

Impact of CARES® Training on Dementia Care Practices
Evaluation of Person-Centered Dementia Care Utilizing the CARES® Observational Tool
Erin Cattoor, PhD1, RN; John V. Hobday, MA2
- University of Missouri-Columbia
- HealthCare Interactive, Minneapolis, MN
OPEN ACCESS
PUBLISHED 30 November 2024
CITATION Cattoor, E., and Hobday, JV., 2024. Evaluation of Person-Centered Dementia Care Utilizing the CARES® Observational Tool. Medical Research Archives, [online] 12(11). https://doi.org/10.18103/mra.v12i11.5531
COPYRIGHT © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i11.5531
ISSN 2375-1924
ABSTRACT
The training of staff in residential long-term care facilities, such as nursing homes and assisted living facilities, is increasingly being conducted via asynchronous, online training platforms. Even when organizations have in-person trainers to conduct synchronous training on-site or via online video tele-conferencing formats, a paucity of research has evaluated how training in any form affects staff members’ actual, observable, person-centered care practices, particularly when working with individuals living with Alzheimer’s disease or other related dementias (ADRD).
This study sought to fill this gap by evaluating the impact of the two CARES® online dementia care training programs on staff members’ observable care practices, as measured by the CARES® Observational Tool (COT), a previously published person-centered observational tool. The study hypothesized that staff completion of the two CARES® online training programs would not only result in increased knowledge of ADRD and person-centered care practices within long-term care facilities, but also lead to an observable increase in the use of person-centered care practices, as measured by the COT. A single group pre-test/post-test design was used, which included a baseline, immediate post-test, and one-month post-test data collection interval among the entire staff of a memory care unit (N = 26) at a nursing home in a large Midwestern city in the United States. The results showed statistically significant increases in both ADRD knowledge (p < .0001) and observable person-centered care (p < .0001). The CARES® online training programs and the COT seem to offer a promising solution to address the ongoing and expanding gaps in delivering and demonstrating effective person-centered care to people living with dementia (PLWD) in residential long-term care.
Keywords:
Alzheimer’s Disease, Dementia, Nursing Home, Skilled Nursing, Person-Centered Care, Observational, Quality of Life, Technology, Online Training, Certification
INTRODUCTION
According to the National Center for Health Statistics, nearly half of all nursing home residents in the United States have Alzheimer’s disease or other related dementias (ADRD). The average annual per-person payments for nursing home services among Medicare beneficiaries the age of 65 and over were $16,523 (USD) for people living with Alzheimer’s disease or related dementias (PLWD) compared to $800 (USD) for those without ADRD. Although nursing homes do not necessarily cause the complex, co-occurring conditions and adverse events of ADRD such as falls or delirium, researchers, advocates, and others have noted that the environments and quality of care provided in some nursing homes can exacerbate the severity of dementia symptoms.
The delivery of person-centered care that is tailored and individualized to the preferences, abilities, and needs of people in nursing homes is a core emphasis of efforts to enhance and optimize dementia care in nursing homes. Staffing that is sufficient, assignments that reflect a degree of continuity to facilitate the development of quality relationships between direct and non-direct care providers and residents, and robust training in/modeling of person-centered care principles all appear to influence the quality of life of PLWD in nursing homes.
The need for enhanced knowledge about ADRD and competency in caring for PLWD in nursing homes for staff across care disciplines (e.g., direct care workers, social workers, and therapists) has received national attention and is a consistent recommendation to enhance quality of care in nursing homes or other residential settings. A variety of training programs for nursing home staff have been shown to increase their knowledge and feelings of competence in caring for residents with Alzheimer’s disease. Studies demonstrating positive effects include the use of person-centered communication by staff, application of person-centered care principles as well as dementia care mapping, illustration of person-centered dementia care with day-to-day care routines, and education with ongoing monthly coaching to identify alternative approaches to the use of restraints for PLWD. Conversely, an analysis of existing systematic reviews of randomized control trials (RCTs) assessing educational interventions targeted at formal caregivers determined that there is inadequate evidence to support the broad adoption of any specific intervention, including those focused on non-pharmacological, behavioral interventions for PLWD.
Time also presents an ongoing barrier to disseminating and implementing staff training programs in nursing homes. Due to the organization of staff roles and responsibilities, it is often challenging to deliver in-person, multi-day training programs that reach large numbers of staff. To this end, a systematic review of the literature suggested both in-person and online training interventions that provide education and skills training are effective, can enhance formal and informal caregivers’ condition and readiness, and have a positive impact on staff attitudes with PLWD. There is a lack of research that has evaluated how training in any form affects staff members’ actual, observable, person-centered care practices, particularly with people living with Alzheimer’s disease or other related dementias (ADRD). Although direct observational tools exist related to dementia care, the challenge in conducting observational studies often involves the implementation of complex, time-consuming, and costly observational rating measures. The CARES® Observational Tool (COT) utilized in this study may be a less-complex, less time-consuming, and less costly measure to assess person-centered care for those individuals living with ADRD.
This study evaluated the effectiveness of the asynchronous, interactive, video-based CARES® Dementia 5-Step Method™ and CARES® Dementia Safety Topics™ Online Training and Certification Programs to enhance staff delivery of person-centered care (hereafter referred to as CARES® Online Training). CARES® online training, content, and techniques have previously been shown to increase dementia-care knowledge and person-centered care interactions between staff and PLWD and reduce antipsychotic medication usage with nursing home residents. To evaluate changes to actual, observable care, investigators hypothesized staff completion of the two CARES® online training programs would not only result in increased knowledge of ADRD and person-centered care practices within long-term care facilities, but also lead to an observable increase in the use of person-centered care practices, as measured by the COT, a validated, 16-item tool focused on critical domains of person-centered dementia care interactions and associated with the five steps of the CARES® Dementia 5-Step Method.
METHODS
DESIGN
A single-group, pre-test/post-test design was utilized to evaluate the potential benefits of CARES® Online Training programs on various care staff in a 60-bed memory care unit (MCU) of a single, 120-bed, private pay long-term care facility within a Midwestern suburb of the United States. The COT was utilized to evaluate observable, person-centered care differences. Investigators utilized a non-randomized, self-select methodology for recruiting MCU staff members.
Sample Size.
A convenience sample of direct and non-direct care providers (n = 26) was initially recruited from a pool of staff members working within the MCU (N = 26); 100% of MCU staff members initially participated in the study. Turnover and attrition were anticipated, but due to time constraints, no new staff members replaced participants during the study period.
Recruitment.
Recruitment was conducted by the owners and director of nursing (DON) at the participating facility, in collaboration with the on-site study coordinator. The on-site study coordinator, who also functioned as the study observer, was a PhD candidate, with a Master’s in Nursing. All full-time staff working inside the MCU were invited to participate and agreed to do so.
Inclusion Criteria.
Inclusion criteria for study participants included being a) assigned to work in the MCU; b) classified as either a direct or non-direct care provider within the MCU; c) employed full-time; d) capable of reading English at a sixth-grade level (as evidenced by reading, understanding, and signing the consent form; all were native English speakers); and e) able to operate basic functions on a computer (operating a mouse and typing in a text box, as evaluated by the on-site coordinator; all were proficient in the use of computers and did not report any issues utilizing CARES® Online Training).
PROCEDURES
Recruitment and enrollment.
After a letter of intent was signed with the facility administration, potentially eligible participants were recruited from the MCU. Potentially eligible participants attended a presentation, followed by a question-and-answer session administered by the on-site study coordinator. Two different educational sessions were conducted to include all staff during their respective shifts. A statement was read aloud to the staff that informed them of their right to refuse to participate without any negative consequences to their employment; this was clearly stated on the IRB-approved consent form. During the first contact with participants, the study observer established eligibility. If individuals chose to participate, time was allowed to answer any questions or concerns about the study process. Each participant was presented with an informed consent form approved by a major university’s Internal Review Board (IRB). A private room was available for participants to review and sign consent forms at the time of recruitment. Study participants were also allowed to take the consent home for further review.
Data Collection.
Data collection was conducted throughout the study period. All related activities occurred during the participant’s working schedule, thereby minimizing barriers to participation. Data collection occurred at three different time points; prior to completion of the CARES® Online Training programs (baseline), following CARES® Online Training (post), and the final data point occurred one month following completion of CARES® Online Training (post-post), with additional observations conducted throughout the study period. In face-to-face, on-site interviews, the study observer gathered initial demographic information (job title, level of education, and length of employment at the respective facility) and administered an initial paper-based CARES® Dementia Knowledge Test (CDKT), which was an investigator-designed exam based upon previously validated CARES® Online Training questions. Since the same CDKT measure was administered to the participants at the three study time points, participants were not informed of which test items were answered incorrectly (if applicable). Total time for completion was variable, with most participants completing the CDKT in less than 10 minutes. To assess the effectiveness of the online training on observable person-centered dementia care, the study observer also completed an observation of each participant utilizing the COT before each participant completed the CARES® Online Training. Thereafter, the study observer conducted participant observations onsite weekly, a method agreed to by the participating facility and approved by the university IRB.
ONLINE TRAINING INTERVENTION
The training intervention consisted of the CARES® Dementia 5-Step Method™ Training and Certification Program (4 modules/4 hours) and the CARES® Dementia Safety Topics™ Training and Certification Programs (6 modules/6 hours). Modules were delivered asynchronously by text, audio narration, videos, and animations. Module topics within the CARES® Dementia 5-Step Method program included an introduction to person-centered care, an introduction to dementia, a discussion of behavior as a form of communication, and training on the 5-step CARES® Approach for providing person-centered care. Module topics within the CARES® Dementia Safety Topics program focused on food and fluid intake, recognizing pain, minimizing falls, rethinking wandering, minimizing and reducing restraints, and communication. The 5-step CARES® Approach stands for C – Connect with the person; A – Assess behavior; R – Respond appropriately; E – Evaluate what works; and S – Share with others. It is the cornerstone of CARES® Online Training programs and delineates the CARES® person-centered care delivery process.
Each participant received an individualized introduction to the CARES® Online Training programs. Participant established their own individual login that was not shared with the study observer. Participants were also instructed not to share their personal login information with other staff members. Each participant was then provided time inside the Nurse Educator’s office for completion of the CARES® Online Training programs, which provided a quiet physical space, the technology/hardware required, and uninterrupted time during the participant’s shift to complete the respective modules. Participants were allotted an hour to complete each module, with a minimum time requirement of 40 minutes to visit all screens in each 1-hour module. Participants completed one module per week during their respective shifts over 10 weeks. The modules included a wide variety of real-life (i.e., no actors) video clips and interviews of actual direct and non-direct care staff members, experts, family members, and PLWD.
EVALUATION MEASURES
CARES® Dementia Knowledge Test (CDKT).
The CDKT is a 16-item, investigator-designed, multiple-choice exam based upon previously validated CARES® Online Training questions. Upon the initial creation of the CDKT, it showed good reliability at pretest (Cronbach’s alpha coefficient = 0.94).
Evaluation of Effectiveness of CARES® Observational Tool (COT)
CARES® Observational Tool (COT). The COT is a validated, 16-item tool focused on critical domains of person-centered dementia care interactions, which can be administered unobtrusively during staff shifts. The COT enables a trained observer to assess person-centered, interpersonal skills between direct and non-direct care workers and the PLWD including ongoing assessment of behavior by the direct or non-direct care worker, connections with the PLWD, appropriate responses to behaviors, evaluation of what works, and the sharing of strategies with other staff members. Total score for the COT is 16, with a score of “1” applied for any item observed and a score of “0” applied for any item not observed during participant interactions with residents. The study observer had access to participating staff schedules and did not announce when COT visits would be occurring so as not to impact the research environment.
ANALYSIS
The level of significance for all hypothesis testing was p < .05. The principal hypothesis for this study was that participants will also demonstrate increased knowledge in dementia care, as measured by the CDKT. A secondary hypothesis was that MCU care workers trained with the CARES® Online Training will demonstrate increased, observable person-centered care interactions with the PLWD, as measured by the 16-point COT. For both hypotheses, Friedman’s non-parametric repeated measure was utilized for analysis.
RESULTS
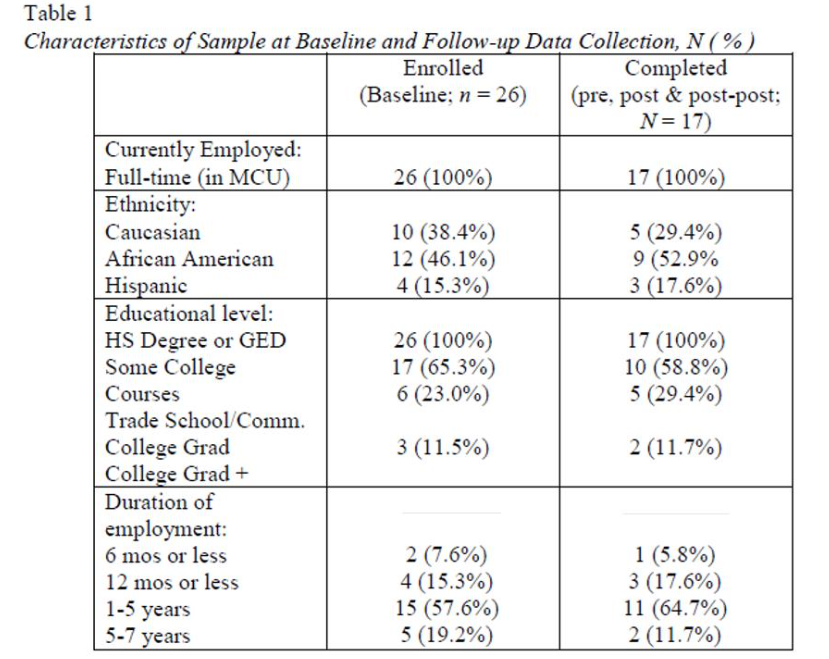
SAMPLE CHARACTERISTICS
Twenty-six (26) full-time direct and non-direct care providers representing various roles and responsibilities within the MCU initially enrolled in the study, which comprised 100% of the staff population of the MCU. These included 14 direct-care providers (9 certified nursing assistants, 3 licensed practical nurses, and 2 registered nurses) as well as 12 non-direct-care providers (3 certified medication technicians, 3 housekeepers, and 6 activity therapists). All participants were women (by chance), and employed full-time within the MCU. Following enrollment, four participants voluntarily withdrew consent, verbalizing a desire to transfer out of the MCU, which was unrelated to the current study. An additional five participants were no longer employed at the study inception. The remaining 17 participants, however, completed all study procedures. A summary of ethnicity, educational level, and duration of employment is included in Table 1.
HYPOTHESIS TESTING
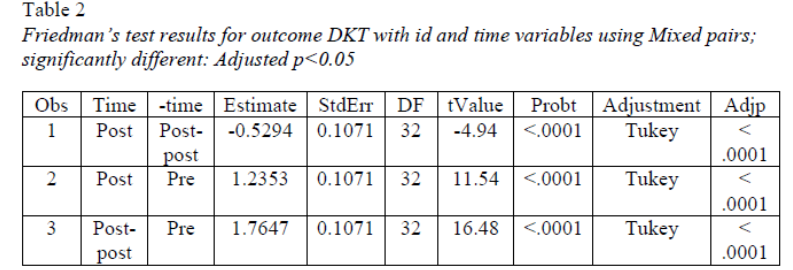
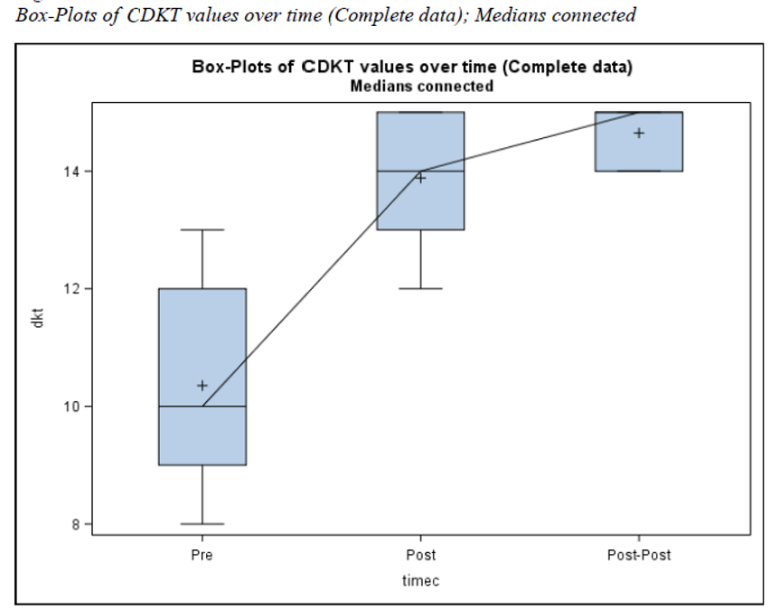
Change in Dementia Knowledge.
Scores on the CDKT increased significantly from baseline in both the immediate follow-up (p <.0001) and the 1-month follow-up (p <.0001) indicating that knowledge of providing dementia care to PLWD increased following completion of the CARES® Online Training and was maintained one month following completion of the program.
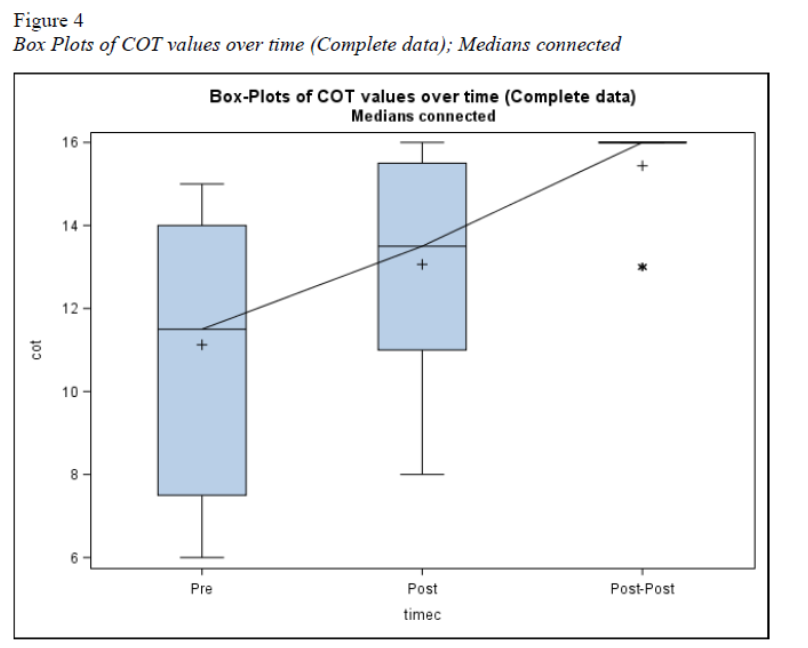
Changes in Observable Person-Centered Care.
Utilizing the COT, the on-site study coordinator conducted a total of 51 individual, unobtrusive observations of the 17 study participants, completing all portions of the study during routine staff-resident interactions. COT scores increased significantly from baseline in both the immediate follow-up observations (p<.0001) and the 1-month follow-up observations (p<.0001). The results suggested that the participants’ observable, person-centered care, as measured by the COT, increased after completing the CARES® Online Training and was sustained one month following program completion.
DISCUSSION
To date, a paucity of research has evaluated how training in any form affects staff members’ actual, observable, person-centered care practices, particularly with people living with Alzheimer’s disease or other related dementias (ADRD). Although direct observational tools exist related to dementia care, the challenge in conducting observational studies often involves the implementation of complex, time-consuming, and costly observational rating measures. In this study, investigators utilized the CARES® Observational Tool, a 16-item tool focused on critical domains of person-centered dementia care interactions, to evaluate the impact of CARES® Online Training on observable person-centered care practices. The tool was shown to be easy-to-use, and effective in evaluating person-centered components of care, demonstrating statistically significant increases in observable person-centered care (p < .0001). The current study builds upon prior research by demonstrating not only an immediate increase in dementia knowledge and observable, person-centered care directly after the completion of the online modules, but also a sustained effect one month following the conclusion of the CARES® online training.
While the COT tool demonstrated the ability to measure person-centered care practices, it may also be suitable as a training option for staff members themselves. In a separate research effort, CARES® Online Training has been shown to decrease the use of antipsychotic medications within the nursing home setting. However, staff still reported frustration due to the lack of alternative approaches to address dementia-related behaviors resulting from such medication reductions. Informal administration of the COT, independent of the current study has also been researched among long-term care facilities that were already utilizing CARES® Online Training COT during individual and group training of direct care workers and other staff members. Initially, staff members were asked to break into a small group of three; one portraying the person living with ADRD, one portraying the direct-care worker delivering care, and one who would utilize the COT to keep track of (i.e., score) observable person-centered care practices. Each group was then asked to conduct role-play scenarios for a particular interaction between the “person living with ADRD” and the “staff member.” After each interaction, small group participants would discuss what person-centered elements they observed. Group members would then switch to a different role, repeating the process until all staff members had rotated through the three roles. Although further, formalized evaluation is necessary, informal results seemed to indicate that the tool itself could also be effective as a staff training activity.
Further evaluation is necessary of newly developed online training programs directed at nursing staff and other supervisors who desire to utilize the COT with staff members. In the current effort, the study observer was directly trained by the developer of the COT over a series of online teleconferencing meetings (e.g., Zoom®). Since widescale dissemination of the COT was desired, an asynchronous training solution was required. A one-hour training was developed to remotely train nursing staff and other supervisors to utilize the COT. To mimic in-person observations, users are asked to view real-life video interactions (i.e., no actors) between actual staff members and individuals living with ADRD and rate them utilizing the 16-point COT. Users are then presented with the correct scored COT for comparison. Multiple examples are presented to help users hone their skills. As with the informal use of the COT for small-group staff training activities, this COT online training program requires a full scientific evaluation.
Few studies have evaluated the effects of online dementia care training on actual, observable care delivery differences, despite national calls to do so. These findings indicate that CARES® Online Training may influence the actual provision of care in the key areas of connections with the PLWD, including effective interpersonal communication, identification and incorporation of personal preference in care routines, and coordination of person-centered techniques with fellow care staff. Moreover, the information and skill development resulting from CARES® Online Training appeared to have a sustained influence on person-centered care delivery over time.
Limitations and Further Research Recommendations.
There are several important limitations to consider when interpreting the findings. The sample is relatively small and was subject to attrition over the study period, potentially biasing the results. Similarly, the evaluation took place in a single MCU, which significantly limits the generalizability of the findings. The sample was entirely female, although this did encompass the entire staff of the selected MCU and does reflect the gender imbalance in nursing home staff in the U.S. Although the inclusion of a measure of observable person-centered care delivery (the COT) is a strength of this study, it was administered and scored by a single study observer, who may have unintentionally introduced bias, since the study observer was not a blinded rater of care activities.
The authors recommend further evaluation and more extensive psychometric testing of the COT measure itself, the use of the COT as a staff training program, the evaluation of a newly developed COT online training program for nursing staff and other supervisors, and pragmatic studies of the COT. The ease of use and administration of the COT by nursing staff and other supervisors, particularly when compared to other more comprehensive approaches such as dementia care mapping, make it a potentially highly useful and feasible tool for widespread, national use in both subsequent research efforts as well as quality improvement in nursing homes or other residential settings that serve high proportions of PLWD.
CONCLUSION
Achieving person-centered care for PLWD in residential long-term care settings remains elusive. Although some interventions may influence/improve the provision of person-centered care, whether these approaches are scalable to the complex and often understaffed and underfunded residential long-term care settings remains unclear. Especially when considering the goal of person-centered care delivery in the context of cataclysmic events to residential long-term care settings, such as COVID-19, the need for easy-to-deliver, asynchronous, easy-to-implement programs to facilitate person-centered care becomes even more imperative.
The use of cost-effective online educational programs for long-term care staff training may be effective in terms of knowledge gain. However, few studies have evaluated whether direct and non-direct caregivers’ observable person-centered care practices can increase as a result of online training utilization. It is important to incorporate and integrate easy-to-use training and observational approaches to potentially enhance the quality of dementia care in a scalable and accessible manner. The findings of this study suggest that CARES® Online Training may be effective in addressing the increasing gaps in providing personalized and effective care to PLWD in residential long-term care. Future research should further evaluate the psychometric properties of the COT tool as well as compare it with other training programs using observational measures.
REFERENCES
- Gaugler JE, Hobday JV, Savik K. The CARES® Observational Tool: A valid and reliable instrument to assess person-centered dementia care. Geriatric Nursing. 2013;34(3):194-198. doi:10.1016/j.gerinurse.2013.01.002
- National Center for Health Statistics. Biennial Overview of Post-acute and Long-term Care in the United States. Accessed November 25, 2023. https://data.cdc.gov/d/wibz-pb5q
- 2020 Alzheimer’s Disease Facts and figures. Alzheimer’s & Dementia. 2020;16(3):391-460. doi:10.1002/alz.12068
- Ma C, Guerra-Santin O, Grave A, Mohammadi M. Supporting dementia care by monitoring indoor environmental quality in a nursing home. Indoor and Built Environment. 2023;32(9): 1843-1861. Doi:10.1177/1420326X231175340
- Gaugler JE, Yu F, Davila HW, Shippee T. Alzheimer’s disease and nursing homes. Health Affairs. 2014;33(4):650-657. doi:10.1377/hlthaff.2013.1268
- Fazio S, Pace D, Flinner J, Kallmyer B. The Fundamentals of Person-Centered Care for Individuals with Dementia. The Gerontologist. 2018;58(suppl_1):S10-S19. doi:10.1093/geront/gnx122
- Person‐Centered Care: a definition and essential elements. Journal of the American Geriatrics Society. 2015;64(1):15-18. doi:10.1111/jgs.13866
- Spilsbury K, Hewitt C, Stirk L, Bowman C. The relationship between nurse staffing and quality of care in nursing homes: A systematic review. International Journal of Nursing Studies. 2011;48(6):732-750. doi:10.1016/j.ijnurstu.2011.02.014
- Kuske B, Hanns S, Luck T, Angermeyer MC, Behrens J, Riedel-Heller SG. Nursing home staff training in dementia care: a systematic review of evaluated programs. International Psychogeriatrics. 2006;19(5):818-841. doi:10.1017/s1041610206004352
- Shaw C, Williams KN, Perkhounkova Y. Educating nursing home staff in dementia Sensitive communication: Impact on antipsychotic medication use. Journal of the American Medical Directors Association. 2018;19(12):1129-1132. doi:10.1016/j.jamda.2018.09.030
- Williams KN, Perkhounkova Y, Jao YL, et al. Person-Centered Communication for Nursing home Residents with Dementia: Four communication analysis methods. Western Journal of Nursing Research. 2017;40(7):1012-1031. doi:10.1177/0193945917697226
- Yasuda M, Sakakibara H. Care staff training based on person-centered care and dementia care mapping, and its effects on the quality of life of nursing home residents with dementia. Aging and Mental Health/Aging & Mental Health. 2016;21(9):991-996. doi:10.1080/13607863.2016.1191056
- Inker J, Jensen C, Barsness S, Stewart MM. Implementing Microlearning in Nursing Homes: Implications for policy and Practice in Person-Centered Dementia Care. Journal of Applied Gerontology. Published online June 11, 2020:073346482092983. doi:10.1177/0733464820929832
- Jacobsen FF, Mekki TE, Førland O, et al. A mixed method study of an education intervention to reduce use of restraint and implement person-centered dementia care in nursing homes. BMC Nursing. 2017;16(1). doi:10.1186/s12912-017-0244-0
- Testad I, Mekki TE, Førland O, et al. Modeling and evaluating evidence‐based continuing education program in nursing home dementia care (MEDCED)—training of care home staff to reduce use of restraint in care home residents with dementia. A cluster randomized controlled trial. International Journal of Geriatric Psychiatry. 2015;31(1):24-32. doi:10.1002/gps.4285
- Sefcik JS, Boltz M, Dellapina M, Gitlin LN. Are interventions for formal caregivers effective for improving dementia care? A Systematic Review of Systematic Reviews. Innovation in Aging. 2022;6(2). doi:10.1093/geroni/igac005
- Jutkowitz E, Brasure M, Fuchs E, et al. Care‐Delivery interventions to manage agitation and aggression in dementia nursing home and assisted living residents: a systematic review and meta‐analysis. Journal of the American Geriatrics Society. 2016;64(3):477-488. doi:10.1111/jgs.13936
- Pleasant M, Molinari V, Dobbs D, Meng H, Hyer K. Effectiveness of online dementia caregivers training programs: A systematic review. Geriatric Nursing. 2020;41(6):921-935. doi:10.1016/j.gerinurse.2020.07.004
- Dobbs D, Hobday J, Roker R, Kaas MJ, Molinari V. Certified nursing assistants’ perspectives of the CARES® activities of daily living dementia care program. Appl Nurs Res. 2018 Feb;39:244-248. doi: 10.1016/j.apnr.2017.11.016
- Pleasant ML, Molinari V, Hobday JV, Fazio S, Cullen N, Hyer K. An evaluation of the CARES® Dementia Basics Program among caregivers. Int Psychogeriatr. 2017 Jan;29(1):45-56. doi:10.1017/S1041610216001526
- McKenna M, Brown LJ, Muller C, Vikram A, Berry K. The impact of psychosocial training on staff attitudes towards people living with dementia: A systematic review. International Journal of Older People Nursing. 2023 May;18(3):e12528. doi:10.1111/opn.12528
- Snow AL, Jacobs ML, Palmer JA, Parmelee PA, Allen RS, Wewiorski NJ…Hartmann CW. Development of a new tool for systematic observation of nursing home resident and staff engagement and relationship. The Gerontologist. 2018;58(2), e15-e24.
- Casey A-N, Low L-F, Goodenough B, Fletcher J, Brodarty H. Computer-assisted direct observation of behavioral agitation, engagement, and affect in long-term care residents. Journal of the American Medical Directors Association. 2014;15(7):1525-8610. https://doi.org/10.1016/j.jamda.2014.03.006
- Ellis-Gray SL, Riley GA, Oyebode JR. Development and psychometric evaluation of an observational coding system measuring person-centered care in spouses of people with dementia. International Psychogeriatrics. 2014;26(11):1885-1895. doi:10.1017/S1041610214001215
- Gilmore-Bykovskyi AL. Caregiver person-centeredness and behavioral symptoms during mealtime interactions: Development and feasibility of a coding scheme. Geriatric Nursing. 2015;36(2) Supplement:S10-S15. https://doi.org/10.1016/j.gerinurse.2015.02.018
- Gaugler JE, Hobday JV, Robbins JC, Barclay MP. Direct care worker training to respond to the behavior of individuals with dementia. Gerontology & Geriatric Medicine. 2016;2:233372141562688. doi:10.1177/2333721415626888
- Hobday JV, Gaugler JE, Mittelman MS. Feasibility and utility of online dementia care training for hospital staff: the CARES® Dementia-Friendly Hospital™ Program. Research in Gerontological Nursing. 2017;10(2):58-65. doi:10.3928/19404921-20170131-01
- Hobday JV, Gaugler JE, Joly LK, Rosopa PJ, Graham BA, CicchinelliA, Lunde AM, Mittelman MS. Efficacy of the CARES® Dementia 5-Step Method for Hospitals™ online training and certification for hospital staff. (In press). Geriatric Nursing
- Roberts E, Schneider EC, Dale M, Henage CB, Kelley CJ, Busby-Whitehead J. Implementation and outcomes of a dementia-friendly training program in five hospitals. (In press). Geriatric Nursing.
- Bradford R, Smith L, Jennings J. Evaluation of an online dementia training program to reduce antipsychotic medication use in a nursing home. Journal of Gerontological Nursing. 2023;49(7):5-8. https://doi.org/10.3928/00989134-20230615-02