

High-Dose Vitamin C in Septic Burn Patients: Outcomes
High dose of Acid ascorbic improves haemodynamic state in septic burn patients?
A. Mokline, 1,2,3,. R. Nachi1,2,. H. Fraj1,2,3., M. Gargouri2,4, AA. Messadi1,2,3,
- Tunis University El Manar, Faculty of Medicine of Tunis. Tunisia
- Intensive Burn Care Department of Tunis. Burn and Trauma Center. Tunis. Tunisia
- UR22SP03 Pharmacy service. Burn and Trauma Center. Tunis. Tunisia
OPEN ACCESS
PUBLISHED: 31 March 2025
CITATION: Mokline, A., Nachi, R., et al., 2025. High dose of Acid ascorbic improves haemodynamic state in septic burn patients? Medical Research Archives, [online] 13(3). https://doi.org/10.18103/mra.v13i3.6415
COPYRIGHT © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i3.6415
ISSN 2375-1924
ABSTRACT
Introduction: Sepsis remains a serious and life-threatening condition with high morbidity and mortality. It is marked by imbalance between increased production of free radicals and insufficient neutralization by endogenous antioxidants, including vitamin C. This causes a spread of oxidation reactions and contributes to organ failure. Although this imbalance has been proven to be more marked in burn patients, few studies have focused on the intake of vitamin C in this population.
Objective: Assess hemodynamic impact of high dose vitamin C (100 mg/weight/day) in septic burn patients.
Methods: Case-control study conducted in intensive burn care department in Tunisia during 28 months (July 2019-October 2021). Were included adult burns presenting sepsis or septic shock (as defined in Sepsis 3). Were excluded pregnant woman, patients with history of lithiasis or vesico-renal calculus, of hemochromatosis or G6PD deficiency, and those on long-term vitamin C or glucocorticoids. Only one septic episode was considered per patient during his hospitalization. After inclusion, ascorbic acid was prescribed at a dose of 100 mg/weight/day in 3 doses over 4 days. The vitamin C group was compared with a retrospective group (non-vitamin C) from the same center matched in terms of age, sex, total body surface area (TBSA) and burn severity. Therapeutic management of sepsis was similar for 2 groups in terms of fluid resuscitation with same hemodynamic objectives (hourly output at 0.5cc to 1cc/weight and MAP > 65 mmHg). The primary endpoint was the impact of Vit C on hemodynamic state evaluated by fluid resuscitation, dose, and duration of catecholamines.
Results: During study period, 100 patients were included divided into 2 groups: G1 (Vit C+ ; n= 50) and G2 (Vit C- : n= 50). Patients of two groups were comparable in terms of sex, age and severity of burns. Administration of vitamin C reduced fluid balance at day 3 (2 ml/weight/day for G1 vs 13 ml/weight/ day for G2; p= 0,008), reduced significantly doses of noradrenaline at day 3 (1,8 mg/h vs 3,5 mg/h ; p= 0,01), and shortened duration of noradrenaline dependence (4 days for G1 vs 4,84 days for G2 ; p= 0,28) in septic shock burns. No ascorbic acid-related adverse events were identified in the treatment group during the study.
Conclusion: High-dose vitamin C therapy was associated with reduced fluid balance, doses of noradrenaline and duration of dependency in burn patients with septic shock during the first 3 days of sepsis.
Keywords
Vitamin C, sepsis, burn patients, hemodynamic state, catecholamines
INTRODUCTION
Sepsis remains a major public health problem, and economic burden in the world. It leads to a systemic inflammatory response by the host response to infection, with the release of pro- and anti-inflammatory mediators and a cytokine storm responsible for organ dysfunction. Management of sepsis and septic shock were dictated by the international recommendations of the Surviving Sepsis Campaign (SSC) in 2004 and updated in 2016 and 2022. However, these recommendations only focus on two main areas: aetiological treatment of infection and management of organ failure.
Sepsis was associated to imbalance between increased production of free radicals and insufficient neutralization by endogenous antioxidants, including vitamin C. This causes a spread of oxidation reactions and contributes to organ failure. Although this imbalance has been proven to be more marked in burn patients, few studies have focused on the intake of vitamin C in this population. In the literature, it has been established that vitamin C protects cells from oxidative damage, reduces the inflammatory response, maintains immune function and increases haemodynamic reserve. All these biological actions may be beneficial in the management of sepsis and septic shock. In addition, the low cost of vitamin C offers clinicians an interesting prospect as an adjunct in the management of sepsis.
Sepsis remains an important cause of mortality in the intensive care unit ICUs worldwide. Prognosis of patients with sepsis or septic shock was closely related to early and efficacy of management procedures. Early fluid resuscitation, hemodynamic support, early administration of appropriate antibiotics are the mainstay of therapy. Therefore, adjuvant therapies have been tested to improve the outcomes such as vitamin C. Experimental and observational studies focusing on the beneficial effect of vitamin C in patients with sepsis are limited and controversial. Some studies suggesting that it is useful, while others indicate a lack of effectiveness. In addition, the results of these studies are difficult to interpret because populations studied are heterogeneous, with different, usually low, doses of vitamin C being used, oral and intravenous vitamin C regimens being mixed and other antioxidant agents (e.g. vitamin E and selenium) often being combined. In addition, most of these studies were retrospective, with a high degree of bias. This made it difficult to offer recommendations concerning the dose of ascorbic acid (varying between 50 and 100 mg/weight/day) and the duration of treatment. Also, in the literature no study was published regarding impact of vitamin C in septic burn patient. So, our study was carried out to assess hemodynamic impact of high dose of vitamin C (100 mg/weight/d) in septic burn patients.
METHODS
Prospective, case-control study was conducted in intensive burn care department in Tunisia during 28 months (July 2019- October 2021). Were included adult patients admitted within 24 hours post-burn for a stay >48 hours, with severe burns according to French Society of Brulology (FSB) and who developed sepsis or septic shock. Sepsis was retained according to the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). Non included pregnant woman, patients with history of lithiasis or vesico-renal calculus, of hemochromatosis or G6PD deficiency, and those on long-term vitamin C or glucocorticoids. Were excluded patients deceased before day 4 of protocol, and those who didn’t receive vitamin C because they were unavailable. Only one septic episode was considered per patient during his hospitalization.
Protocol of the study: After inclusion, ascorbic acid was prescribed at a dose of 100 mg/weight/day in septic patients from day 1 over 4 days. Vitamin C was administered intravenously in 3 doses. Patients who received vitamin C (vitamin C group) were compared retrospectively to those who did not receive vitamin C (control group) from the same center, matched in terms of age, sex, extent and severity of burns (according to prognostic scores).
Outcomes: The primary outcome was hemodynamic state assessed by dose and duration of vasopressor administration and fluid volume within 1, 3, and 7 days of admission. The secondary outcomes included kinetics of blood biology parameters: lactatemia, white blood cell count, platelet count and procalcitonin levels. Occurrence of multiorgan failure (MOF) and mortality attributed to sepsis at day 10.
Data Collection: Demographic, clinical and injury data were collected included age, sex, weight, body mass index (BMI), total body surface area (TBSA), full-thickness burn injury, inhalation injury, outcome, and hospital length of stay. Clinical and biological sepsis data were recorded. Use of vasopressor, fluids for resuscitation, mechanical ventilation, renal replacement therapy (RRT), were reported. Outcome was considered:
- Favourable with control of sepsis, assessed on clinical and biological parameters (apyrexia, withdrawal of vasoactive drugs, improvement of biological inflammatory syndrome, improvement in SOFA score, reduction in hydric hyperinflation with its repercussions).
- Unfavourable in relation to the occurrence of secondary and/or general complications of sepsis or death attributable to sepsis.
Statistical Analysis: Statistical analysis was performed using Statistical Package for Social Sciences (SPSS) 26.0 software. Continuous variables were reported as median and interquartile range (IQR), and categorical variables were reported as number and percentage. The normal distribution of quantitative variables was verified using the Shapiro-Wilk test. The two study groups were compared using the Mann-Whitney U test to compare means when the variables were not normal, and Student’s T test in the opposite case. Comparisons of numbers were made using Pearson’s chi-square test. Changes in the various parameters were compared using the Wilcoxon test. The significance level was less than 0.05. The influence of vitamin C on mortality attributable to sepsis within 10 days of sepsis was assessed.
RESULTS
During study period, fifty patients were prospectively enrolled (vitamin C group) and matched to a (control group) from the same center. Patients were assigned into 2 groups and received enoxaparin as follows:
- G1 (vitamin C group: n= 50)
- G2 (control group: n= 50)
1-Characteristics of patients
There were no significant differences in demographic, injury characteristics of 2 groups (table 1).
| G1 (vitamin C group) | n=50 | G2 (control group) | n=50 | p |
|---|---|---|---|---|
| Age (yrs) | 36±13 | 37± 14 | 0,67 | |
| sex-ratio | 2,33 | 3,55 | 0,36 | |
| TBSA (%) | 36±12 | 33±18,7 | 0,35 |
TBSA: Total body surface area;
In our series, there was no difference in terms of comorbidities between the vitamin C group and control group (table 2).
| Comorbidities | G1 (vitamin C group) | n=50 | G2 (control group) | n=50 | p |
|---|---|---|---|---|---|
| Pathological history | 25 | 50 | 19 | 38 | 0,227 |
| Hypertension | 4 | 17 | 2 | 11 | 0,564 |
| Diabetes | 5 | 21 | 6 | 32 | 0,423 |
| Chronic respiratory failure | 2 | 8 | 0 | 0 | 0,198 |
| Cardiopathy | 5 | 21 | 2 | 11 | 0,363 |
| Cancer | 0 | 0 | 2 | 11 | 0,104 |
| Psychiatric history | 12 | 48 | 5 | 26 | 0,143 |
| Drug addiction | 10 | 20 | 5 | 10 | 0,343 |
| long-term corticosteroid therapy | 0 | 0 | 1 | 5 | 0,255 |
Patients of 2 groups were comparable in terms of clinical data regarding the day of sepsis except for vasopressor’s use which was higher in vitamin C group compared to control group (Table 3).
| G1 (vitamin C group) | n=50 | G2 (control group) | n=50 | p |
|---|---|---|---|---|
| Glasgow coma scale (mean±SD) | 12±2 | 13±2 | 0,558 | |
| Temperature, °C, (mean±SD) | 37,8±2,8 | 38,3±1,6 | 0,353 | |
| Blood pressure (mmHg) | 133/88 | 121/70 | 0,096 | |
| Noradrenaline, n (%) | 34 (68%) | 28 (56%) | 0,220 | |
| Dose Noradrenaline, gamma/weight/min(mean±SD) | 0,62±0,6 | 0,25±0,37 | 0,005 | |
| Dobutamine, n (%) | 2 (4%) | 2 (2%) | 0,983 | |
| Dose Dobutamine, gamma/weight/min (mean±SD) | 2,5±3,54 | 2,5±3,54 | 1,000 |
Evaluation of severity of patients according to severity illness scores at day 1 of sepsis was as follows (table 4).
| Scoring of severity (day1) | G1 (vitamin C group) | n= 50 | G2 (control group) | n= 50 | p |
|---|---|---|---|---|---|
| APACHE II (mean±DS) | 20±9 | 14,6±9 | 0,004 | ||
| IGS II (mean±DS) | 45±21 | 34±20 | 0,05 | ||
| SOFA (mean±DS) | 8±5 | 4±4 | <10-3 |
APACHEII: acute and physiology chronic health evaluation II, SD: standard deviation, IGSII: simplified severity index II, SOFA: sepsis-related organ failure assessment.
Regarding biological parameters on the day of sepsis, group 1 had a higher lactataemia and PCT value than group 2 (Table 5).
| G1 (vitamin C group) | n= 50 | G2 (control group) | n= 50 | p |
|---|---|---|---|---|
| Leucocytes, elements/mm3 (mean±SD) | 15562±10148 | 12805±9161 | 0,159 | |
| Plaquettes, elements/mm3 (mean±SD) | 180,880±126325 | 245,800±155746 | 0,024 | |
| Lactataemia, mmol/L (mean±SD) | 3,24±1,45 | 1,71±1,05 | <10-3 | |
| Procalcitonine, ng/ml (mean±SD) | 19,97±28,95 | 8,17±15,05 | 0,014 | |
| Urea, mmol/L (mean±SD) | 4,65±2,34 | 4,29±2,6 | 0,821 | |
| Creatinine, µmol/L (mean±SD) | 74,08±30,7 | 80,25±37,9 | 0.248 | |
| Clairance of creatinine, ml/mn (mean±SD) | 141,89±69,66 | 148,16±91,53 | 0,701 |
Sepsis was frequently related to skin infection in respectively 74% and 70% for group 1 and 2. Origin of infection was bacterial, fungal and/or viral (table 6).
| G1 (Vitamin C group) | n= 50 | G2 (control group) | n=50 | p | |
|---|---|---|---|---|---|
| Gram négative bacteria | 18 | 36 | 5 | 10 | 0,002 |
| Cocci gram positive | 36 | 72 | 31 | 62 | 0,412 |
| Fungus | 20 | 40 | 8 | 16 | <10-3 |
| Viruses | 5 | 10 | 4 | 8 | 0,729 |
For 2 groups, three predominant Gram-negative bacteria were isolated: Klebsiella Pneumoniae, Acinetobacter Baumanii and Pseudomonas Aeuroginosa.
2-Management of patients
Antimicrobial therapy: Antibiotic therapy was started early on day 1 of sepsis, after microbiological investigation. According to the ecology of our ICU, antibiotic therapy was empiric in 39 patients for group 1 and 42 patients for group 2, with no statistically significant difference (p=0.611). Antifungal treatment was prescribed in 23 cases for group 1 and in 34 cases for group 2 (p=0.026). Addition of antiviral treatment was required in 29 cases for group 1 and 34 cases for group 2 (p=0.408). Addition of stress doses of corticosteroids: Supplementation of stress doses of hydrocortisone for 2 groups was similar (p=0,83).

Management of sepsis in 2 groups was similar in terms of:
- Initial fluid resuscitation: Fluid resuscitation using crystalloids with similar haemodynamic objectives (hourly urine out put of 0.5 to 1 ml/weight/h and MAP > 65 mmHg) for 2 groups.
- Ventilatory support: There were multiple ventilatory modalities: Non invasive ventilation (NIV) via High flow oxygen therapy, or bilevel pressure mode NIV (PSV), and invasive mechanical ventilation (IMV). NIV (PSV) mode was necessary for 4 patients in group 1 and 1 patient in group 2. High flow oxygen therapy was required for 4 patients in group 1 and 1 patient in group 2. Invasive ventilation was necessary in 34 patients in group 1 and 23 patients in group 2.
3- Haemodynamic impact of the addition of vitamin C in septic patients
a. Assessment of the use of amines: On day 1 of the protocol, patients of group 1 were more severe with statistically higher doses of noradrenaline (p=0,005). The addition of vitamin C reduced significantly the dose of noradrenaline during the study period (p<10-3). However, similar irregular fluctuations in the dose of dobutamine were reported in both groups (Table 7).
| G1 (Vitamin C group) | n= 50 | G2 (control group) | n=50 | p |
|---|---|---|---|---|
| Noradrenaline, Gamma/wght/min (mean±SD) | d1 0,62±0,6 | 0,25±0,37 | 0,005 | |
| d3 0.42±0.6 | 0.84±0.66 | 0,011 | ||
| d7 0,26±0,58 | 1,56±0,1 | <10-3 | ||
| Delta noradrenaline (d7-d1), Gamma/wght/min (mean±SD) | -0,36±0,02 | +1,31±0,27 | <10-3 | |
| Dobutamine, Gamma/wght/min (mean±SD) | d1 1,67±0,84 | 2,50±0,84 | 0,789 | |
| d3 6,25±1,26 | 15,00±3,36 | 0,499 | ||
| d7 2,50±0,87 | 2,80±0,81 | 0,956 | ||
| Delta Dobutamine (d7-d1), Gamma/wght/min (mean±SD) | 0,83±0,03 | 0,3±0,03 | 0,167 |
SD: standard deviation. Duration of amines’s dependancy was 4.12 days (0-12 days) for group 1 and 4.84 jours (1-12 days) for group 2 (p=0.28).
b. Assessment of fluid requirement: Fluid intake, based essentially on Ringer lactate and albumin, was similar in both groups. At day 1, group 1 was more severe, requiring more fluid intake. Amounts of fluids decreased significantly in group 1 with a delta D7-D1 (ml/wght/d) of -70.01 ml/wght/d compared with -43.46 ml/wght/d for group 2 (p=0.02) (table 8).
| G1 (Vitamin C group) | n= 50 | G2 (control group) | n=50 | p |
|---|---|---|---|---|
| Total, ml/wght/d (mean±SD) | d1 95,68± 37,84 | 72,76±26,38 | 0,632 | |
| d3 41,81±15,9 | 41,84±15,9 | 0,994 | ||
| d7 25,67±8,83 | 29,30±10,65 | 0,130 | ||
| Delta (d7-d1), ml/wght/d (mean+ SD) | -70,01±29,01 | -43,46±15,73 | 0,02 |
SD: Standard deviation.
c. Assessment of water balance: At D1, water balance was positive in 2 groups and was higher in group 1. During the protocol period, the addition of vitamin C reduced significantly the water balance at D3 and D4 of fluid resuscitation (table 9). Water balance between day 4 and day 1 was frankly negative at (-2281. 83±1000.41 ml/d) for group 1 against a continuing positive balance at (+60.14±1000.42 ml/d) for group 2, p<10-3 (table 9).
| G1 (Vitamin C group) | n=50 | G2 (control group) | n=50 | p |
|---|---|---|---|---|
| Water balance, ml/d (mean±SD) | d1 1783±2930 | 1197±3214 | 0,345 | |
| d2 850±2063 | 898±1873 | 0,904 | ||
| d3 209±1606 | 1051±1771 | 0,008 | ||
| d4 -530±1515 | 1261±1785 | <10-3 | ||
| Delta water balance (d4-d1), ml/d (mean±SD) | -2281,83±1000,41 | +60,14±1000,42 | <10-3 |
SD: Standard deviation.
d. Assessment of weight: From day 1 to day 4, there was no significant difference in weight between the two groups. On the other hand, a decrease in delta weight, between D1 and D4 of sepsis, of -0.28±0.65 kg was observed for patients in group 1, compared with an increase in weight of 1.36±078 kg for patients in group 2. (p=0,046) (Table 10).
| G1 (Vitamine C group) | n=50 | G2 (control group) | n= 50 | p |
|---|---|---|---|---|
| Weight, (mean±SD) | D1 81.42±19.26 | 74.94±17.22 | 0.079 | |
| D2 82.45±19.28 | 76.38±17.45 | 0.102 | ||
| D3 82.13±18.94 | 76.48±17.67 | 0.126 | ||
| D4 81.14±18.61 | 76.43±18.00 | 0.201 | ||
| Delta weight (D4-D1), (mean±SD) | -0.28±0.65 | 1.36±0.78 | 0.046 |
SD: standard deviation.
4. Impact of vitamin C supplementation in septic patients
• Sepsis control: Delay of sepsis control was 3 days for group 1 versus 4.1 days for group 2 (p=0,029).
• Length of ICU stay: Length of ICU stay for comparable for 2 groups, respectively 10 days was for group 1 versus 11 days for group 2 (p=0,7).
• Complications in ICU: Complications were lower in group 1 compared to group 2 respectively at 37 patients versus 48 patients (p=0,224) (Table 11).
| G1 (Vitamin C group) | n= 50 | G2 (control group) | n= 50 | p |
|---|---|---|---|---|
| Acute renal failure n (%) | 21(43) | 19(40) | 0,743 | |
| Compartimental abdominal syndrom, n (%) | 10(20) | 11(22) | 0,248 | |
| Acute respiratory failure, n (%) | 26(25) | 38(76) | 10-3 |
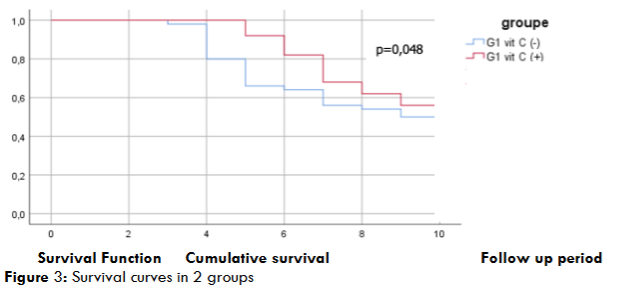
• Survival analysis: Survival during the first 10 days following sepsis was greater for patients in group 1, 22 patients (63% of survivors) compared with 13 patients (37% of survivors) in group 2. (p=0,048).
• Mortality: We used mortality at day10 as the mortality attributable to sepsis. Mortality attributable to sepsis during the first 10 days of sepsis, was lower in group 1, 28 patients (43% of deaths) versus 37 patients (57%) in group 2 (p=0.09).
DISCUSSION
Sepsis represents a real challenge for clinician due to the complexity of its pathogenesis, with the involvement of numerous immune and non-immune mediators, endothelial dysfunction, coagulation anomalies, altered cellular function and dysregulated cardiovascular responses. This pathogenesis makes it difficult to find a specific, effective therapy targeting the mediators of sepsis.
The principles of sepsis management were dictated by the international recommendations of the Surviving Sepsis Campaign (SSC) in 2004 and updated in 2016 and recently 2021 with the implementation of ‘bundles’. These recommendations focus solely on the main lines of treatment based on the rapid administration of appropriate antibiotics, as well as fluid and electrolyte resuscitation and oxygenation. In addition, new therapies are beginning to be studied, including vitamin C. Septic states are accompanied by an imbalance between increased production of free radicals and insufficient neutralisation by endogenous antioxidants, including vitamin C. This causes oxidation reactions contributing to organ dysfunction and therefore mortality. Vitamin C has many physiological molecular functions due to its role as an electron donor/reducer. It is known for its anti-inflammatory and antioxidant properties, and its role as an enzymatic cofactor in the synthesis of vasopressin, cortisol and catecholamines. Despite these beneficial effects, there is little medical evidence for its use in the septic population, and no data regarding its use in septic burn population. Hence the interest of our study, which aimed to analyse haemodynamic impact of the addition of vitamin C in septic burn patients in terms of fluid resuscitation, use of amines and duration of amine dependence.
In burn patients, the beneficial effect of vitamin C has been reported in the initial hydro-electrolytic resuscitation to reduce fluid inflation with a dose of 66 mg/weight/h. In addition, this dose has been reported to be effective and safe in severely burned patients. Our results showed that the addition of vitamin C at a dose of 100 mg/weight/day reduced the fluid balance on day 3 of fluid resuscitation in septic patients receiving vitamin C (Group 1) compared to those who did not receive vitamin C (Group 2) (209±1606 ml/d versus 1051±1771 ml/d) (p=0.008). At day 4, the balance was negative at (-530±1515 ml/d) in group 1 compared with a positive balance of (+1261±1785ml/d) in group 2 (p<10-3). The delta water balance (D4-D1) was negative in group 1 at (-2281.83±1000.41 ml/d) compared with a net increase to (+60.14±1000.42ml/d) in group 2. This relative negativation of the water balance in group 1 reflects the control of capillary hyperpermeability. Also, in our study, administration of vitamin C reduced the dose of noradrenaline from D3. The dose of noradrenaline was 0.42±0.6 gamma/weight/min (1.8 mg/h) on day 3 of sepsis in group 1, whereas we noted an increase in requirement of noradrenaline to 1.56±0.66 gamma/weight/mi (3.5 mg/h) in group 2 (p=0.011). The delta requirement of noradrenaline (D7-D1) in group 1 was (-0.36±0.02 gamma/weight/min) compared with (+1.31±0.27 gamma/weight/min) in group 2 (p<10-3).
Sepsis is associated with a profound intravascular fluid deficit due to vasoplegia and capillary leakage. Compared with healthy patients, burn patients have a lower response to plasma volume expansion with lower intravascular oncotic pressure, resulting in greater capillary leakage of albumin and fluid. Vitamin C leads to a reduction in the 3rd sector and an improvement in microvascular function in septic patients due to its antioxidant role.
In burn patients, beneficial effects of vitamin C on fluid inflation have been validated by some studies during the initial resuscitation of burns. Matsuda and al reported that for extensive burns, a continuous intravenous (IV) infusion of 340 mg/weight/d of vitamin C reduced resuscitation fluid volume requirements by 75%. A randomised controlled trial conducted in Japan by Tanaka and al in 2000 included 37 burn patients with burns of more than 30% extent, hospitalized within 2 hours of the burn, randomly assigned to receive either IV ascorbic acid at a dose of 66 mg/weight/h or standard treatment. The study showed that water intake was statistically lower in the intervention group at 3±1.7 ml/weight/% TBSA compared with 5.5±3.1 ml/weight/% TBSA in the control group, i.e. a 45.5% reduction (p<0.004).
In the literature, a systematic review was published on PubMed, Embase and the Cochrane Central Register. The review included randomised clinical trials (RCTs) with vitamin C as the intervention arm in the septic patient population. Twenty-three studies were included with a sample size of 2712 patients. In patients treated with vitamin C, there was a statistically significant reduction in the duration and need for vasopressors with a gain of 1.034 days (-1.622 to -0.445), p =0.001.
High incidence of mortality attributable to sepsis and the problem of antibiotic resistance have led to fears that sepsis-related mortality will increase over the coming decades. As a result, therapeutic clinical trials based on adjuvant treatments are constantly being updated to improve the prognosis of septic patients, including vitamin C. In the literature, it has been reported in the series by Fowler and al that treatment with vitamin C resulted in a significant reduction in the 28-d mortality. In fact, mortality was 46.3% (38/82) in the placebo group compared with 29.8% (25/84) in the vitamin C group (χ2 =4.84; p=0.03). Zabet and al obtained similar results in surgical critically ill patients with septic shock, with a significantly lower 28-day mortality in the ascorbic acid group than in the placebo group (14.28% versus 64.28% respectively; p=0.009) at a dose of 25 mg/kg intravenous ascorbic acid every 6 h. Also, mean dose of norepinephrine during the study period (7.44 ± 3.65 vs. 13.79 ± 6.48 mcg/min, P = 0.004) and duration of norepinephrine administration (49.64 ± 25.67 vs. 71.57 ± 1.60 h, P = 0.007) were significantly lower in the ascorbic acid than the placebo group.
In our study, survival during the first 10 days of follow-up of sepsis was greater for vitamin C group, at 63% compared with 37% for the no vitamin C group (p=0.048). Mortality attributable to the septic episode was lower in group 1 (n=28; 43% of deaths) compared to group 2 (n=37; 57%) (p=0.09).
So, high-dose ascorbic acid may be considered as an effective and safe adjuvant therapy in severely burned patients with septic shock. It has beneficial effect on restoring haemodynamic state and allows to reduce fluid intake during fluid resuscitation, dose of noradrenaline, without any reported side-effects. The monocentric nature and relatively small size of our population, with the absence of monitoring of serum vitamin C levels to adapt dosage to haemodynamic targets, constitute the main limitations of our study.
CONCLUSION
In septic burn patients, High-dose vitamin C therapy was associated with reduced fluid balance, doses of noradrenaline and duration of dependancy within the first 3 days of sepsis. Therefore, an evidence-based guideline providing a standard protocol in terms of its administration and dosage, aiming to minimize possible adverse effects was necessary in the future.
Declaration of authors:
All the authors who contributed to the development of this work: protocol, data collection, interpretation of results of this manuscript, approve the revised version and publication.
REFERENCES
- Torio CM, Andrews RM. National inpatient hospital costs: the most expensive conditions by payer, 2011 [En ligne]. Juil 2013 [Consulté le 30 juil 2023] ; [12 pages]. Consultable à l’URL: https://www.ncbi.nlm.nih.gov/books/NBK169005/pdf/Bookshelf_NBK169005.pdf
- Rhodes A, Evans LE, Alhazzani W, Levy MM, Antonelli M, Ferrer R, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. 2017 Mar;43(3):304-77.
- Evans L, Rhodes A, Alhazzani W, and al. Executive Summary: Surviving Sepsis Campaign: International Guidelines for the Management of Sepsis and Septic Shock 2021. Crit Care Med. 2021;49:1974–1982.
- Padayatty S, Levine M. Vitamin C: the known and the unknown and goldilocks. Oral Dis. 2016 Sep;22(6):463-93.
- Wilson JX. Evaluation of vitamin C for adjuvant sepsis therapy. Antioxid Redox Signal. 2013 Dec;19(17):2129-40.
- Wilson JX. Mechanism of action of vitamin C in sepsis: ascorbate modulates redox signaling in endothelium. Biofactors. 2009 Jan;35(1):5-13.
- Martimbianco ALC, Pacheco RL, Bagattini ÂM, and al. Vitamin C-based regimens for sepsis and septic shock: Systematic review and meta-analysis of randomized clinical trials. J Crit Care. 2022;71:154099.
- Juneja D, Nasa P, Jain R. Current role of high dose vitamin C in sepsis management: a concise review. World J Crit Care Med. 2022 Nov;11(6):349-63.
- Singer M, Deutschman CS, Seymour CW, Shankar Hari M, Annane D, Bauer M, et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). J Am Med Assoc. 2016 Feb;315(8):801-10.
- Eipper BA, Mains RE. The role of ascorbate in the biosynthesis of neuroendocrine peptides. Am J Clin Nutr. 1991 Dec;54 Suppl 6:1153-6.
- Carr AC, Shaw GM, Fowler AA, Natarajan R. Ascorbate-dependent vasopressor synthesis: a rationale for vitamin C administration in severe sepsis and septic shock? Crit Care. 2015 Nov; 19:418.
- Soltany A, Alaissami M. A scoping review of the role of ascorbic acid in modifying fluid requirements in the resuscitation phase in burn patients. Ann Med Surg. 2022 Mar;75:1-4.
- Nagel SS, Radu CA, Kremer T, Meess D, Horter J, Ziegler B, et al. Safety, pharmaco-dynamics, and efficacy of high- versus low-dose ascorbic acid in severely burned adults. J Burn Care Res. 2020 Jul;41(4):871-7.
- Marx G. Fluid therapy in sepsis with capillary leakage. Eur J Anaesthesiol. 2003 Jun;20(6):429-42.
- Zdolsek M, Hahn RG, Sjöberg F, Zdolsek JH. Plasma volume expansion and capillary leakage of 20% albumin in burned patients and volunteers. Crit Care. 2020 May;24(1):191.
- Tanu wijaya LY. Vitamin C as prevention in burn sepsis. Jurnal Plastik Rekonstruksi. 2020 Feb;7(2):65-76.
- Tanaka H, Matsuda T, Miyagantani Y, Yukioka T, Matsuda H, Shimazaki S. Reduction of resuscitation fluid volumes in severely burned patients using ascorbic acid administration: a randomized, prospective study. Arch Surg. 2000 Mar;135(3):326-31.
- Muhammad M, Jahangir A, Kassem A, Sattar SA, Jahangir A, Sahra S, et al. The role and efficacy of vitamin C in sepsis: a systematic review and meta-analysis. Adv Respir Med. 2022 Jul 28;90(4):281-99.
- Rhee C, Jones TM, Hamad Y, Pande A, Varon J, O’brien C, et al. Prevalence, underlying causes, and preventability of sepsis-associated mortality in US acute care hospitals. JAMA Netw Open. 2019 Feb;2(2):e187571.
- Gaieski DF, Edwards JM, Kallan MJ, Carr BG. Benchmarking the incidence and mortality of severe sepsis in the United States. Crit Care Med. 2013 May;41(5):1167-74.
- Fowler AA, Truwit JD, Hite RD, Morris PE, De Wilde C, Priday A, et al. Effect of vitamin C infusion on organ failure and biomarkers of inflammation and vascular injury in patients with sepsis and severe acute respiratory failure: the CITRIS-ALI randomized clinical trial. J Am Med Assoc. 2019 Oct;322(13):1261-70.
- Zabet MH, Mohammadi M, Ramezani M, Khalili H. Effect of high-dose ascorbic acid on vasopressor’s requirement in septic shock. J Res Pharm Pract. 2016 Apr;5(2):94-100.