





Genetic Polymorphism of ERAP-1 in Ankylosing Spondylitis
Genetic Polymorphism for the Gene Encoding Endoplasmic Reticulum Aminopeptidase-1 (ERAP-1) in Iraqi Patients with Ankylosing Spondylitis
Muataz Mohammed Al-Taee1,2*
- Department of Biotechnology, College of Science, University of Baghdad, Baghdad, Iraq.
- Department of Medical Laboratory Technology, AL-Nisour University College, Baghdad, Iraq.
OPEN ACCESS
PUBLISHED: 30 September 2024
CITATION: Al-Taee, M., 2024. Genetic Polymorphism for the Gene Encoding Endoplasmic Reticulum Aminopeptidase-1 (ERAP-1) in Iraqi Patients with Ankylosing Spondylitis. Medical Research Archives, [online] 12(9).
https://doi.org/10.18103/mra.v12i9.XXXX
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i9.XXXX
ISSN 2375-1924
ABSTRACT
Ankylosing spondylitis (AS) is a common, highly heritable inflammatory arthritis affecting primarily the spine and pelvis. This study was aimed to investigate the relationship between the rs27044 polymorphism in Endoplasmic reticulum aminopeptidase-1 (ERAP-1) with the susceptibility and severity of AS correlated with some biochemical markers such as hematological parameter (Erythrocytes sedimentation rate (ESR)) and immunological parameters (C-reactive protein (CRP), Human leukocyte antigen-B27 (HLA-B27), Interleukin-6 (IL-6) and Interleukin-23 (IL-23)), and oxidative stress parameters (Glutathione (GSH) and Malondialdehyde (MDA)) in a sample of Iraqi population. A total of 60 blood samples were collected from AS patients required Rheumatology Consultation Clinic in Baghdad Teaching Hospital in Baghdad Governorate. Those patients are males and females with age ranged between 26-32 years for early diagnosed patients (10 samples) and other medically treated patients with age ranged between 22-52 years (50 samples). The rest (30 blood samples) were collected from healthy controls with age ranged between 14-68 years. Results showed that there is a significant increase in Erythrocytes Sedimentation Rate (ESR) as a hematological parameter in newly diagnosed and medically treated patients. For the immunological parameters, results showed that C-reactive protein (CRP) was detected in all serum samples taken from newly diagnosed patients, and 80% positive were detected in medically treated patients in comparison with 100% negative results in healthy controls. On the other hand, Human leukocyte antigen-B27 (HLA-B27) was also detected in all serum samples taken from newly diagnosed patients and 76% positive were recorded in medically treated patients as compared with negatively resulted in healthy controls. For the Interleukins (IL-6 and IL-23), results showed that there is a significant increase in levels of both interleukins in serum samples of newly diagnosed patients compared with healthy controls and medically treated patients, in which any significant difference was recorded. Results of oxidative stress parameters showed that there is a significant decrease in Glutathione (GSH) levels in serum samples of newly diagnosed patients compared with its level in serum sample of controls and medically treated patients, in which significantly not different. Results also showed that there is a significant increase in Malondialdehyde (MDA) levels in serum samples of newly diagnosed patients compared with its levels in healthy controls and medically treated patients, in which no significant difference in MDA levels in serum samples of both groups. Genetic polymorphism of ERAP-1 gene (rs27044 SNP) in exon15 within chromosome 5 was studied. The genomic DNA was extracted from blood samples for controls and AS patients at concentrations of extracted DNA was ranged between 100-200 ng/μl with purity of 1.8-2.0. Exon 15 was amplified by using specific primers showed that a single band of 298 bp was obtained after electrophoresis on agarose gel (2%) represents the complete nucleotide sequence of exon 15. Results showed that the single nucleotide polymorphism (rs27044) was cSNP in all controls, while gSNP was found in 64% of polymorphic AS patients with a significant difference than non-polymorphic AS patients (36%).
Keywords: Endoplasmic reticulum aminopeptidase-1 (ERAP1) gene, ankylosing spondylitis.
1. Introduction
Ankylosing spondylitis (AS) is a chronic and systemic seronegative inflammatory spondyloarthropathy, which causes destruction and fusion of the spinal vertebrae and sacroiliac joints. It has been proposed that the sites of attachment of the ligaments or tendons to the bone, called entheses, are the major target of the inflammatory, traumatic and degenerative pathological changes occurring in AS. Enthesitis is believed to play a primary role in the ligament calcification process, which results in pain. It can lead to reduced flexibility of the spine, and eventually complete loss of spinal mobility, destruction as well as ankylosis (fusion) of the spine and sacroiliac joints (Ghasemi-rad et al., 2015).
Serum and plasma biomarkers have been examined extensively in assessing disease activity, treatment response, and as predictors of radiographic severity. For assessing disease activity, other than C-reactive protein and erythrocyte sedimentation rate, the most work has been in examining cytokines (particularly interleukin 17 and 23), matrix metalloproteinase (MMP) markers (particularly MMP3). For assessing those at the highest risk for radiographic progression, biomarkers of bony metabolism, cartilage and connective tissue degradation products, and adipokines have been most extensively assessed (Reveille J. D., 2015).
Recently, genomic studies of patients with AS have identified and validated other loci aside from the HLA-B27 that are involved in the pathogenesis of this disease. These genes include the endoplasmic reticulum-associated aminopeptidase-1 (ERAP-1), IL-23 receptor (IL-23R), IL-1 receptor (IL-1RII), and two loci that code for unknown genes. The risk attributed to populations with the three known associated genes is 90%, 26%, and 1%, respectively (Reveille et al., 2010).
Endoplasmic Reticulum Aminopeptidase-1 (ERAP-1) is the term currently accepted by the human genome organization (HUGO) nomenclature committee (HGNC), though in the past it was known by such names as endoplasmic reticulum aminopeptidase associated with antigen processing (ERAAP), adipocyte-derived leucine amino peptidase (A-LAP), and aminopeptidase regulated tumor necrosis factor receptor I (TNFRI) shedding (ARTS-1). ERAP-1 is a zinc aminopeptidase belonging to the M1 family of the metallopeptidases with several proposed biological functions that make it a strong candidate in AS (Kochan et al., 2011).
The association of ERAP-1 SNPs with AS can be explained from a functional perspective. The protein ERAP-1 has three known biological functions. First, in the endoplasmic reticulum, ERAP-1 acts as a molecular ruler, trimming peptide antigens to optimal length for binding to MHC class I molecules (Saveanu et al., 2005). Second, the cleavage of cell surface receptors by pro-inflammatory cytokines results in the down-regulation of their intracellular signaling (Cui et al., 2003). Third, ERAP-1 is involved in the activation of macrophages induced by lipopolysaccharide (LPS) and interferon (IFN)-γ (Goto et al., 2011).
In 2007, the Wellcome Trust Case Control Consortium and the Austrao-Anglo-American Spondylitis Consortium (WTCCC-TASC) performed a genetargeted association study of 14500 nsSNPs in 1000 AS cases and 1500 controls. They confirmed the known strong association with the major histocompatibility complex (MHC) and also provided preliminary evidence for several non-MHC associations. Five nsSNPs in ERAP-1 (rs30187, rs27044, rs2887987, rs17482078 and rs10050860) were genotyped, all producing significant associations with AS (Burton et al., 2007).
According to those mentioned above and to determine the relationship between the genetic polymorphism in ERAP-1 gene and the incidence of ankylosing spondylitis in a sample of Iraqi population, this study was aimed to collection of blood samples from patients diagnosed with ankylosing spondylitis, measurement of some inflammatory markers and immunological markers, measurement of some biochemical parameters and markers of oxidative stress, extraction the genomic DNA from Iraqi healthy controls and AS patients, amplification of exon 15 of ERAP-1 by designing a specific primer and then, sequencing the amplified PCR products and determine the presence of genetic polymorphism in this exon.
2. Materials and methods
2.1. SUBJECTS
Blood samples were collected from 60 male and female Ankylosing spondylitis patients (with either newly diagnosed or already treated patients) from Rheumatology consultation clinic in Baghdad Teaching Hospital. The Ankylosing spondylitis patients included 10 newly diagnosed (untreated) patients (8 men and 2 women) with an age range of 26-32 year. Also, another 50 already diagnosed as having Ankylosing spondylitis and currently receiving treatment included 44 men and 6 women with an age range of 22–54 year. The range of diseases duration was between three months to 30 yr. Before blood sampling, all participants were informed about the study objectives, and their consent were obtained. Another blood samples were collected from 30 apparently healthy controls from Al-Harithia laboratory. They included 20 women and 10 men with an age range of 16–68 year.
Medically treated patients were received several types of drugs for curing the disease, such as Methotrexate (MTX), Humera, Prednisolone, Biology, Immuron, Hydroxychloroquine, Enbrel and Salazopyrin. Other patients suffering from Ankylosing spondylitis were not received any medical treatment.
2.2. DETERMINATION OF C-REACTIVE PROTEIN
C-reactive protein (CRP) was determined in serum sample at 6 mg/l or higher causes a visible agglutination on slide of a suspension of latex particles coated with anti-human C-reactive protein.
2.3. HUMAN LEUKOCYTE ANTIGEN B27 (HLA-B27) ELISA KIT
This ELISA kit uses Sandwich-ELISA as the method. The micro ELISA plate provided in this kit has been pre-coated with an antibody specific to HLA-B27. Standards or samples were added to the appropriate micro ELISA plate wells and combined with the specific antibody. Then a biotinylated detection antibody specific for HLA-B27 and Avidin-Horseradish Peroxidase (HRP) conjugate is added to each micro plate well successively and incubated. Free components are washed away. The substrate solution is added to each well. Only those wells that contain HLA-B27, biotinylated detection antibody and Avidin-HRP conjugate will appear blue in color. The enzyme-substrate reaction is terminated by the addition of a sulphuric acid solution and the color turns yellow. The optical density (OD) is measured spectrophotometrically at a wavelength of 450 nm ± 2 nm. The OD value is proportional to the concentration of HLA-B27. One can calculate the concentration of HLA-B27 in the samples by comparing the OD of the samples to the standard curve.
2.4. DETECTION OF INTERLEUKIN-6 (IL-6)
Interleukin 6 (IL-6) was determined in serum samples by using IL-6 ELIAS Kit. This kit uses enzyme-linked immune sorbent assay (ELISA) based on biotin double antibody sandwich technology to assay Human Interleukin 6. Interleukin 6 was added to wells that are pre-coated with Interleukin 6 monoclonal antibody and then incubate. After incubation, anti-Interleukin 6 antibodies labeled with biotin were added to unite with Streptavidin-HRP, which forms the immune complex. Unbound enzymes were removed after incubation and washing, and then substrate A and B were added. The solution will turn blue and change to yellow with the effect of acid. The shades of solution and the concentration of Human Interleukin 6 are positively correlated.
2.5. DETECTION OF INTERLEUKIN-23 (IL-23)
Interleukin 23 (IL-23) in serum samples was determined by using IL-23 ELIAS Kit. This kit uses enzyme-linked immune sorbent assay (ELISA) based on biotin double antibody sandwich technology to assay Human Interleukin 23. Interleukin 23 was added to wells that are pre- coated with Interleukin 23 monoclonal antibody and then incubated. After incubation, anti-Interleukin 23 antibodies labeled with biotin were added to unite with Streptavidin-HRP, which forms the immune complex. Unbound enzymes were removed after incubation and washing, and then substrate A and B were added. The solution will turn blue and change to yellow with the effect of acid. The shades of solution and the concentration of Human Interleukin 23 are positively correlated.
2.6. DETECTION OF GLUTATHIONE (GSH)
Glutathione was detected in blood serum from patients and healthy controls by using GSH ELISA Kit. This kit uses enzyme-linked immune sorbent assay (ELISA) based on biotin double antibody sandwich technology to assay Human glutathione (GSH). Glutathione (GSH) was added to wells that are pre-coated with glutathione (GSH) monoclonal antibody and then incubated. After incubation, anti-glutathione (GSH) antibodies labeled with biotin were added to unite with Streptavidin-HRP, which forms the immune complex. Unbound enzymes were removed after incubation and washing, then substrate A and B was added. The solution will turn blue and change to yellow with the effect of acid. The shades of solution and the concentration of Human glutathione (GSH) are positively correlated.
2.7. DETECTION OF MALONDIALDEHYDE (BUEGE AND AUST, 1978)
- HCl solution (0.25 N): This solution was prepared by adding 2.08 ml of concentrated hydrochloric acid to 98 ml of distilled water.
- Thiobarbituric Acid (TBA) Reagent: This reagent was prepared by dissolving 0.375 g of Thiobarbituric acid (TBA) and 15 g of trichloroacetic acid (TCA) in 100 ml of 0.25 N of hydrochloric acid solution.
- Malondialdehyde assay procedure:
Malondialdehyde (MDA) concentration in serum samples were assayed as follows:
A. Aliquot of 0.5 ml of serum samples were added to 1 ml of TBA reagent and mixed thoroughly, then mixture was incubated at 100°C for 15 minutes.
B. The mixture was centrifuge at 14000 rpm for 10 minutes.
C. After centrifugation, optical density for supernatant was measured at 532 nm against blank of distilled water (0.5 ml) and TBA reagent (1 ml).
D. Malondialdehyde concentration was calculated according to the following formula (Buege and Aust, 1978).
2.8. DNA EXTRACTION
Total genomic DNA was extracted from 25 blood samples collected from Ankylosing spondylitis patients, and from 10 blood samples collected from healthy volunteers. DNA extraction was carried out by using ReliaPrep™ Blood gDNA Miniprep System supplied by Promega / USA protocol.
2.9. PCR PRIMERS
Amplification of endoplasmic reticulum aminopeptidase-1 (ERAP-1) was achieved by using specific primers indicated in Table-1. These primers were supplied by Alpha DNA Company in a lyophilized form of different picomols concentrations. Lyophilized primers were dissolved in a free DNase/RNase water to give a final concentration of 100 pmol/μl as a stock solution. A working solution of 10 pmol/μl of these primers was prepared by adding 10 μl of primer stock solution to 90 μl of deionized distilled water to get a final concentration of 10 pmol/μl.
Table-1: Oligonucleotide primers used for the amplification of ERAP-1
| Primers | Sequence (5′- 3′) | Product Size (bp) |
|---|---|---|
| Forward | CTCAGGCCTTCCTCATCA | 298 |
| Reverse | CAGGGGAGACACTTAAACTT |
2.10. AMPLIFICATION OF ERAP-1 EXON 15
PCR was carried out in a total volume of 50ul. The reaction components are indicated in Table-2. Exon 15 of ERAP-1 gene was amplified by using specific primers in a thermal cycler. Polymerase chain reaction was carried out according to the amplification program shown in Table-3, and then amplification products were analyzed on agarose gel (2%) in presence of 100bp DNA ladder marker.
Table-2: Components of reaction mixture for amplification of exon 15 of ERAP-1
| Component | Volume (μl) |
|---|---|
| Master Mix: TaqDNA Polymerase, dNTPs, MgCl2, and reaction buffer. | 25 |
| Forward Primer | 2.5 |
| Reverse Primer | 2.5 |
| DNA Template | 7.5 |
| D.W. | 12.5 |
Table-3: PCR amplification program for Exon 15 of ERAP-1
| Steps | Temperature (°C) | Time | No. of Cycles |
|---|---|---|---|
| Initial Denaturation | 94 | 5 min. | 1 |
| Denaturation | 94 | 30 sec. | |
| Annealing | 58 | 30 sec. | 40 |
| Extension | 72 | 1 min | |
| Final Extension | 72 | 10 min. | 1 |
2.11. SEQUENCING OF AMPLIFICATION PRODUCTS
Amplification products for exon 15 of the gene ERAP-1 was sent for sequencing to Macrogen Company (USA). Then, the sequencing for these products was compared with the information in gene bank of the National Center for Biotechnology Information (NCBI) for standard ERAP-1 gene, using (Mega-6) software.
2.12. STATISTICAL ANALYSIS
The Statistical Analysis System- SAS (2012) program was used to evaluate difference factors in study parameters. Chi-square test was used to investigate significant comparisons between percentages and the least significant difference –LSD test was used to significant compare between means of the present parameter. Estimation of correlation coefficient between some parameters was performed, as well.
3. Results and Discussion
3.1 LEVEL OF ERYTHROCYTE SEDIMENTATION RATE
Erythrocyte sedimentation rate (ESR) is the most widely used laboratory measure of disease activity in clinical medicine and still remains a useful tool for monitoring inflammatory diseases such as Ankylosing spondylitis (Wolfe et al., 2001). Also it was the most frequently indicator used for detection the inflammatory activity in patients with Ankylosing spondylitis (Wallis et al., 2013).
In this study, ESR was detected in whole blood samples of 60 patients with Ankylosing spondylitis and other 30 healthy control persons. Results indicated in table (3-1) showed that, the level of ESR was significantly increased in medically treated and newly diagnosed Ankylosing spondylitis patients in comparison with its levels in healthy controls (P = 0.0012). The increase in ESR levels in newly diagnosed and treated Ankylosing spondylitis patients refers to the presence of an inflammatory response by the immune system against the disease. This finding agrees with other studies described by Dixon et al (1981); Benjamin et al (2001); Londono et al (2012) who demonstrated higher ESR levels in blood samples of AS patients compared to healthy controls. The failure of various treatments employed to normalize ESR values may be due to the presence of other mechanisms responsible for the pathogenesis of AS not corrected by the current therapy.
Table (3-1): Erythrocyte sedimentation rate in healthy control and Ankylosing spondylitis Patients
| Parameters | Controls N=30 | AS Patients Newly diagnosed N=10 | Treated N=50 |
|---|---|---|---|
| ESR (mm/hr) | 21.07 ± 3.79ᵇ | 58.40±3.04ᵃ | 49.77 ± 11.42ᵃ |
Values are expressed as Mean ± SD. N=Number, different letters indicate a significant difference at P<0.01.
3.2. IMMUNOLOGICAL PARAMETERS
3.2.1. C-reactive protein
C-reactive protein (CRP) and ESR are two currently used biomarkers for the evaluation of inflammatory activity of Ankylosing spondylitis (Spoorenberg et al., 1999).
In this study, Results indicated in table (3-2) showed that C-reactive protein was detected in serum samples of all ten newly diagnosed patients with Ankylosing spondylitis (100.0%), and in the forty patients (80%) among the fifty treated patients. While this protein was not detected in serum samples of all healthy controls (0.00%) with a highly significant difference (P = 0.0001). These results showed that the CRP test is one of the most important immunological biomarkers for the diagnosis of AS, and was highly related to the infection with the disease.
These results are agreed with those obtained by Londono et al (2012) who mentioned that higher CRP levels was present in serum of AS patients compared with healthy controls, and also agreed with Przepiera-Bwdzak et al (2015) who detect high levels of CRP in all patients with AS in comparison with the healthy controls (0.0%).
Table (3-2): levels of C-reactive protein in Iraqi patients with Ankylosing spondylitis and healthy controls
| Parameters | Controls N (%) | AS patients Newly diagnosed N (%) | Treated N (%) |
|---|---|---|---|
| CRP Positive | 0 (0.00) | 10 (100.0) | 40 (80.0) |
| Negative | 30 (100.0) | 0 (0.00) | 10 (20.0) |
Values are expressed as Mean ± SD. N=Number, (%) = Percentage, ** (P<0.01).
3.2.2. Human Leukocyte Antigen B27
Typing for histocompatibility antigen HLA-B27 has been suggested as a clinically valuable diagnostic test for Ankylosing spondylitis (Londoño et al., 2005). A genetic predisposition exists for the development of the disease, as evidenced by its strong association with HLA-B27, especially in the case of AS, where 90% of the patients are positive for this allele (Khan et al., 1992).
In this study, Results indicated in table (3-3) showed that Human Leukocyte Antigen B27 was detected in serum samples of all ten newly diagnosed patients with Ankylosing spondylitis (100.0%) with a highly significant difference (P=0.0001) as compared to the healthy controls, and in serum samples of thirty eight treated patients (76.0%) among 50 treated patients, while this protein was not detected in serum samples of all healthy controls (0.00%) with a highly significant difference (P<0.01). According to these results, the HLA-B27 test was regarded as one of the most important immunological biomarkers in the diagnosis of AS, and was highly related to the infection with the disease.
These findings were agreed with that obtained by Chen et al (2012) who found that the positivity of HLA-B27 test in patients with AS was 99.2%.
Table (3-3): levels of Human Leukocyte Antigen B27 in Iraqi patients with Ankylosing spondylitis and healthy controls
| Parameters | Controls N (%) | AS patients Newly diagnosed N (%) | Treated N (%) |
|---|---|---|---|
| HLA-B27 Positive | 0 (0.00) | 10 (100.0) | 38 (76.0) |
| Negative | 30 (100.0) | 0 (0.00) | 12 (24.0) |
Values are expressed as Mean ± SD. N=Number, (%) = Percentage, ** (P<0.01).
3.2.3. Interleukin-6
Some cytokines such as interleukin-6 (IL-6) and interleukin-23 (IL-23) are considered to be associated with the pathogenesis of chronic inflammatory joint disease (Cauli and Mathieu, 2012). IL-6 is a pleiotropic cytokine that plays role in arthritis but its role in the pathogenesis of AS remains controversial (Hayer et al., 2010).
Levels of IL-6 in Iraqi patients with AS and healthy controls was determined. Results indicated in figure (3-1) showed that the mean level of IL-6 in newly diagnosed and medically treated patients with AS was 258.23 ng/ml and 68.97 ng/ml respectively in comparison with 61.47 ng/ml in healthy controls. On the other hand, results illustrated in figure (3-1) showed that there is a significant increase in serum levels of IL-6 in newly diagnosed Ankylosing spondylitis patients compared with healthy controls (P<0.01). Furthermore, medical treatment of those patients showed no any significantly difference in IL-6 levels at a value compared with that of healthy controls.
The present finding of increasing serum IL-6 levels in newly diagnosed AS patients suggests the presence of an inflammatory response by the immune system against AS. These results were agrees with that obtained by Tarner et al. (2009) and Przepiera-Bwdzak et al. (2015) who found that higher IL-6 levels in serum samples of AS patients compared with healthy controls. According to these results, the level of IL-6 in blood samples was regarded as one of the important biomarkers for detecting AS.
Interleukin-6 was observed to be involved in diverse biological processes, such as the activation of T cells, induction of the acute-phase response, stimulation of the growth and differentiation of hematopoietic precursor cells, and proliferation of synovial fibroblasts results in synovial inflammation and ultimately joints damage (Choy et al., 2001).
It was concluded that elevated serum IL-6 level may be a useful biomarker to detect active AS and disease progression in patients with AS (Figure 3-1).
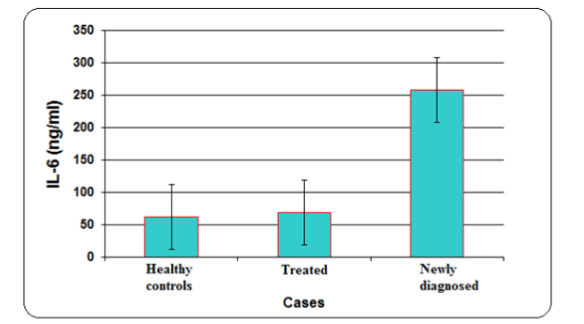
Figure (3-1): Levels of Interleukin-6 in Iraqi patients with Ankylosing spondylitis and healthy controls. The values are means of two biological replicates, and the error bars indicate standard deviation.
3.2.4. Interleukin-23
IL-23 is a heterodimeric proinflammatory cytokine belonging to the IL-6/IL-12 cytokine family and it is produced by dendritic cells, macrophages, keratinocytes, and other antigen-presenting cells. IL-23 plays an important role in the pathogenesis of spondyloarthritis (Singh et al., 2011).
To determine the role of IL-23 in susceptibility to AS, the levels of IL-23 in serum samples of AS patients and healthy controls was determined. Results indicated in figure (3-2) showed that the mean level of IL-23 in newly diagnosed and medically treated patients with AS was 439.25 ng/ml and 134.44 ng/ml respectively in comparison with 134.2 ng/ml in healthy controls. On the other hand, results showed serum levels of IL-23 were significantly increased in newly diagnosed Ankylosing spondylitis patients compared with healthy controls (P<0.01) as shown in figure (3-2). Furthermore, medical treatment of those patients does not cause any significant change in IL-23 levels at a value compared with its level in healthy controls.
The significant increase in serum levels of IL-23 in newly diagnosed AS patients suggests the presence of an inflammatory response by the immune system against AS. These results were agreed with those described in many studies described by Tarner et al (2009), Chen et al (2012) and Przepiera-Bwdzak et al (2015) who found that higher levels of IL-23 in serum samples of AS patients compared with healthy controls.
According to these results, the level of IL-23 in blood samples was regarded as one of the important biomarkers for detecting AS, and it may be a useful biomarker to detect active AS and disease progression.
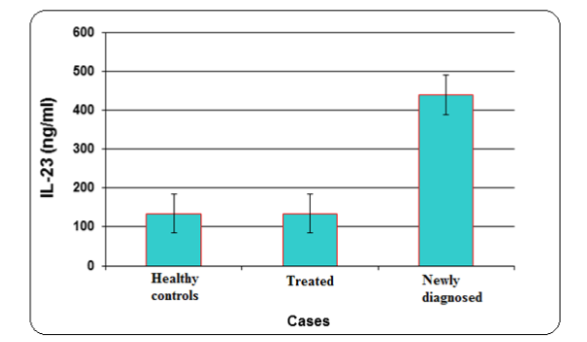
Figure (3-2): Levels of Interleukin-23 in Iraqi patients with Ankylosing spondylitis and healthy controls. The values are means of two biological replicates, and the error bars indicate standard deviation.
3.3. OXIDATIVE STRESS PARAMETERS
Oxidative stress phenomenon can be found as the pathophysiological basis of chronic inflammatory joint diseases like rheumatoid arthritis and Ankylosing spondylitis, conditioning its evolving status (Kalpakcioglu and Senel, 2008). In this study, association of two oxidative stress parameters with the infection of AS were examined.
3.3.1. Serum levels of Glutathione
Glutathione (GSH) is an important non-enzymatic antioxidant factor preventing damage to important cellular components caused by reactive oxygen species such as free radicals and peroxides (Pompella et al., 2003).
Results indicated in figure (3-3) showed that the mean level of GSH in newly diagnosed and medically treated patients with AS was 1.38 ng/ml and 7.10 ng/ml respectively in comparison with 6.74 ng/ml in healthy controls.
In this study, serum levels of GSH were significantly decreased in newly diagnosed Ankylosing spondylitis patients compared with healthy controls (P<0.01) as shown in figure (3-3). Furthermore, medical treatment of those patients revealed no any significant change in GSH levels compared with that of healthy controls. The decrease in serum levels of GSH in newly diagnosed AS patients suggests the presence of an inflammatory response by the immune system against AS. These results agrees with those mentioned by Feijóo et al (2010) who found that lower GSH levels in serum samples of AS patients compared to healthy controls.
According to these results, the level of GSH in blood samples was regarded as one of the important biomarkers for detecting AS.
Intracellular glutathione acts as an antioxidant in several ways. It can reduce peroxides to form H₂O or scavenge directly ROS (Cuzzocrea et al., 2004). It can also act as a chelator of Cu²⁺ and reduces its activity to generate ROS (Halliwell and Gutteridge, 2003).It could be concluded that decreased serum GSH level may be a useful marker to detect active AS and disease progression in patients with AS.
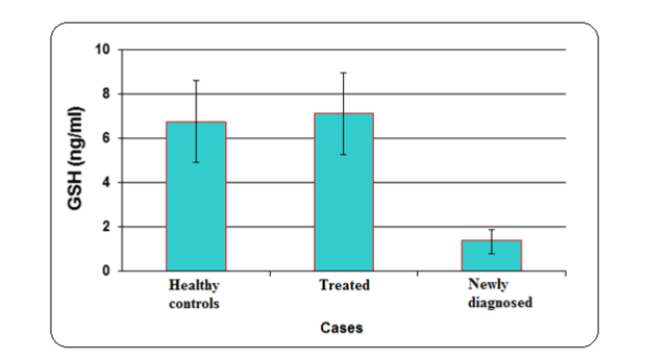
Figure (3-3): Levels of Glutathione in Iraqi patients with Ankylosing spondylitis and healthy controls. The values are means of two biological replicates, and the error bars indicate standard deviation.
3.3.2. Serum levels of Malondialdehyde
Malondialdehyde (MDA) was regarded as a biomarker of lipid peroxidation and accumulation of reactive oxygen species (ROS) in Ankylosing spondylitis patients and control subjects. Reactive oxygen species play an important role in the pathogenesis of inflammatory joint diseases like rheumatoid arthritis and Ankylosing spondylitis (Ozgocmen et al., 2001).
In this study, the role of MDA in susceptibility to AS was examined. Results indicated in figure (3-4) showed that the mean level of MDA in newly diagnosed and medically treated patients with AS was 1.39 nmol/L and 0.289 nmol/L respectively in comparison with 0.266 nmol/L in healthy controls.
On the other hand, serum levels of MDA were significantly increased in newly diagnosed Ankylosing spondylitis patients compared with healthy controls (P<0.01) as shown in figure (3-4). Furthermore, medical treatment of those patients revealed no any significant change in MDA levels at a value compared with healthy controls. The increase of serum MDA levels in newly diagnosed AS patients was due to the inflammatory response by the immune system against AS. These results agrees with those mentioned by Feijóo et al (2010) who referred that higher MDA levels in serum of AS patients was recorded compared to the healthy controls.
According to these results, the level of MDA in blood samples was regarded as one of the important biomarkers for detecting AS, and it could be concluded that the levels of MDA in serum samples is a useful biomarker to detect active AS and disease progression.
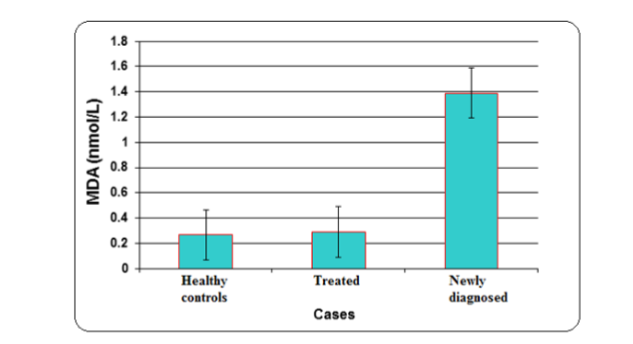
Figure (3-4): Levels of Malondialdehyde in Iraqi patients with Ankylosing spondylitis and healthy controls. The values are means of two biological replicates, and the error bars indicate standard deviation.
3.4. GENOMIC DNA EXTRACTION
In order to study the genetic polymorphism in Iraqi patients with Ankylosing spondylitis, genomic DNA was extracted from blood samples of patients and healthy controls by using ReliaPrep™ Blood gDNA Miniprep System (Promega / USA).
Results indicated in figure (3-5) showed a sharp DNA bands obtained after extraction and electrophoresis on agarose gel (0.7%). The concentration of DNA solution extracted from all samples was ranged between 200-400 μg/ml, while the purity was ranged between 1.8-2.0. This purity and concentration of DNA solutions were suitable and recommended for further genetic analysis by using PCR technique (Boesenberg-Smith et al., 2012).
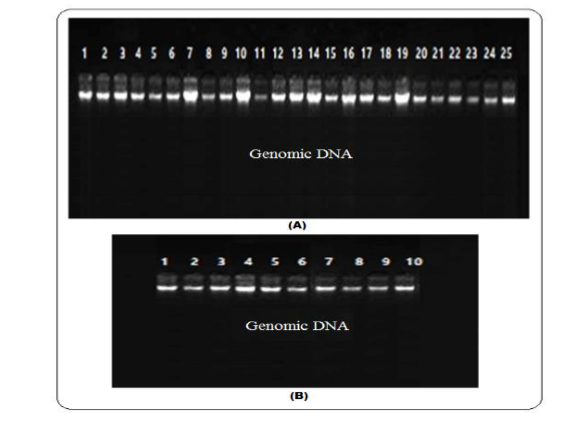
Figure (3-5): Gel electrophoresis of genomic DNA on agarose gel (0.7%) for 1 hour at 5 v/cm. (A): DNA extracted from blood sample of patients with Ankylosing spondylitis. (B): DNA extracted from blood sample of healthy controls.
3.5. GENETIC POLYMORPHISM IN ERAP1 GENE
Endoplasmic reticulum aminopeptidase-1 (ERAP1) gene is one of the important non-HLA genes associated with susceptibility of Ankylosing spondylitis. Single nucleotide polymorphisms (SNPs) in ERAP1 gene, such as rs27044, are highly associated with the disease in several ethnic populations (Zambrano-Zaragoza et al., 2013). Several studies mentioned that the most effective genetic risk outside of the HLA region is a functional single nucleotide polymorphism in the ERAP1 gene which is a C→G substitution (rs27044), which results in a substitution of Glutamine (Q) for Glutamic acid (E) at codon 671 (Wang et al., 2012).
In this study, exon 15 of ERAP1 was amplified in DNA solution extracted from each blood samples of patients with Ankylosing spondylitis and healthy controls. Polymerase chain reaction was achieved under optimum amplification conditions by using specific primers indicated in (2.2.4.). Results illustrated in figure (3-6) showed that the amplified products were appeared as clear bands after electrophoresis on agarose gel (2%) with molecular size of 298 base pair for each blood sample obtained from healthy controls, newly diagnosed AS patients and medically treated patients. These fragments represent the reagion of exon 15 for ERAP1 gene located on short arm of chromosome 5 (Alvarez-Navarro and López de Castro, 2014).
The real molecular size of this exon was 184 bp in length as mentioned in (NCBI: http://www.ncbi.nlm.nih.gov), while the molecular size of the amplified fragment was 298 bp and that’s due to the nucleotide sequences of primers designed in this study which was centered on the aplification of the completed sequence of exon 15 in addition to the two border sequences located on either sides of the exon.
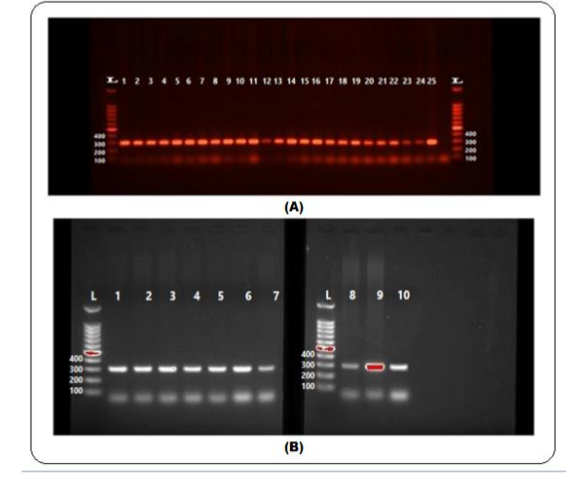
Figure (3-6): Gel electrophoresis for PCR products of ERAP1 exon 15 on agarose gel (2%) after electrophoresis for 1 hour at 5v/cm volt in the presence of 1 kb DNA Ladder marker. (A): PCR products for amplified DNA extracted from blood samples of patients with Ankylosing spondylitis. (B): PCR products for amplified DNA extracted form blood samples of healthy controls.
In this study, twenty five Iraqi patients with Ankylosing spondylitis were recruited to investigate the relationship between rs27044 SNP in exon 15 of ERAP1 gene and the severity of the disease in compared with ten healthy controls.
3.5. Sequencing of Amplified exon 15 of ERAP1 gene
To examine the role of the ERAP1 SNP (rs27044) polymorphism in disease susceptibility and severity in Iraqi population with Ankylosing spondylitis, because this (rs27044) SNP is the most important risk factor for susceptibility to Ankylosing spondylitis (Szczypiorska et al., 2011). Exon 15 who was 184 base pair in length was selected to study the genetic polymorphism in this gene.
The complete nucleotide sequence of ERAP1, exon 15 was determined for genotyping the genetic polymorphism in this exon. Results of sequencing illustrated in figure (3-7) showed the complete nucleotide sequence of this exon in healthy controls and the position of the expected rs27044 SNP that may be associated with the incidence of Ankylosing spondylitis. Furthermore, the complete nucleotide sequence of this exon and the position of the expected SNP in reference sequence of ERAP1 recorded in (NCBI Reference Sequence: ERAP1 ID: 51752) was illustrated in figure (3-8).
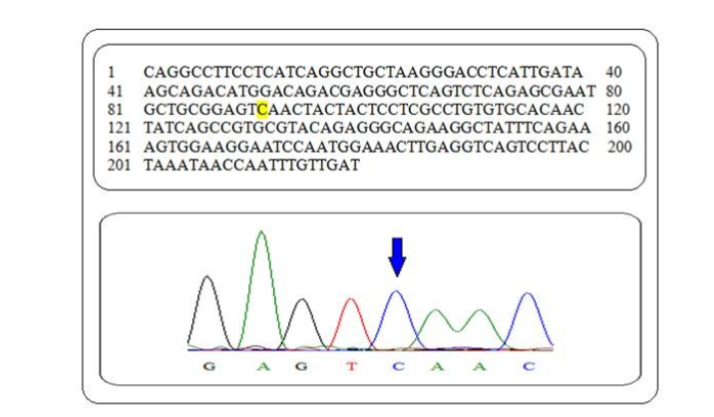
Figure (3-7): Nucleotide sequence of exon 15 of ERAP1 in healthy controls group. Yellow letter indicates the position (96144608) of expected SNP in a sample of Iraqi population.
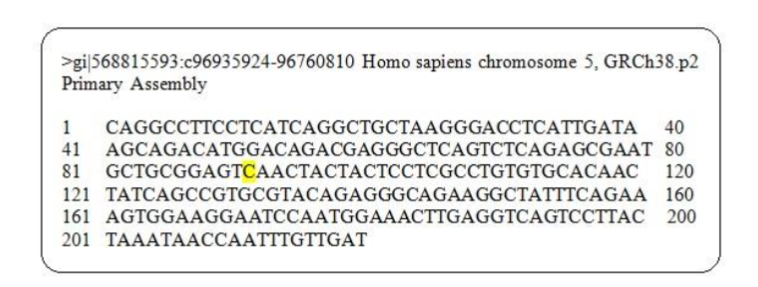
Figure (3-8): NCBI Reference sequence of exon 15 of ERAP1 gene. Yellow letter indicated the position (96144608) of the expected rs27044 SNP.
3.6. NUCLEOTIDE SEQUENCE ALIGNMENT OF THE AMPLIFIED EXON 15 OF ERAP1 GENE
The results of the sequence analysis was analyzed by blastn in the National Center Biotechnology Information (NCBI) online at (http://www.ncbi.nlm.nih.gov) and BioEdit program to detect rs27044 polymorphism in exon 15 of ERAP1 gene. Results illustrated in figure (3-9) and table (3-5) showed the nucleotide alignment and the position of the cytosine (C) nucleotide of healthy control group was matched with cytosine (C) nucleotide in reference sequence mentioned in NCBI, that showed 100% identity, under sequence ID: ref|NG_027839.1| from 35907-36126 number of nucleotide from Homo sapiens endoplasmic reticulum aminopeptidase 1 (ERAP1).
Figure (3-9): Alignment between the nucleotide sequence of healthy control samples of Iraqi and reference sequence. Query represents healthy control samples; Subject represent of database of National Center for Biotechnology Information (NCBI). Yellow letters indicates the position of matched SNP.
On the other hand, results of the nucleotide sequence for ERAP1 exon 15 in Iraqi patient with Ankylosing spondylitis illustrated in figure (3-10) and table (3-4) showed that 9 (36%) out of 25 patients were genotyped as homozygous CC and non-polymorphic as compared to the healthy controls because the expected SNP (rs27044) does not occur in exon 15 sequence understudy, hence the Cytosine nucleotide was located in the same position as in the healthy controls without any base substitution to other nucleotides compared to reference sequence (figure (3-8)). These results are also observed in other ethnic populations such as some Taiwanese population which were non-polymorphic in their nucleotide sequence of this exon (Wang et al., 2012).
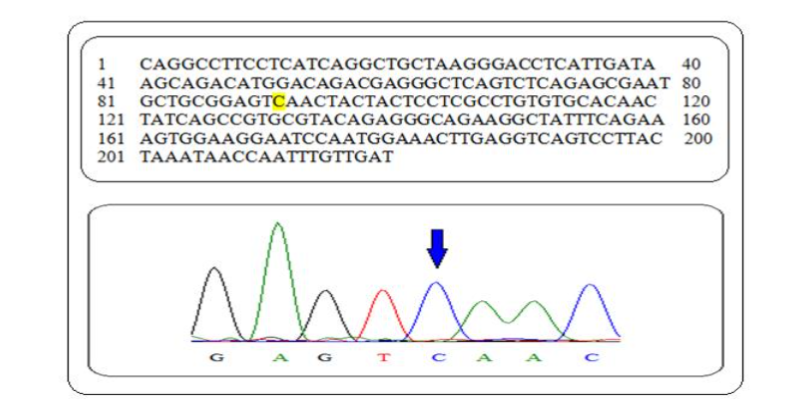
Figure (3-10): Nucleotide sequence of exon 15 of ERAP1 in non-polymorphic Ankylosing spondylitis patients group. Yellow letter indicates the position (96144608) of SNP in Iraqi population.
Table (3-4): Genotyping and alleles frequency in Ankylosing spondylitis patients and healthy controls
| Sample | No. | CC (%) | GC (%) | GG (%) | C | G |
|---|---|---|---|---|---|---|
| Controls | 10 | 10 (100.00) | 0 (0.00) | 0 (0.00) | 1.00 | 0.00 |
| AS Patients | 25 | 9 (36.00) | 16 (64.00) | 0 (0.00) | 0.68 | 0.32 |
Results illustrated in figure (3-11) and table (3-5) showed the nucleotide alignment and the position of the C nucleotide (cSNP) of non-polymorphic Ankylosing spondylitis patients matched with C nucleotide in reference sequence mentioned in NCBI, showed that 100% identity, under sequence ID: ref|NG_027839.1| from 35907-36126 number of nucleotide from Homo sapiens endoplasmic reticulum aminopeptidase 1 (ERAP1).
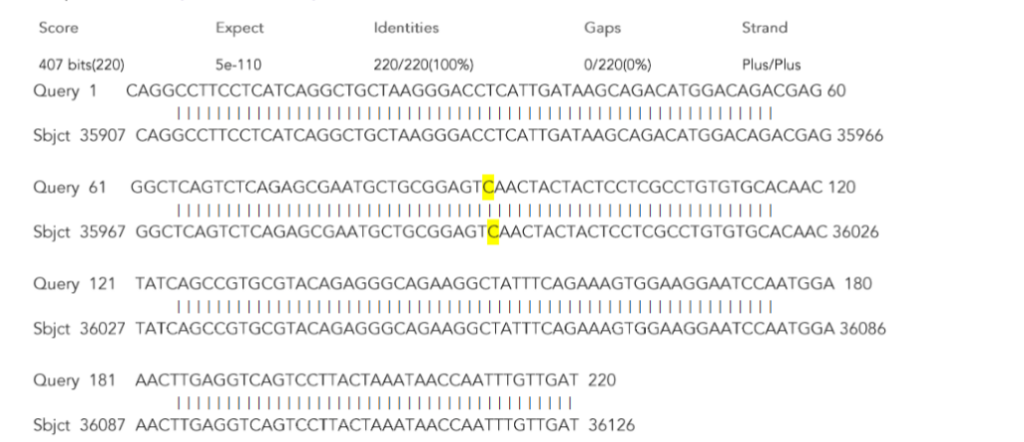
Figure (3-11): Alignment between the nucleotide sequence non-polymorphic Ankylosing spondylitis patients and reference sequence. Query represents non-polymorphic patient samples; Subject represent of database of National Center for Biotechnology Information (NCBI). Yellow letters indicates the position of matched SNP.
These results were also observed in figure (3-12) that show the nucleotide sequence alignment between ERAP1 gene, exon 15 in those patients and Iraqi healthy controls with 100% identity, from 1-220 number of nucleotide from Homo sapiens endoplasmic reticulum aminopeptidase 1 (ERAP1). This result was agreed with (Szczypiorska et al., 2011) who mentioned that a nucleotide sequence of ERAP1, exon 15 in a sample of Ankylosing spondylitis patients was identical to healthy controls and reference sequence without occurring any genetic variation or single nucleotide polymorphism in their sequences.
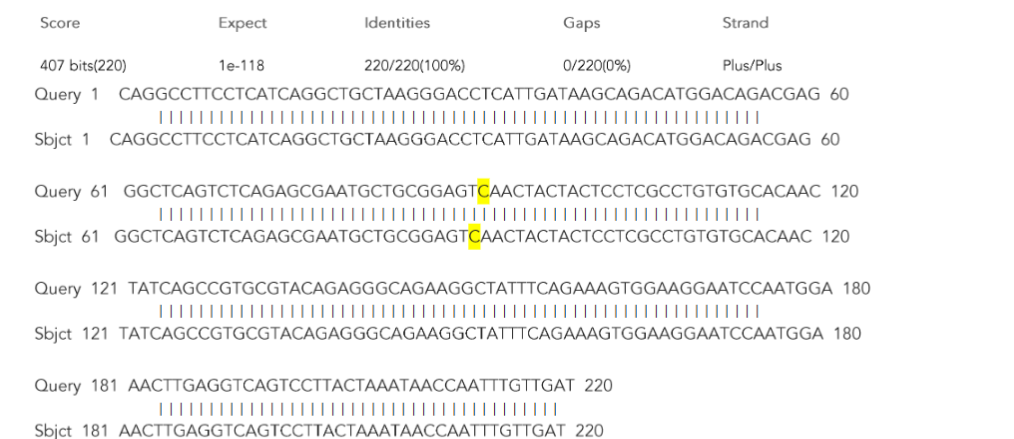
Figure (3-12): Alignment between the nucleotide sequence for ERAP1 (Exon 15) in Iraqi healthy controls and non-polymorphic Ankylosing spondylitis patients. Query represents healthy control samples; Sbject represent non-polymorphic patients. Yellow letters indicates the position of matched SNP.
On the other hand, results illustrated in figure (3-13) and table (3-4) also showed that 16(64%) of Iraqi patients with Ankylosing spondylitis were genotyped as heterozygous GC and were positive for rs27044 SNP exon 15 of ERAP1, as cytosine nucleotide was substituted by guanine.
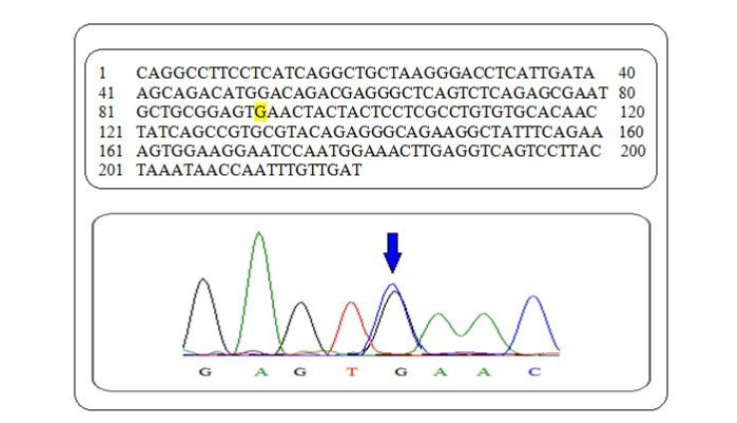
Figure (3-13): Nucleotide sequence of exon 15 of ERAP1 in Ankylosing spondylitis patients group. Yellow letter indicates the position of SNP in Iraqi population.
Furthermore, results illustrated in figure (3-14) and table (3-5) showed the nucleotide sequence alignment and the position of the C nucleotide (cSNP) of polymorphic Ankylosing spondylitis patients matched with C nucleotide in reference sequence mentioned in NCBI, with 99% identity, under sequence ID: ref|NG_027839.1| from 35907-36126 number of nucleotide from Homo sapiens endoplasmic reticulum aminopeptidase 1 (ERAP1).
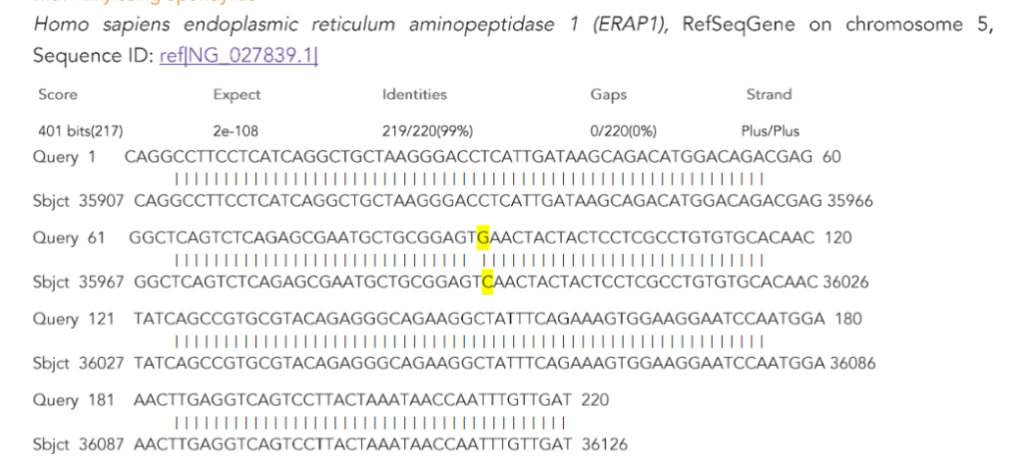
Figure (3-14): Alignment between the nucleotide sequence of polymorphic Ankylosing spondylitis patients and reference sequence. Query represents polymorphic patient samples; Subject represent of database of National Center for Biotechnology Information (NCBI). Yellow letters indicates the position of matched SNP.
These results also shown in figure (3-15), with 99% identity, from 1-220 number of nucleotide from Homo sapiens endoplasmic reticulum aminopeptidase 1 (ERAP1), the cSNP allele carriers was substituted with gSNP in those 16 patients who was significantly different (P<0.01) than other nine patients who were the gSNP was not occur in the sequence of the gene exon 15 as indicated in figure (3-10).
Table (3-5): Sequencing ID in gene bank, identity, expect, score and range of DNA sequence obtained from National Center for Biotechnology Information (NCBI)
| No. | Accession number | Identity | Expect | Score | Range | No of samples |
|---|---|---|---|---|---|---|
| 1 | ref | NG_027839.1 | 100 % | 5e-110 | 407 | |
| 2 | ref | NG_027839.1 | 100 % | 5e-110 | 407 | |
| 3 | ref | NG_027839.1 | 99% | 2e-108 | 401 |
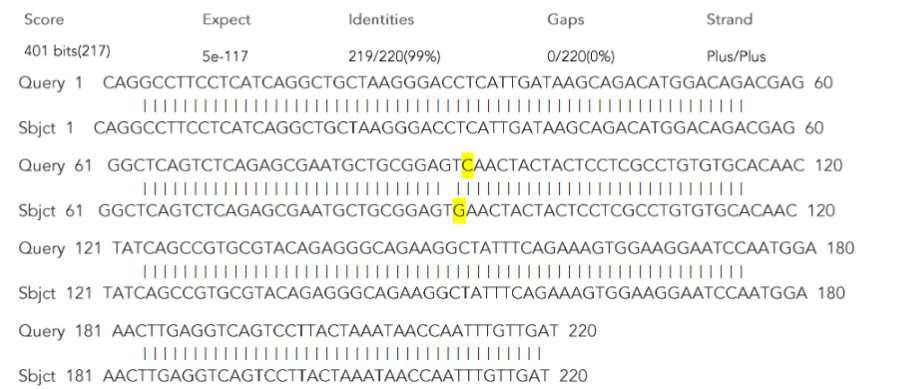
Figure (3-15): Alignment between the nucleotide sequence for ERAP1 (Exon 15) in Iraqi healthy controls and polymorphic Ankylosing spondylitis patients. Query represents healthy control samples; Sbject represent polymorphic patients. Yellow letters indicates the position of matched SNP.
3.7. ALIGNMENT OF EXON 15 AMINO ACIDS
The amino acids sequence encoded by exon 15 in ERAP1 gene, in healthy controls and Iraqi patients with Ankylosing spondylitis were examined and compared with the reference sequence recorded in NCBI. Results illustrated in figure (3-16a) and table (3-6) showed the amino acids alignment between healthy controls and reference sequence, under sequence ID: pdb|3RJO|A, and the position of amino acid (Glutamine, Q) related to the expected rs27044 SNP that may be occurred in this exon. These results showed that there is no any change in the sequence of amino acids (100% identity) between healthy controls and reference sequence. On the other hand, results illustrated in figure (3-16b) and table (3-6) also showed that the amino acid (Glutamine, Q) related to the expect rs27044 SNP was the same in non-polymorphic Iraqi patients with ankylosing spondylitis and reference sequence (100% identity) because those patients does not suffering from any polymorphism as showed in figure (3-11).
Amino acid alignment between Iraqi patients with Ankylosing spondylitis (gSNP) and reference ERAP1, under sequence ID: pdb|3RJO|A, was shown in figure (3-16c) and table (3-6). As a consequence of the substitution of Cytosine by Guanine in exon 15 of ERAP1 gene in those patients, the amino acid sequence result from the wild-type allele was changed, and the amino acid encoded by the original codon was changed to another codon encoding to different amino acid as Glutamine (Q) was substituted by Glutamic acid (E). occurrence of transversion mutation in this position causing missense mutation leading to change neutral, polar amino acid (Gln) to negatively charged, polar aliphatic amino acid (Glu) as indicated in table (3-7) may alter the structure and function of ERAP1 enzyme may associated with the incidence of Ankylosing spondylitis as the malfunctioning of ERAP1 would lead to either an increase or decrease in the number of cell surface receptors available for cytokine (IL-6 and IL-23), thus propitiating pro-inflammatory effects and finally raising disease susceptibility to Ankylosing spondylitis (Zambrano-Zaragoza et al., 2013). This alteration in ERAP1 structure may cause the evaluation of cytokines levels (Interlukin-6 and Interlukin-23) (Cui et al., 2003) and immunological parameters levels (C-reactive protein and HLA-B27) as well as the change in oxidative stress parameters levels (Malondialdehyde and Glutathione). Furthermore this SNP was a risk factor for the susceptibility to the disease because this change revealed a highly response for the infection with this disease as it was mentioned by (Harvey et al., 2009).
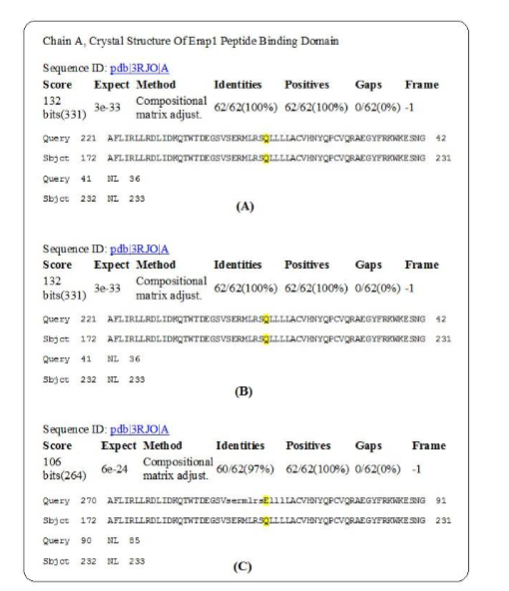
Figure (3-16): Alignment of amino acid encoded by exon 15 of ERAP1 gene in Ankylosing spondylitis Iraqi patients (Query) and with the reference sequences (Sbject) recorded by National Center Biotechnology Information (NCBI). Yellow letters indicates the position of the expected polymorphic amino acid. (A): Healthy controls. (B): Non-polymorphic patients. (C): Polymorphic patients.
These results agree with those obtained by (Szczypiorska et al., 2011) who mentioned that cSNP substituted with gSNP in a sample of Spanish population. These results also agree with those obtained by Wang et al., 2012) who mentioned that cSNP substituted with gSNP in a sample of Taiwanese population.
Table (3-6): Sequencing ID in gene bank, identity, range and expect of amino acid sequence obtained from National Center Biotechnology Information (NCBI)
| No. | Accession number | Identity | Range | Expect |
|---|---|---|---|---|
| 1 | pdb | 3RJO | A | 100 % |
| 2 | pdb | 3RJO | A | 100 % |
| 3 | pdb | 3RJO | A | 97% |
Table (3-7): Type of polymorphism in Homo sapiens endoplasmic reticulum aminopeptidase 1 (ERAP1)
| Type of substitution | Predicted effect | Amino acid change | No. of patient (%) | Nucleotide change | Location of Cod in gene bank | Location of polymorphic nucleotide |
|---|---|---|---|---|---|---|
| Transversion | Missense | Glutamine (Q) / Glutamic acid (E) | 16 (64 |
Conflict of Interest:
None
Funding Statement:
None.
Acknowledgements:
None.
References
• Ghasemi-rad, M.; Attaya, H.; Lesha, E.; Vegh, A.; Maleki-Miandoab, T.; Nosair, E.; Sepehrvand, N.; Davarian, A.; Rajebi, H.; Pakniat, A.; Fazeli, S. and Mohammadi, A. (2015). Ankylosing spondylitis: A state of the art factual backbone. World J Radiol September 28; 7(9): 236-252.
• Reveille, J.D. (2015). Biomarkers for diagnosis, monitoring of progression, and treatment responses in ankylosing spondylitis and axial spondyloarthritis. Clin Rheumatol. 34(6): 1009–1018. doi: 10. 1007/s 10067-015-2949-3.
• Reveille, J.D.; Sims, A.M.; Danoy, P.; Evans, D.M.; Leo, P. and Pointon, J.J. et al. (2010). Genome-wide association study of ankylosing spondylitis identifies non-MHC susceptibility loci. Nat Genet; 42(2):123–7.
• Kochan, G.; Krojer, T. and Harvey, D. (2011). Crystal structures of the endoplasmic reticulum aminopeptidase-1 (ERAP1) reveal the molecular basis for N-terminal peptide trimming. Proceedings of the National Academy of Sciences of the United States of America, vol. 108, no. 19, pp.7745–7750.
• Saveanu, L.; Carroll, O. and Lindo, V. (2005). Concerted peptide trimming by human ERAP1 and ERAP2 aminopeptidase complexes in the endoplasmic reticulum. Nature Immunology, vol.6, no.7, pp.689 –697.
• Cui, X.; Rouhani, F.N.; Hawari, F. and Levine, S.J. (2003). An aminopeptidase, ARTS-1, is required for interleukin-6receptor shedding. Journal of Biological Chemistry. vol. 278, no. 31, pp. 28677–28685.
• Goto, Y.; Ogawa, K.; Hattori, A. and Tsujimoto, M. (2011). Secretion of endoplasmic reticulum aminopeptidase 1 is involved in the activation of macrophages induced by lipopolysaccharide and interferons. Journal of Biological Chemistry. vol. 286, no. 24, pp.21906–21914.
• Burton, P.R.; Clayton, D.G.; Cardon, L.R.; Craddock, N.; Deloukas, P.; Duncanson, A.; Kwiatkowski, D.P.; McCarthy, M.I.; Ouwehand, W.H. and Samani, N.J. et al. (2007). Association scans of 14,500 non-synonymous SNPs in four diseases identifies autoimmunity variants. Nat. Genet., 39, 1329–1337.
• SAS, (2012). Statistical Analysis System, User’s Guide. Statistical. Version 9.1th ed. SAS. Inst. Inc. Cary. N.C. USA.
• Wolfe, F. and Pincus, T. (2001). The level of inflammation in rheumatoid arthritis is determined early and remains stable over the long term course of the illness. J Rheumatol; 28:1817-1824.
• Wallis, D.; Haroon, N.; Ayearst, R.; Carty, A. and Inman, R.D. (2013). Ankylosing spondylitis and nonradiographic axial spondyloarthritis: part of a common spectrum or distinct diseases? J Rheumatol. 40(12):2038–2041. [PubMed: 24187102].
• Dixon, J.S.; Bird, H.A. and Wright, V. (1981). A comparison of serum biochemistry in ankylosing spondylitis, seronegative and seropositive rheumatoid arthritis. Annals of the Rheumatic Diseases, 40, 404-408.
• Benjamin, M. and Ralphs, J.R. (2001). Entheses the bony attachments of tendons and ligaments. Ital J Anat Embryol; 106: 151157 [PMID: 11729950].
• Londono, J.; Romero-Sanchez, M.C.; Torres, V.G.; Bautista, W.A.; Fernandez, D.J.; Quiroga, J.A.; Valle-Oñate, R.; Santos, A.M. and Medina, J.F. (2012). The association between serum levels of potential biomarkers with the presence of factors related to the clinical activity and poor prognosis in spondyloarthritis. Rev Bras Reumatol; 52(4):529-544.
• Spoorenberg, A.; van der Heijde, D.; de Klerk, E.; Dougados, M.; de Vlam, K.; Mielants, H.; van der Tempel, H. and van der Linden, S. (1999). Relative value of erythrocyte sedimentation rate and C-reactive protein in assessment of disease activity in ankylosing spondylitis. J Rheumatol. 26(4):980–984. [PubMed: 10229432].
• Przepiera-Bwdzak, H.; Fischer, K. and Brzosko, M. (2015). Serum IL-6 and IL-23 Levels and Their Correlation with Angiogenic Cytokines and Disease Activity in Ankylosing Spondylitis, Psoriatic Arthritis, and SAPHO Syndrome. Hindawi Publishing Corporation Mediators of Inflammation Volume 2015, Article ID 785705, 7 pages. http://dx.doi.org/10.1155/2015/785705
• Londoño, J.; González, L.; Ramírez, A.; Santos, P.; Avila, L. and Santos, A. et al (2005). Caracterización de las espondiloartropatías y determinación de factores de mal pronostico en una población de pacientes colombianos. Rev Colomb Reumatol, 12(3):195–207.
• Khan, M.A. and Kellner, H. (1992). Immunogenetics of spondylo-arthropathies. Rheum Dis Clin North Am, 18(4):837–64.
• Chen, W.S.; Chang, Y.S.; Lin, K.C.; Lai, C.C.; Wang, S.H. and Hsiao, K.H. (2012). Association of serum interleukin-17 and interleukin-23 levels with disease activity in Chinese patients with ankylosing spondylitis. J Chin Med Assoc. 75(7):303–308. [PubMed: 22824043].
• Tarner, H.; Müller-Ladner, U.l.f.; Uhlemann, C. and Lange, U. (2009). The effect of mild whole-body hyperthermia on systemic levels of TNF-alpha, IL-1beta, and IL-6 in patients with ankylosing spondylitis. Clin Rheumatol, 28:397–402.
• Cauli, A. and Mathieu, A. (2012). Th17 and interleukin 23 in the pathogenesis of psoriatic arthritis and spondyloarthritis. Journal of Rheumatology, vol.39,no.89,pp.15–18.
• Hayer, S.; Niederreiter, B.; Nagelreiter, I.; Smolen, J. and Redlich, K. (2010). Interleukin 6 is not a crucial regulator in an animal model of tumour necrosis factor-mediated bilateralsacroiliitis. Annals of the Rheumatic Diseases, vol.69,no.7, pp.1403–1406.
• Choy, E.H. and Panayi, G.S. (2001). Cytokine pathways and joint inflammation in rheumatoid arthritis. N Engl J Med Mar 22; 344(12):907-916.
• Singh, A.K.; Misra, R. and Aggarwal, A. (2011). Th-17 associated cytokines in patients with reactive arthritis/undifferentiated spondylo-arthropathy. Clinical Rheumatology, vol.30, no.6, pp.771–776.\
• Kalpakcioglu, B. and Senel, K. (2008). The interrelation of glutathione reductase, catalase, glutathione peroxidase, superoxide dismutase, and glucose-6-phosphate in the pathogenesis of rheumatoid arthritis. Clin Rheumatol. 27(2):141-5.
• Pompella, A.; Visvikis, A.; Paolicchi, A.; De Tata, V.; Casini, A.F. (2003). The changing faces of glutathione, a cellular protagonist. Biochem. Pharmacol. 66, 1499-1503. 10. 1016/S0006-2952 (03) 00504-5.
• Feijóo, M.; Túnez, I.; Ruiz, A.; Tasset, I.; Muñoz, E. and Collantes, E. (2010). Oxidative stress biomarkers as indicator of chronic inflammatory joint diseases stage. Reumatol Clin; 6(2):91–94.
• Cuzzocrea, S.; Thiemermann, C. and Salvemini, D. (2004). Potential Therapeutic Effect of Antioxidant Therapy in Shock and Inflammation. Current Medicinal Chemistry 11, 1147-1162.
• Halliwell, B. and Gutteridge, J.M.C. (2003). Free Radicals in Biology and Medicine. (Oxford University Press: Oxford, UK).
• Ozgocmen, S.; Sogut, S.; Ardicoglu, O.; Fadillioglu, E.; Pekkutucu, I. and Akyol, O. (2004). Serum nitric oxide, catalase, superoxide dismutase, and malondialdehyde status in patients with ankylosing spondylitis. Rheumatol Int 24, 80-83.
• Boesenberg-Smith, K.A.; Mohammad, M.; Pessarakli, M.D. and Donna, M.W. (2012). Assessment of DNA Yield and Purity: an Overlooked Detail of PCR Trouble shoots in. Clinical Microbiology Newsletter. Vol. 34, No. 1.
• Zambrano-Zaragoza, J.F.; Agraz-Cibrian, J.M.; González-Reyes, C.; Jesús-Durán, A. and Vibanco-Pérez, N. (2013). Ankylosing Spondylitis: From Cells to Genes. Hindawi Publishing Corporation International Journal of Inflammation. Article ID501653, 16 pages.
• Wang, C.; Ho, H.; Chang, S.; Wu, Y.; Lin, J.; Chang, P.; Wu, J. and Chen, J. (2012). ERAP1 genetic variations associated with HLA-B27 interaction and disease severity of syndesmophytes formation in Taiwanese ankylosing spondylitis. Arthritis Research and Therapy, 14:R125.
• Alvarez-Navarro, C.l. and López de Castro, J.A. (2014). ERAP1 structure, function and pathogenetic role in ankylosing spondylitis and other MHC-associated diseases. Mol Immunol. Jan; 57(1):12-21.
• Szczypiorska, M.; Sanchez, A.; Bartolome, N.; Arteta, D.; Sanz, J. and Brito, E. (2011). ERAP1 polymorphisms and haplotypes are associated with ankylosing spondylitis susceptibility and functional severity in a Spanish population. Rheumatology (Oxford). 50:1969-75.
• Harvey, D.; Pointon, J.J.; Evans, D.M.; Karaderi, T.; Farrar, C.; Appleton, L.H.; Sturrock, R.D.; Stone, M.A.; Oppermann, U.; Brown, M.A. and Wordsworth, B.P. (2009). Investigating the genetic association between ERAP1 and ankylosing spondylitis. Human Molecular Genetics 18, 4204–4212.