





Impact of Golden Hour Practices on Preterm Outcomes
The Effect of Postnatal Golden Hour Practices on Preterm Morbidity and Mortality
Assoc.Prof.Elif Özalkaya¹, MD.Gökhan Çolak¹, Prof.Dr.Sevilay Topçuoğlu¹, Assoc.Prof. Selim Sancak¹, Assoc.Prof. Emre Dinçer¹, MD.Özge Yatır Alkan¹, Prof.Dr.Güner Karatekin¹
- Zeynep Kamil Maternity and Children’s Hospital, University of Health Sciences, Istanbul 34668, Turkey
OPEN ACCESS
PUBLISHED: 31 October 2024
CITATION: Özalkaya, E., Çolak, G., et al., 2024. The Effect of Postnatal Golden Hour Practices on Preterm Morbidity and Mortality. Medical Research Archives, [online] 12(10).
http://doi.org/10.18103/mra.v12i10.5817
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
DOI http://doi.org/10.18103/mra.v12i10.5817
ISSN 2375-1924
Abstract
Aim: Although the survival rates of extremely premature babies have increased significantly in recent years, these babies have a high risk of morbidity. The period covering the process of the newborn leaving the mother’s womb and moving to the neonatal unit with resuscitation is called golden minutes. Coordinated and multidisciplinary approach to extremely low birth weight babies who are open to sudden changes of blood pressure, blood sugar, body temperature and respiratory parameters will prevent many short and long-term complications. The aim of this study is to evaluate postnatal golden hour practices in our own center and to contribute to the literature by evaluating its effect on premature morbidity.
Methods: 105 very low birth weight (<1500 gram) neonates born in University of Health Sciences Zeynep Kamil Women and Children’s Disease Training and Research Hospital Neonatal Intensive Care Unit between April 2021 and April 2022 were included in our study. The frequency of the antenatal meeting, late cord clamping, hypothermia protection, respiratory support, cardiovascular support, nutritional support, infection prevention practices, and the frequency of morbidity and mortality of the patients were recorded. The effect of golden hour practices on morbidity and mortality was evaluated.
Result: Gestational age of 105 patients included in the study was between 20+2 and 35+3 week; birth weights were between 350-1490 grams. We determined that antenatal meeting, protection from hypothermia, respiratory and cardiovascular support, nutritional support and infection prevention were applied among the golden hour practices. Delayed cord clamping could not be applied. Necrotizing enterocolitis incidence is increased with red cell transfusion and no inotropic support initiation in the first 48 hours in multivariate logistic regression analysis while intraventricular hemorrhage is increased with red cell transfusion, bronchopulmonary dysplasia and patent ductus arteriosus with low birth week and lastly mortality rate with intubation in delivery room, administration of an inotropic agent within the first 48 hours and slow infusion rate.
Conclusion: As a result of this study, we need to improve the delayed cord clamping or milking protocol, we should choose noninvasive ventilation methods instead of empirical intubation and invasive ventilation, and if delayed cord clamping or milking is not performed, the initial fluid amount should be started over 3.3 cc/kg/hour, taking into account the hypovolemia and hypotension possibilities of the patient and we concluded that we should plan the treatment of hemodynamic insufficiency by evaluating the mean arterial pressure in the first hour.
Keywords
- Postnatal Golden Hour
- Preterm Infants
- Morbidity
- Mortality
- Neonatal Care
Introduction
According to data from the World Health Organization, approximately 15 million preterm babies (born before 37 weeks of gestation) are born worldwide each year. Complications associated with preterm births are a major cause of morbidity and mortality. Around one million preterm infants die each year due to these complications. The mortality rate for extremely low birth weight (<1000 grams) and severely preterm infants (<27 weeks of gestation) can rise up to 50%. Although the survival rates of severely preterm infants have significantly increased in recent years, these infants remain at high risk for morbidities such as chronic lung disease, retinopathy of prematurity, and intraventricular hemorrhage. The golden hour of neonatal life is defined as the first hour after birth, both for preterm and term infants.
Implementing all aspects of postnatal golden hour practices for preterm infants significantly reduces preterm morbidity and mortality. Studies have shown that routine postnatal golden hour practices reduce hypothermia, intraventricular hemorrhage (IVH), bronchopulmonary dysplasia (BPD), and mortality during hospitalization.
The postnatal golden hour includes the resuscitation performed in the delivery room, transport, and admission to the neonatal intensive care unit (NICU). The interventions carried out during this first hour include antenatal consultation, prevention of hypothermia, respiratory, cardiovascular, and nutritional support, as well as infection prevention. During antenatal consultation, the questions addressed include the baby’s birth weight, gestational age, risk factors, and the frequency of antenatal steroid administration. The number of personnel in the resuscitation team, their qualifications, and their roles are determined.
To prevent hypothermia, the delivery room temperature should be set to 26°C, the radiant warmer should be turned on during resuscitation, and preterm babies should be placed in plastic bags and hats, transported in a preheated double-walled incubator with heated oxygen. Respiratory support includes the use of pulse oximetry, a blender, and positive pressure ventilation with a T-piece, noninvasive positive end expiratory pressure (PEEP) / PEEP + peak inspiratory pressure (PIP), intubation, invasive PEEP + PIP, surfactant administration, and confirming endotracheal tube placement with a chest X-ray. Cardiovascular support includes chest compressions and adrenaline during resuscitation, followed by hemodynamic echocardiography, cord or 1st-hour blood gas analysis (pH, HCO3, lactate), and inotropic support. Nutritional support includes IV glucose (mg/kg/min) and protein (g/kg/day) via a peripheral or umbilical catheter, with the initiation of minimal enteral feeding if possible, and blood glucose monitoring. Broad-spectrum antibiotics are administered within the first hour to prevent infection.
Objective
Our objective is to determine whether we implement the postnatal golden hour protocol in our delivery room routine and to evaluate the effects of the practices performed during the postnatal golden hour on the morbidity and mortality of premature infants.
Material and Methods
This study is a prospective, observational study. Ethical approval was obtained from the Clinical Research Ethics Committee of SBÜ Zeynep Kâmil Women and Children’s Health Training and Research Hospital on March 17, 2021 (decision number 63). Due to clinical responsibilities, the preparation process for publication progressed slowly. Between April 2021 and April 2022, a total of 105 preterm infants weighing less than 1500 grams, with no congenital anomalies and not planned for transfer to another neonatal intensive care unit, were included in the study at Zeynep Kamil Women and Children’s Health Training and Research Hospital. In our hospital’s delivery room routine, two members of the obstetrics team, including one trained in neonatal resuscitation program (NRP), attend preterm births after learning about maternal and neonatal risks. The infant is placed under a ventilated radiant (Resuscitaire® Draeger) beside the mother in the operating room or delivery room for resuscitation. All materials recommended by NRP guidelines are prepared at each infant’s bedside. Controlled peak inspiratory pressure (PIP) and positive end-expiratory pressure (PEEP) are given to the baby, who is dressed in a plastic bag and hood, via nasal (noninvasive) or endotracheal routes (invasive) with a Resuscitaire® Draeger. Oxygen is administered according to NRP guidelines, with pulse oximetry monitoring. After resuscitation, the infant is transferred to a Resuscitaire® Draeger in the post-resuscitation care room, where they are monitored using pulse oximetry. Peripheral intravenous (IV) access is established, and IV glucose is initiated. A chest X-ray is performed, and blood gas, blood glucose, blood culture, and blood type are obtained. Surfactant is administered within the first hour to infants meeting respiratory distress syndrome (RDS) criteria. The infant is then transferred to the NICU within the first hour using a transport incubator with ventilator. Once in the NICU, the infant is placed in a double-walled, humidified, and pre-warmed incubator, and an umbilical venous catheter is inserted. Total parenteral nutrition, ampicillin, gentamicin, fluconazole, and caffeine is initiated via the umbilical vein. To determine whether these practices align with postnatal golden hour applications and to assess the frequency of postnatal golden hour implementations in our delivery room routine, a pediatric resident observed the first hour of preterm births under 1500 grams over the course of a year. The pediatric resident observed the practices performed on preterm infants in the delivery room, during transport, and upon admission to the neonatal unit, recording morbidity and mortality data from the files in the neonatal unit. The frequency of postnatal practices and their relationship with preterm morbidity and mortality were evaluated.
Monitoring in the Delivery Room, Post-Resuscitation Care Room and During Transport
In antenatal consultation, questions were addressed regarding birth weight, gestational age, risk factors, the number of resuscitation team members, their NRP training, the frequency of antenatal steroid administration, and task allocation. Delayed or early cord clamping was assessed. To prevent hypothermia, the room temperature was set to a minimum of 26°C, and the use of a radiant warmer, plastic bags, hats, heated oxygen, and preheated double-walled incubators during transport was evaluated. For respiratory support, pulse oximetry, a blender, balloon mask or T-piece for positive pressure ventilation, noninvasive positive end expiratory pressure (PEEP) / PEEP + peak inspiratory pressure (PIP), intubation, invasive PEEP + PIP and surfactant administration were recorded. Cardiovascular support included chest compressions, adrenaline administration, and blood gas analysis. For nutritional support, the presence of peripheral/umbilical venous catheters, initial 24-hour fluid intake (cc/kg/hour), IV glucose/protein support, and blood glucose levels were recorded. To prevent infection, blood cultures and antibiotic administration were documented.
Monitoring in NICU
Hypothermia, hypoglycemia, inotropic support within the first 48 hours, erythrocyte transfusion, BPD, retinopathy of prematurity (ROP), IVH, patent ductus arteriosus (PDA), necrotizing enterocolitis (NEC), clinical early-onset sepsis, and mortality were recorded during clinical follow-up.
Definitions
Hypothermia: Defined as an axillary temperature <36.5°C upon admission to the NICU.
Hypoglycemia: Defined as a blood glucose level <50 mg/dl upon NICU admission.
BPD: Diagnosed if oxygen dependence persists at 36 weeks of postmenstrual age.
ROP: Defined according to the International Classification of Retinopathy of Prematurity Stages 1-4 were included in the study.
IVH: Defined according to the criteria by Volpe Stages 1-4 were included.
PDA: Diagnosed by pediatric cardiology based on echocardiographic findings indicating hemodynamically significant PDA.
NEC: Diagnosed clinically by characteristic features such as abdominal distension, bilious vomiting or aspirates, and rectal bleeding, and radiologically by the presence of pneumatosis intestinalis, pneumoperitoneum, or sentinel bowel loops. Stages 1-3 were included.
Early-Onset Sepsis: Defined as sepsis detected within the first 72 hours of life.
Mortality: Defined as death before discharge.
RBC Transfusion: The frequency of erythrocyte transfusion up to the onset of morbidity was recorded.
Lactate: The value from the first blood gas analysis (within the first hour) was recorded.
Delayed cord clamping [DCC]: Defined as clamping between 30 seconds and 3 minutes post-birth or when the cord pulse ceases.
Early cord clamping [ECC]: Defined as clamping the umbilical cord within 15-30 seconds post-birth.
Statistical Analysis
Statistical analyses were performed using the NCSS 2007 Statistical Software (Utah, USA). Descriptive statistical methods (mean, standard deviation, median, interquartile range) were used to evaluate the data, and the Shapiro-Wilk test was applied to assess the normality of the distribution. The independent t-test was used for normally distributed variables, while the Mann-Whitney U test was used for non-normally distributed variables. Chi-square and Fisher’s exact tests were used for categorical data comparisons. A p-value of <0.05 was considered significant. Variables with a p-value of <0.05 in univariate analyses were included in multivariate logistic regression models to assess their association with IVH, NEC, PDA, BPD, ROP and mortality. Variables without a clinical cause-and-effect relationship or with an observed frequency of zero were excluded from the model even if the p-value was <0.05 to avoid disrupting model fit.
Results
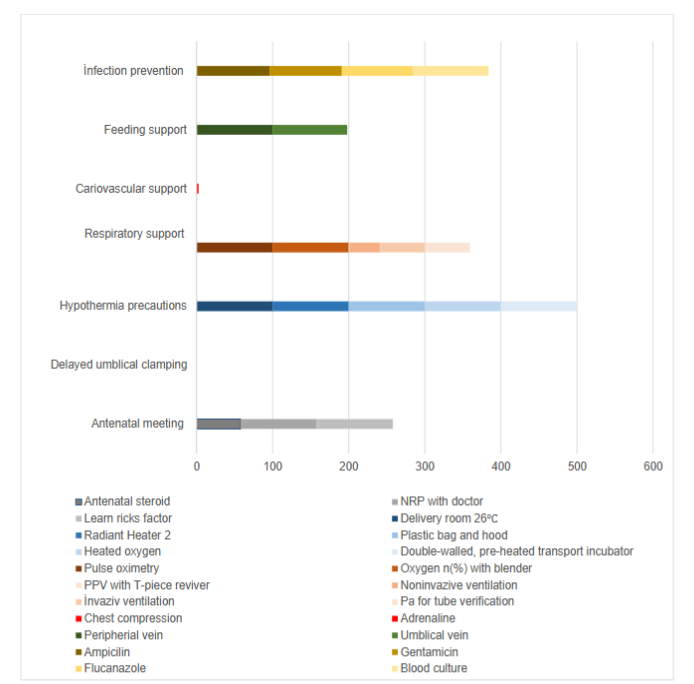
Frequency of Postnatal Golden Hour Practices
In the antenatal meeting, the average gestational age was 26.89±3.74 weeks, and the average birth weight was 926.07±355.5 grams. Antenatal steroids were administered in 57 cases (58.76%). It was decided that at least two people trained in NRP (one of whom was a doctor) would be part of the resuscitation team for all patients, duties were assigned, and maternal and neonatal risk factors were determined. DCC was not applied to any of the patients. Among the patients who had ECC, the need for RBC transfusion was observed in 68 (64.76%), and the need for inotropic support within the first 48 hours was seen in 40 (38.10%). Hypothermia prevention measures (delivery room temperature at least 26°C, radiant warmer during resuscitation, plastic bag, hat, heated oxygen, and pre-warmed, double-walled incubator during transport) were applied to all patients. For respiratory support, all patients were given oxygen through a blender and monitored with a pulse oximeter during resuscitation. Noninvasive PIP+PEEP with a T-piece was applied to 1 patient (0.95%). Noninvasive PEEP was applied to one patient (0.95%) using a Draeger Resuscitaire®, noninvasive PIP +PEEP was applied to 41 patients (39.05%), and invasive PIP +PEEP was applied to 62 patients (59.05%). Surfactant was administered to 50 patients (56.19%). Regarding surfactant administration, the less invasive surfactant administration (LISA) method was used in 1 patient (1.69%), and the classical method was applied in 58 patients (98.31%). The need for multiple doses of surfactant within the first 48 hours was noted in 48 patients (45.71%). In all 62 patients who were intubated, the position of the endotracheal tube was confirmed with a chest X-ray. Cardiovascular support measures included chest compressions in 2 patients (1.90%) and adrenaline in 1 patient (0.95%). Inotropic agents and prostaglandins were not used, and no echocardiography was performed. The average pH in blood gas analysis was 7.31±0.13, HCO3 was 20.08±3.92, and lactate was 4.00±3.24. For nutritional support, peripheral intravenous access was established in all patients. Umbilical venous catheters were inserted in 103 (98.10%) patients, and umbilical arterial catheters in 4 (3.81%). In all 103 patients who had umbilical catheters, X-rays were taken to confirm the catheter’s position. The average intravenous fluid rate was 3.32±1.01 cc/kg/hour, and the average glucose infusion rate was 6.00±0.80 mg/kg/min. Protein was not started within the first hour. The average initial blood glucose level was 86.67±27.84. To prevent infection, ampicillin was started in 101 (96.19%) patients, gentamicin in 100 (95.24%), and fluconazole in 99 (94.29%). Blood cultures were obtained from 104 patients (99.05%).
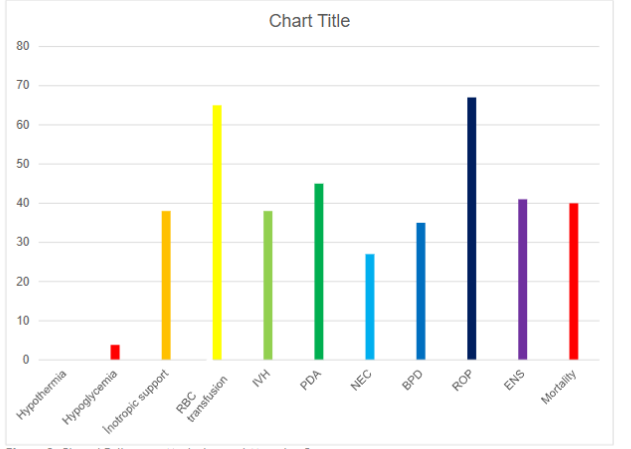
Clinical Follow-up: Morbidity and Mortality Rates
No hypothermia was detected in patients upon admission to the neonatal intensive care unit. The frequency of hypoglycemia was 4 (3.81%). ROP was detected in 44 patients (67.69%), BPD in 23 (35.38%), IVH in 35 (38.04%), PDA in 41 (45.05%), NEC in 23 (27.06%), and clinical early sepsis in 36 (41.38%). The average duration of invasive ventilation was 10.68±21.30 days, and the average hospital stay was 41.17±40.25 days. Mortality occurred in 42 patients (40%).
Impact of Postnatal Golden Hour Practices on Morbidity and Mortality
The relationships between respiratory support (T-piece, noninvasive PEEP/ PIP+PEEP, invasive PIP+ PEEP, surfactant), cardiovascular support (lactate), nutritional support (parenteral fluid amount), the need for erythrocyte and inotropic support (due to early cord clamping), and clinical outcomes such as IVH, BPD, ROP, PDA, NEC, and mortality were evaluated.
| IVH (-) | n=57(%) | IVH (+) | n=35(%) | p | NEC (-) | n=62(%) | NEC (+) | n=23(%) | p | PDA (-) | n=50(%) | PDA (+) | n=41(%) | p | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Prenatal meeting | Birth weight ≥1000 gr | 33 (57.9) | 24 (42.1) | 15 (42.9) | 20 (57.1) | 0.235 | 31 (50) | 31 (50) | 16 (69.6) | 7 (30.4) | 0.172 | 38 (76) | 12 (24) | 10 (24.4) | 31 (75.6) | <0.001 |
| Birth week ≥ 28 weeks | 35 (61.4) | 22 (38.6) | 12 (34.3) | 23 (65.7) | 0.021 | 31 (50) | 31 (50) | 15 (65.2) | 8 (34) | 0.314 | 42 (84) | 8 (16) | 5 (12.2) | 36 (87.8) | <0.001 | |
| Early cord clamp | RBC transfusion | 32 (56.14) | 32 (91.43) | 0.0001 | 40 (64.52) | 2 (91.30) | 0.015 | 28 (56) | 36 (87.80) | 0.001 | ||||||
| Inotrop support | 14 (24.56) | 16 (45.71) | 0.036 | 21 (33.87) | 2 (8.70) | 0.020 | 9 (18.00) | 20 (48.78) | 0.002 | |||||||
| Respiratory Support | T-Piece | 1 (1.75) | 1 (1.75) | 31 (54.3) | 24 (42.11) | 23 (40.35) | – | – | 10 (28.57) | 25 (71.43) | 23 (65.71) | – | – | 0.019 | 0.009 | 0.018 |
| 1 (1.6) | 1 (1.6) | 30 (48.3) | 30 (48.39) | 28 (45.16) | – | – | 0.808 | 0.627 | 0.5 | |||||||
| 1 (2.0) | 1 (2.0) | 35 (70) | 13 (26) | 11 (22.00) | – | – | 6 (14.6) | 35 (85.37) | 34 (82.93) | – | – | 0.0001 | 0.0001 | 0.0001 |
Discussion
In our delivery room routine, we observed that we implemented antenatal meetings, hypothermia prevention, and infection protection, as well as respiratory, cardiovascular, and nutritional support, which are part of the postnatal golden hour practices. In our study, no hypothermia was detected upon admission to the neonatal intensive care unit after transport in a 26°C delivery room, under a radiant warmer, with the infant placed in a plastic bag with a cap and transported in a pre-warmed, double-walled incubator. In Sheng et al.’s meta-analysis of 10 studies evaluating the effects of postnatal golden hour practices on preterm morbidity, hypothermia was found to decrease in five of the studies following these practices.
Despite the administration of ampicillin, gentamicin, and fluconazole within the first postnatal hour for infection protection, a high rate of early neonatal sepsis (41%) was detected. The predominance of extended-spectrum beta-lactamase (ESBL) positive gram-negative bacteria as the causative agents of early neonatal sepsis in our unit explained the high frequency of early neonatal sepsis despite antibiotic treatment. Considering the frequent occurrence of ESBL-positive gram-negative bacteria in our unit, we planned to review our antibiotic policy. Nutritional support was provided to all infants through glucose infusion via a peripheral venous route within the first postnatal hour. We believe the reason for the low incidence of hypoglycemia upon admission to the NICU was our initiation of glucose infusion via the peripheral intravenous route before umbilical access.
For respiratory support, we avoided using a self-inflating bag and instead applied controlled PIP and PEEP pressures using a ventilator. However, we frequently applied controlled PIP and PEEP through invasive ventilation, and surfactant was administered via the classical route. We found that invasive ventilation in the delivery room increased mortality by 11-fold. In Cochrane’s 2016 analysis, even non-invasive PEEP alone, whether surfactant was administered or not, led to clinically significant reductions in the incidence of BPD and BPD/mortality when compared to invasive ventilation support. It was shown that non-invasive ventilation during the postnatal golden hour reduced BPD. Therefore, we planned to improve our frequency of non-invasive ventilation and LISA surfactant administration in the delivery room.
In our delivery room routine, the only postnatal golden hour practice we did not perform was delayed cord clamping. Only one of the studies involving postnatal golden hour practices included DCC. If cord clamping occurs before the onset of breathing, the loss of umbilical venous return is not compensated for by the increase in pulmonary venous return, leading to a decrease in ventricular filling, cardiac output, and systemic blood pressure. DCC has been shown to reduce hypotension in preterm infants. The blood pressure of our patients who underwent ECC was not assessed. However, high average blood lactate levels indicated poor perfusion within the first hour. In patients born with poor perfusion due to early cord clamping, starting fluids at a rate of less than 3.3 cc/kg increased mortality by 89-fold, and 38% required inotropic support within 48 hours, with mortality increasing by 8-fold in these infants. As a result, we concluded that cardiovascular support provided during the postnatal golden hour in infants born with poor perfusion due to ECC needs to be improved to prevent increased mortality. For infants who did not undergo DCC, we aimed to evaluate perfusion using hemodynamic echocardiography in cases of high lactate levels and initiate higher fluid and inotropic support within the golden hour. Another advantage of DCC is that by increasing placental blood volume, it increases neonatal blood volume, improves neonatal and infant iron stores, and reduces neonatal and infant anemia. DCC has been shown to reduce the need for red blood cell transfusions in preterm infants. In our study, 64% of patients who underwent ECC required multiple blood transfusions. Multiple transfusions were associated with a 9-fold increased risk of IVH and a 10-fold increased risk of NEC. Several studies have also shown an increased incidence of transfusion-associated NEC and IVH. A meta-analysis of 48 studies demonstrated that DCC could reduce the risk of death before discharge compared to early cord clamping. Consequently, to reduce the frequency of transfusions and transfusion-associated preterm morbidities, we planned to include delayed cord clamping in our delivery room routine.
Conclusion
In our delivery room routines, we appropriately implemented antenatal meetings, hypothermia prevention, nutritional support, and controlled PIP and PEEP in respiratory support as part of the postnatal golden hour practices. However, we applied respiratory support invasively. We started antibiotics on time to prevent early sepsis, but our rate of early neonatal sepsis was high. DCC was not applied to any of the patients. During the postnatal golden hour, invasive ventilation, the use of resistant antibiotics in the first hour in our unit with a high frequency of ESBL-positive gram-negative sepsis, and the absence of DCC increased the incidence of early neonatal sepsis, IVH, NEC, and mortality. We planned to implement a postnatal golden hour protocol in our delivery room routine that includes non-invasive ventilation and DCC. Future studies focusing on DCC, which has been neglected in postnatal golden hour practices, will be appropriate.
References
- Lambeth TM, Rojas MA, Holmes AP, Dail RB. First Golden Hour of Life: A Quality Improvement Initiative. Adv Neonatal Care. 2016;16(4):264-272.
- Wyckoff MH. Initial resuscitation and stabilization of the periviable neonate: The Golden-Hour approach. Semin Perinatol. 2014;38(1):12-16.
- Vento M, Cheung PY, Aguar M. The first golden minutes of the extremely-low-gestational-age neonate: a gentle approach. Neonatology. 2009;95(4):286-298.
- American Academy of Pediatrics. Neonatal Resuscitation, 8th ed, Weiner G, Zaichkin J (Eds), American Academy of Pediatrics, Itasca, IL 2021.
- Jobe AH, Bancalari E. Bronchopulmonary dysplasia. Am J Respir Care Med 2001;163:1723-1729.
- Chiang MF, Quinn GE, Fielder AR, Ostmo SR, Paul Chan RV, Berrocal A, et.al. International Classification of Retinopathy of Prematurity, Third Edition. Ophthalmology. 2021:S0161-6420(21)00416-4.
- Çizmeci MN, Akın MA, Özek E. Germinal Matriks Kanaması İntraventriküler Kanama ve Komplikasyonlarının Tanı ve Yönetimi Rehberi. Türk Pediatri Arşivi. 2021; 53(Supp: 1): 5-2.
- Evans N. Preterm patent ductus arteriosus: A continuing conundrum for the neonatologist. Semin Fetal Neonatal Med. 2015;20:272-7.
- Walsh MC. & Kliegman RM. Necrotizing enterocolitis: treatment based on staging criteria. Pediatric clinics of North America. 1986; 33(1): 179- 201.
- Sheng L, Zhong G, Xing R, Yan X, Cui H, Yu Z. Quality improvement in the golden hour for premature infants: a scoping review. BMC Pediatrics. 2024;24: 88.
- Demirhan S, Topcuoglu S, Karadag N, Ozalkaya E, Karatekin G, Vasoactive inotropic score as a predictor of mortality in neonatal septic shock. Journal of Tropical Pediatrics. 2022; 68(6): 1–9.
- Subramaniam P, Ho JJ, Davis PG. Prophylactic nasal continuous positive airway pressure for preventing morbidity and mortality in very preterm infants. Cochrane Database of Systematic Reviews. 2016; CD001243.
- Peleg B, Globus O, Granot M, Leibovitch L, Mazkereth R, Eisen I et al. Golden hour quality improvement intervention and short-term outcome among preterm infants. J Perinatol. 2019;39(3):387–92.
- Vergales BD, Dwyer EJ, Wilson SM, Nicholson EA, Nauman RC, Jin L et al. NASCAR pit-stop model improves delivery room and admission efficiency and outcomes for infants<27 weeks’ gestation. Resuscitation. 2015; 92:7–13.
- Croop S, Thoyre SM, Aliaga S, McCaffrey MJ, Peter-Wohl S. The golden hour: a quality improvement initiative for extremely premature infants in the neonatal intensive care unit. J Perinatol. 2020;40(3):530-9.
- Hemodynamic Effects of Delayed Cord Clamping in Premature Infants. Sommers R, Stonestreet BS, Oh W, Laptook A, Yanowitz TD, Raker C, Mercer. J. Pediatrics. 2012; 129: 667–672.
- Mascola MA, Porter TF, Chao TT. ACOG committee opinion. Delayed Umbilical Cord Clamping After Birth. ACOG.2020;136:100-105.
- Teiserskas J, Bartasiene R, Tameliene R. Associations between Red Blood Cell Transfusions and Necrotizing Enterocolitis in Very Low Birth Weight Infants: Ten-Year Data of a Tertiary Neonatal Unit. Medicina. 2019; 55(1): 16.
- Crawford TM, Andersen CC, Hodyl NA, Robertson SA, Stark MJ. The contribution of red blood cell transfusion to neonatal morbidity and mortality. J Pediatr Child Health. 2019; 55(4):387-392.
- Rabe H, Gyte GM, Díaz-Rossello JL, Duley L. Effect of timing of umbilical cord clamping and other strategies to influence placental transfusion at preterm birth on maternal and infant outcomes. Cochrane Database Syst Rev. 2019;9(9):3248.