the literature documents that they have been doing so for more than three decades in the past.
Conflict of Interest
None
Funding Statement
None
Acknowledgements
The author acknowledges the literature searching and copy-editing support from Brandy Harman whose assistance was essential to the completion of this work.
References:
- U.S. Department of Health & Human Services, Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau. (2024). Child Maltreatment 2022. Available from https://www.acf.hhs.gov/cb/data-research/child-maltreatment. Accessed 01-07-2025
- Klika, J.B., Rosenzweig, J. & Merrick, M. Economic Burden of Known Cases of Child Maltreatment from 2018 in Each State. Child Adolesc Soc Work J 37, 227–234 (2020). https://doi.org/10.1007/s10560-020-00665-5
- Peterson C, Florence C, Klevens J. The economic burden of child maltreatment in the United States, 2015. Child Abuse Negl. 2018;86:178-83. doi: 10.1016/j.chiabu.2018.09.018
- McColgan MD, Siconolfi DA, DeJong A. Multidisciplinary Teams. In: Giardino A, Lyn M, Giardino E, eds. A Practical Guide to the Evaluation of Child Physical Abuse and Neglect. Cham: Springer; 2019:447-467. doi:10.1007/978-3-030-00635-8_15
- Scribano PV, Giardino AP. Interdisciplinary approaches to child maltreatment: Accessing community resources. In: Giardino AP, ed. Medical Evaluation of Child Sexual Abuse: A Practical Guide. 2019:331-354. Elk Grove Village, IL: American Academy of Pediatrics. doi:10.1542/9781610022965-ch13.
- Ells, M. Forming a Multidisciplinary Team to Investigate Child Abuse. Rockville, MD: Office of Juvenile Justice and Delinquency Prevention; 2000. https://www.ojp.gov/pdffiles1/ojjdp/170020.pdf, Accessed 01-07-2025
- Wallace GH, Makoroff KL, Malott HA, Shapiro RA. Hospital-based multidisciplinary teams can prevent unnecessary child abuse reports and out-of-home placements. Child Abuse Negl. 2007 Jun;31(6):623-9. doi: 10.1016/j.chiabu.2006.12.010. Epub 2007 Jun 27. PMID: 17590436.
- Kupfer GM, Giardino AP. Reimbursement and insurance coverage in cases of suspected sexual abuse in the emergency department. Child Abuse Negl. 1995;19(3):291-5. doi.org:10.1016/S0145-2134(94)00128-6
- Giardino AP, Montoya LA, Richardson AC, Leventhal JM. Funding realities: child abuse diagnostic evaluations in the health care setting. Child Abuse Negl. 1999;23(6):531-8. doi.org:10.1016/S0145-2134(99)00034-4
- Tien I, Bauchner H, Reece RM. What is the system of care for abused and neglected children in children’s institutions? Pediatrics. 2002;110(6):1226-31. doi: 10.1542/peds.110.6.1226
- Giardino AP, Montoya LA, Leventhal JM. Financing medically-oriented child protection teams in the age of managed health care: a national survey. Child Abuse Negl. 2004;28(1):25-44. doi.org:10.1016/j.chiabu.2003.05.003
- Socolar RR, Fredrickson DD, Block R, Moore JK, Tropez-Sims S, Whitworth JM. State programs for medical diagnosis of child abuse and neglect: case studies of five established or fledgling programs. Child Abuse Negl. 2001;25(4):441-55. doi:org:10.1016/S0145-2134(01)00219-8
- Kairys S, Ricci L, Finkel MA. Funding of child abuse evaluations: survey of child abuse evaluation programs. Child Maltreat. 2006 May;11(2):182-8. doi: 10.1177/1077559505285778. PMID: 16595851.
- National Association of Children’s Hospitals and Related Institutions. Responding to Child Maltreatment: Children’s Hospitals Child Abuse Services 2005 survey results. 2005
- National Association of Children’s Hospitals and Related Institutions. Responding to Child Maltreatment: Children’s Hospitals Child Abuse Services 2008 survey results. 2008
- Children’s Hospital Association. (2012). Survey findings of children’s hospitals’ child abuse services Accessed at https://www.childrenshospitals.org/issues-and-advocacy/population-health/child-abuse/reports/2012/2012-survey-findings-childrens-hospitals-child-abuse-services
- Bachim, A., Culotta, P., Thompson, R., Giardino, A., & Greeley, C. (2023). National Children’s Hospital Child Abuse services survey: 2015 executive summary. Available from https://www.medicpresents.com/download-free-medical-notes/national-childrens-hospital-child-abuse/1293.html
- Peeler E, Dakil S, Culotta P, Giardino A, Greeley C, Bachim A. Financing pediatric hospital child abuse teams in 2015: national survey results. Child Abuse Negl. 2023;139:106114. doi: https://doi.org/10.1016/j.chiabu.2023.106114
- Children’s Hospital Association. Defining the Children’s Hospital Role in Child Maltreatment (2nd Ed). https://xdocs.net/preview/defining-the-childrens-hospital-role-in-child-maltreatment-5e0a57af5c257 2011
- Sister Irene Kravis quote no margin no mission. https://www.forbes.com/sites/sachinjain/2022/04/29/when-margin-becomes-the-mission-healthcares-sometimes-unholy-pursuit-of-profit/
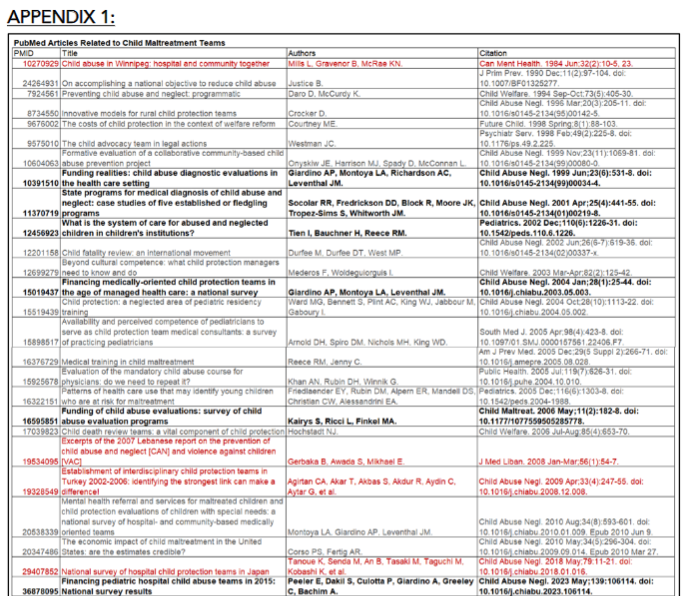
APPENDIX 1:
Bold are included in paper along with the NACHRI/CHA reports; grey are US reports but not relevant to staffing, services offered, or finances of the child maltreatment teams; and red are reports for countries other than the US.