





Impact of COVID-19 on Lung Cancer Diagnosis and Care
The Association of COVID-19 and Patients Diagnosed with Lung Cancer
Danielle Hanuschak BS¹, Mallori DePiero BS², Melissa DeMoraes MBA², Shamoore Bailly MPH², Muni Rubens PhD², Paul Lindeman MD², Mark Dylewski MD¹˒², John DeRosimo MD¹˒², Michael Zinner MD¹˒², Geoffrey Young MD¹˒²
- Herbert Wertheim College of Medicine, Florida International University;
- Miami Cancer Institute, Baptist Health South Florida
OPEN ACCESS
PUBLISHED: 30 September 2024
CITATION: Hanuschak, D., et al., 2024. The Association of COVID-19 and Patients Diagnosed with Lung Cancer. Medical Research Archives, [online] 12(9).
https://doi.org/10.18103/mra.v12i9.5823
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i9.5823
ISSN 2375-1924
ABSTRACT
Objectives: The COVID-19 pandemic’s impact on the healthcare system resulted in decreased rates of screening, diagnosis, and treatment of lung malignancies. Long-term longitudinal studies are needed to analyze resultant stage migration.
Materials and Methods: Retrospective cohort study of patients diagnosed with a primary thoracic malignancy (lung, main bronchus, hilum, and carina) who received first-course therapy at a single institution. Clinical and pathological staging values were compared utilizing 12 and 22-month timeframes before (pre-COVID-19) and after (post-COVID-19) the outbreak of the pandemic.
Results: A total of 1,002 patients with clinical stage 0 to IV and 538 patients with pathological stage 0 to IV were analyzed in the pre-COVID-19 and post-COVID-19 populations. Between the 12-month pre- and post-COVID-19 groups, clinical T4 significantly increased (+9.68%). In the 22-month pre- and post-COVID-19 groups, clinical T2 decreased (-7.15%) and T4 increased (+11.53%), pathological T2 decreased (-8.97%) and T4 increased (+8.89%), clinical N2 increased (+6.26%), pathological N0 decreased (-9.22%) and N2 increased (+8.91%), clinical M0 decreased (-8.47%) and M1 increased (+8.47%), pathologic M0 decreased (-11.23%) and M1 increased (+11.23%), clinical stage II decreased (-4.28%) and IV increased (+7.78%), and pathologic stage II decreased (-8.06%) and stage IV increased (+11.08%).
Conclusions: Following the COVID-19 pandemic, significant decreases in the number and availability of lung cancer screenings emerged. This study found statistically significant stage migration at initial diagnosis, particularly when analyzing lengthened time periods of 22 months post-COVID-19 compared to 12 months. Stage migration following the COVID-19 pandemic appears to become more distinguished over time.
Keywords: Thoracic malignancies, lung cancer, COVID-19, pandemic, stage migration
Introduction
On March 11, 2020, the World Health Organization (WHO) declared the global COVID-19 pandemic, a disease caused by a novel enveloped RNA betacoronavirus named severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).¹ Since then, the virus has produced unforeseen consequences for the United States healthcare system caused by the reallocation of resources and additional efforts aimed to contain the spread of disease. Specifically, the pandemic lockdown and ensuing waves significantly decreased rates of screening, diagnosis, and treatment for several different cancer types, including lung cancer.²˒³
As the second most common cancer and leading cause of cancer death in the United States, timely lung cancer screenings are critical for obtaining early-stage diagnosis, and therefore better prognosis with amenable treatment response.⁴ However, to mitigate risks of exposing vulnerable patients and to adapt to evolving pandemic circumstances, it was deemed appropriate to defer screening and lung nodule investigations during the COVID-19 pandemic.⁵ A likely subsequent result, a decrease in the number of biopsies and newly identified thoracic malignancies emerged.⁶˒⁷ Newly discovered evidence suggests these effects caused by the COVID-19 pandemic are now resulting in significant advancements in initial stage at presentation of lung cancer compared to pre-COVID-19 time periods.⁸⁻¹⁴ Alternatively, there are also contrary reports which did not identify any significant changes in stage at presentation of lung cancers post-COVID-19. These conflicting results may be explained by an increase in incidental early tumor stage detection due to diagnostic workup related to COVID-19 infection.¹⁵˒¹⁷
To thoroughly analyze the effects of the COVID-19 pandemic on stage migration of thoracic malignancies such as lung cancer, long-term longitudinal studies are required. The investigation of the comprehensive association of the COVID-19 pandemic and lung cancer stage migration has been limited by restricted pre- and post-COVID-19 observation periods of 4-13 months while the pandemic progressed.⁹˒¹¹˒¹⁴˒¹⁶˒¹⁷ This study aims to evaluate pre- and post-COVID-19 outbreak data of extended time periods up to 22 months, which captures the results of the initial COVID-19 wave, delta wave, and omicron wave. We hypothesize there will be significant advancement in clinical and pathological staging in patients who presented with thoracic malignancies (specifically lung, main bronchus, hilum, and carina) in the post-COVID-19 period compared to those who presented pre-COVID-19 due to the pandemic’s extensive impact on the healthcare system.
Materials and Methods
After receiving institutional review board approval, a retrospective analysis was completed for Miami Cancer Institute (MCI) patients diagnosed with a primary thoracic malignancy at Baptist Hospital South Florida (BHSF)/MCI that had all or part of their first-course therapy at BHSF/MCI. Thoracic malignancies investigated in the study include cancers of the upper, middle, and lower lung lobes, main bronchus, hilum, and carina. The analysis aimed to compare 2 populations – patients with a diagnosis date before (pre-COVID-19) and after (post-COVID-19) the onset of the pandemic. Data available via the American College of Surgeon’s National Cancer Database (NCDB) Participant User Files (PUF’s) was extracted from the Miami Cancer Institute’s Cancer Data Registry. Demographic data as well as diagnostic data including diagnosis date, topography code, and histology were collected. AJCC 8ᵗʰ edition TNM pathological and clinical staging data, as well as clinical and pathological grade data, were also collected.
Clinical and pathological diagnosis staging values were compared 22 months pre-COVID-19 (05/01/2018 – 02/29/2020) and 22 months post-COVID-19 (04/01/2020 – 01/31/2022). Diagnoses from 03/01/2020 – 03/31/2020 were not included in the analysis as this date range was identified as the start of the COVID-19 pandemic and would disproportionally skew the data. A secondary comparison was completed for diagnosis dates 12 months pre-COVID-19 and 12 months post-COVID-19. The secondary 12- month sub-analysis was performed to account for possible staging value increases diagnosed closer to the COVID-19 pandemic start.
Descriptive statistics were used to describe and compare the study population between pre-COVID-19 and post-COVID-19 periods. Frequencies and percentages were used to describe the population. Comparison of pre-COVID-19 and post-COVID-19 periods was done using Chi-square test. SAS version 9.4 was used for data analysis. Statistical significance was set at P<0.05 and all tests were two-tailed.
Results focused on the association of the COVID-19 pandemic as it relates to appropriate clinical and pathological staging. Based on anecdotal data, it was hypothesized that clinical and pathological staging values would be higher at diagnosis post-COVID-19 due to resource restriction and decreased utilization of elective or preventative healthcare caused by the pandemic.
Results
There were 1,129 patients diagnosed with a primary, malignant thoracic cancer (lung, main bronchus, hilum, and carina) from 05/01/2018 – 02/29/2020 and 04/01/2020 – 01/31/2022. Within this population, 127 patients did not have a clinical stage documented and 591 did not have a pathological stage documented, accounting for 11.25% and 52.35% of the population, respectively. The missing data is explained by the cancer registry data collecting procedures. Specifically, cancer registry data collection is retrospective and abstracted once, after diagnosis, limiting data availability. Therefore, this population was excluded due to the lack of staging present at the time of cancer registry patient abstraction. A greater number of patients were excluded from the pre-COVID-19 population due to missing pathological stages.
The remaining 1,002 patients with clinical stage 0 to IV and 538 patients with pathological stage 0 to IV were compared and analyzed. Statistically significant differences in the demographic variables for the pre-COVID-19 and post-COVID-19 populations are denoted in Table 1.
Table 1: Demographic Variables
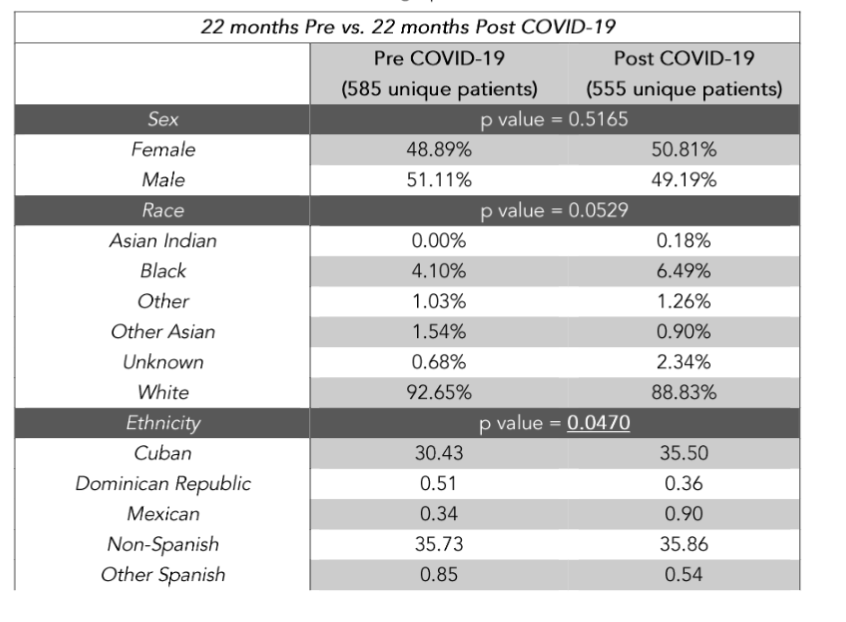
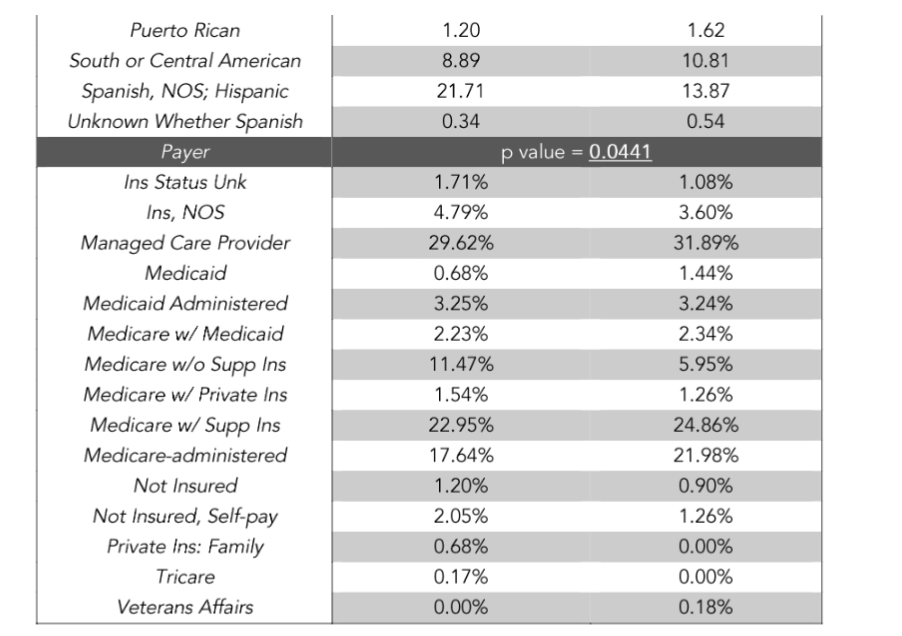
Caption: Comparison of demographic variables (sex, race, ethnicity, and payer) between 22 months pre- and post-COVID-19 populations. Underlined p-value indicates statistical significance.
22 MONTHS PRE- AND POST-COVID-19
In the analysis of patients diagnosed 22 months pre-COVID-19 and 22 months post-COVID-19, there was a statistically significant decrease (-7.15%) between those diagnosed with clinical T2 (Table 2) and a statistically significant increase (+11.53%) for those diagnosed with clinical T4 (Table 2). Also noted was a statistically significant decrease (-8.97%) between those diagnosed with pathological T2 (Table 3) and a statistically significant increase (+8.89%) for those diagnosed with pathological T4 (Table 3).
There was a statistically significant increase (+6.26%) between the number of patients diagnosed with clinical N2 (Table 2), a statistically significant decrease (-9.22%) for those diagnosed with pathological N0 (Table 3), and a statistically significant increase (+8.91%) for those diagnosed with pathological N2 (Table 3).
There was a statistically significant decrease (-8.47%) of patients diagnosed with clinical M0 (Table 2) and a statistically significant increase (+8.47%) for those diagnosed clinical M1 (Table 2). Also noted was a statistically significant decrease (-11.23%) of patients diagnosed with pathological M0 (Table 3) and a statistically significant increase (+11.23%) for those diagnosed with pathological M1 (Table 3).
Within the patient population, there was a statistically significant decrease (-4.28%) between those diagnosed with clinical stage II (Figure 1) and a statistically significant increase (+7.78%) for those diagnosed with clinical stage IV (Figure 1). There was also a statistically significant decrease (-8.06%) between those diagnosed with pathological stage II (Figure 2) and a statistically significant increase (+11.08%) for those diagnosed with pathological stage IV (Figure 2).
Patients with both clinical and pathological T, N, and M values were further compared to determine if there were disparities between the diagnosed clinical and pathological T, N, and M staging values. Table 4 can be referenced for the population stratification.
Table 2: Clinical AJCC TNM Values Pre vs. Post COVID-19
22 months Pre vs. 22 months Post COVID-19
Pre COVID-19 (505 unique patients)
Post COVID-19 (497 unique patients)
12 months Pre vs. 12 months Post COVID-19
Pre COVID-19 (267 unique patients)
Post COVID-19 (275 unique patients)
Thoracic (lung, main bronchus, hilum, and carina)
| Stage | 22 mo Pre | 22 mo Post | p value | 12 mo Pre | 12 mo Post | p value |
|---|---|---|---|---|---|---|
| T0 | 1.06% | 0.63% | 0.468 | 0.79% | 0.37% | 0.526 |
| T1 | 41.01% | 37.87% | 0.320 | 41.27% | 36.19% | 0.234 |
| T2 | 23.68% | 16.53% | 0.005 | 22.62% | 16.79% | 0.094 |
| T3 | 16.07% | 15.27% | 0.735 | 16.27% | 17.91% | 0.619 |
| T4 | 18.18% | 29.71% | <.0001 | 19.05% | 28.73% | 0.009 |
| N0 | 47.61% | 44.58% | 0.344 | 47.01% | 47.96% | 0.829 |
| N1 | 7.48% | 5.52% | 0.214 | 6.77% | 3.35% | 0.073 |
| N2 | 29.94% | 36.20% | 0.038 | 31.47% | 37.55% | 0.145 |
| N3 | 14.97% | 13.70% | 0.573 | 14.74% | 11.15% | 0.222 |
| M0 | 55.49% | 47.02% | 0.006 | 55.51% | 48.74% | 0.111 |
| M1 | 44.51% | 52.98% | 0.006 | 44.49% | 51.26% | 0.111 |
Caption: Clinical AJCC TNM values of study participants comparing pre-COVID-19 and post-COVID-19 timeframes. T = tumor, N = nodal, M = metastases. Highlighted p-value indicates statistical significance.
Table 3: Pathological AJCC TNM Values Pre vs. Post COVID-19
22 months Pre vs. 22 months Post COVID-19
Pre COVID-19 (266 unique patients)
Post COVID-19 (272 unique patients)
12 months Pre vs. 12 months Post COVID-19
Pre COVID-19 (156 unique patients)
Post COVID-19 (160 unique patients)
Thoracic (lung, main bronchus, hilum, and carina)
| Stage | 22 mo Pre | 22 mo Post | p value | 12 mo Pre | 12 mo Post | p value |
|---|---|---|---|---|---|---|
| T0 | 1.78% | 1.22% | 0.617 | 0.76% | 1.35% | 0.630 |
| T1 | 49.78% | 47.15% | 0.569 | 48.48% | 41.22% | 0.222 |
| T2 | 28.89% | 19.92% | 0.023 | 25.76% | 24.32% | 0.782 |
| T3 | 9.33% | 12.60% | 0.258 | 12.12% | 12.84% | 0.856 |
| T4 | 10.22% | 19.11% | 0.006 | 12.88% | 20.27% | 0.098 |
| N0 | 67.83% | 58.61% | 0.037 | 66.91% | 59.44% | 0.196 |
| N1 | 10.87% | 7.79% | 0.247 | 8.82% | 7.69% | 0.731 |
| N2 | 16.09% | 25.00% | 0.016 | 18.38% | 25.87% | 0.132 |
| N3 | 5.22% | 8.61% | 0.147 | 5.88% | 6.99% | 0.705 |
| M0 | 69.78% | 58.55% | 0.005 | 68.10% | 60.12% | 0.133 |
| M1 | 30.22% | 41.45% | 0.005 | 31.90% | 39.88% | 0.133 |
Caption: Pathological AJCC TNM values of study participants comparing pre-COVID-19 and post-COVID-19 timeframes. T = tumor, N = nodal, M = metastases. Highlighted p-value indicates statistical significance.
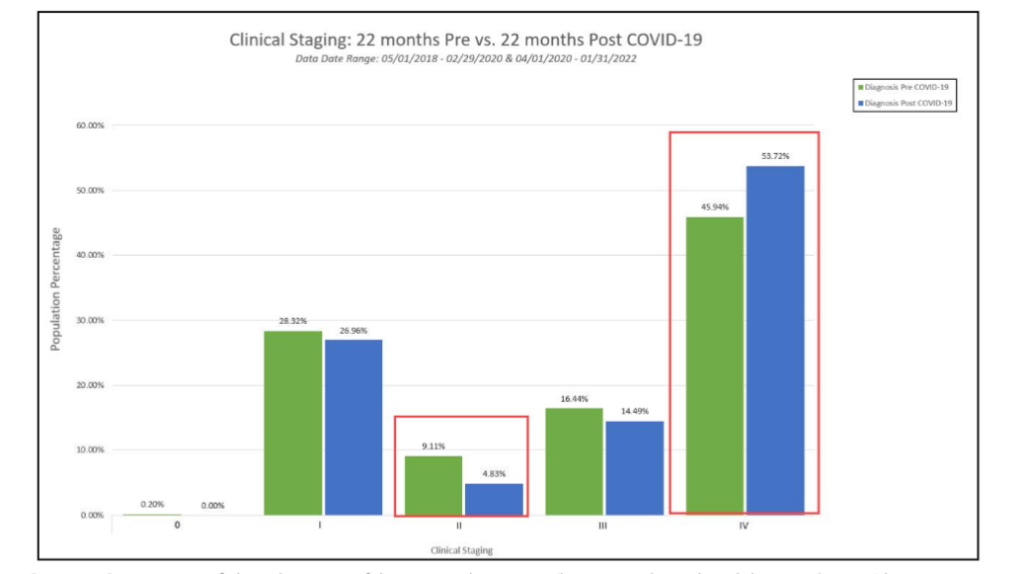
Figure 1: Diagnosed Clinical Stages 22 Months Pre vs. 22 Months Post COVID-19
Caption: Comparison of clinical staging of thoracic malignancies (lung, main bronchus, hilum, and carina) between pre-COVID-19 and post-COVID-19 study participants. Statistically significant changes in clinical stage II and IV are highlighted.
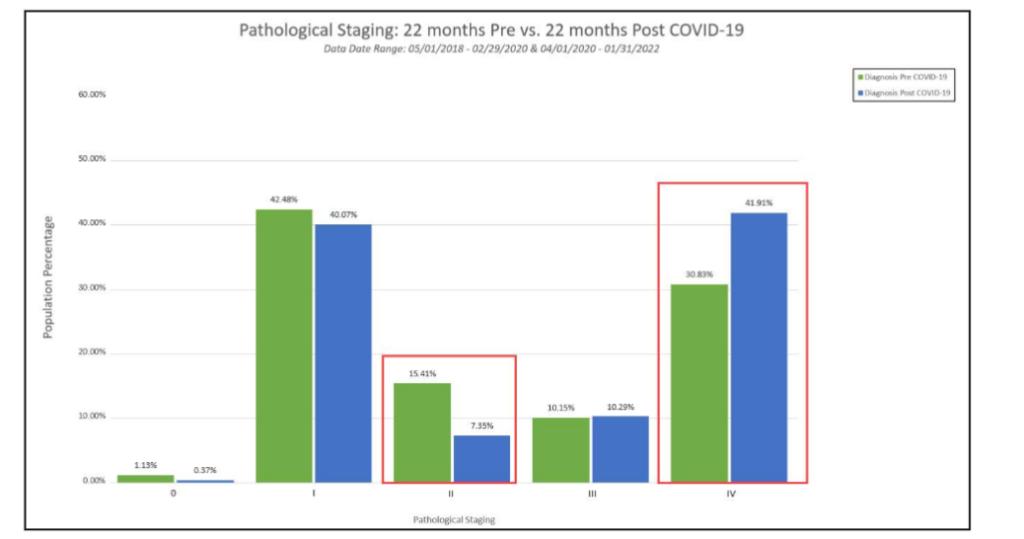
Figure 2: Diagnosed Pathological Stages 22 Months Pre vs. 22 Months Post COVID-19
Caption: Comparison of pathological staging of thoracic malignancies (lung, main bronchus, hilum, and carina) between pre-COVID-19 and post-COVID-19 study participants. Statistically significant changes in pathological stage II and IV are highlighted.
Table 4: Disparate Clinical vs. Pathological AJCC TNM Values
22 months Pre vs. 22 months Post COVID-19
| Comparison | Pre COVID-19 | Post COVID-19 |
|---|---|---|
| Clinical T = Pathological T | 63.84% | 54.81% |
| Clinical T ≠ Pathological T | 36.16% | 45.19% |
| Clinical N = Pathological N | 59.69% | 54.45% |
| Clinical N ≠ Pathological N | 40.31% | 45.55% |
| Clinical M = Pathological M | 50.35% | 47.01% |
| Clinical M ≠ Pathological M | 49.65% | 52.99% |
Caption: Population stratification comparing clinical and pathological tumor (T), nodal (N), and metastases (M) values.
12 MONTHS PRE- AND POST-COVID-19
When comparing the patient population diagnosed 12 months pre-COVID-19 and 12 months post-COVID-19, there was a statistically significant increase (+9.68%) between those diagnosed with clinical T4 (Table 2).
No statistical significance was noted for the patient population when analyzing the clinical or pathological N values, M values, and staging diagnosed 12 months pre- and 12 months post-COVID-19.
Discussion
This extended study analyzing thoracic malignancies (lung, main bronchus, hilum, and carina) from the fourth busiest cancer center in the state of Florida illustrates the effects the COVID-19 pandemic had on resultant stage migration. Review of our institutional pre-COVID-19 and post-COVID-19 data revealed statistically significant differences in clinical and pathological stage of lung cancers at initial diagnosis. These results highlight the aftermath of reallocation of resources and additional efforts aimed to contain the spread of disease ultimately leading to decreased rates of screening and diagnosis of lung cancer.
During post-COVID-19 time periods, annual lung cancer screening with low-dose computer tomography scans decreased as much as 72% and the number of lung cancer diagnoses decreased by 39%.² Our study indicates lengthened follow-up observation periods are needed to fully understand the extent of resultant stage migration from these occurrences.
When comparing 12 months pre- and post-COVID-19, limited statistically significant stage migration findings were captured, specifically only for clinical T4. However, when increasing our data window to 22 months pre- and post-COVID-19, more substantial stage migration changes were found across all tumor, nodal, and metastases stages. In particular, overall trends show more advanced stages increased while earlier stages decreased. Notably, clinical T4 further increased by 11.53%, up from the 9.68% seen in the 12-month post-COVID-19 sample. Overall, while earlier clinical T2, M0, stage II decreased, advanced clinical T4, N1, and stage IV increased. Additionally, while earlier pathological T2, N0, M0, and stage II decreased, advanced pathological T4, N2, M1, and stage IV increased. These results characterize increased distinguishment of stage migration in thoracic malignancies (lung, main bronchus, hilum, and carina) at initial diagnosis over extended time periods.
In contrast to our results with an expanded observational period of 22-months, there are previous reports in the literature which utilized a shorter study timeframe that did not find any significant changes in stage migration. An earlier retrospective study at a large regional medical center utilizing pre- and post-COVID-19 timeframes of 6 months found no statistically significant differences in clinical staging between the two populations. Moreover, they reported the proportion of patients with stage I-II lung cancer in the pre-COVID-19 group was 84.6% while the post-COVID-19 group was 87.5% without any statistically significant difference between the two groups.¹⁷ These findings likely correspond to the limited time interval utilized before and after the onset of the pandemic. Another retrospective multi-center cohort study analyzing data from 8 months post-COVID-19 did not find any changes in initial tumor stage for diagnosed lung cancers. However, it was postulated incidental new diagnoses may have been discovered at an early tumor stage due to chest CT scans related to COVID-19 diagnostic workup.¹⁵ Therefore, the findings may have been influenced by increased chest imaging procedures secondary to the pandemic, thereby leading to earlier lower stage diagnoses which would have gone undetected otherwise. In addition to the shorter time period which was studied, these incidental findings may have mitigated any stage migration. Future studies should continue to analyze changes in lung cancer staging with longer observational periods to account for such factors.
Although the true effects of the COVID-19 pandemic on lung cancer staging is still under debate at this time, previous reports have also indicated advancements in stage migration similar to our study. Several retrospective studies with observational periods ranging from 4-12 months post-COVID-19 reported increases in the number of patients diagnosed with more advanced lung cancer compared to pre-pandemic times.⁹˒¹¹˒¹⁴ Further expansion of the analyzed timeframe to 24 months after the onset of the pandemic also revealed a significant increase in advanced disease.¹⁸ These findings highlight the need for continuous monitoring to understand the full scale of stage migration. Another study examining individual terms within the pandemic found migration in initial staging of lung cancer in later terms of the pandemic compared to the beginning of the pandemic’s onset.¹⁰ Similarly, our study found more substantial stage migration when expanding the observed timeframe to 22 months compared to 12 months. The pattern of detecting advancements in disease with lengthened time intervals reflect the importance of extended observation periods to capture the comprehensive effect of the COVID-19 pandemic on lung cancer staging. To fully characterize the magnitude of stage migration caused by the COVID-19 pandemic, additional multi-institutional studies are needed to detect these advancements as they present later in time.
STUDY LIMITATIONS
There are several limitations within this study. Inherent constraints exist due to the study’s design as a retrospective cohort study. Despite coming from the fourth busiest cancer center in the state of Florida, the generalizability of the data and results may not represent an accurate prediction of outcomes for other cancer institutions or areas around the country. Limitations to applying our results nationwide may be due to the specific socioeconomic factors attributed to the demographic of the South Florida patient population analyzed. There may have also been limitations of the database used in terms of accuracy. An additional limitation involves the exclusion of patients due to lack of clinical (11.25%) and pathological (52.53%) staging data due to restrictions from how data extraction from the cancer registry is completed. Larger multi-institutional studies from various regions are needed to reduce the impact of these interfering variables and better isolate the outcome of interest. Despite attempts to ensure the COVID-19 pandemic as the predominant cause of lung cancer state migration, additional unaccounted factors may have influenced the findings.
Conclusions
Following the onset of the COVID-19 pandemic, significant decreases in the number and availability of lung cancer screenings emerged secondary to reallocation of resources and additional efforts aimed to contain the spread of disease. After healthcare operations resumed for non-emergent and preventative care, statistically significant stage migration at initial diagnosis of lung cancers appeared. Such findings were especially true in this study, particularly when analyzing lengthened time periods of 22 months post-COVID-19 compared to 12 months. Overall, our expanded study time intervals detected statistically significant stage migration in thoracic malignancies (lung, main bronchus, hilum, and carina) compared to previous studies with limited observation periods of 8 months or less which did not find any significant differences between pre- and post-COVID-19 populations.¹⁵˒¹⁷ The findings described in this study indicate a substantial impact from lack of screening and delayed diagnoses, as resultant stage migration appears to become more distinguished over time. Despite thoracic malignancy and lung cancer treatment guidelines not being revised at this time, these observed changes are imperative to account for as they further illustrate the importance of prioritizing decreasing screening and care delays for future pandemics or health crises. Future studies with extended observational periods of up to five years when attainable are required to better characterize the extensive influence of COVID-19 on patients with thoracic and lung cancers as stage migration may continue further.
Acknowledgements and Disclosures
N/A
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
1. Cucinotta D, Vanelli M. WHO Declares COVID-19 a Pandemic. Acta Biomed. 2020;91(1): 157-160. Published 2020 Mar 19. doi:10.23750/abm.v91i1.9397
2. Barsouk A, Saginala K, Aluru JS, Rawla P, Barsouk A. US Cancer Screening Recommendations: Developments and the Impact of COVID-19. Med Sci (Basel). 2022;10(1):16. Published 2022 Mar 1. doi:10.3390/medsci10010016
3. Van Haren RM, Delman AM, Turner KM, et al. Impact of the COVID-19 Pandemic on Lung Cancer Screening Program and Subsequent Lung Cancer. J Am Coll Surg. 2021;232(4):600-605. doi:10.1016/j.jamcollsurg.2020.12.002
4. US Preventive Services Task Force, Krist AH, Davidson KW, et al. Screening for Lung Cancer: US Preventive Services Task Force Recommendation Statement. JAMA. 2021;325(10):962-970. doi:10.1001/jama.2021.1117
5. Mazzone PJ, Gould MK, Arenberg DA, et al. Management of Lung Nodules and Lung Cancer Screening During the COVID-19 Pandemic: CHEST Expert Panel Report. Chest. 2020;158(1):406-415. doi:10.1016/j.chest.2020.04.020
6. Kaufman HW, Chen Z, Niles J, Fesko Y. Changes in the Number of US Patients With Newly Identified Cancer Before and During the Coronavirus Disease 2019 (COVID-19) Pandemic [published correction appears in JAMA Netw Open. 2020 Sep 1;3(9):e2020927. doi: 10.1001/jamanetworkopen.202 0.20927]. JAMA Netw Open. 2020;3(8):e2017267. Published 2020 Aug 3. doi:10.1001/jamanetworkopen.2020.17267
7. Patt D, Gordan L, Diaz M, et al. Impact of COVID-19 on Cancer Care: How the Pandemic Is Delaying Cancer Diagnosis and Treatment for American Seniors. JCO Clin Cancer Inform. 2020; 4:1059-1071. doi:10.1200/CCI.20.00134
8. Mynard N, Saxena A, Mavracick A, et al. Lung Cancer Stage Shift as a Result of COVID-19 Lockdowns in New York City, a Brief Report. Clin Lung Cancer. 2022;23(3):e238-e242. doi:10.1016/j.cllc.2021.08.010
9. Cantini L, Mentrasti G, Russo GL, et al. Evaluation of COVID-19 impact on DELAYing diagnostic-therapeutic pathways of lung cancer patients in Italy (COVID-DELAY study): fewer cases and higher stages from a real-world scenario. ESMO Open. 2022;7(2):100406. doi:10.1016/j.esmoop.2022.100406
10. Minamimoto R, Hotta M, Okafuji T, et al. Change in cancer diagnosis during the COVID-19 pandemic: Trends estimated from FDG-PET/CT. Glob Health Med. 2022;4(2):108-115. doi:10.35772/ghm.2022.01016
11. Terashima T, Tsutsumi A, Iwami E, Kuroda A, Nakajima T, Eguchi K. Delayed visit and treatment of lung cancer during the coronavirus disease 2019 pandemic in Japan: a retrospective study. J Int Med Res. 2022;50(5):3000605221097375. doi:10.1177/03000605221097375
12. Park JY, Lee YJ, Kim T, et al. Collateral effects of the coronavirus disease 2019 pandemic on lung cancer diagnosis in Korea. BMC Cancer. 2020;20 (1):1040. Published 2020 Oct 29. doi:10.1186/s12885-020-07544-3
13. Mangone L, Marinelli F, Bisceglia I, et al. The Influence of COVID-19 on New Lung Cancer Diagnoses, by Stage and Treatment, in Northern Italy. Biology (Basel). 2023;12(3):390. Published 2023 Feb 28. doi:10.3390/biology12030390
14. Mojsak D, Dębczyński M, Kuklińska B, et al. Impact of COVID-19 in Patients with Lung Cancer: A Descriptive Analysis. Int J Environ Res Public Health. 2023;20(2):1583. Published 2023 Jan 15. doi:10.3390/ijerph20021583
15. Priou S, Lamé G, Zalcman G, et al. Influence of the SARS-CoV-2 outbreak on management and prognosis of new lung cancer cases, a retrospective multicenter real-life cohort study. Eur J Cancer. 2022;173:33-40. doi:10.1016/j.ejca.2022.06.018
16. Keogh JAJ, Chhor AD, Begum H, Akhtar-Danesh N, Finley C. Impact of the COVID-19 pandemic on non-small-cell lung cancer pathologic stage and presentation. Can J Surg. 2022;65(4):
E496-E503. Published 2022 Aug 4. doi:10.1503/cjs.016721
17. Zhang Y, Li J, Li ZK, et al. Impact of Coronavirus Disease 2019 on Clinical Characteristics in Patients With Lung Cancer: A Large Single-Centre Retrospective Study. Front Oncol. 2021;11:693002. Published 2021 Aug 16.
doi:10.3389/fonc.2021.693002
18. Kasymjanova G, Rizzolo A, Pepe C, et al. The Impact of COVID-19 on the Diagnosis and Treatment of Lung Cancer over a 2-Year Period at a Canadian Academic Center. Curr Oncol. 2022; 29(11):8677-8685. Published 2022 Nov 14. doi:10.3390/curroncol29110684