





Housing Vouchers Enhance Recovery for Mothers Post-Treatment
Maintaining Recovery with Contingent Housing Payments: A Pilot Program for Women with Children Who Completed Residential Substance Use Disorder Treatment
Ahmad A Kittaneh PhD 1; Stephen Alex Crockett MD 2; Essence Hairston LCSW, LCAS, CCS 1; Elisabeth Johnson PhD, FNP-BC, CARN-AP, LCAS 1; Jocelyn Foxworth BA Ed 1; Ginny Carter, PhD 1; Kim Andringa PhD, MSPH 1; Hendrée E. Jones PhD 1,3
- Horizons Division and Department of Obstetrics and Gynecology, University of North Carolina at Chapel Hill, Chapel Hill, NC 27510
- Departments of Psychiatry and Behavioral Sciences and Obstetrics and Gynecology, School of Medicine, Johns Hopkins University, Baltimore, MD 21224
OPEN ACCESS
PUBLISHED: 31 May 2025
CITATION: Kittaneh, AA., Crockett, SA., et al., 2025. Maintaining Recovery with Contingent Housing Payments: A Pilot Program for Women with Children Who Completed Residential Substance Use Disorder Treatment. Medical Research Archives, [online] 13(5). https://doi.org/10.18103/mra.v13i5.6577
COPYRIGHT © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i5.6577
ISSN 2375-1924
ABSTRACT
Housing insecurity is a critical social driver of health, strongly associated with increased risk of substance use, adverse medical and psychiatric outcomes, and legal and employment instability. These risks are particularly acute during pregnancy and parenting times of life, where housing instability exacerbates maternal stress and adversely affects infant and early childhood health. Patients who have completed residential substance use disorder treatment often have limited options regarding housing as they are often reintroduced to low-income environments and experience discrimination associated with their substance use problems. This pilot project evaluated the impact of a structured housing voucher intervention on housing stability and substance use–related outcomes among perinatal patients and mothers following discharge from residential substance use disorder treatment. Participants (n = 12) were enrolled in a voucher-based housing payment program for up to 12 months that provided rental assistance alongside integrated medical, psychiatric, substance use disorder treatment, and case management services. Monthly assessments were conducted to evaluate housing status, mental and physical health, legal and employment outcomes, and substance use outcomes. Our results indicated that participants showed reductions in housing insecurity and little substance use over the course of their participation in the study. Improvements were also observed in legal and employment domains, as well as in self-reported mental health indicators. These findings underscore the critical role of housing interventions in promoting sustained recovery and maternal–child well-being. Further investigation in larger, randomized samples is warranted to establish generalizability and inform policy implementation.
Keywords: Pregnancy, opioids, housing, vouchers
Introduction
Drug overdose remains among the leading causes of mortality among pregnant and postpartum women in the United States. Between 2017 and 2020, the rate of fatal drug overdose rose 80% among pregnant and postpartum women. Unstable housing is a known risk factor linked to increased rates of substance use disorder and fatal overdose. Numerous studies demonstrate an increased risk and incidence of poor control of chronic medical conditions among those experiencing housing insecurity. Being both pregnant and experiencing housing instability or being fully unhoused presents unique challenges in accessing medical care and social support services, such that housing instability is associated with increased rates of low fetal birth weight, extreme preterm delivery, and severe maternal morbidity and mortality. The economic and emotional distress associated with housing instability may trigger pregnant and postpartum patients to rely on maladaptive coping mechanisms such engagement in substance use or a return to use. A reported 9% of individuals experience homelessness and unstable housing while pregnant. Interventions aimed to help pregnant and parenting patients access housing support resources could address the public health crisis of substance use disorder and fatal overdose among this population and improve perinatal health outcomes.
Pregnancy is a time that can create the opportunity for engagement with healthcare resources and behavioral health treatments that may be otherwise inaccessible given broadened access to publicly funded health insurance for pregnant patients. Many patients with substance use problems who become pregnant cite key motivating factors for substance use disorder treatment as the desire to protect their infant’s wellbeing and to stop their drug and alcohol use. Their goals are more achievable when housing and comprehensive prenatal and pediatric care are provided. However, compared to the prenatal time, care during the postpartum period is not as widely accessible given varying degrees of Medicaid coverage, increased social isolation, limited opportunities for continuation of care and social support, and increased stress with newborn caretaking responsibilities. The extant research provides evidence of the need for more support during the postpartum period given that most pregnancy-related deaths secondary to drug overdose occur in the postpartum period. Additionally, studies have linked substance use disorder treatment discontinuation and subsequent overdose with unique stressors associated with the postpartum period, such as postpartum depression and interactions with child protective services. However, limited research exists on effective interventions to support pregnant and newly postpartum patients with a substance use disorder who are also experiencing housing insecurity.
Current research demonstrates that pregnant and recently postpartum women experiencing housing insecurity have better mental health and substance use outcomes when housing and wrap-around social services and mental health resources are provided compared to mothers who receive emergency shelter and brief subsidized housing. However, these studies are limited in their longitudinal follow-up of pregnant and recently postpartum patients following the completion of substance use disorder (SUD) treatment programs. The current project was developed following the violent death of a former University of North Carolina (UNC) Horizons patient, Cara, who completed residential substance use disorder treatment at Horizons yet had no other place to live other than with the unsafe individuals who contributed to her death. The current pilot project aimed to assess the long-term outcomes of a voucher-based housing payment model aimed at increasing access to safe, sustainable housing and associated recovery and childcare services for perinatal patients who had engaged with and graduated from a residential substance use disorder treatment during their pregnancy.
Methods
PARTICIPANT SELECTION AND STUDY PROCEDURES
All study procedures were approved by the UNC School of Medicine. Participants in this pilot study were perinatal and parenting women who had received care in the UNC Horizons SUD treatment program. Data collection occurred from February 2022 to April 2023. To be eligible, participants were required to have been actively engaged with Horizons treatment services for at least 6 months, currently receiving services offered by Horizons (e.g., outpatient therapy, psychiatry, case management), and be clinically stable (no active substance use, pursuing financial stability, etc.). Participants were only allowed to opt out of outpatient services with a letter of support from their therapist or case manager detailing an alternative recovery plan. Participants were eligible for up to 12 months of funding for housing if they could provide proof of current employment or 3 months of funding if they were unemployed. Participants could receive up to $500 or 50% of their rent for up to 12 months (if rent was less than $1000). Participants were no longer eligible for the housing payments if they were no longer deemed clinically stable by their treatment team or no longer engaged in treatment at Horizons without a letter of support from their case manager or therapist. Each month, three attempts were made to reach the participant. If no contact was made to verify lease information, no payment was issued to the landlord. If a participant resumed contact with the research team, they were eligible for the following month’s payment assuming the other inclusion criteria were met.
Participants applied to the program by providing proof of apartment or other housing lease and completed an interview prior to the final determination of approval. In the interview, participants were asked to justify the amount of funding requested by describing how the funds would supplement their paycheck to achieve safe housing, what they had accomplished at Horizons, how the funding would help them maintain sobriety and an action plan to develop financial stability by the end of the funding period. Once approved, participants completed an initial baseline assessment and agreed to be contacted monthly for follow-up visits. The initial assessment consisted of demographic information, contact information, substance use diagnoses, a shortened version of the Addiction Severity Index (ASI) that examines life functioning in medical, employment, legal, alcohol, drugs, social and psychiatric domains and a housing stability measure as assessed by the Housing Instability Index (HII). Total scores for the HII were calculated by summing the scores of individual items, with higher scores representing greater levels of housing instability. At each follow-up visit, the research team reviewed contact information and collected HII scores, ASI follow-up self-reported data, Child Protective Services (CPS) involvement, and current involvement with Horizons treatment services.
ANALYTIC PLAN
Trend analysis was utilized to examine changes in participant mental and physical health and substance use as measured by the ASI. Additionally, participant reporting on housing stability was also examined. Total means were observed for changes over the course of participant engagement in the study. A content analysis was conducted to assess the participant experience receiving this funding and the impact on their housing situation and health status. All statistical analyses were conducted with SPSS, version 28.
Results
PARTICIPANT CHARACTERISTICS
A total of 13 women applied for the housing voucher program. One woman did not qualify. Thus, the sample was comprised of 12 women who received funding. The overall mean age was 32.8 (SD = 6.6). Participants identified as white (n=5), black (n=3), and American Indian (n=1); 3 participants did not provide demographic information. Half (50%) of participants had some college education and 83% reported at least completing a high school or equivalent degree. Participants, on average, received funding for roughly 8 months (8.8; SD = 3.4) and received $487.83 of funding per month. One participant initially was approved for $500 a month in voucher payments but was given a payment of $1399 due to a motor vehicle collision. On average, participants paid $1020.58 in rent per month.
HOUSING STABILITY, ALCOHOL USE, AND DRUG USE
At baseline, participants had a mean HII score of 2.8 (SD = 0.9) with scores decreasing with each month of funding. At 6-month follow-up, 9 participants maintained contact with the program and were still receiving funding. These participants had an average HII score of 0.4 (SD = 0.9). Participants who received 10 months of funding (n = 7) had an average HII score of 0.9 (SD = 1.1) and participants who received 12 months of funding (n = 3) reported an average score of 0.3 (SD = 0.6). Significant differences were observed between HII baseline means and 6-month follow-up means (t = 4.67, p = .003) and 10-month follow-up means (t = 3.21, p = .015). However, no significant differences were observed between mean baseline (m = 0.85) and mean scores at 12-month follow-up (m = 0.33; t = 1.00, p = .423).
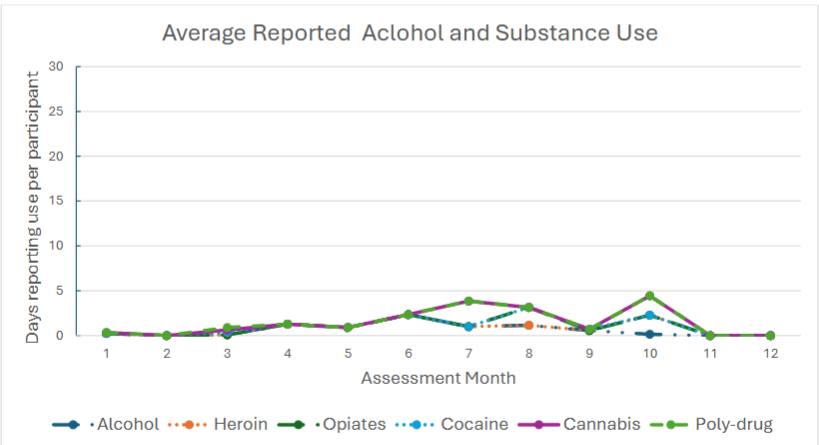
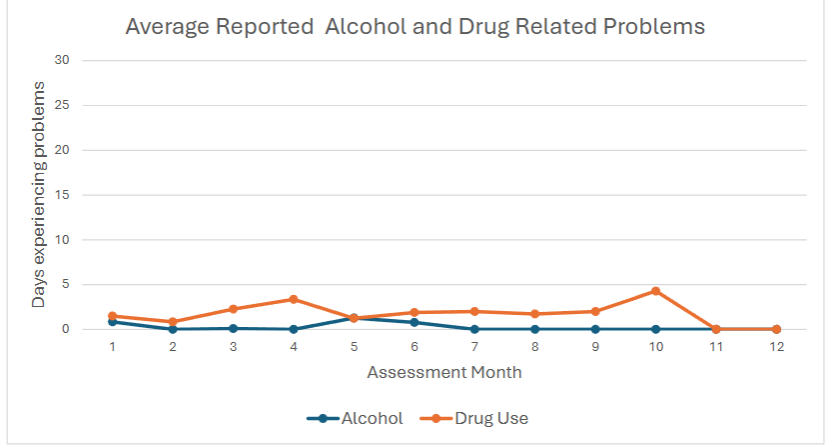
Over half of the participants (58%; n = 7) remained drug free over the course of their time receiving funding. We observed shifting trends in reported daily alcohol consumption from month to month, however these differences were not statistically significant. Similarly, some participants reported substance use during their time in the study. Participants denied misusing methadone or using sedatives, amphetamines, or hallucinogens. One participant reported the use of opiates and heroin at 7-month and 9-month follow-up, respectively. Two participants reported the use of cocaine, one at 2-month follow-up and the other at 9-month follow-up. Four different participants reported cannabis use while receiving rent payments. None of these participants reported use for consecutive months. No significant differences were observed between baseline and follow-up across any substance reported. No participants had a fatal or non-fatal overdose. More than 70% of participants reported they found their treatment as very important or extremely important throughout the duration of their participation except for 6-month follow-up when only 57% reported very high importance or greater.
TREATMENT SERVICES UTILIZED, MEDICAL AND MENTAL HEALTH, EMPLOYMENT AND LEGAL HISTORY
Participants utilized treatment services consistently while receiving funding. On average, participants utilized at least three treatment services while receiving housing vouchers. Medications for substance use disorders, psychiatric services, and self-help/recovery groups were the three most reported used services. Following baseline assessments, only 2 participants reported utilizing Emergency Room services over the course of their time in the housing voucher program and only 1 patient was hospitalized for medical treatment. On average, participants reported experiencing psychological distress for 11.1 (SD = 11.7) days in the previous 30 days.
At baseline, 2 participants reported that they were awaiting trial for pending legal issues. After baseline, all participants denied awaiting any trial, obtaining any drug-related charges, or receiving any charges of driving under the influence. Furthermore, of those who completed baseline assessments, 10 out of the 11 participants reported having a job. The 2 participants who were seeking work at baseline obtained employment. At baseline, participants reported working on average roughly 17 days throughout the month (SD = 9.2). A total of 5 participants reported enrolling in classes or training courses throughout their time in the voucher program.
PROGRAM ASSESSMENT
We examined the efficacy of the program through qualitative statements from participants who completed follow-up and were in contact following completion. Six participants filled out the completion surveys and provided feedback regarding the housing vouchers. These participants reported finding the rent payments helpful to securing housing, with representative statements including that obtaining the housing vouchers was “Great! Love (the) neighborhood” and “It’s really perfect.” All participants indicated that participation afforded them safe housing they otherwise would not have been able to secure. Additionally, they reported these payments helped with maintaining sobriety or reducing substance use issues by reducing stress. For example, one participant reported the rent payments “reduced stress,” and “this funding gave me a cushion which took a lot of stress away.” Others reported the program was “Letting me thrive for my kids keeps me sober” and “It kept me on the right path for a while. It kept me clean for a long time.” The consistent suggestion to providing support to future participants was to provide funding for a longer duration. Participants indicated the barriers that prevent them from accessing safe housing include not having enough money in their savings and having a criminal history.
Discussion
The key aim of this pilot study was to assess the effectiveness of a housing voucher program for women who completed a SUD treatment program. Housing voucher effectiveness was based on participants’ experience securing safe housing, housing security based on the HII, and self-reported alcohol and substance use. We found significant reductions in housing insecurity over the duration of study participation. We also found that participants reported that the program was effective in securing safe housing and assisted participants in maintaining sobriety from substances. And lastly, we found that alcohol and drug use did not increase significantly during receipt of housing vouchers. This is likely due to participants having completed substance use treatment prior to entering the housing voucher program and remaining engaged in services over the duration of receiving funds. Thus, participants were unlikely to experience significant problems related to use over time. Participants who reported use of drugs or alcohol likely were equipped with the skills to cope with return to use and solicit the necessary support to preclude further use. This was evidenced by the fact that no participant reported use in consecutive months. However, stable housing remains a consistent issue, even among those who have received substance use treatment.
Lack of housing is a known risk-factor in maintaining long-term abstinence and managing chronic health conditions, therefore, ensuring safe housing when leaving a treatment program is necessary. The financial support provided through the program enabled participants to prioritize their health and recovery by alleviating economic stress. For these pregnant and parenting women, securing stable and safe housing played a critical role in sustaining recovery behaviors and reducing the risk of relapse. These findings are consistent with previous research indicating that individuals who achieve abstinence are more likely to maintain it when stably housed, compared to those experiencing housing instability. Moreover, structural factors, such as community instability and exposure to violence have been linked to both fatal and non-fatal overdose. Participants who received funding were able to choose housing environments they perceived as safe for themselves and their families, which likely minimized exposure to substance-related cues and triggers. Individuals with SUDs are among the highest utilizers of Emergency Department (ED) services often due to comorbid conditions such as cancer, cardiovascular disease, and soft tissue infections. By maintaining a drug free status and accessing housing support, participants likely reduced their reliance on ED care. Furthermore, employment benefits combined with economic relief, may have facilitated engagement in routine healthcare, promoting patient health and reducing the strain on ED services.
To our knowledge, this is the first study to examine the impact of participation in a contingent housing payment program for women following the completion of substance use disorder treatment. This study provides critical evidence that the financial support offered through monthly rent payments helped women secure safe housing, continue employment, and maintain their recovery. While the extant literature indicates that residential substance use disorder treatment programs are effective in reducing substance use and improving mental health, there are few studies that have examined the significant barrier of procuring safe and secure housing after completing treatment. Addressing this “hand-off” to safe housing can help reduce relapses and fatal overdoses. The current study indicates that a safe and stable housing environment contributed to the ability to commit to and maintain employment among our participants. These perinatal and parenting women likely experienced greater security related to housing and were better able to attend to job responsibilities, increasing the likelihood of taking greater responsibility and the potential of earning a higher salary position. Additionally, employment has been shown to be a positive predictor of reducing relapse rates. Taken together, the housing program demonstrated broad benefits across multiple different domains of the participant’s lives by providing consistently monthly payments to safe housing.
This study has several limitations. First, alcohol and drug use were assessed via self-report. However, self-report has been found to be as accurate as urine drug testing. Second, the sample was only comprised of 12 participants. We were limited to 12 participants due to funding resources. This pilot study provided preliminary evidence of the impact of the housing vouchers in securing safe and stable housing. Future studies would benefit from replication with a larger sample size.
Conclusions
The current study provides preliminary evidence of the effectiveness of a housing voucher program to provide stable housing and reduce alcohol- and drug-related harms. Future evaluations comprehensively assessing outcomes among larger samples will be critical to furthering policy related to accessible and safe housing to patients departing residential substance use programs.
Conflict of Interest Statement: The authors have no conflicts of interest to declare.
Funding Statement: This study was funded by the Van Every Foundation.
Acknowledgements: We extend our gratitude to the families who generously contributed their time and effort to participate in this study.
Sources of support/funding for the work: R01DA047867 NIDA; Van Every Foundation and the North Carolina Collaboratory at The University of North Carolina at Chapel Hill with funding appropriated by the North Carolina General Assembly ID Collab_471
Conflicts of interest: None
References
- Building U.S. Capacity to Review and Prevent Maternal Deaths. (2018). Report from Nine Maternal Mortality Review Committees. https://www.cdcfoundation.org/sites/default/files/files/ReportfromNineMMRCs.pdf
- Trost SL, Busacker A, Leonard M, et al. Pregnancy-Related Deaths: Data from Maternal Mortality Review Committees in 38 U.S. States, 2020. Centers for Disease Control and Prevention, U.S. Department of Health and Human Services; 2024
- Han, B., Compton, W. M., Einstein, E. B., Elder, E., & Volkow, N. D. (2024). Pregnancy and Postpartum Drug Overdose Deaths in the US Before and During the COVID-19 Pandemic. JAMA psychiatry, 81(3), 270–283. https://doi.org/10.1001/jamapsychiatry.2023.452
- Austin, A. E., Shiue, K. Y., Naumann, R. B., Figgatt, M. C., Gest, C., & Shanahan, M. E. (2021). Associations of housing stress with later substance use outcomes: A systematic review. Addictive behaviors, 123, 107076. https://doi.org/10.1016/j.addbeh.2021.107076
- WANG, S., TOLOMICZENKO, G., KOUYOUMDJIAN, F., & GARNER, R. (2005). Interventions to Improve the Health of the Homeless: A Systematic Review. American Journal of Preventive Medicine, 29(4), 311–311. https://doi.org/10.1016/j.amepre.2005.06.017
- Joint Center Housing for Housing Studies of Harvard University. (2024). The state of the nation’s housing. https://www.jchs.harvard.edu/sites/default/files/reports/files/Harvard_JCHS_The_State_of_the_Nations_Housing_2024.pdf
- Gu, K.D., Faulkner, K.C. & Thorndike, A.N. Housing instability and cardiometabolic health in the United States: a narrative review of the literature. BMC Public Health 23, 931 (2023). https://doi.org/10.1186/s12889-023-15875-6
- DiTosto, J. D., Holder, K., Soyemi, E., Beestrum, M., & Yee, L. M. (2021). Housing instability and adverse perinatal outcomes: a systematic review. American journal of obstetrics & gynecology MFM, 3(6), 100477. https://doi.org/10.1016/j.ajogmf.2021.100477
- Green, J. M., Fabricant, S. P., Duval, C. J., Panchal, V. R., Cahoon, S. S., Mandelbaum, R. S., … & Matsuo, K. (2023). Trends, characteristics, and maternal morbidity associated with unhoused status in pregnancy. JAMA Network Open, 6(7), e2326352-e2326352.
- Pantell, M. S., Baer, R. J., Torres, J. M., Felder, J. N., Gomez, A. M., Chambers, B. D., … & Jelliffe-Pawlowski, L. L. (2019). Associations between unstable housing, obstetric outcomes, and perinatal health care utilization. American journal of obstetrics & gynecology MFM, 1(4), 100053.
- Tsai, J. (2020). Is the housing first model effective? Different evidence for different outcomes. American Journal of Public Health, 110(9), 1376.
- Herriott, A. L. (2024). “I just want the best for him.” Pregnancy in the context of substance use disorders: Perspectives of postpartum women. Birth, 51(1), 81-88.
- Frazer, Zane, Krystle McConnell, and Lauren M. Jansson. “Treatment for substance use disorders in pregnant women: Motivators and barriers.” Drug and alcohol dependence 205 (2019): 107652.
- Klaman, S., Andringa, K., Horton, E., Jones, H., 2019. Concurrent opioid and alcohol use among women who become pregnant: historical, current, and future perspectives. Subst. Abuse 13, 1–7.
- Mazel, S., Alexander, K., Cioffi, C., & Terplan, M. (2023). Interventions to Support Engagement in Addiction Care Postpartum: Principles and Pitfalls. Substance abuse and rehabilitation, 14, 49–59. https://doi.org/10.2147/SAR.S375652
- Schiff, D. M., Nielsen, T., Terplan, M., Hood, M., Bernson, D., Diop, H., Bharel, M., Wilens, T. E., LaRochelle, M., Walley, A. Y., & Land, T. (2018). Fatal and Nonfatal Overdose Among Pregnant and Postpartum Women in Massachusetts. Obstetrics and gynecology, 132(2), 466–474. https://doi.org/10.1097/AOG.000000000000273
- Metz, T. D., Rovner, P., Hoffman, M. C., Allshouse, A. A., Beckwith, K. M., & Binswanger, I. A. (2016). Maternal deaths from suicide and overdose in Colorado, 2004–2012. Obstetrics & Gynecology, 128(6), 1233-1240.
- Smid, M. C., Schauberger, C. W., Terplan, M., & Wright, T. E. (2020). Early lessons from maternal mortality review committees on drug-related deaths-time for obstetrical providers to take the lead in addressing addiction. American journal of obstetrics & gynecology MFM, 2(4), 100177. https://doi.org/10.1016/j.ajogmf.2020.100177
- Mattocks, K. M., Clark, R., & Weinreb, L. (2017). Initiation and engagement with methadone treatment among pregnant and postpartum women. Women’s Health Issues, 27(6), 646-651.
- Schauberger, C. W., Borgert, A. J., & Bearwald, B. (2020). Continuation in treatment and maintenance of custody of newborns after delivery in women with opioid use disorder. Journal of Addiction Medicine, 14(2), 119-125.
- Guo, X., Slesnick, N., & Feng, X. (2016). Housing and Support Services with Homeless Mothers: Benefits to the Mother and Her Children. Community mental health journal, 52(1), 73–83. https://doi.org/10.1007/s10597-015-9830-3
- Slesnick, N., Zhang, J., Feng, X., Mallory, A., Martin, J., Famelia, R., Brakenhoff, B., Yilmazer, T., Wu, Q., Ford, J., Holowacz, E., Jaderlund, S., Hatsu, I., Luthy, E., Chavez, L., Walsh, L., & Kelleher, K. (2023). Housing and supportive services for substance use and self-efficacy among young mothers experiencing homelessness: A randomized controlled trial. Journal of substance abuse treatment, 144, 108917. https://doi.org/10.1016/j.jsat.2022.108917
- McLellan, A. T., Kushner, H., Metzger, D., Peters, R., Smith, I., Grissom, G., … & Argeriou, M. (1992). The fifth edition of the Addiction Severity Index. Journal of substance abuse treatment, 9(3), 199-213.
- Farero, A., Sullivan, C. M., López-Zerón, G., Bowles, R. P., Sprecher, M., Chiaramonte, D., & Engleton, J. (2024). Development and validation of the housing instability scale. Journal of Social Distress and Homelessness, 33(1), 142-151.
- Gerber E, Gelberg L, Rotrosen J, Castelblanco D, Mijanovich T, Doran KM. Health-related material needs and substance use among emergency department patients. Substance Abuse. Published online August 2019:1-7. Doi: https://doi.org/10.1080/08897077.2019.163596
- Lin C, Cousins SJ, Zhu Y, et al. A scoping review of social determinants of health’s impact on substance use disorders over the life course. Journal of Substance Use and Addiction Treatment. 2024;166:209484-209484. Doi: https://doi.org/10.1016/j.josat.2024.209484
- Fleury MJ, Cao Z, Grenier G, Huỳnh C. Predictors of Frequent Emergency Department Use and Hospitalization among Patients with Substance-Related Disorders Recruited in Addiction Treatment Centers. International Journal of Environmental Research and Public Health. 2022;19(11):6607. Doi: https://doi.org/10.3390/ijerph1911660
- Zhang X, Wang N, Hou F, et al. Emergency Department Visits by Patients with Substance Use Disorder in the United States. Western Journal of Emergency Medicine. 2021;22(5):1076-1085. Doi: https://doi.org/10.5811/westjem.2021.3.50839
- de Andrade, D., Elphinston, R. A., Quinn, C., Allan, J., & Hides, L. (2019). The effectiveness of residential treatment services for individuals with substance use disorders: A systematic review. Drug and alcohol dependence, 201, 227-235.
- Shadloo, B., Baheshmat, S., Rostam-Abadi, Y., Shakeri, A., Gholami, J., & Rahimi-Movaghar, A. (2022). Comparison of self-reported substance use with biological testing among treatment-seeking patients with opioid use disorder. Journal of substance abuse treatment, 134, 108555.