





Hip Ankylosis in Children: Treatment Methods Reviewed
Hip Ankylosis in Young Children: Osteo-Arthroplasty Reconstruction Versus Cephaloburator Neocephaloplasty and Classification
Gheorghe Burnei¹, Mioara Georgescu MD, Ph.D.², Mihaela Banculescu MD, Ph.D.³, Maricela Dragomir MD, Ph.D.⁴
- Professor of Paediatric Orthopaedics, Constanţa Macta Clinic, Bucharest Tinos Clinic, Romania
- Paediatric Surgeon and Orthopaedist, ‘Sf. Apostol Andrei’ County Emergency Hospital in Constanţa, Romania
- Anaesthesiology-Intensive Care, ‘Sf. Apostol Andrei’ County Emergency Hospital in Constanţa, Romania
- University Assistant, ‘Dunărea de Jos’ University in Galaţi, Faculty of Physical Education and Sports, ‘Health with Ozone’ Clinic of Integrative Medicine in Galaţi, Romania
OPEN ACCESS
PUBLISHED: 30 October 2024
CITATION: Burnei, G., et al., 2024. Hip Ankylosis in Young Children: Osteo-Arthroplasty Reconstruction Versus Cephalobturator Neoacetabuloplasty and Classification. Medical Research Archives, [online] 12(10).
https://doi.org/10.18103/mra.v12i11.5769
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i11.5769
ISSN 2375-1924
ABSTRACT
Background and context.
The appearance of a bony ankylosis in a preschool child, located at the level of the hip, is a disabling, extremely severe complication. In the medical literature, this problem was not addressed directly, and in medical practice, the therapeutic conduct is limited to subtrochanteric directional osteotomies to correct the position of the pelvic limb and hip endoprosthesis (replacement) surgery in teenagers.
Purpose.
The paper compares and presents the effectiveness of surgical treatment in children with complex forms and severe complications following operated developmental dislocation of the hip. It proposes a differentiated approach to hip ankylosis and the choice of reconstruction technique, either through reconstruction of the acetabulum or by constructing a new joint.
Also this communication is to make known two innovative surgical interventions, hip osteoarthroplasty reconstruction (HOR) and cephalobturator neoacetabuloplasty (CN), useful in the treatment of hip ankylosis in young children.
The two interventions present some data on indications and intra- and postoperatively beneficial effects. The paper also includes the classification of hip ankylosis, as a useful tool in the choice of HOR versus CN.
There is an indissoluble link between the two surgical interventions and the classification of ankylosis. Knowing them allows a better understanding of this subject matter and extends the indications for CN.
The classification serves as a guide for practitioners and provides notes about the type and incidence rate of ankylosis in diseases that affect the hip.
Study design.
Analysis and synthesis of data observed in a period of 49 years of practice in paediatric orthopaedic surgery.
Patient sample.
The study sets out the knowledge gathered from the medical literature and from the experience acquired during the years 1990–2023, on a group of 143 patients (164 hips).
HOR was performed on 138 patients (164 hips) and CN was performed on 5 patients, 3 presenting hip dislocation amid cerebral palsy with spastic paraparesis and 2 with developmental dislocation of the hip after two reluxations. Extensive chondrosis at the level of the femoral head or the acetabulum revealed that plastic osteoarthroplasty reconstruction was contraindicated. In these cases, replacing the dislocation would have been equivalent to arthrodesis of the hip, an inadmissible attitude in young children.
Method.
All patients underwent radiological and imaging investigations and benefited from physical therapy to determine the real limits of movement. Before the surgical intervention, the range of hip motion was assessed, and the type of ankylosis was determined. All types of ankylosis found in the patients were included in the general classification of ankylosis.
Results.
After the first open reduction surgery and first reluxation, no patient had a second reluxation, femoral head necrosis or ankylosis. After the second reluxation (third intervention), 12 patients (16 hips), 9 years after the surgery, had signs of limited ankylosis and 3 hips had other complications with minor clinical manifestations; discomfort during intense and prolonged exertion, oblique pelvis with lopsided limp, and painless lumbar scoliotic deviation.
Conclusion.
HOR corrects all deformities following complex forms of developmental dislocation of the hip in a single surgical stage: acetabular dysplasia, femoral head anteversion and deformation, muscle imbalance, and allows the transposition of the acetabular portion with minimal iliac cartilage lesions in the weight-bearing zone.
CN configures a new hip joint.
The classification of ankylosis is a guide for the practitioner in choosing between surgical reconstruction or cephalobturator neoacetabuloplasty as a therapeutic solution, in the treatment of hip ankylosis in preschool children.
Keywords: Osteoarthroplasty reconstruction of the hip in children aged between 1 and 4 years. Cephalobturator neoacetabuloplasty. Complications of developmental dislocation of the hip. Ankylosis in young children. Diseases with potential evolution towards a hip ankylosis.
1. Introduction
Diseases likely to manifest as a rigid hip, with fibrous or bony etiopathogenesis, appear in children in a series of diseases that significantly limit the function of the hip and ultimately lead to severe, vicious and/or painful ankylosis.
When these ankyloses occur in young children (1–3 years) and pre-schoolers (3–6 years), the waiting period for endoprosthesis is long and other conditions caused by ankylosis frequently appear. The waiting time exceeds 10 years and corresponds to an important stage both for psychomotor development and for the accumulation of notions during the school period. Surgical interventions applied to correct ankylosis in these children, such as arthroplastical interventions and subtrochanteric osteotomies, present a number of drawbacks.
Hip ankylosis in preschool children is a disability, extremely severe and irreversible. The historical past in the field has a tumultuous background with orientations towards reckless solutions to solve such a complication.
Arthroplasty interventions for the treatment of fibrous ankyloses of the hip in children aimed at restoring joint mobility through the interposition of tissues between the joint surfaces: auto-¹,³, allo-, xenografts or polymer cups that may or may not also include a titanium casing¹,⁴. These surgeries had a major drawback. After 1–2 years postoperatively, stiffness returned progressively reaching 27–50% ⁵,⁶, which is why they disappeared from medical practice.
The complications of the interventions that resulted in ankylosis guided orthopaedic surgeons towards choosing specific surgical techniques. Pelvic osteotomies in young children diagnosed late with developmental dislocation of the hip did not take into account the possible variants of acetabular deformation and the corrective potential that a particular pelvic osteotomy provides. Given that the choice of surgical intervention was made based on the surgeon’s experience and preferences, preoperative imaging analysis of the hip must consider the acetabular index, the Wiberg angle, the neck–shaft angle, the anteversion angle of the proximal femur, the degree of bone coverage, the acetabulum depth, the pelvic height, degree of femoral head coverage, and the presence or absence of a chondral portion of the acetabular margin, which defines the coverage potential during growth and development.
All these data have guided and oriented surgical interventions towards HOR (without endoprosthesis) or towards CN, a new hip joint when reconstruction is not feasible. HOR includes surgical interventions on the pelvis and the proximal extremity of the femur. This procedure allows the complete reconstruction of the hip and the preservation of the potential for regeneration and remodelling on the reconstituted matrix. The triple or double osteotomy is the most important component of the reconstruction and can be performed on children aged between 1 and 4 years. After the procedure, the pelvis and the proximal femur present a great regenerating capacity for regeneration and remodelling. These osteotomies were initially performed on teenagers and older children. The indications have been extended to children aged 1 to 4 years by highly trained surgeons due to advances in anaesthesia and intensive care, the emergence of new implants, instruments, and surgical techniques. The role of surgeons in the effectiveness of HOR and CN is crucial.
2. Indications for Surgery
2.1 SUBTROCHANTERIC femoral OSTEOTOMIES
ensure orientation of the limb to provide effective static and dynamic support. The remote assessment of osteotomies revealed that the vicious ankylosis was temporarily corrected and the vicious position of the limb recurred. Another negative aspect is the fact that hip endoprosthesis surgery after directional osteotomies has difficulty implanting the femoral component due to changes in the medullary canal⁵.
2.2 HIP ENDOPROSTHESIS (REPLACEMENT) SURGERY IN TEENAGERS.
The preliminary results were good, but in the medium and long term, hypoplasia of the pelvis and shortening of the operated limb, repeated interventions to change the endoprosthesis and dysplasia of the hip with a lack of bone tissue, which complicated the choice and installation of the implant, were found⁷.
2.3 OSTEOARTHROPLASTY RECONSTRUCTION VERSUS CEPHALOBTURATOR NEOACETABULOPLASTY
In the case of the presence of joint injuries incompatible with a HOR and obtaining a normal mobility or a limitation at most moderate to ensure comfort until the time of endoprosthetics, CN can be resorted to. These eventualities are rare and occur after extensive necrosis of the femoral head that has an eccentric configuration and excessive cephalic or acetabular chondrolisis.
2.3.1 OSTEOARTHROPLASTY RECONSTRUCTION
HOR is the intervention of choice in the case of a dislocated hip with a loose or rigid fibrous ankylosis after a first intervention, or two interventions performed to reduce the dislocation. Children between 1 and 4 years of age have the greatest capacity to regenerate and remodel the operated hip⁸. Reconstruction in young children does not exclude complications, but their frequency is much reduced and the beneficial effects are relevant; maximum capacity for architectural reconfiguration of the acetabulum and femoral head, it integrates the pelvis without secondary consequences in the biomechanics of walking, it balances the spine and ensures the development and toning of the kinematic chains of the limbs and spine.
The elective indications for HOR are high developmental dislocations, unresolved dislocations after other surgeries, dislocations from osteogenesis imperfecta, and motor or sensory neuropathies. This procedure can also be applied in residual acetabular dysplasia following orthopaedic treatment and in acetabular dysplasia in teenagers when coxa valga, coxa breva magna, and femoral neck anteversion are present. The current use of this procedure in all cases involving children over the age of 1 reduces the rate of certain complications to 0 and significantly lowers the frequency of others.
Overall, HOR is a quadruple osteotomy of the pelvis and hip, followed by the reconstruction of the hip joint within the limits of the Y-cartilage memory. Sometimes, in children aged between one and two years, the triple osteotomy can be simplified to a double osteotomy depending on the possibility of repositioning and orienting the acetabulum. The subtrochanteric femoral osteotomy must be a centring osteotomy. If necessary, shortening will also be performed. It corrects anteversion or retroversion, valgus or varus deviation, or torsion present in dislocations from osteogenesis imperfecta.
In a group of 138 patients (164 hips), we never recorded relaxation, femoral head necrosis. Only after the second reduction (the 3rd surgical intervention) did complications appear; limited fibrous ankylosis in 12 patients (13 hips). Of these patients, those with ankylosis with evolutionary potential will be submitted to surgery for endoprosthesis. Even after the second reduction, other complications appeared; two subluxations and non-unions of the acetabulum in one hip.
2.3.2 CEPHALOBTURATOR NEOACETABULOPLASTY
In the case of the presence of joint injuries incompatible with HOR, chondrolisis, synostoses, etc., cephalobturatory CN [Fig.1] can also be considered.
The treatment of young children who have suffered rigid fibrous ankylosis is a debatable issue. In these cases, the hip is immobile and a bony ankylosis cannot be excluded during the clinical examination. The radiological and imaging examination eloquently illustrates the injuries present. If the present injuries contraindicate hip reconstruction, the only solution to save hip mobility in a young child can be CN⁹. I performed this intervention on 2 children with rigid fibrous ankylosis, each having in their personal history two interventions to reduce the dislocation preceded by a period of 3 weeks of traction-extension. Another 3 children with spastic paraparesis amid cerebral palsy with rigid fibrous ankylosis benefited from the CN.
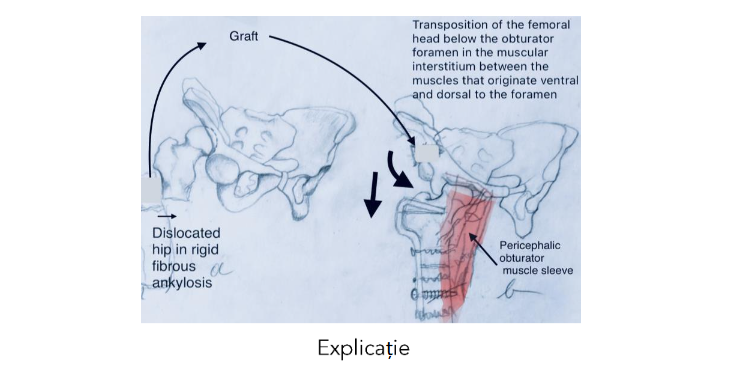
Fig.1 Cephalobturator neoacetabuloplasty shown schematically.
a) Femoral bone graft resulting from subtrochanteric osteotomy with shortening is used to fix the acetabulo-obturator segment after distal translation and anterior rotation.
b) The femoral head is placed below the obturator foramen surrounded by a muscular sleeve that originates on the obturator ring.
All 5 patients have regained their hip mobility, are walking and 4 of them are making continuous progress. For the first operated patient, 12 years have passed since the surgery and she walks normally and has the amplitude of hip movements within normal limits. She runs, plays sports and is a medical student. The case is work-in-progress for publication.
3. Classification
The existing data in the literature and the experience gained in over 45 years of medical practice give me the conviction that a certain group of rigid ankylosis in young children arising on the background of other conditions can lend themselves to CN. Labelling them according to certain criteria brings useful information for therapeutic conduct. The types of ankylosis, the age of the patient and the underlying condition are essential criteria that allow the orthopaedist to choose the optimal moment and type of intervention.
3.1 CLASSIFICATION ACCORDING TO THE LOCATION OF THE FACTORS THAT GENERATE HIP ANKYLOSIS
Ankylosis or stiffness of the hip is a limitation of mobility, generated by congenital, infectious, traumatic or inflammatory conditions. It can be total or partial and has extra-articular causes, intramuscular structural changes of the tendons, muscles or other peri-articular tissues, or intra-articular causes¹⁰.
3.1.1 EXTRA-ARTICULAR ANKYLOSES
appear as disabilities amid conditions that include several types of injuries.
3.1.1.1 MUSCLE STIFFNESS
is the iatrogenic retraction of the quadriceps¹¹ or glutes¹².
3.1.1.2 LOCAL SPASTIC SYNDROMES
can be transient and the involved muscles are not structurally affected. These syndromes respond to treatment with drugs that have a muscle relaxant effect. Their persistence or recurrence implies surgical relaxation. A case with idiopathic local muscle spasm that manifested as a contracture of the periauricular musculature of the hip and that subsided under general anaesthesia¹³ and another considered as idiopathic local hypertonia that was surgically relieved and that later recurred were described in the literature¹⁴. These manifestations are spastic contractions, similar to those in cerebral palsy, generated by the hyperreactivity of the motor cells in the anterior horns of the spinal cord.
3.1.1.3 CEREBRAL PALSIES
are stabilized brain injuries with progressive musculoskeletal manifestations that can range from muscle contractures to spasticity to bone deformities and dislocations. Hip pathology in spastic paraparesis from cerebral palsy ranks second, after equine foot¹⁵. The predominance of spasticity in the adductor muscle group reverses the effect of the normal evolution of decreasing the angle of inclination of the femoral neck from 150 degrees to 130 degrees. The femoral neck deviates in valgus, the contracture and retraction of the adductors becomes evident, walking is delayed or becomes heavier and on radiological examination the hip appears subluxated or dislocated. Hip migration is appreciated in 30–60% of children with cerebral palsy¹⁶. In children with spastic tetraparesis, hip migration reaches 79%¹⁷.
A screening conduct for radiological assessment of the hips allows establishing the optimal moment for the medial relaxation surgery and the prophylaxis of hip migration¹⁸. When should the medial thigh release be done? The optimal moment for the prophylaxis of hip migration is indicated by the value of the circular arc ‘head centre – acetabulum centre’ (HC–AC) [Fig.2]. The head centre – acetabulum centre discrepancy assesses the rate of decrease of the tilt angle from 150° to 130° and indicates the need for muscle relaxation if it has a value less than –15°¹⁹.
Hip migration is asymptomatic and becomes symptomatic with destruction of the articular cartilage. In neglected cases with arthritis, CN eliminates pain and allows mobilization of the hip. [Fig. 3]

Explicație
Fig. 2 A 2.8-year-old patient with spastic paraparesis who had never walked presented with bilateral equine foot associated with thigh adduction with adductor contracture and retraction. Pelvis X-ray (radiograph) showed a CH-AH angle of less than -15 degrees. Surgical intervention was carried out for the prophylaxis of the dislocation, performing medial relaxation of the thigh bilaterally and the lengthening of the Achilles tendon. 6 months postoperatively, the patient walked and after 20 months the femoral head returned to normal limits (-15°/+15° degrees).
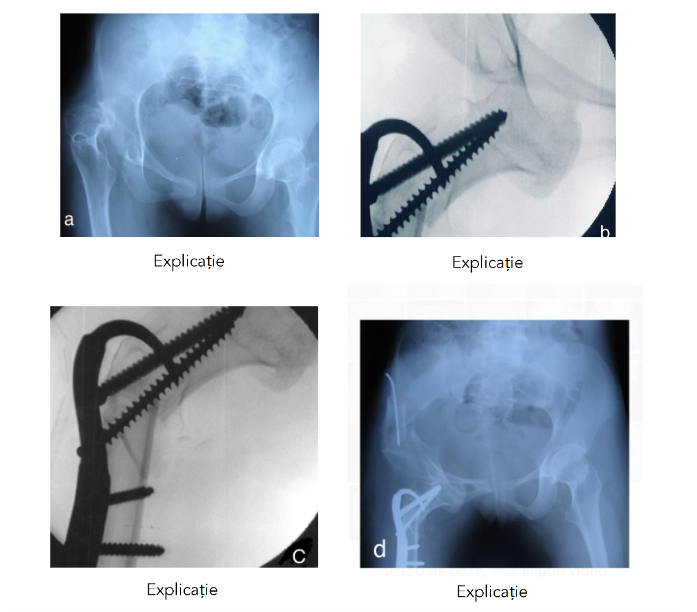
Fig. 3 Cephalo-obturatory neoacetabuloplasty in a 9.8-year-old female patient with a severe form of spastic paraparesis and unbearable pain at the level of the right hip:
a) dislocation of the right hip, coxa valga and antalgic position of the femur in adduction and internal rotation;
b) intraoperative verification of the position of the femoral head under the obturator ring;
c) fluoroscopic appearance of subtrochanteric osteotomy and trochantero-capital osteosynthesis;
d) radiological image 6 months postoperatively; the pain disappeared 30 days postoperatively and after 3 months she resumed walking.
3.1.1.4 HETEROTOPIC OSSIFICATIONS
Heterotopic ossification (HO) represents a mature, lamellar bone structure formed in muscle, interstitial tissue or tendons. In children, at the hip level, the most common cause is acetabular fracture and polytrauma associated with traumatic brain and spinal cord injuries²⁰. Non-accidental HO may also be present in young children. In familial hypocalciuric hypercalcemia (FHH), HO can be accompanied by discrete joint pains and appear later²¹.
Some ossifications are asymptomatic and others give a noisy symptomatology with pain and limitation of movements²².
The incidence of HO in children is lower than in adults and has a frequency between 4 and 22%²³. The hip joint is involved in 53% of cases and is followed by the shoulder, elbow and knee²⁴.
3.1.2. INTRA-ARTICULAR ANKYLOSIS:
3.1.2.1 INTRA-ARTICULAR FIBROUS ANKYLOSIS
Fibrous ankylosis in children appears in a series of systemic diseases such as tuberculous arthritis, infectious or inflammatory arthritis. In adults, the most common fibrous ankylosis occurs after trauma. The installation of these injuries activates a type of stem cells called mesenchymal stromal cells (MSCs) that can differentiate into osteoblasts, chondrocytes, and fibroblast growth factors, factors that induce angiogenesis or other factors that have a role in self-repair. While the vessels are being restored, blood extravasates from the capillaries and forms a hematoma. At the level of hematomas, the reconstructive process is disrupted by MSCs that induce improper restoration of the injured part²⁵. Hip surgery and prolonged immobilization induce fibrous ankylosis through the same process²⁶. As a rule, this precedes bony ankylosis.
3.1.2.2 INTRA-ARTICULAR BONY ANKYLOSIS
In the evolution of fibrous ankylosis, fusion of the femoral head with the acetabulum may occur. Normally the formed hematomas disappear after physical therapy. Their persistence will lead to the formation of bony ankylosis²⁵. The newly formed tissue slowly and progressively reduces mobility and bony ankylosis gradually occurs²⁷.
3.2 BIOMECHANICAL AND ETIOPATHOGENIC CLASSIFICATION OF HIP ANKYLOSIS IN CHILDREN
At the time of consulting a child who has impaired hip mobility or in the case of repeated surveillance and assessment of diseases susceptible to hip ankylosis, we can encounter several forms of manifestation generated by impaired mobility.
3.2.1. HIP WITH NORMAL MOBILITY AND EVOLUTIONARY ANKYLOSING POTENTIAL
The average normal values of the hip range of motion have the following limits: flexion 110–120 degrees, extension 10–15 degrees, abduction 30–50 degrees, adduction 25–30 degrees, external rotation 40–60 degrees and internal rotation 30–40 degrees. Intra-tester reliability for the passive assessment of the range of motion (ROM) is moderate to excellent and inter-tester reliability is from poor to excellent²⁸,²⁹.
3.2.1.1 CONGENITAL DISEASES
DEVELOPMENTAL DYSPLASIA OF THE HIP (DDH) is a dysplastic syndrome characterized by articular and periarticular structural abnormalities, hip instability, capsular laxity, and abnormal acetabulum. It is a disease with multiple evolutionary complications that can go from acetabular dysplasia to subluxation and dislocation. Early diagnosis of DDH is established by ultrasonography of the hips according to the Graf method. The screening test done in the first 30 days after birth allows the selection of newborns with dysplasia, their treatment with the Pavlik harness and the cure of dysplasia in the first 3–4 months³⁰.
Late detection or neglect of DDH leads to the occurrence of acetabular dysplasia, subluxation or developmental dislocation of the hip. The dislocated and neglected hip causes the appearance of a vicious cephalic and neck angulation [Fig. 4] which induces difficulties of care and handling infants, difficulty for both children and parents when breastfeeding.
Failed surgical interventions to reduce and stabilize the dislocated hip lead to reluxation and increase the risk of ankylosis. To eliminate this risk, HOR in young children provides more safety and allows the stability of the joint during the period with the greatest remodelling potential⁸,³¹.
3.2.1.2 INFECTIONS
3.2.1.2.1 CHRONIC OSTEOMYELITIS
All acute osteomyelitis, including that of the hip, whether in the form of osteomyelitis of the neck or acetabulum, of the ilium, ischium or pubis, can be cured by restitutio ad integrum if an early diagnosis is established and an energetic treatment is instituted, in an intensive therapy regime, in the first 3–5 days after onset³².
The infection of the hip begins suddenly, in full apparent health, or insidiously, with fever, alteration of the general condition and the inherent and antalgic position of the hip. In the first 3 days, it evolves as osteomyelitis of the neck or acetabulum and the pus from the infiltrative abscess diffuses into the joint giving rise osteomiylitic osterarthritis. After 5 days osterarthritis appears due to maceration of the articular cartilages of both surfaces.
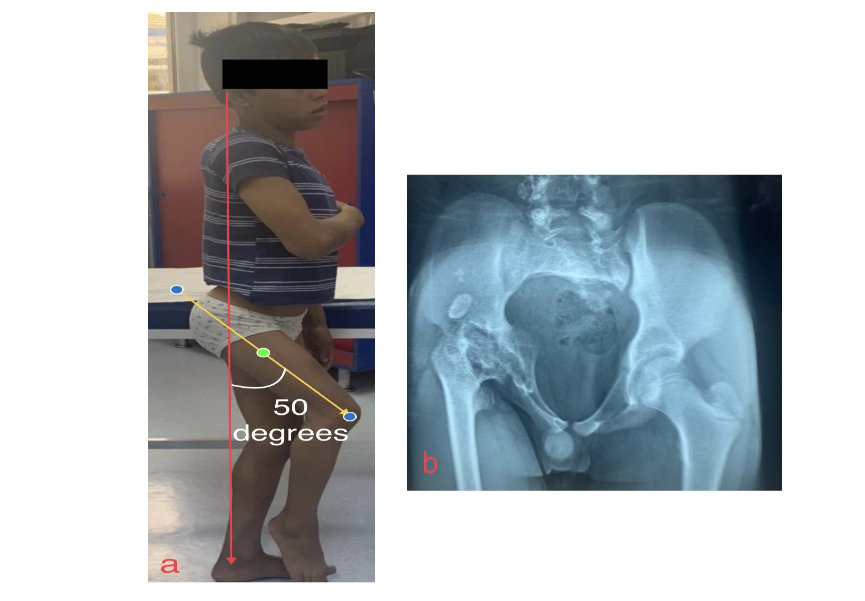
Fig 4 Right hip with abolished mobility:
a) thigh fixed in 50 degree flexion;
b) cephalioasic synostosis.
A neoacetabuloplasty could allow anatomical repositioning of the right pelvic limb and mobilization of the hip.
Lack of adequate treatment means chronic osteomyelitis. Eradication of chronic osteomyelitis is done by correct treatment and cure of acute osteomyelitis³³.
Chronic osteomyelitis can be the cause of severe complications, the heaviest of which is the pathological dislocation of the hip. Such a complication in the newborn, infant or young child could benefit from CN to save stability and mobility of the limb. In older children, teenagers, or young adults, inadequate treatment is the cause of early hip arthritis that occurs either before the age of 18 or in young adults between the ages of 18 and 40.
3.2.1.2.2 OSTEOARTICULAR TUBERCULOSIS
Osteoarticular tuberculosis occurs in 2% of patients with tuberculosis and represents 10–20% of cases with extrapulmonary tuberculosis³⁴. The condition begins insidiously in a patient known to have pulmonary tuberculosis, usually in the first year after the pulmonary infection. Location at the hip level is less compared to tuberculosis of the rachis³⁵.
Clinically and radiologically, it is necessary to differentiate from the following diseases: rheumatoid arthritis, transient synovitis, osteomyelitic arthritis, retroviral synovitis and various benign or malignant bone lesions³⁶,³⁷. The treatment is administered by combining 4 drugs as a result of the growth of multiresistant strains, after identifying the sensitivity of the strains to antibiotics³⁸.
Tuberculosis of the hip also occurs in young children aged 1–3 years. Hip mobility affected by serious destructive hip injuries at this age can be saved by CN.
3.2.1.3 INFLAMMATORY CONDITIONS
3.2.1.3.1 JUVENILE IDIOPATHIC ARTHRITIS
Juvenile idiopathic arthritis (JIA) affects the hip in up to 40% of patients and is the most common rheumatic disease in children³⁹. It occurs in children under the age of 16 and also affects children younger than 9 years. In children under this age, hip inflammation influences the growth cartilage, stimulates the excessive growth of the femoral neck, and a longer and anteverted femoral neck appears⁴⁰. The femoral head remains exposed for more than 20% and may later subluxate or dislocate. 2 years after the onset, the joint space narrows, the joint surfaces degenerate and ankylosis appear⁴¹. Ankylosis usually appears after the age of 9 years and extremely rarely in preschool children.
The therapeutic conduct of JIA includes medication and hip inflammation and inflammation cannot be controlled; hip arthroscopy is used for intra-articular lavage, synovectomy and limited capsulotomies followed by physical therapy, open synovectomy or iliopsoas and rectus ventralis lengthening/disinsertion to improve comfort of the patient by conserving the mobility of the hip and bringing the patient to an older age to be set in a prosthesis.
Pain, mobility and walking ability are significantly improved 4 years after synovectomy⁴².
Regardless of treatment, the disease is considered to be clinically inactive or in total remission if arthritis is absent, the patient does not have early morning stiffness, uveitis and ESR (erythrocyte sedimentation rate) and CRP (C-reactive protein) are normal⁴³. Clinical involvement of the hip in JIA in children aged 2 to 17 years results in the onset of hip arthritis or osteoarthritis.
Of 753 patients with JIA, 22.3% had the hip affected and of these 31.4% suffered from osteoarthritis (6.4% of the entire group of 753). Hip endoprosthesis (replacement) surgery was performed in 2.1% of those who had an affected hip⁴⁴.
Susceptibility to a CN is an exceptional or theoretical assumption because clinical manifestations occur in teenagers and extremely rarely in children under 4 years of age.
3.2.1.4 TRAUMATIC INJURIES
The most common traumatic hip injuries that can cause hip ankylosis in children and teenagers are traumatic dislocations and transacetabular fractures.
Yang describes 3 cases of 5 arthroscopically treated children, aged 11 to 15 years, from a cohort of 34 traumatic hip dislocations with post-reduction stiffness. All were treated arthroscopically for stiffness. After a short interval, the stiffness expanded and they were submitted to surgery after skeletal maturation, applying hip endoprosthetics⁴⁵.
I have conducted surgery on 2 cases of acetabular fractures; a 10-year-old boy and a 14-year-old girl with transacetabular comminuted fracture. Arthritis occurred and persisted 5 and 7 years after the surgical treatment. One patient’s hip was endoprosthesised at 18 months and the other at 20 years. The hip replacement surgery was done at 20 and 22 years, respectively.
3.2.1.5 IDIOPATHIC CHONDROLYSIS OF THE HIP (ICH)
It is a condition of unknown aetiology and has no specific symptoms. It was described for the first time by Jones⁴⁶. It is characterized by hip pain, contracture and retraction of the adductor muscles, intermittent claudication while walking, tilting of the pelvis on the affected side⁴⁷ and as such apparently unequal limbs.
Inflammatory tests to detect rheumatoid arthritis, osteomyelitis infection or tuberculosis are negative. The disease progresses and goes through 2 stages, the acute stage which lasts approximately 18 months and the chronic stage which lasts 3–5 years⁴⁸. In the acute stage, synovial inflammation is present and children complain of pain and limited range of motion. In the chronic stage, arthritic injuries are present and can appear in children aged between 8 and 10 years. The progressive destruction is cartilage of both articular surfaces of the hip, which forms an osteochondral macerate that transforms into bone metaplasia. In the most common cases, ICH manifests as a painful and vicious ankylosis of the hip. Conditions with a statistical risk of ankylosis can benefit from prophylactic treatment to avoid ankylosis or can make the moment of ankylosis appear at an age as old as possible so that the patient can benefit from the best possible treatment.
3.2.2. THE HIP WITH LIMITED MOBILITY
presents a partial ankylosis and is the consequence of a fibrous process amid a condition that poses risks.
3.2.2.1 TERATOLOGIC HIP DISLOCATION
Teratologic hip dislocation is an eloquent entity for a hip with limited mobility. The dislocation occurs intrauterinely and is present at birth. When attempting orthopaedic reduction, the hip is irreducible⁴⁹ even if this manoeuvre is performed under general anaesthesia⁵⁰. High teratologic dislocations are difficult to reduce even by open reduction. Some authors have proposed to try open reduction in all teratologic dislocations to improve hip mechanics and prevent pain⁵¹. The surgical intervention to reduce and stabilize the dislocation is indicated between 4 and 6 months. The risk of ankylosis is susceptible at preschool age. The rate of hip ankylosis in children between 1 and 6 years of age is not known. The presence of a pseudoacetabulum and the association with arthrogryposis, myelomeningocele, Ehlers–Danlos syndrome, Larsen syndrome or other genetic disorders increases the risk of the extension of hip ankylosis and the occurrence of bony ankylosis.
3.2.2.2 ARTHROGRYPOSIS
Arthrogryposis (A) is a rare condition, with unknown aetiology, with multiple rigid joints and with a frequency of 1 in 3,000 live births. More than 300 clinical forms of arthrogryposis have been described. Amyoplasia has a frequency of approximately 1 in 10,000 live births. This is the most common type⁵² and accounts for at least half of all children diagnosed with A.
Ankylosis of the hip in arthrogryposis has a very high frequency and affects up to 90% of patients. In unilateral dislocations of the hip, open hip reduction is indicated even if the risk of ankylosis is significant. Ankylosis can occur either as a result of reductions or after avascular necrosis and reluxation⁵³. Drummond⁵⁴ found that stiffness and persistent flexion deformity usually occurred after open reduction of any arthrogryptotic dislocation. The hips are usually flexed and internally or externally rotated and associated with other knee or leg deformities. The ankylosed arthrogryptotic hip is the most important problem to solve for a child to have a chance to walk functionally. Hip dislocation in a patient with A is usually defined as a teratologic dislocation. About one-third of arthrogryposis hips are dislocated at the time of birth.
Considering data according to which children with A and affected hips have a severe prognosis and only 50% can walk independently (25% are dependent on a wheelchair and 25% on walking orthoses)⁵⁵, CN could be a solution. In these ankyloses, it can save the mobility of the hip. An extended gluteal release followed by a cephalobturator repositioning will not result in a stiff hip as occurs in partial releases that can cause ankyloses. In evolution, the arthrogryptotic hip degenerates and early arthrosis occurs with limitation or loss of mobility and pain. Hip endoprosthesis surgery in arthrogryptics involves a series of difficulties, has potential indications and is presented and published in limited medical literature⁵⁶.
3.2.2.3 DEVELOPMENTAL DISLOCATION OF THE HIP
is an evolutionary complication of DDH and occurs during the period of growth and development of children who are under one year old. Hip mobility is limited to certain movements only. Ankylosis can occur in neglected children from isolated families who have very low education and living standards or after surgical interventions for developmental dislocations and prolonged immobilizations.
Long-term complications of hip dislocations include stiffness and decreased range of motion. Stiffness is more likely if intervention is required and immobilization is maintained for more than 3 months or if osteonecrosis of the femoral head occurs.
3.2.2.4 PROGRESSIVE OSSIFYING FIBRODYSPLASIA
is an autosomal dominant genetic disease and is characterized by progressive ankylosis of all joints⁵⁷ through progressive heterotopic ossification of periarticular structures.
No cases have been described with hip damage in young children. Traumatic agents, minor and even more so the major ones, generate progressive heterotopic ossifications. Surgical interventions induce and amplify ossification, which is why they are contraindicated.
3.2.3 HIP WITH ABOLISHED MOBILITY
3.2.3.1 RIGID FIBROUS ANKYLOSIS
is an advanced stage of fibrous ankylosis [Fig. 5]. In addition to the intra-articular degenerative processes, the peri-articular structures also participate. The hip capsule and ligaments are thickened and retracted and the periarticular muscles are contracted and shortened. The predominance of these changes in certain muscle groups positions the thigh viciously.
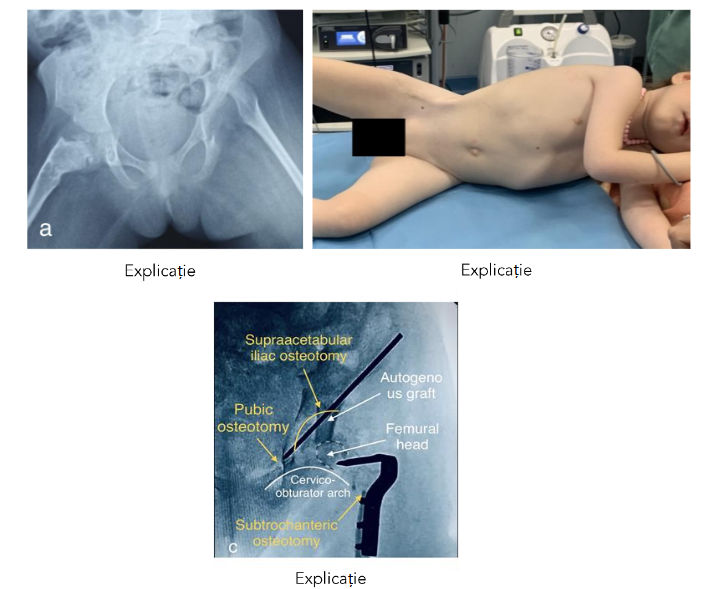
Fig 5 Rigid fibrous ankylosis of the right hip in a 5.4-year-old girl with bilateral developmental dislocation of the hip, operated on the right hip at the age of 1.4 years and then at 2 years:
a) right articular space absent and the femur fixed in abduction; dislocated left hip;
b) in left lateral decubitus, the right thigh remains rigid, fixed in abduction and lateral rotation;
c) fluoroscopic appearance of the hip after osteoarthroplasty reconstruction performed at 5.1 years.
6 months after surgery, passive hip flexion is normal. To resume walking, neoacetabuloplasty of the right hip can be lifesaving.
3.2.3.2 BONY ANKYLOSIS
totally compromises mobility. Fibrous ankylosis precedes bony ankylosis and, through bone metaplasia of the ‘osteochondral maceration’, it forms a compact bone mass that leads to the abolition of mobility. The joint becomes fibrous and rigid or bony²⁵.
3.2.3.3 CONGENITAL DISEASES
Congenital ankyloses can be synchondroses or synostoses. They are theoretically possible⁵⁸,⁵⁹. However, there are no reports of this type of complication.
4. Discussions
Both interventions can be performed through the same approach. A ventrolateral incision is made, following a path along the ventral third of the iliac crest, directed toward the ventrocranial iliac spine, the anterior side of the thigh, and branching laterally approximately 5 cm from the prominence of the greater trochanter. In HOR, a quadruple osteotomy of the pelvis and hip is performed, while if chondral lesions of the femoral head or acetabulum incompatible with HOR are present, CN can be performed by carrying out only the supraacetabular osteotomy followed by distal translation and ventral rotation of the acetabulum-obturator fragment. Chondral lesions that may contraindicate reconstruction can be identified in imaging exploration or detected intraoperatively after capsulotomy. Conversion from HOR to CN does not require an extension of the approach. HOR restores normal relationships and reconfigures the architecture of the hip. It transposes the internal iliac cortex and reconstructs the superior half corresponding to the acetabular rim. Through the regeneration process, the weight-bearing surface is thus consolidated. This translation utilizes the growth potential and memory of the Y-cartilage, and the acetabulum does not remain insufficient when the disproportion between the hypertrophied femoral head and the hypoplastic acetabulum makes reduction and stabilization impossible.
The first CN was a revelation. In 1986, a 40-year-old female patient was brought to the emergency room following a car accident. Her medical history mentioned that she was suffering from Ehlers–Danlos syndrome. The accident had caused her an explosive pelvic fracture. The femoral head was dislocated, and the acetabulum was literally shattered. Intuitively, I realized that the only point of support could be the obturator foramen⁶⁰.
The tissue hyperlaxity caused by the genetic disorder easily allowed the placement of the femoral head beneath the obturator foramen. The pelvic limb on the affected side appeared longer, as the level of the femoral head was lower than on the opposite side. She wore a shoe lift, and after three months, she was walking normally. Six years later, at the Orthopaedic Surgeons’ Congress in Oltenia, Professor Radu Constantin from the Orthopaedic Clinic in Craiova, who treated the female patient for another traumatic condition, presented a paper titled “The Obturator Foramen: A New Acetabulum?”. The medical report showed that the hip mobility had widened, and pain had diminished remarkably. Impressed by this evolution, we used this exceptional case as a model.
The classification of ankyloses synthesizes the types of ankylosis and allows for the differentiated use of the two surgeries. The indication for CN becomes predictable in cases of arthrogryposis, sequelae following pathological hip dislocation, idiopathic chondrolysis of the hip, other types of osteoarthritis, or other conditions.
Conclusion
HOR is the surgery of choice in the case of a dislocated hip with a loose or rigid fibrous ankylosis at the first intervention, or after the first reluxation (second intervention) and especially if the interventions were preceded by traction-extension.
CN is an exceptional intervention and a successful therapeutic solution with multiple advantages especially for young children to avoid dislocation reduction with the risk of arthrodesis after replacement. The classification of ankylosis, presented as synthesis in the paper and dispersed in the literature, is a useful tool for choosing a certain intervention at the right time. Some ankyloses of the hip occurred amid conditions susceptible to get complicated with this disease can benefit from HOR or cephalobturator neoacetabuloplasty.
Conflict of Interest:
None
Acknowledgements:
None
References
1. Sloan M, Kamath AF. Capsular augmentation in Colonna arthroplasty for the management of chronic hip dislocation. J Hip Preserv Surg. 2018 Jan 11;5(1):34-38. doi: 10.1093/jhps/hnx045. PMID: 29423248; PMCID: PMC5798024.
2. Bak Z, Farkas B. Früh- und Spätergebnisse von Operationen nach Colonna [Early and late results after Colonna arthroplasties of the hip-joint (author’s transl)]. Z Orthop Ihre Grenzgeb. 1975Oct;113 (5):896-9. German. PMID: 1202795.
3. Ganz R, Slongo T, Siebenrock KA. et al. Surgical technique: The capsular arthroplasty: a useful but abandoned procedure for young patients with developmental dysplasia of the hip. Clin Orthop Relat Res 2012; 470: 2957–67
4. Garkavenko YE. Bilateral pathological hip dislocation in children. Pediatric traumatology, orthopaedics and reconstructive surgery. 2017;5 (1):12-27. doi: 10.17816/PTORS515-12.
5. Kozhevnikov OV, Gorochov VY, Kralina SE. Experience in total hip replacement in adolescents. Russian Bulletin of Pediatric Surgery, Anesthesiology and Reanimatology; 2012;2(3):72-84.
6. Baskov VE, Neverov VA, Bortulev PI, et al. Total hip arthroplasty in children who have undergone arthroplasty with demineralized bone-cartilage allocups. Pediatric traumatology, orthopaedics and reconstructive surgery. 2017;5 (1):13-20. doi:10.17816PTORS5113-20.
7. Khrypov SV, Krasavina DA, Veselov AG, et al. Features of total hip arthroplasty in the treatment of secondary coxarthrosis of different genesis in older children. Pediatrician. 2017;8(4):43-7. doi: 10.17816/PED8443-47.
8. Burnei G , Burnei C , Dan D , Raducan ID. Acetabular Remodeling after Osteo-Arthroplasty Reconstruction on a Patient with Dislocation of Hip Development. Clin Surg. 2020;5:2783.
9. Burnei G, Dragomir M, Iordache IE. Cephalobturatory neoacetabuloplasty. Medical Life, 3 nov 2023;48:p13
10. Chisholm H, ed. “Ankilosis”. Encyclopaedia Britanica. Vol. 2 (11th ed.) 1911. Cambridge University Press. p. 58.l
11. Burnei G, Neagoe P, Margineanu BA, Dan D, Bucur PO. Treatment of severe iatrogenic quadriceps retraction in children. J Pediatr Orthop B 2004; 13:254-8.
12. Gonzalez R. Gluteal Retractions: Classification and Treatment Techniques. Aesthetic Surgery Journal. 2006;26(5):537–50, https://doi.org/10.1016/j.asj.2006.08.007
13. Alanazi H, Almalik F, Alanazi N, Alhussainan T. Relapsed hip stiffness after recovery of range of motion in a hip treated for developmental dysplasia of the hip? Think again: A case report. Int J Surg Case Rep. 2020;77:843-847. doi: 10.1016/j.ijscr.2 020.11.133. Epub 2020 Nov 30. PMID: 33395909; PMCID: PMC8253858
14. Akgül T, Göksan SB, Eren I. Idiopathic hypertonicity as a cause of stiffness after surgery for developmental dysplasia of the hip. Int J Surg Case Rep. 2014;5(3):155-8. doi: 10.1016/j.ijscr.2014.01.012. PMID: 24568944; PMCID: PMC3955227.
15. Howard JJ, Willoughby K, Thomason P, Shore BJ, Graham K and Rutz E. Hip Surveillance and Management of Hip Displacement in Children with Cerebral Palsy: Clinical and Ethical Dilemmas. J. Clin. Med. 2023;12(4), 1651;
16. Pountney T, Green EM. Hip dislocation in cerebral palsy. BMJ. 2006 Apr 1;332(7544):772-5. doi: 10.1136/bmj.332.7544.772. PMID: 16575079; PMCID: PMC1420759.
17. Hägglund G, Lauge-Pedersen H, Wagner P. Characteristics of children with hip displacement in cerebral palsy. BMC Musculoskelet Disord. 2007. 26;8:101. doi:10.1186/1471-2474-8-101. PMID: 17963501; PMCID: PMC2194677.
18. Burnei G, Ciobanu C, Neagoe P, Galinescu M, Bucur OP. Prophylaxis of subluxation and dislocation of the hip in children with cerebral motor disabilities. The Journal of Orthopaedics and Traumatology. 2002;12(4): 215-218.
19. Georgescu I. Burnei’s technique of femoral neck variation and valgisation by using the intramedullary rod in Osteogenesis imperfecta. J Med Life. 2014;7(4):493-498. PMID: 25729442; PMCID: PMC4316125
20. Ranganathan K, Loder S, Agarwal S, Wong VW, Forsberg J, Davis TA, et al. Heterotopic ossification: basic-science principles and clinical correlates. J Bone Joint Surg Am. 2015;97:1101–1111.
21. Burnei G, Țandea V, Răducan ID, Burnei C. Familial Hypocalciuria– Hypercalcemia. Clin Surg. 2020;5:2814.
22. Markes AR, Venishetty N, Holthausen H. Pediatric Heterotopic Ossification: A Comprehensive Review. Cure Rev Musculoskelet Med. 2023; https://doi.org/10.1007/s12178-023-09862-y
23. Feroe AG, Hassan MM, Flaugh RA, Maier SP, Cook DL, Yen YM, et al. Incidence and risk factors for heterotopic ossification in a matched cohort adolescent population undergoing hip arthroscopy. J Pediatr Orthop. 2022;42:e331-335.
24. Kluger G, Kochs A, Holthausen H. Heterotopic ossification in childhood and adolescence. J Child Neurol. 2000;15:406-413.
25. Zhang PP, Liang SX, Wang HL, Yang K, Nie SC, Zhang TM, Tian YY, Xu ZY, Chen W, Yan YB. Differences in the biological properties of mesenchymal stromal cells from traumatic temporomandibular joint fibrous and bony ankylosis: a comparative study. Animal Cells and Systems. 2021;25(5):296–311. doi:10.1080/197683 54.2021.1978543.ISSN1976-8354. PMC 8567918. PMID 34745436.
26. Vaishya R, Singh AK, Agarwal AK, Vijay V. Bilateral Spontaneous Bony Ankylosis of the Elbow Following Burn: A Case Report and Review of the Literature. J Orthop Case Rep. 2018;8(5):43-46. doi:10.13107/jocr.2250-0685.1204. PMID:30740374; PMCID: PMC6367284.
27. Yan YB, Liang SX, Shen J, Zhang JC, Zhang Y. Current concepts in the pathogenesis of traumatic temporomandibular joint ankylosis. Head Face Med. 2014;10:35. doi:10.1186/1746-160X-10-35. PMID: 25189735; PMCID: PMC4158390.
28. Charlton PC, Mentiplay BF, Pua YH, Clark RA. Reliability and concurrent validity of a Smartphone, bubble inclinometer and motion analysis system for measurement of hip joint range of motion. J Sci Med Sport. 2015;18(3):262-267. doi:10.1016/j.jsa ms.2014.04.008. PMID: 24831757.
29. Prather H, Harris-Hayes M, Hunt DM, Steger-May K, Mathew V, Clohisy JC. Reliability and agreement of hip range of motion and provocative physical examination tests in asymptomatic volunteers. PMR. 2010;2(10):888-895. doi:10.1016/j.pmrj.2010.05.005. Erratum in: PMR. 2011;3(3):286. PMID: 20970757; PMCID: PMC3438506.
30. Burnei G. Eradicating developmental dislocation of the hip: a national program in Romania using the Graf method of ultrasound examination. Med Ultrason. 2014;16(4):391-392. PMID: 25463898.
31. Atilla B. Reconstruction of neglected developmental dysplasia by total hip arthroplasty with subtrochanteric shortening osteotomy. EFORT Open Rev 2016;1:65-71. DOI:10.1302/2058-5241.1.000026.
32. Burnei G, Ionut Daniel Răducan ID, Lală CG, Klinaku I, Daraban AM, Burnei C. Multiple Enostosis After 8 Years of Chronic Fistulised Osteomyelitis After 40 Years as of the Onset of the Acute Osteomyelitis. J Adv Clin Case Rep. 2020;1(1):1-6
33. Burnei G. Eradication of chronic osteomielitis in Romania. Retrospective analysis with practicat applicability. International Journal of Medical Dentistry. 2023; 27(1): 151-153
34. Teo HE, W.C. Peh WC. Skeletal tuberculosis in children. Pediatr Radiol. 2004;34:853-860
35. Jiménez E, et al. Artritis tuberculosa en paciente de 2 años de edad. Reumatol Clin. 2011; 7(6):417–418.
36. Mohideen MAF, Rasool MN. Tuberculosis of the hip joint region in children. SA orthop. j.
2013;12(1) Centurion Jan
37. Wang MN, Chen WM, Lee KS, et al. Tuberculous osteomyelitis in young children. J Pedr Orthop 1999;19:151-155.
38. Swaminathan S, Rekha B. Pediatric tuberculosis: global overview and challenges. Clin Infect Dis, 50 (2010), pp. S184-S194.
39. Batthish M, Feldman BN, Babin PS, Tyrrell PN, Schneider R. Predictors of hip disease in The systemic arthritis subtype of juvenile idiopathic arthritis. J Reumatol 2011; 38(5): 954-958
40. McCulough CJ. Surgical management of the hip in juvenile chronic arthritis. Br J Rheumatol 1994; 33(2): 178-183.
41. Goodman SB. The Hip in Juvenile Idiopathic Arthritis.The Open Orthopaedics Journal 2020;14: 88-94. Publisher ID: TOORTHJ-14-88
42. Carl HD, Schraml A, Swoboda B, Hohenbrger G. Synovectomy of the hip in patients with juvenile rheumatoid arthritis. J Bone Joint Surg Am 200; 89(9):1986-1992.
43. Foley CM, McKenna D, Gallagher K, McLellan K, Alkhdher H, Lacassagne S, Moraitis E, Papadopoulou C, Pilkington C, Al Obaidi M, Eleftheriou D and Brogan P. Systemic juvenile idiopathic arthritis: The Great Ormond Street Hospital experience (2005-2021). Front. Pediatr. 2023;11:1218312. doi: 10.3389/fped.202
44. Sorokina LS, Avrusin IS, Raupov RK, Lubimova NA, Khrypov SV, Kostik MM. Hip Involvement in Juvenile Idiopathic Arthritis: A Roadmap From Arthritis to Total Hip Arthroplasty or How Can We Prevent Hip Damage? Front Pediatr. 2021;5(9):7 47779. doi:10.3389/fped.2021.747779. PMID: 34805045; PMCID: PMC8604160.
45. Yang D, Lee J, Orellana K, Batley M, Syed AN, Sankar W. Traumatic hip dislocations in a pediatric cohort: The importance of advanced imaging. Journal of Children’s Orthopaedics. 2023;17(3): 259-267. doi:10.1177/18632521231164990.
46. Jones BS. Adolescent chondrolysis of the hip joint. S Afr Med J 1971;45:196–202.
47. Guan T, Zhao D, Xiong H, Fang B, Li Y. Diagnosis and treatment of 10 cases of idiopathic chondrolysis of the hip. J Child Orthop. 2023;17(2): 105-115.doi:10.1177/18632521221144061. PMID: 37034189; PMCID: PMC10080235.
48. Morrissy RT, Weinstein SL. Lovell and Winter’s pediatric orthopaedics. 6th ed. Philadelphia, PA: Lippincott Williams & Wilkins, 2006, 1147–1155.
49. Rombouts JJ, Rossillon R. Teratologic dislocation of the hip: review of a series of 17 cases. Acta Orthop Belg. 1990;56(1Pt A):181-189. PMID:2382543.
50. Wada A, Yamaguchi T, Nakamura T, Yanagida H , Takamura K , Oketani Y et al . Surgical treatment of hip dislocation in amyoplasia- type arthrogryposis. J Pediatr Orthop B. 2012; 21: 381–385.
51. Benjamin Joseph, Selvadurai Nayagam, Randall Loder, Ian Torode. Teratologic hip dislocation in multiple congenital contractures: Paediatric Orthopaedics. Second Edition. 2015. Chapter 27; 225-229.
52. Hall JG. Arthrogryposis multiplex congenita: etiology, genetics, classification, diagnostic approach, and general aspects. J Pediatr Orthop B. 1997;6 (3):159-166. PMID: 9260643.
53. Stilli S, Antonioli D, Lampasi M, Donzelli O. Management of hip contractures and dislocations in arthrogryposis. Musculoskelet Surg. 2012;96(1): 17-21.doi:10.1007/s12306-012-0180-9. PMID:22278604.
54. Drummond DS, Siller TN, Cruess RC. Management of arthrogryposis multiplex congenita. AAOS Instructional Course Lecture, 1974;23:79-95.
55. Gibson DA, Urs NDK. Arthrogryposis multiplex congenita. J Bone Joint Surg [Br] 1970;52 pp:483-493.
56. Fisher KA, Fisher DA. Total Hip and Knee Replacement in a Patient with Arthrogryposis Multiplex Congenita. Am J Orthop. 2014;43(4):E 79-E82.
57. Pignolo, R.J., Shore, E.M. & Kaplan, F.S. Fibrodysplasia Ossificans Progressiva: Clinical and Genetic Aspects. Orphanet J Rare Dis 6, 80 (2011). https://doi.org/10.1186/1750-1172-6-80.
58. Kéry L, Wouters HW. Congenital ankylosis of joints. Arch Chir Neerl. 1971;23(2):173-184. PMID:5148467.
59. Steel HH, Kohl EJ. Multiple congenital dislocations associated with other skeletal anomalies (Larsen’s syndrome) in three siblings. J Bone Joint Surg Am. 1972;54(1):75-82. PMID: 4626580.
60. Stancu A. “Punctual” Show, RTV Galati – Braila, June 2023. https://www.youtube.com/watch?v=wytU9byeZPo
Most read articles by the same author(s)
- Gheorghe Burnei, Mioara Georgescu, MD, PhD, Maricela Dragomir, MD, PhD, Mihaela Banculescu, MD, PhD, Congenital Muscular Torticollis: A Chapter that Led to the Establishment of the Specialty of Paediatric Orthopaedics , Medical Research Archives: Vol 13 No 10 (2025): Vol.13, Issue 10, October 2025