





Impact of Iron and Folic Acid Supplementation in Pregnancy
Assessing the need for and impact of use of iron folic acid supplementation in pregnant women: Role of haemoglobin and ferritin
Prema Ramachandran1, K. Kalaivani2
- Prema Ramachandran Director, Nutrition Foundation of India
 http://orcid.org/0000-0003-1974-8281
http://orcid.org/0000-0003-1974-8281 - K. Kalaivani Deputy Director, Nutrition Foundation of India http://orcid.org/0000-0002-9582-4488
OPEN ACCESS
PUBLISHED: 31 July 2025
CITATION: Ramachandran, P., Kalaivani, K., 2025. Assessing the need for and impact of use of iron folic acid supplementation in pregnant women: Role of haemoglobin and ferritin. Medical Research Archives, [online] 13(7). https://doi.org/10.18103/mra.v13i7.6747
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i7.6747
ISSN 2375-1924
Abstract
In India, there are substantial inter-state and urban-rural variations in the prevalence of anaemia and iron, folic acid and vitamin B 12 deficiency in pregnant women as well as the type and dose of micro-nutrient supplements provided in antenatal clinics. Our institution had conducted two hospital-based randomized studies on treatment of anaemia in pregnant women with Haemoglobin (Hb) between 8.0 to 10.9 g/dL with different doses of iron, folic acid and vitamin (vit) B12. Blood samples were collected at enrolment and after 8 weeks of supplementation and Hb, ferritin, C reactive protein (CRP), folic acid and Vitamin B 12 levels were estimated. Data were re-analysed to assess:
- prevalence of iron, folic acid and vit B12 deficiency in anaemic pregnant women at enrolment, and
- usefulness of Hb, ferritin, folic acid and vit B12 estimations in assessing the improvement in the Hb and micro-nutrient status after supplementation.
Analysis of data in anaemic pregnant women at the time of enrolment showed that:
- iron deficiency was the most common micro-nutrient deficiency,
- prevalence of folic acid deficiency was low (< 5%), and
- vit B12 deficiency was seen in 40% women.
Paired data analysis of Hb at enrolment and after 8 weeks supplementation showed that:
- there was no difference in Hb response to 60 or 240 mg supplementation for 8 weeks,
- higher dose of folic acid or addition of vitamin B12 did have any impact on Hb, and
- it was possible to identify individual non-responders to supplementation who required referral to higher medical facilities for investigation and treatment.
Mean ferritin improved with supplementation; improvement following 60 mg and 240 mg iron supplementation was similar. Ferritin estimation was not useful in assessing the response to iron supplementation in individuals. Concurrent CRP estimation along with ferritin was not useful in the detection of iron deficiency in women with inflammation because very few women had ferritin levels beyond 70 ng/ml. Improvement in mean folic acid levels were similar after 5 mg or 1.5 mg of folic acid supplementation; supplementation did not have any impact on reduction in folic acid deficiency because of low folic acid deficiency at enrolment. There was a fall in mean vit B12 levels and an increase in vit B12 deficiency with 5 mg folic acid supplementation. Hence, supplementation with 5 mg of folic acid should not be done. Addition of oral Vit B12 to iron and folic acid supplementation did not improve either Hb or vit B12 level.
Keywords
iron, folic acid, vitamin B12, supplementation, pregnant women, anaemia
Introduction
India had and continues to have the highest prevalence of anaemia in pregnancy in the world and is the home of the largest number of anaemic pregnant women. Research studies in 1960s and 70s showed that anaemia preceded pregnancy and got aggravated during pregnancy; over 80% of pregnant women were anaemic. Anaemia in pregnancy was associated with higher maternal morbidity, mortality, low birth weight and high perinatal mortality. Anaemia was mainly due to iron and folic acid deficiency; vitamin B12 (vit B12) deficiency was not as common. Research studies in the 70s reported that iron and folic acid supplementation to pregnant women resulted in improvement in Hb levels; but the addition of Vit B12 did not result in further improvement in Hb.
The country initiated the National Anaemia Prophylaxis Programme aimed at providing iron and folic acid supplements to all identified pregnant women. Taking into account the poor bio-availability of iron from fibre-rich plant based Indian diets, the supplement contained 60 mg of elemental iron with 500 µg of folic acid. Initially the coverage under the programme was low, but improved over time. Continuation rates were low because of the minor but troublesome side effects of iron. An ICMR survey in 1980s showed that there was no improvement in the mean Hb even in women who took 90 tablets of iron and folic acid. National Anaemia Control Programme (NACP) recommended that all pregnant women should be screened and anaemic pregnant women should receive 100 mg of elemental iron and 500 µg of folic acid (IFA supplementation) twice a day. The NACP has been implemented as a major component of antenatal care across the country but coverage under the programme, availability, access and utilisation of supplementation varied between states and in different levels of health care in urban and rural areas.
Hospital based studies have shown that there were wide variations in the prevalence of anaemia and micro-nutrient deficiencies in anaemic women between states, urban and rural areas and income groups and that over time there were changes in the prevalence of micro-nutrient deficiencies. Iron deficiency continued to be the most common deficiency in anaemic women; but there has been some reduction in folate deficiency and an increase in Vit B12 deficiency. In addition to Hb estimation, bio-marker estimations are increasingly used in tertiary care institutions to assess prevalence of micro-nutrient deficiencies and tailor the micro-nutrient supplementation accordingly.
During the first decade of the NACP, the central government procured and distributed the IFA supplements to all the states. Under the National Iron Plus Initiative (NIPI) the states have been purchasing micro-nutrient supplementation to be given to pregnant women. There are differences between states in the type and dose of micro-nutrient supplements provided. It is important to assess whether there are differences in the response to the micro-nutrient supplements with varying dose and composition, in terms of Hb, ferritin, folic acid and Vit B12. This information will be of help in choosing the optimal dose and combination of micro-nutrient for supplementation.
The guidelines under Intensified National Iron Plus Initiative (I-NIPI) suggest that all anaemic pregnant women should be followed up and Hb estimation should be done during follow-up to identify those who are not responding to IFA supplementation; identified non-responders should be referred to secondary care centres for further investigations and management. Biomarker assays are being used as a part of investigations to find out the reason for the non-response as assessed by Hb.
In India anaemia, iron deficiency and inflammation are common. Ferritin levels are high during inflammation. In order to ensure that iron deficiency is not missed because ferritin levels were high due to inflammation, WHO recommended that concurrent C Reactive Protein (CRP) assay should be carried out with ferritin assay. WHO those with ferritin levels above 70 ng/ml should be considered as not having iron deficiency. As iron deficiency is the most common deficiency associated with anaemia, it is important to assess the usefulness of the 70 ng/ml cut-off for ferritin for defining iron deficiency in Indian pregnant women. In view of the reported progressive increase in vit B12 deficiency in the last three decades, it is important to assess the need for and impact of vit B12 supplementation in addition to iron and folic acid supplementation to pregnant women.
Material and methods
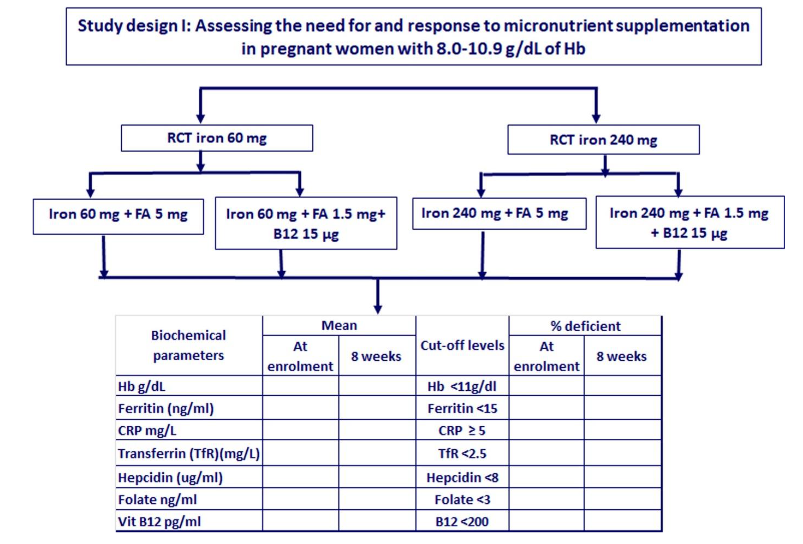
Our institution had undertaken two hospital-based randomized studies on treatment of anaemia in pregnant women. In one study pregnant women with Hb between 8.0 and 10.9 g/dL at enrolment early in second trimester of pregnancy were given iron tablet containing 60 mg of elemental iron along with either one tablet containing 5 mg of folic acid or 1 tablet of vitamin B complex containing 1.5 mg of folic acid and 15 µg Vit B12 to be taken daily. In the second hospital-based open randomised study pregnant women with Hb between 8.0 and 10.9 g/dL at enrolment early in second trimester of pregnancy were given four iron tablets each containing 60 mg of elemental iron (to be taken as two tablets twice a day after meals) along with either one tablet containing 5 mg of folic acid or 1 tablet of vitamin B complex containing 1.5 mg of folic acid and 15 µg Vit B12. Blood samples were collected at enrolment, after 8 weeks of supplementation and at 38 weeks of pregnancy. Data on biochemical parameters at enrolment and paired data at enrolment (0 weeks) and at 8 weeks were re-analysed with the primary objective of assessing:
- prevalence of iron, folic acid and vit B12 deficiency in anaemic pregnant women,
- usefulness of the concurrent CRP assay in assessment of iron deficiency in presence of inflammation in pregnant women,
- usefulness of Hb, ferritin, folic acid and Vit B12 in assessing the improvement in the Hb and micro-nutrient status brought about by different regimens of micro-nutrient supplements provided to these women. (Study designs I, II and III)
Secondary objectives were to assess:
➢ usefulness of the bio-marker assays in identifying the individuals who are not responding to the micro-nutrient provided as supplements,
➢ impact of supplementation with folic acid 5 mg (Study design III) on folic acid and Vit B12 status.
Results
Analysis of blood samples from pregnant women with Hb between 8.0-10.9 g/dL showed that the prevalence of iron deficiency as assessed by ferritin, soluble transferrin receptor (TfR) and hepcidin was high. These data suggest that iron deficiency was the most common micro-nutrient deficiency in anaemic pregnant women.
| Biochemical parameters at enrolment | Cut-off | % deficient | |
|---|---|---|---|
| Hb (g/dL) | 9.7±0.72 (637) | Hb <11 | 100 |
| Ferritin (ng/ml) | 18.5±24.21 (630) | Ferritin <15 | 64.3 |
| TfR (mg/L) | 2.5±1.44 (628) | TfR <2.5 | 62.5 |
| Hepcidin (ug/ml) | 7.1±11.92 (398) | Hepcidin <8 | 73.6 |
| Folic acid (ng/ml) | 7.9±5.74 (549) | folate <3 | 7.1 |
| Vit B12 (pg/ml) | 250.4±189.11 (552) | B12 <200 | 43.3 |
| CRP mg/L | 4.7±4.23 (624) | CRP | 37.5* |
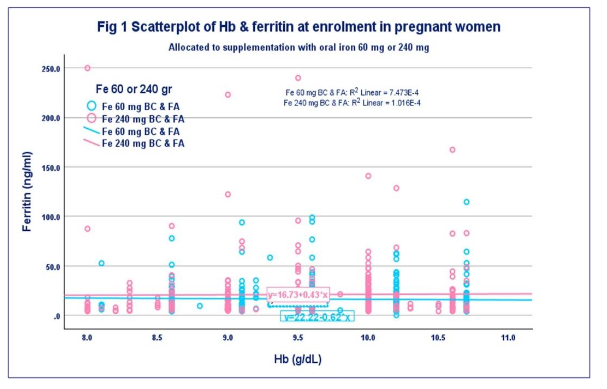
Prevalence of folate deficiency was low (<5%). Vit B12 deficiency was seen in over 40% of the pregnant women. At the time of blood collection all these women were apparently healthy and did not have any overt infections. Despite this over one-third women had CRP levels above 5 mg/L suggestive of inflammation. This has to be taken into account while assessing the prevalence of iron deficiency using ferritin as the parameter. Studies in non-pregnant women showed that iron deficiency existed even among non-anaemic women and that with decrease in Hb there was an increase in prevalence of iron deficiency. To assess whether there is a similar trend in anaemic pregnant women, mean ferritin levels were computed in relation to Hb levels. Nearly 50% of women had Hb between 10-10.9 g/dL; less than 1/6th had Hb between 8.0 to 8.9 g/dL. There were no differences in the mean ferritin levels in relation to Hb levels.
| Relationship between Hb and ferritin in anaemic pregnant women at enrolment | Hb | Mean ferritin (ng/ml) |
|---|---|---|
| 8.0-8.9 | 8.4±0.23 (90) | 18.6±29.68 (90) |
| 9.0-9.9 | 9.3±0.26 (243) | 18.9±26.79 (240) |
| 10.0-10.9 | 10.3±0.28 (304) | 18.0±19.92 (300) |
| Total | 9.7±0.72 (637) | 18.5±24.21 (630) |
Data on micro-nutrient deficiencies in anaemic pregnant women in relation to their Hb are shown in the following table. There were no differences in the prevalence of iron deficiency (as assessed by ferritin, TfR, and hepcidin), folate and Vit B12 deficiency in pregnant women with Hb 8+, 9+ or 10+ g/dL.
| Prevalence of micro-nutrient deficiencies in relation to Hb levels in anaemic pregnant women | Biochemical Parameter cut-off | Hb g/dL | |||
|---|---|---|---|---|---|
| Ferritin (ng/ml) | <15 | 68.9 | 63.9 | 63.2 | 64.3 |
| TfR (mg/L) | <2.5 | 40.2 | 61.0 | 70.2 | 62.5 |
| Hepcidin (ug/ml) | <8 | 78.8 | 71.4 | 73.7 | 73.6 |
| Folic acid (ng/ml) | <3 | 4.3 | 7.1 | 7.8 | 7.1 |
| Vit B12(pg/ml) | <200 | 40.6 | 44.9 | 42.8 | 43.3 |
| CRP (mg/L) | 29.1 | 36.3 | 38.5 | 36.3 |
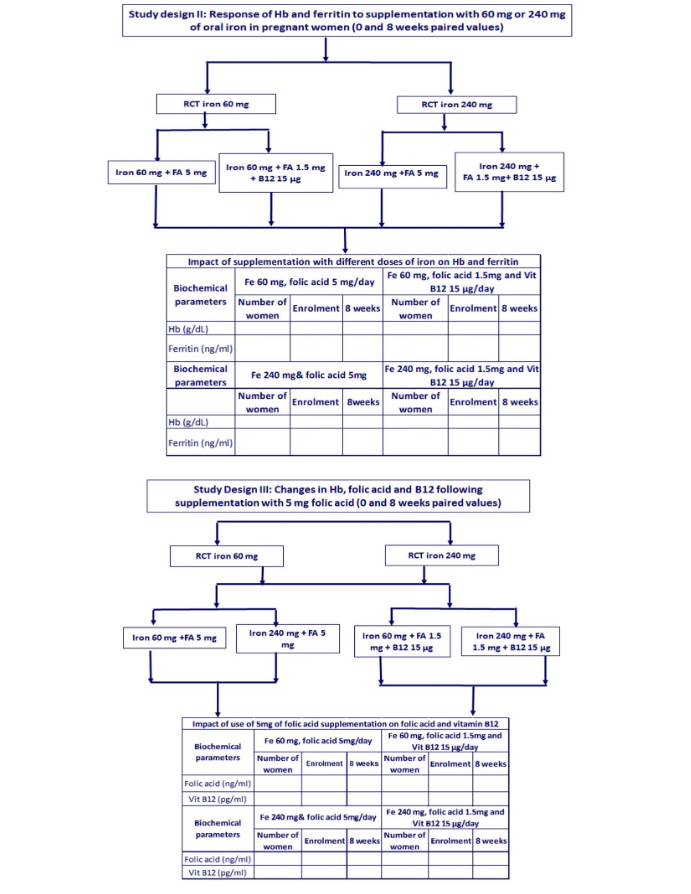
Paired data on Hb and iron status of women who had received 60 mg of iron (either with folic acid 5mg or folic acid 1.5mg and vit B12 15 ug) were compared with those who had received 240 mg iron (either with folic acid 5mg or folic acid 1.5mg and vit B12 15 ug). There were no significant differences in the improvement in mean Hb or ferritin level between these four groups.
| Impact of supplementation with different doses of iron on Hb and ferritin | Paired data | |||||
|---|---|---|---|---|---|---|
| Biochemical parameters | Fe 60 mg, folic acid 5 mg/day | Fe 60 mg, folic acid 1.5mg and Vit B12 15 µg/day | Number of women | Enrolment | 8 weeks | |
| Hb (g/dL) | 68 | 9.8±0.66 | 10.9±0.98 | 91 | 9.9±0.69 | 11.0±0.92 |
| Ferritin (ng/ml) | 66 | 14.3±13.26 | 18.9±16.32 | 85 | 18.5±16.86 | 22.3±19.30 |
| Biochemical parameters | Fe 240 mg& folic acid 5mg | Fe 240 mg, folic acid 1.5mg and Vit B12 15 µg/day | Number of women | Enrolment | 8weeks | |
| Hb (g/dL) | 95 | 9.5±0.70 | 10.6±0.84 | 102 | 9.5±0.70 | 10.6±0.87 |
| Ferritin (ng/ml) | 87 | 29.2±43.73 | 28.6±37.09 | 92 | 19.9±29.12 | 23.8±35.88 |
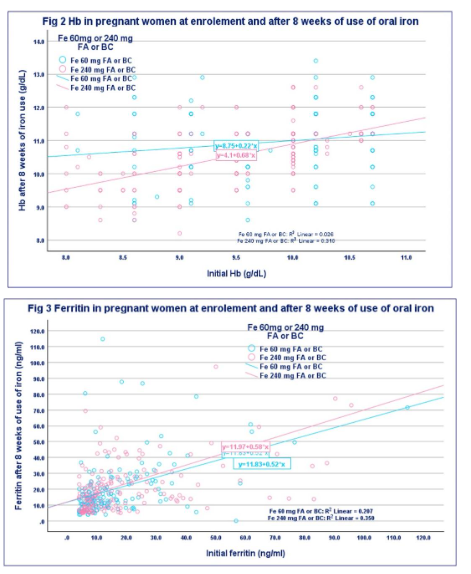
Paired data from all the four groups were analysed to assess impact of different supplements on Hb and ferritin at enrolment and after 8 weeks supplementation. Scatter plots indicate that improvement in Hb and ferritin was seen across all values at enrolment and that there were no differences either with Hb or ferritin between the supplementation at 60 mg and 240 mg of oral iron.
| Impact of iron supplementation (60 and 240mg/day) for 8 weeks on anaemia and iron deficiency | Biochemical parameter | Fe 60 mg& folic acid 5mg | Fe 60 mg, folic acid 1.5mg and Vit B12 15 µg | Enrolment | 8 weeks |
|---|---|---|---|---|---|
| Hb<11g/dl | 100.0 | 50.0 | 100.0 | 41.8 | |
| Ferritin <15ng/ml | 68.2 | 61.2 | 64.1 | 45.6 | |
| Fe 240 mg& folic acid 5mg | 100.0 | 62.2 | 100.0 | 61.8 | |
| Ferritin <15ng/ml | 58.0 | 35.6 | 66.7 | 48.9 |
The computed prevalence of anaemia and iron deficiency after 8 weeks of supplementation with either 60 or 240 mg of iron/day is given in the table. There were no differences in prevalence of anaemia or iron deficiency following 60 or 240 mg of iron supplementation for 8 weeks. Clinical data showed that prevalence of and discontinuation due to side effects were more in women who received 240 mg of iron daily. Based on these data and data from other research studies I-NIPI recommended that anaemic pregnant women should take 120mg of elemental iron and 1mg of folic acid after meal once a day till delivery. Analysis of data from our study showed that it was possible to identify non-responders (increase in Hb less than 0.5 g/dl after 8 week supplementation). Ferritin assays were not useful in identifying individuals who were not showing improvement iron deficiency.
IMPACT OF SUPPLEMENTATION WITH 5MG FOLIC ACID/DAILY FOR 8 WEEKS
Supplementation with 5 mg folic acid either with 60 or 240 mg of iron for 8 weeks resulted in higher mean folic acid as compared to women who received folic acid 1.5 mg and Vit B12 15 µg/day. However, there was a fall in the mean Vit B12 levels in those who received 5 mg of folic acid supplementation.
| Impact of use of 5mg of folic acid supplementation on folic acid and vitamin B12 | Biochemical parameters | Fe 60 mg, folic acid 5mg/day | Fe 60 mg, folic acid 1.5mg and Vit B12 15 µg/day | Number of women | Enrolment | 8 weeks |
|---|---|---|---|---|---|---|
| Folic acid (ng/ml) | 64 | 8.6±6.80 | 12.9±7.79 | 89 | 8.6±5.59 | 11.2±4.88 |
| Vit B12 (pg/ml) | 66 | 288.4±159.18 | 196.6±114.04 | 88 | 295.7±236.04 | 267.1±140.08 |
| Biochemical parameters | Fe 240 mg& folic acid 5mg/day | Fe 240 mg, folic acid 1.5mg and Vit B12 15 µg/day | Number of women | Enrolment | 8 weeks | |
| Folic acid (ng/ml) | 44 | 7.7±5.25 | 14.5±11.94 | 44 | 7.0±4.88 | 11.5±6.18 |
| Vit B12 (pg/ml) | 43 | 243.3±151.30 | 214.9±138.77 | 46 | 282.1±374.84 | 242.6±197.10 |
Computed prevalence of folic acid deficiency and vit B12 deficiency in women who received supplementation with 5 mg folic acid either with 60 or 240 mg of iron for 8 weeks is shown in the following table. Supplementation with either 5 mg or 1.5 mg of folic acid did not have any impact on folic acid deficiency because prevalence of folic acid deficiency in these women was low at enrolment.
| Impact of use of 5mg of folic acid supplementation on folic acid and vitamin B12 deficiency | Parameter | Fe 60 mg& FA 5mg | Fe 60 mg, FA 1.5mg and Vit B12 15 µg | Enrolment | 8 weeks |
|---|---|---|---|---|---|
| Folic acid <3 ng/ml | 4.7 | 4.7 | 3.4 | 5.6 | |
| Vit B12 <200pg/ml | 27.3 | 59.1 | 32.6 | 36.0 | |
| Parameter | Fe 240 mg & FA 5mg | Fe 240 mg, FA 1.5mg and Vit B12 15 µg | Enrolment | 8 weeks | |
| Folic acid <3 ng/ml | 4.5 | 0.0 | 19.0 | 2.4 | |
| Vit B12 <200pg/ml | 40.9 | 58.1 | 50.0 | 50.0 |
Prevalence of Vit B12 deficiency was high at enrolment in these women. Supplementation with 5 mg folic acid resulted in increase in the prevalence of Vit B12 deficiency. Despite the high prevalence of Vit B12 at enrolment supplementation with Vit B12 (in addition to 1.5mg of folic acid) did not have any impact either on Hb levels or Vit B12 levels, prevalence of anaemia or Vit B12 deficiency.
Discussion
Diagnosis of anaemia is by Hb estimation. The World Health Organisation (WHO) had reviewed global data and made recommendations for cut-off Hb levels to define anaemia and grading the severity of anaemia in different age, sex and physiological groups. These cut-offs are made from statistical analysis of available data with appropriate methods. These are used widely so that it is possible to compare the prevalence of anaemia inter-country, inter-state, urban-rural areas and between different income groups in the same locale. National surveys and hospital-based studies showed that there were:
- changes in the prevalence anaemia and micro-nutrient deficiencies over time,
- substantial inter-state and urban-rural differences in the prevalence anaemia and iron, folic acid and vit B12 deficiencies, and
- differences between states and institutions in the dose and content of micro-nutrient supplementation to pregnant women.
The I-NIPI programme reviewed all epidemiological, clinical, research, and programme data pertaining to anaemia in pregnancy in 2018 and modified the intervention under the National Iron Plus Initiative (NIPI programme). I-NIPI reiterated that Hb estimation should be done in all pregnant women as a part of antenatal care to detect anaemic pregnant women.
The Intensified national Iron Plus initiative (I-NIPI) recommended that:
- all pregnant women should be screened for anaemia by Hb estimation,
- non-anaemic women should take one tablet containing 60 mg of elemental iron and 500 µg of folic acid/day after a meal,
- anaemic women should take 2 tablets each containing 60 mg of elemental iron and 500 µg of folic acid/day after a meal, and
- anaemic pregnant women should undergo Hb estimation after 2 months of supplementation; women not responding to supplements as assessed by Hb estimation should be referred to secondary care centres for further investigations and management.
In the last two decades many secondary and tertiary care centres have been undertaking, bio-marker assays to assess iron, folic acid and Vit B12 status in anaemic pregnant women and to assess response to micro-nutrient supplementation, especially in those who did not respond to micro-nutrient supplementation. Nutrition surveys are undertaking these assays to assess trends in prevalence of these micro-nutrient deficiencies in pregnant women in different states and urban and rural areas in the same state.
Data from our hospital-based open randomised studies on micro-nutrient supplementation to pregnant women from urban low middle-income group were re-analysed to:
- assess prevalence of micro-nutrient deficiencies in urban anaemic pregnant women,
- usefulness of Hb, ferritin, folic acid and Vit B12 assays in assessing the improvement in the Hb and micro-nutrient status brought about by different regimens of micro-nutrient supplements provided to these women.
HAEMOGLOBIN AND MICRO-NUTRIENT PROFILE OF PREGNANT WOMEN AT ENROLMENT
Over the last two decades there has been a reduction both in the prevalence and severity of anaemia. In the present study nearly 50% of women had Hb between 10-10.9 g/dL; less than 1/6th had Hb between 8.0 to 8.9 g/dL. At enrolment, prevalence of iron deficiency as assessed by ferritin, TfR and hepcidin was high in anaemic pregnant women with Hb between 8.0 and 10.9g/dL. Nearly 2/3rd of the women had low ferritin (<15 ng/ml), and low TfR (<2.5 mg/L) and three fourth had low hepcidin (<8 ug/ml). The prevalence of folate deficiency at enrolment was low (<5%) but Vit B12 deficiency was seen in 40% of women. Data on micro-nutrient deficiencies in anaemic pregnant women in relation to their Hb are shown in the following table. There were no differences in the prevalence of iron deficiency (as assessed by ferritin, TfR, and hepcidin), folate and Vit B12 deficiency in pregnant women with Hb 8+, 9+ or 10+ g/dL.
USEFULNESS OF CONCURRENT C REACTIVE PROTEIN AND FERRITIN ESTIMATION FOR DETECTION IRON DEFICIENCY
Anaemia, iron deficiency and infections are common in pregnant women in India. Ferritin levels are high in persons with inflammation. In order to minimise the mis-classification of iron deficient women who had high ferritin levels because of inflammation, WHO has recommended that CRP estimation should be done concurrently with ferritin estimation; if the persons had CRP level 5mg/L only those with ferritin levels 70ng/ml should be classified as not having iron deficiency. All the pregnant women enrolled for the study were apparently healthy and did not have any overt infection at the time of blood collection either at enrolment or at the time of 8 week follow up. Despite this over one third of the pregnant women at enrolment and 1/4th of the pregnant women at follow-up had CRP level 5mg/L. There were no significant differences in the mean ferritin levels and prevalence of ferritin levels below 15 ng/ml (WHO cut-off for iron deficiency in women without inflammation) between women who had CRP <5 mg/L and those who had CRP mg/L. Less than 5% of women who had CRP mg/L had ferritin levels ng/ml. Analysis of data on CRP and ferritin levels after iron and micro-nutrient supplementation for 8 weeks showed similar findings. These data suggest that concurrent CRP estimation with ferritin may not be of use in assessing iron deficiency in presence of inflammation.
RATIONALE FOR THE RANDOMISED STUDY ON MICRO-NUTRIENT SUPPLEMENTATION
Iron deficiency was the most common deficiency in anaemic women with Hb between 8.0 to 10.9 g/dL. Our research study compared supplementation with low dose (60 mg of elemental iron/day) provided by the state govt in its antenatal clinics, with high dose (240 mg of elemental iron/day) similar to the dose recommended (200 mg of elemental iron/day) in the national programme for treatment of anaemic pregnant women. The impact of supplementation with these two dosage schedules of iron for 8 weeks on the Hb and ferritin levels were assessed using paired samples collected at enrolment and after 8-week supplementation. The national programme recommended supplementation with 1 mg of folic acid/day; the state government had been implementing the supplementation of 5 mg folic acid/day. The impact of supplementation with these two doses of folic acid on the Hb and folic acid levels were assessed at 8 week follow up samples. At enrolment the prevalence of Vit B12 deficiency was over 40% in pregnant women. Other research studies have also reported high prevalence of Vit B12 deficiency from India and adverse consequences associated with low vit B 12 levels in pregnant women. In view of this one group in the randomised study received Vit B12 in addition to iron and folic acid supplementation. Paired samples at enrolment and after 8-week supplementation were compared to assess the impact of supplementation with Vit B12 on Hb and Vit B12 levels.
USEFULNESS OF HAEMOGLOBIN IN ASSESSING THE IMPACT OF DIFFERENT DOSES OF SUPPLEMENTATION
Data from our study showed that the mean Hb in anaemic pregnant women (Hb between 8.0-10.9) was 9.7 g/dl. Of these only 14.1% had Hb between 8.0- 8.9 g/dL; 38.2% had Hb between 9.0-9.9g/dL and 47.7 % had Hb between 10.0-10.9g/dl. In all the four groups of pregnant women who received different doses and combination of micro-nutrient supplementation for 8 weeks, there was an improvement in the mean Hb by over 1 g/dl and a 50% reduction in the prevalence of anaemia. There were no differences in Hb or prevalence of anaemia in the group of women who received 60 mg or 240 mg of elemental iron supplementation. Gastro-intestinal side effects were lower in the groups where women received 60 mg of elemental iron supplementation. If side effects are lower the compliance and continuation rates are likely to be higher.
Paired data on Hb at enrolment and after 8 weeks of supplementation showed that it was possible to identify non-responders who did not show any improvement after 8-week supplementation as envisaged in the I-NIPI guidelines. In our study group, we screened women and enrolled only women who were healthy. Because of the strict inclusion criteria used for enrolment of the subjects in the study, very few women did not respond to supplementation. These women were referred to secondary care centres for further investigation and management.
The I-NIPI programme envisaged continuation of micro-nutrient supplementation till delivery. Earlier studies (from our institution and elsewhere in India) had shown that improvement in Hb with oral iron supplementation is slow. In view of this the research team requested all women who showed improvement in Hb after 8 weeks supplementation to continue the supplementation till delivery. Hb estimation in those who continued taking the supplements till 38 weeks of pregnancy showed that there was further improvement in Hb by over 0.5 g/dl and reduction in the prevalence of anaemia to 30% in all the four groups. Even in the women who failed to cross the cut-off and become non-anaemic at 38 weeks of pregnancy, there had been substantial improvement in Hb after supplementation. It is therefore imperative that micro-nutrient supplementation is continued till delivery and where ever possible for the first few months of lactation.
IMPACT OF SUPPLEMENTATION ON FERRITIN LEVELS
Paired data of ferritin at enrolment and after 8 weeks supplementation showed that there was an improvement in the mean ferritin in all the four groups. There were no significant differences in the mean ferritin or iron deficiency (ferritin <15 ng/ml) among women who received 60 mg of iron and those who received 240 mg of iron either at enrolment or after supplementation for 8 weeks. Comparison of paired data in women receiving supplementation showed that ferritin levels were not useful in assessing improvement in iron status in individuals. Similar results had been reported in women in reproductive age using iron fortified iodised salt for one year. Analysis of the paired values of TfR and hepcidin at enrolment and after 8 weeks of supplementation showed that they were also not useful in assessing improvement in iron status of individuals after supplementation.
IMPACT OF SUPPLEMENTATION WITH FOLIC ACID AND VITAMIN B12
In the last two decades there has been increase in the availability and use of serum folic acid and vit B12 estimation to assess folic acid and vit B12 status. Prevalence of folic acid deficiency in women at enrolment was low; about 40% of women had vit B12 deficiency. Analysis of the paired data on folic acid at enrolment and after 8-week supplementation showed that there was improvement in the mean folic acid with either of the doses. Supplementation with either 5 mg or 1.5 mg of folic acid did not have any impact on folic acid deficiency because prevalence of folic acid deficiency in these women was low at enrolment. Supplementation with 5 mg folic acid resulted in deterioration in mean vit B12 level and increase in the prevalence of vit B12 deficiency. In view of the low prevalence of folic acid deficiency, high prevalence of vit B12 deficiency in the study population and the reported adverse consequences of low vit B12 levels on mother child dyad, supplementation with 5 mg of folic acid should not be given.
Studies from several parts of the country have reported that over time there had been a reduction in the prevalence of folic acid deficiency and an increase in the prevalence of vit B12 deficiency and that there were adverse consequences of vit B12 deficiency. Prevalence of vit B12 deficiency was high at enrolment in our study. In our randomised supplementation studies, one group received vit B12 supplementation in addition to iron and folic acid and the impact was assessed on Hb and vit B12 status. Comparison of paired data, at enrolment and after 8 weeks of supplementation, showed that there was no significant improvement either in the mean Hb or mean vit B12 levels in those who received vit B12 supplementation. Similar lack of response to oral supplementation with vit B12 had been reported from studies over the last four decades. There is a need for further investigations to find out the reasons for the lack of response to oral vit B12 supplementation and explore how to improve the vit B12 status in pregnant women. Until a strategy to improve vit B12 status using oral vit B12 is found, the iron folic acid supplementation to pregnant women recommended in I-NIPI will have to continue.
ASSESSMENT OF MICRO-NUTRIENT STATUS BY HAEMATOLOGICAL PARAMETERS
Data from the present study showed that Hb is a good indicator for assessing the presence and severity of anaemia at enrolment, improvement after supplementation and identifying the non-responders to supplementation. Ferritin, folic acid and Vit B12 assays are very useful in assessing the prevalence of micro-nutrient deficiency at enrolment. Analysis of paired data on mean ferritin, folic acid and Vit B12 suggest that they are good indicators for assessing response of groups of women to different regimens of supplementation, but are not of use to identify individuals who are not responding to the supplementation with specific nutrients.
Until two decades ago, in clinical settings initial assessment of micro-nutrient deficiencies in nutritional anaemia was based on haematological parameters: RBC counts and morphological change in RBC seen in the peripheral smear; reassessment of these parameters along with reticulocyte count after 8 to 12 weeks of supplementation provided information on response to therapy. There has been a revival of interest in using these haematological indicators for assessment of micro-nutrient deficiencies in anaemic individuals. Re-introduction of these may help in improving access to detection of specific nutrient deficiencies at enrolment, providing appropriate supplementation and assessing the response in pregnant women with nutritional anaemia in primary health care settings.
Conclusions
Data from the present study showed that Hb is the optimal parameter for diagnosis of anaemia and severity of anaemia at enrolment. Biochemical estimations undertaken at enrolment showed that in pregnant women with Hb between 8.0 and 10.9 g/dl iron deficiency was the most common micro-nutrient deficiency, prevalence of folic acid deficiency was low (<5%), and Vit B12 deficiency was seen in 40% women.
Analysis of paired Hb at enrolment and after 8 weeks supplementation showed that there was no difference in response to 60 and 240 mg supplementation for 8 weeks, and higher dose of folic acid or addition of Vit B12 did have any impact on Hb. Paired data on Hb is useful in identifying the women who were not responding to supplementation. Therefore, it will be possible to implement I-NIPI recommendation that Hb be estimated in all pregnant women at enrolment and used to monitoring improvement after supplementation, identifying and referring the non-responders for investigation and management.
There was an improvement in the mean ferritin and reduction in iron deficiency as assessed by ferritin levels with supplementation (either 60 mg or 240 mg/day); the magnitude of improvement was similar in women who received 60 or 240 mg of iron daily. Mean ferritin was useful for monitoring the impact of iron supplementation in groups of women but not in assessing improvement in iron status in individual women. Concurrent CRP estimation along with ferritin was not useful in improving the detection of iron deficiency in women with inflammation because very few women had ferritin levels beyond 70 ng/ml (cut-off for iron deficiency recommended by WHO for those with CRP mg/L).
Mean folic acid levels were similar after 8-week supplementation with 5 mg or 1.5 mg of folic acid; supplementation did not have any impact on folic acid deficiency because folic acid deficiency at enrolment was <5%. There was a fall in mean vit B12 levels and an increase in vit B12 deficiency with 5 mg folic acid supplementation. In view of this supplementation with 5mg of folic acid should not be done. Addition of oral Vit B12 to iron and folic acid supplementation did not have any impact either on Hb or on Vit B12 level. There is a need to undertake studies to assess the reasons for the lack of improvement in Vit B12 levels following oral Vit B12 supplementation in pregnant women and also assess interventions to improve Vit B12 status in pregnant women.
Conflict of Interest Statement: None.
Funding Statement: The analysis of data and preparation of the manuscript was funded by Nutrition Foundation of India.
Acknowledgements: The authors gratefully acknowledge permission given by Nutrition Foundation of India for us to undertake this analysis.
ORCID ID: Prema Ramachandran: 0000-0003-1974-8281, K. Kalaivani: 0000-0002-9582-4488
References:
- De Maeyer E, Adiels-Tegman M. The prevalence of anaemia in the world. World Health Stat Quarterly. 1985;38(3):302-316.
- WHO The global prevalence of anaemia in 2011 (2015) Available from: https://apps.who.int/iris/handle/10665/177094 Accessed on 24.05.2025
- WHO Global Anaemia estimates: Anaemia in women and children 2021 Available from: https://www.who.int/news-room/fact-sheets/detail/anaemia accessed on 23.4.2025
- Menon MKK. Observations on anaemia in pregnancy. Proc Nutr Soc India. 1968;2:1-18.
- Prema K, Neela Kumari S, Ramalakshmi B. Anaemia and adverse obstetric outcome. Nutr Rep Int. 1981;23:637-643.
- Kalaivani K. Prevalence and consequences of anaemia in pregnancy. Indian J Med Res. 2009;130:627-633.
- Yusufji, D., Mathan, V. I. & Baker, S. J. 20. Iron, folate, and vitamin B12 nutrition in pregnancy: a study of 1 000 women from southern India. Bulletin of the World Health Organization. 1973;4(1). Accessed on 23.04.2025; Available from: https://apps.who.int/iris/handle/10665/263679
- Sood S, Ramachandran K, Mathur M, Gupta K. et al Effect of supplemental oral iron administration to pregnant women. WHO sponsored collaborative studies on nutritional anaemia in India. Q J Med. 1975;44:241-245.
- Ministry of Health and Family Welfare (MoHFW). Prophylaxis against nutritional anaemia among mothers and children Technical Information, MCH No. 1. New Delhi: Government of India; New Delhi. 1970
- Ministry of Health and Family Welfare. Report of the meeting on Prevention and control of nutritional anaemias. New Delhi: Government of India and UNICEF; 1989.
- Ramachandran P, Kalaivani K. Prevalence of Anaemia in India and Strategies for Achieving Sustainable Development Goals (SDG) Target. Proc Indian Natn Sci Acad. 2018;84(4):899-912.
- Muthayya S, Kurpad A, Duggan C, Bosch R. Low maternal vitamin B12 status is associated with intrauterine growth retardation in urban South Indians. Eur J Clin Nutr. 2006;60(6):791-801.
- Sharma A, Ravinder P, Nair M, Kalaivani K, Ramachandran P. Management of anaemia in based open randomized study. Indian J of Obst and Gyn Res. 2023;10(3):320-329.
- Sharma A, Ravinder P, Nair M, Kalaivani K, Ramachandran P. Treatment of anaemia in pregnancy with oral iron, folic acid or iron, folic acid and vitamin B12 supplementation: A hospital-based open randomized study. Indian J of Obst and Gyn Res. 2024;11(3):364-373.
- MOHFW. Govt. of India: National iron plus initiative for anaemia control. Accessed 5th Aug 2024. Available from: https://www.nhm.gov.in/images/pdf/programmes/child-health/guidelines/Control-of-Iron-Deficiency-Anaemia.pdf
- MOHFW. Anaemia Mukht Bharat Intensified National Iron Plus (INIPI) initiative and POSHAN Abhiyaan. Ministry of Health and Family Welfare, Government of India. April, 2018. accessed on 23.3.2025; available from: https://resources.anemiamuktbharat.info/Awareness_Generation/Anemia-Mukt-Bharat-brochureI-NIPI
- WHO Guideline on use of ferritin concentrations to assess iron status in individuals and populations 2020 accessed on 23.3.2025; available from: https://www.who.int/publications/i/item/9789240000124
- WHO Serum and red cell folate concentrations for assessing folate status in populations 2014 accessed on 23.3.2025; available from: https://www.who.int/publications/i/item/WHO-NMH-NHD-EPG-15.01
- WHO: Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. Geneva: 2011 accessed on 23.3.2025; available from: https://iris.who.int/handle/10665/85839
- WHO Guideline on haemoglobin cutoffs to define anaemia in individuals and populations accessed on 23.3.2025; available from: https://www.who.int/publications/i/item/9789240088542
- Katre P, Bhat D, Lubree H, Otiv S, Joshi S, Joglekar C, et al. Vitamin B12 and folic acid supplementation and plasma total homocysteine concentrations in pregnant Indian women with low B12 and high folate status. Asia Pac J Clin Nutr. 2010;19(3):335 43.
- Yajnik CS, Deshpande SS, Jackson AA, Refsum H, Rao S, Fisher DJ, et al. Vitamin B12 and folate concentrations during pregnancy and insulin resistance in the offspring: the Pune Maternal Nutrition Study. 15 Diabetologia. 2008;51(1):29 38.
- Nair KM, Bhaskaram P, Balakrishna N, Ravinder P, Sesikeran B. Response of haemoglobin, serum ferritin, and serum transferrin receptor during iron supplementation in pregnancy: a prospective study. Nutrition. 2004;20(10):896-
- J Chandra et al: Diagnosis, Treatment and Prevention of Nutritional Anemia in Children: Recommendations of the Joint Committee of Pediatric Hematology Oncology Chapter and Pediatric and Adolescent Nutrition Society of the Indian Academy of Pediatrics Indian Pediatr. 2022 Oct 15;59(10):782-801
- Ramachandran, P., and Kalaivani, K., 2025. Use of haemoglobin and ferritin to assess the need for and impact of use of iron fortified iodised salt. Medical Research Archives, [online] 13(5). Accessed on 21.07.2025; available from: https://doi.org/10.18103/mra.v13i5.6431