





Impact of Music in Stroke Rehabilitation: A Pilot Study
Impact of Accompaniment Music in App-Assisted Music-Based Therapy on Home Compliance and Movement Performance in Stroke: A Pilot Study
Yi-An Chen1*, Dhruv Pargai2, Martin Norgaard3, Gil Weinberg2
- Department of Occupational Therapy, Georgia State University, Atlanta, GA, USA.
2. Center for Music Technology, Georgia Institute of Technology, Atlanta, GA, USA.
3. School of Music, Georgia State University, Atlanta, GA, USA.
OPEN ACCESS
PUBLISHED 30 June 2025
CITATION Chen, Y., Pargai, D., et al., 2025. Impact of Accompaniment Music in App-Assisted Music-Based Therapy on Home Compliance and Movement Performance in Stroke: A Pilot Study. Medical Research Archives, [online] 13(6). https://doi.org/10.18103/mra.v13i6.6678
COPYRIGHT © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i6.6678
ISSN 2375-1924
ABSTRACT
Background: Technology-assisted home programs offer a promising approach to expanding access to rehabilitation, but may be limited by low patient compliance. Music-based therapy has been shown to enhance motivation and support holistic stroke recovery. Integrating music into technology-assisted home programs may improve adherence and amplify therapeutic benefits. To better understand how technology-assisted music-based therapy supports stroke recovery, it is important to identify features that promote high compliance and positive outcomes.
Aim: This pilot study examined the impact of accompaniment music on home rehabilitation compliance and motor performance during app-assisted music-based therapy in stroke survivors.
Methods: Six community-dwelling adults with chronic stroke completed a 2-week, within-subject study using KeyStroke, a stroke-specific music-based therapy app designed for self-directed upper extremity home exercise. Participants practiced piano-based song exercises under two alternating conditions: Music Mode (with accompaniment music) and Non-Music Mode (without accompaniment music). Two outcomes were analyzed: (1) total engagement time, measuring app usage as a proxy for home rehabilitation compliance, and (2) mean absolute delta time, assessing timing accuracy as an indicator of motor performance. Data were further categorized by the hand-use requirements of each song: more-affected hand only, less-affected hand only, and bimanual practice.
Results: Participants used the app for an average of ~30 minutes per day, 4-5 days per week over two weeks (4.51 ± 3.67 total hours), with an average total of ~14,000 keypresses. Total engagement times were higher in Music Mode than in Non-Music Mode across categories, with a particularly consistent result across participants for songs targeting the more-affected hand. Mean absolute delta times were also consistently better in Music Mode across all song categories. Notably, the training elicited a high volume of repetitions (~1,555 keypresses within 30 minutes), exceeding typical levels seen in outpatient clinics and approaching thresholds believed to promote neuroplasticity.
Conclusion: App-assisted music-based therapy with accompaniment music may support higher training compliance and improve motor performance in stroke rehabilitation. Background music may engage feedforward motor planning and enrich the rehabilitation experience. Although findings are preliminary due to the small, heterogeneous sample, they offer promising direction for future studies and app refinements targeting upper extremity recovery post-stroke.
Keywords
music therapy, stroke rehabilitation, home compliance, motor performance, technology-assisted therapy
INTRODUCTION
Stroke is one of the primary causes leading to significant long-term disabilities. To allow stroke survivors to sustain independence and to age-in-place, advanced healthcare services and rehabilitation therapies are needed. However, these services commonly come at a high cost and are limited to individuals without financial and insurance constraints. Limited access to healthcare services has been shown to be associated with poor health outcomes. Although clinical trials have demonstrated that a large dosage of rehabilitation exercises can lead to better stroke recovery, stroke survivors still generally receive inadequate rehabilitation assistance during the recovery process. To increase rehabilitation access and dosage for stroke survivors, home exercise or home rehabilitation programs are possible strategies to optimize stroke recovery. Specifically, technology-assisted home rehabilitation programs, such as app-assisted home exercises or telerehabilitation, have been shown to effectively improve motor functions, independence, and quality of life in stroke survivors. The potential low cost due to no transportation burden and the flexibility in terms of time and location enhance the advantages and benefits of technology-assisted home rehabilitation for individuals with stroke.
One of the biggest challenges of home exercise programs is patient compliance. Because of no direct guidance and side-by-side monitoring from therapists, home training sessions often require a high level of self-discipline and motivation. Stroke survivors need to adhere to a regimen which requires strong willpower, even when the home exercises are difficult or when they feel tempted to give up. Therefore, motivating and engaging patients in rehabilitation exercises in the home environment remains challenging, especially after an extended period.
To address rehabilitation adherence and enhance compliance with technology-assisted home rehabilitation programs, music can offer an effective approach. Listening and playing music has been shown to provide psychological and mental health benefits, including increased motivation and engagement. A recent systematic review reported that 85% of the reviewed seventy-nine studies indicated increased motivation with music compared to no music, and 90% of these articles also demonstrated improved clinical outcomes. Recently, researchers have explored the benefits of music-based therapy (MBT) in stroke rehabilitation. Systematic reviews and meta-analyses of clinical trials have emphasized its holistic effects on motor function and psychological well-being in stroke survivors, especially for those who undergo MBT training involving active musical instrument playing. We propose that the integration of technology-assisted MBT can further provide in-home rehabilitation services to support and empower individuals with stroke, helping them receive the rehabilitation training they need and improve or maintain their ability to live independently.
Previously, our team completed a pilot study (N=10) examining the feasibility of using a commercial mobile app to deliver a 3-week MBT program to stroke survivors at home. Our stroke participants reported high motivation (e.g., interest in extending training time), good compliance (i.e., no noteworthy decline in usage and an average app use time of approximately 33 minutes per day, 4-5 days per week), and positive motor outcomes (e.g., better finger dexterity) after training. The commercial app (Yousician, https://yousician.com) provides multi-sensory stimulation (e.g., auditory feedback from played musical notes, accompaniment music, visual cues for timing and accuracy) and includes several components known to enhance engagement (e.g., gaming elements). However, the commercial app was developed for the general public, without specific consideration for the needs of stroke survivors. To gain better insights related to how the app-assisted MBT supports stroke home rehabilitation and to facilitate the development of a stroke-specific MBT app, it is essential to identify which features led to the high compliance and positive outcomes observed in our previous study.
In this current study, we aimed to understand the potential impacts of accompaniment music during app-assisted MBT in stroke recovery as a first step. We provided in-home MBT using a newly developed piano training app created by our team to address the specific needs of stroke survivors and to generate rich data to support further development. Stroke participants received the MBT with two different modes of training (with or without accompaniment music), which were alternated daily over a two-week period. The purpose of the study was to examine participants’ home rehabilitation compliance and motor performance under both modes in order to explore the effect of incorporating background music into home-based rehabilitation exercises for stroke survivors. Based on the benefits of music-driven rehabilitation described above, we hypothesized that stroke survivors would demonstrate higher home rehabilitation compliance (i.e., longer app usage time) and better motor performance (i.e., greater timing accuracy) in the mode with accompaniment music compared to the mode without it.
METHODS
Participants
Participants were enrolled if they met the following inclusion criteria: (1) were 18 years or older, (2) had experienced a chronic stroke more than 6 months prior, (3) had at least minimal arm and hand motor capacity, as measured by the Fugl-Meyer Upper Extremity Assessment (FM, total motor score ≥ 20), (4) were community-dwelling, (5) were able to read and communicate in English, and (6) were capable of learning and using the mobile app after instruction. Participants were excluded if they had: (a) severe spasticity in elbow flexors, forearm supinators, wrist flexors, and digit flexors, as measured by Modified Ashworth Scale (MAS, score > 3 in each muscle group) to the extent that they cannot be properly positioned for piano playing, (b) unilateral spatial neglect, as screened by Albert’s Test, (c) impaired trunk balance that prevents them from maintaining a seated position, and (d) any active medical or neurological condition that would interfere with participation.
Prior to enrollment, all participants reviewed and signed an informed consent form according to the standard procedures of the Georgia State University Institutional Review Board.
Study Design
The study was conducted over a two-week period using a within-subject design. Stroke participants were provided with the MBT app developed by our team to play music and exercise their upper extremities using a piano keyboard at home. Two home visits were conducted by members of our team, one before and one after the two-week period, for clinical assessments, equipment setup, and equipment return.
Procedure
During the first home visit, participants completed a demographic form and a battery of screening and outcome assessments. We provided the keyboard and iPad with our piano training app pre-installed. After instruction, participants were asked to demonstrate their ability to use the app and keyboard independently.
Throughout the 2-week training, participants were encouraged to practice with the app as much as possible, with a suggested goal of one hour per day. Participants received a study contact phone number for assistance with any issues. At the end of the training, a second home visit was conducted for equipment collection, outcome assessments, and an exit interview.
Intervention (The Music-Based Therapy App)
Our team developed an app, KeyStroke, that provides music-based rehabilitation exercises for upper extremity motor recovery. The exercise protocol was specifically designed for stroke survivors and included three training tracks focusing on finger, wrist, and arm movements for either range of motion or coordination. Each track included multiple difficulty levels; for example, exercises range from using one digit (e.g., individual index finger) to coordinating multiple digits (e.g., thumb and index finger). Within each difficulty level, participants were instructed to start with the less-affected side, followed by the more-affected side, and then progress to bimanual practice. The app version used in this study contained 38 songs: 8 for the less-affected side, 8 for the more-affected side, and 22 for bimanual practice. Each song lasted approximately one minute. Participants were instructed to follow the instructions presented by the app to self-initiate music playing and exercise at home.
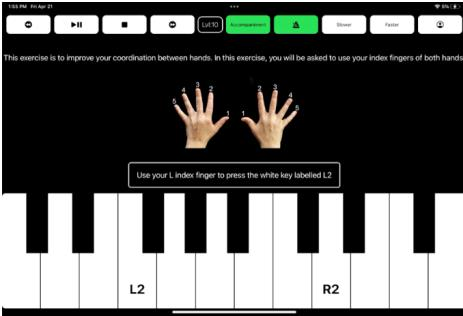
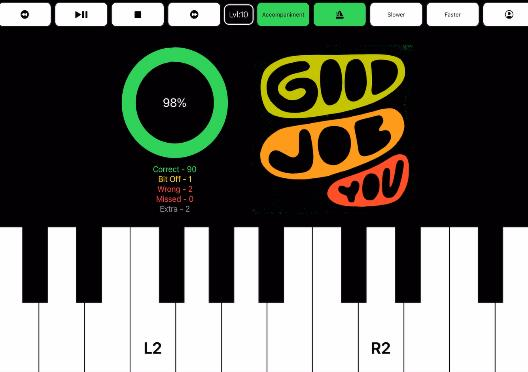
The app includes adjustable settings to meet participants’ needs. For example, participants can follow the default song sequence from the easiest to the most difficult, but they can also select specific songs and adjust song speed to match their capabilities, or repeatedly play preferred songs if desired. During the exercises, participants saw green blocks descending vertically on the screen, providing visual cues for timing and piano key selection. They also heard real-time auditory feedback from the piano keys they pressed. If a key was played correctly and accurately (within 200 milliseconds), it lit up green on the iPad. If it was slightly off (between 200 and 600 milliseconds), it lit up yellow. If pressed incorrectly, too early or too late (over 600 milliseconds), it lit up red, providing real-time visual feedback. If an extra key was pressed, it lit up gray instead. At the end of each practiced song, a scoreboard displayed performance metrics, including verbal-style encouragement (e.g., “Good job!â€) and a count of correct and missed key presses.
To explore the effects of accompaniment music on stroke survivors, the app alternated between two training modes: Music Mode and Non-Music Mode. In Music Mode, participants heard accompaniment music while performing the exercises; in Non-Music Mode, they heard only the notes they played, with no background music. All other visual cues and feedback remained consistent across both modes. The modes alternated daily over the two-week period, with participants counterbalanced on their initial starting mode.
Equipment
At the first home visit, participants were provided with a lightweight, portable piano keyboard (Yamaha Piaggero NP-12, 61 keys), which has a slightly lighter action than a full piano keyboard to facilitate use. Participants also received an iPad with our app installed, which could be placed on the built-in music stand on the piano keyboard.
Outcome Measures and Data Analysis
Musical Instrument Digital Interface (MIDI) data were collected from the keyboard and transmitted to cloud storage via the app during the 2-week participation. Two outcome measures were derived from the raw MIDI data: (1) total engagement time and (2) mean absolute delta time.
Total engagement time was used to quantify participants’ overall use of the app as an indicator of home rehabilitation compliance. It reflected the cumulative duration participants spent actively playing songs. For each song, engagement time was calculated as the interval between the start of each exercise song and the final keypress recorded for that song (i.e., engagement time = time of last keypress – song start time), and these values were summed across all songs played. Periods of app navigation between songs were excluded from this calculation.
Delta time served as an index of motor control accuracy in timing performance. It was defined as the temporal deviation between the expected keypress time and the actual keypress time. To assess each participant’s mean timing accuracy, the absolute delta times for each note were calculated first (i.e., absolute delta time = | actual keypress time – expected keypress time |) and then averaged across all keypresses. Smaller mean absolute delta times indicated better motor timing accuracy, with a value of zero representing the most optimal performance.
In addition to analyzing overall usage and timing accuracy across all songs, we categorized the results of the two outcome measures based on the song requirements for hand selection: (a) more-affected hand only (8 songs), (b) less-affected hand only (8 songs), and (c) bimanual practice (22 songs). This categorization allowed for a more detailed examination of the impacts of accompaniment music on individuals’ participation and performance, comparing between the more-affected and less-affected hands.
RESULTS
Participants
We enrolled six participants with chronic stroke from local hospitals and stroke support groups. Table 1 presents the characteristics of each individual participant. Even though no prior music experience was required, five of the six participants had previously played piano or another instrument (e.g., drums, violin, or guitar). During the study, most of them no longer played, except for one participant who still played the guitar almost daily (Participant 05). Additionally, three participants (Participants 03, 04, 05) were concurrently receiving therapy, including occupational therapy, physical therapy, and/or speech therapy, ranging from one to two sessions per week.
| Age | Sex | Race | Hand Dominance | Side of Weakness | Onset since Stroke (year) | Baseline FMA | Self-Reported Piano Skill Level | |
|---|---|---|---|---|---|---|---|---|
| Participant 01 | 72 | Male | Caucasian | Right | Left | 2.34 | 64 | Beginner, <1 year |
| Participant 02 | 49 | Female | Caucasian | Right | Right | 1.76 | 66 | Intermediate, 1-5 yrs |
| Participant 03 | 64 | Male | African American | Right | Right | 1.11 | 53 | Intermediate, 5-10 yrs* |
| Participant 04 | 27 | Female | Bi-Racial | Right | Right | 6.53 | 24 | Never Played* |
| Participant 05 | 69 | Male | Caucasian | Left | Right | 3.03 | 60 | Never Played* |
| Participant 06 | 43 | Female | African American | Left | Left | 4.81 | 54 | Never Played |
Mean ± SD: 56.9 ± 17.7, 3.2 ± 1.9, 50.1 ± 16.6
Overall Participation
During the study, participants actively used the app for an average of 9.00 ± 4.38 days (approximately 4-5 days per week over the two-week period) and played an average of 279.83 ± 202.81 attempts of song (range, 74 – 541 attempts).
Total Engagement Time
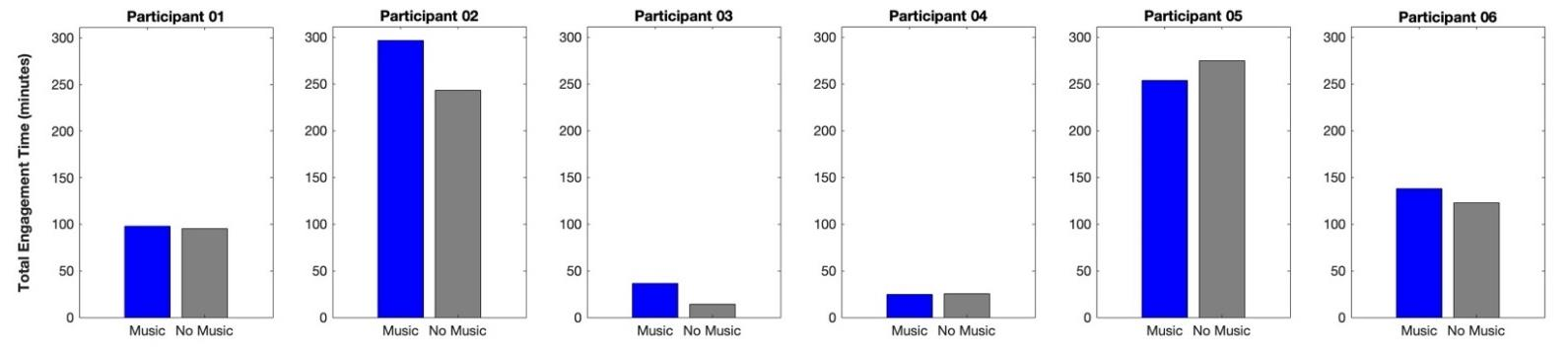
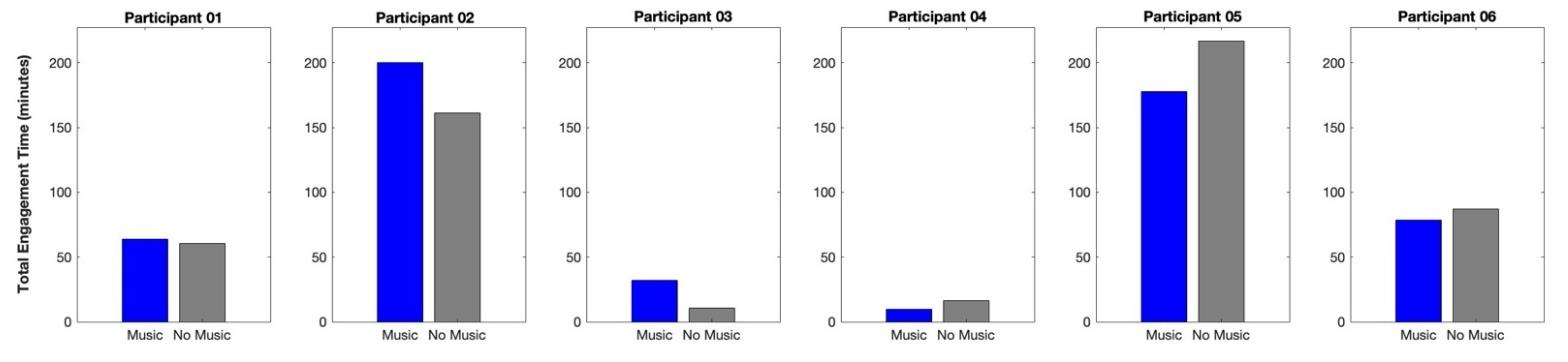
The average total engagement time across all participants was 4.51 ± 3.67 hours over the study period, with more time spent in Music Mode (141.24 ± 112.47 minutes) than in Non-Music Mode (129.33 ± 109.04 minutes). On active days (i.e., the days participants used the app), the average total engagement time was 26.81 ± 14.03 minutes per day. Participants generally used the app slightly more for exercise in Music Mode (28.56 ± 15.46 minutes per day) than in Non-Music Mode (25.61 ± 14.47 minutes per day). However, we observed variations among participants.
While most participants used the app more in Music Mode, the difference between modes was less than 10 minutes for two participants (Participant 01 and Participant 04) over the two-week period. Notably, one participant (Participant 05) engaged more in Non-Music Mode.
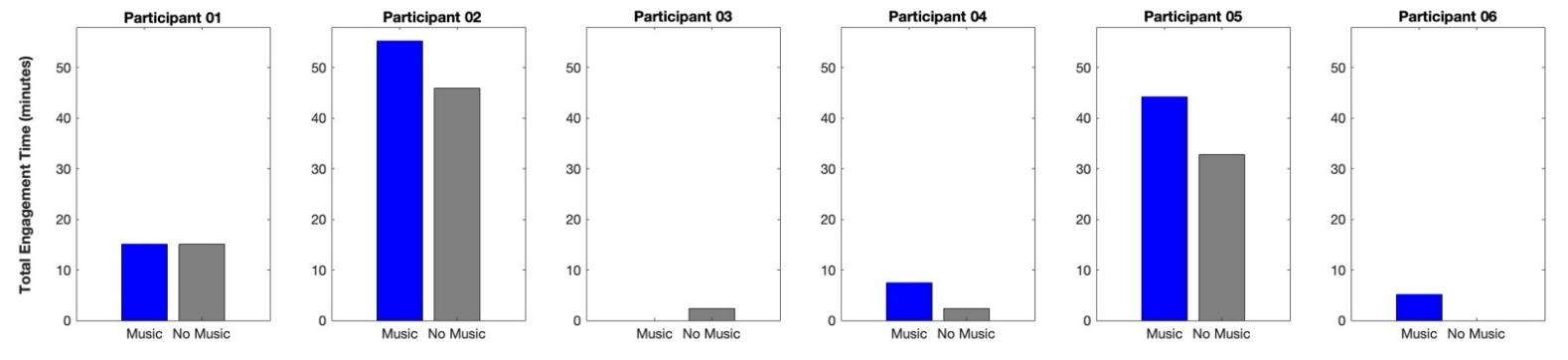
Interestingly, for the eight songs that required practice using only the more-affected hand, all participants consistently showed greater total engagement time in Music Mode (26.03 ± 19.62 minutes) compared to Non-Music Mode (20.29 ± 14.61 minutes).
Conversely, for songs that required playing with the less-affected hand only or bimanual practice, the total engagement time varied among participants.
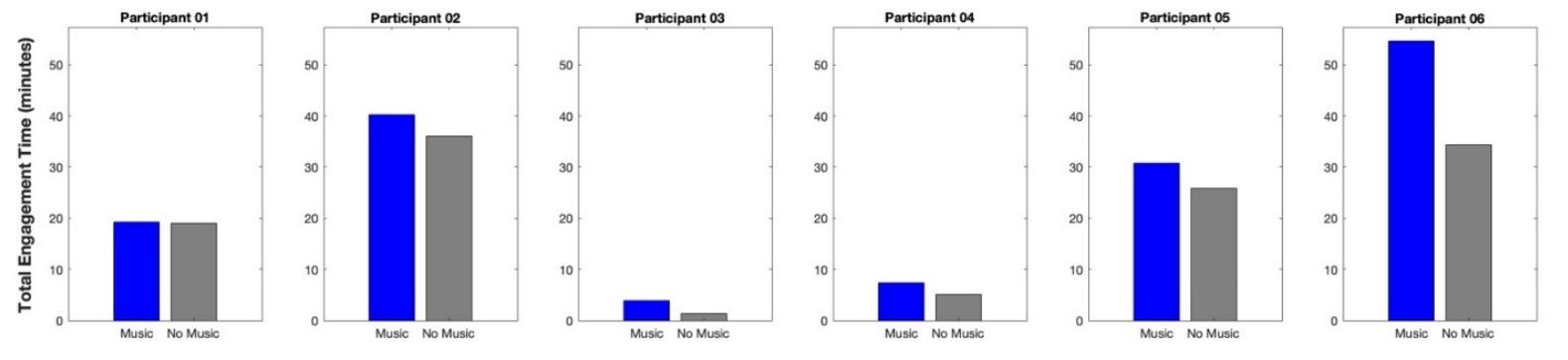
However, group averages still indicated a trend of greater total engagement time in Music Mode (21.20 ± 22.89 minutes for less-affected hand only; 93.66 ± 78.02 minutes for bimanual practice) compared to Non-Music Mode (16.45 ± 18.99 minutes for less-affected hand only; 92.10 ± 82.09 minutes for bimanual practice).
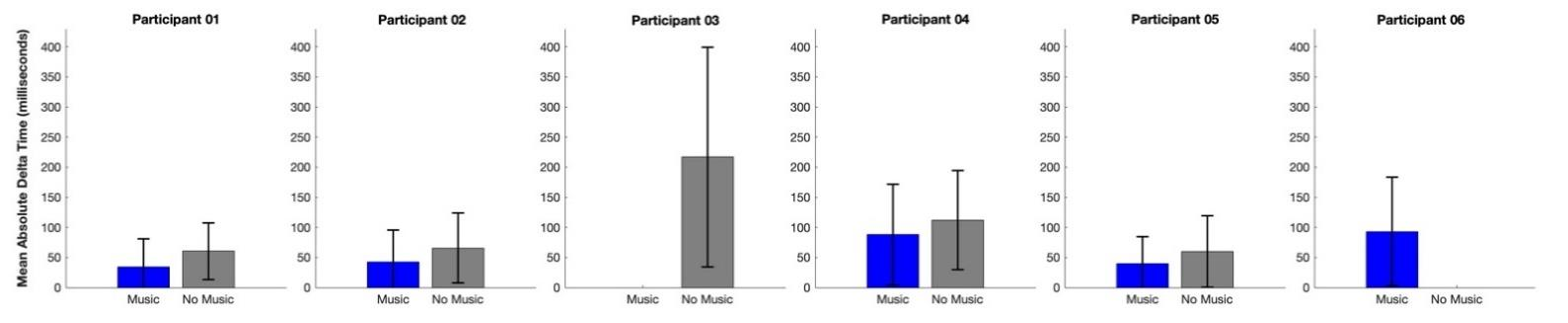
Mean Absolute Delta Time
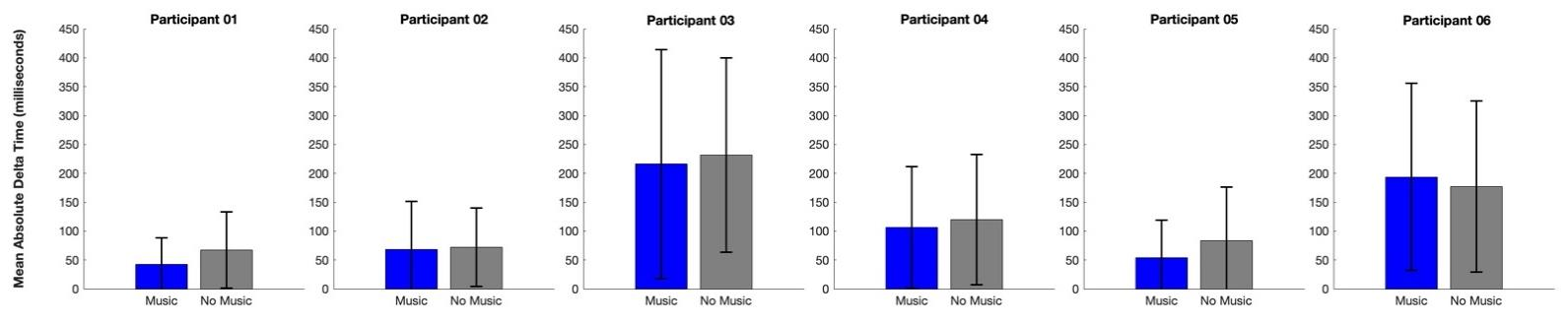
Throughout the two-week period, participants played and pressed an average of 13,956.83 ± 11,154.48 keys (range, 2360 – 27,940 keys across modes) during the app-assisted, in-home piano training. The mean absolute delta time of keypresses across all participants was 113.55 ± 74.28 milliseconds, with a better accuracy in Music Mode (119.08 ± 68.39 milliseconds) compared to Non-Music Mode (125.46 ± 66.30 milliseconds). We observed generally better accuracy performance in Music Mode across participants, except for one participant (Participant 06).
When examining the songs specifically required using the more-affected hand only, participants pressed an average of 1,694.83 ± 1,354.04 keys (range, 89 – 3,173 keys across modes) over the two weeks. They showed consistently better accuracy performance in Music Mode (70.38 ± 41.17 milliseconds) than in the Non-Music Mode (105.16 ± 40.38 milliseconds).
For songs that required playing with the less-affected hand only or bimanual practice, although some variance was present, we still observed a relatively consistent pattern among participants.
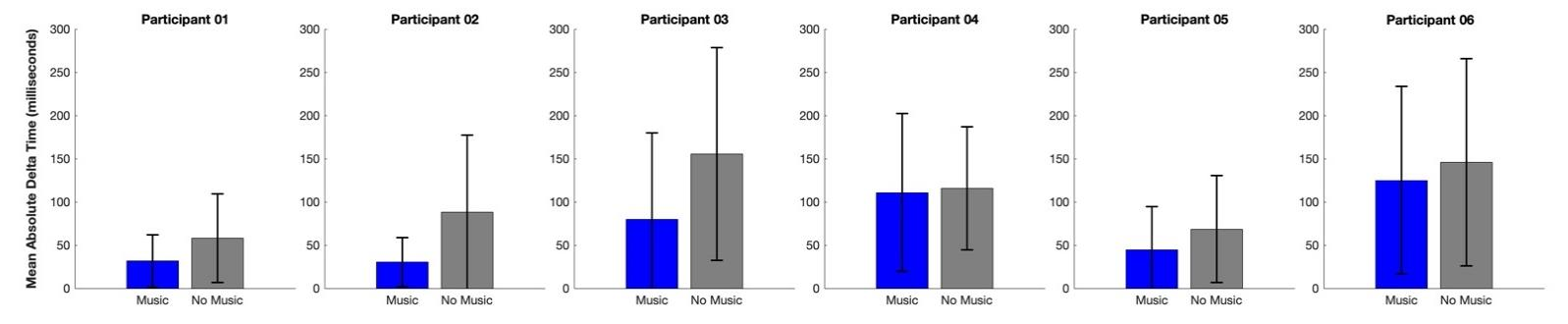
Group averages showed a smaller mean absolute delta time in Music Mode (59.44 ± 28.56 milliseconds for less-affected hand only; 121.52 ± 77.98 milliseconds for bimanual practice) compared to Non-Music Mode (102.92 ± 97.32 milliseconds for less-affected hand only; 128.20 ± 68.21 milliseconds for bimanual practice), indicating generally more accurate motor performance in Music Mode.
DISCUSSION
Consistent with our previous study and a recent MBT systematic review, stroke participants in this current study demonstrated good compliance, averaging approximately 30 minutes of exercise per day, 4-5 days per week over two weeks. During the exit interviews, participants provided positive feedback about receiving upper extremity rehabilitation through the app-assisted MBT, describing the training as entertaining and motivating due to the music. Three participants even reported that it inspired them to pursue piano playing as a leisure activity “for real†(Participant 02) or to learn something new after stroke (Participants 04 and 06). Others noted that the app-assisted training was convenient, allowing them to exercise at home without needing to travel. The challenge presented by the songs also encouraged continued practice and a desire to improve (Participants 04 and 06).
At the group level, we observed consistently higher engagement (i.e., greater app usage) in Music Mode than in Non-Music Mode, both across all songs and when categorizing the results by hand selection in song requirements. This finding aligned with our hypothesis that music would add a fun component to home rehabilitation and motivate stroke survivors to exercise more consistently. This was also supported by participant feedback, such as “The days without music were very boring†(Participant 02) and “I preferred the music days†(Participant 03).
However, two noteworthy points emerged upon closer examination. First, the differences in total engagement time between modes were relatively small. For example, across the two-week study period, the difference was about 12 minutes (141.24 vs. 129.33 minutes in Music and Non-Music Modes, respectively), and for bimanual practice songs, the difference was only 1.5 minutes (93.66 vs. 92.10 minutes). Second, greater usage in Music Mode was not consistent among all participants. For instance, Participant 05 exercised slightly more in Non-Music Mode, and Participants 04 and 06 showed somewhat higher app usage in Non-Music Mode for bimanual practice.
We speculate that the small differences of usage between modes may be influenced by a combination of social desirability bias and the Hawthorne effect. Social desirability bias refers to the tendency of participants to behave or respond in ways they believe will be viewed favorably by researchers. The Hawthorne effect describes behavioral changes that occur simply due to the awareness of being observed or participating in a study, rather than as a result of specific experimental manipulation. Given that our stroke participants were likely educated by healthcare professionals throughout their recovery journey about the importance of rehabilitation exercises and were aware of their involvement in the study, it is possible they were highly motivated to exercise consistently, regardless of the mode. Although they reported that training with music was more engaging and preferable, they may have been equally committed to completing the exercises under Non-Music Mode. Additionally, because the training period lasted only two weeks, a relatively short timeframe, it may have been easier for participants to maintain the exercise level even during the less preferred condition. A longer study period may be necessary to more fully examine how social desirability bias and the Hawthorne effect influence participants’ commitment and compliance.
Regarding timing accuracy, we observed a consistent pattern in participants’ motor performance, as indicated by the mean absolute delta time. Overall, participants demonstrated better motor accuracy (i.e., smaller mean absolute delta time) when exercising in Music Mode compared to Non-Music Mode. Although there was also some variation (i.e., Participants 02 and 06 showed better performance in Non-Music Mode for bimanual practice), nearly all participants exhibited consistently better motor performance across all song categories.
We propose that this effect may be attributed to the feedforward learning mechanism. In music performance, the feedforward loop involves anticipatory motor planning and auditory-motor interactions. For example, expert pianists develop internal models through extensive training that enable rapid and precise note execution. Notably, neural activity indicative of error detection has been observed approximately 70 milliseconds before an incorrect note is played. This pre-error signal suggests that the feedforward loop in the brain predicts potential errors and initiates internal corrections before external feedback is received. Such anticipatory monitoring underscores the role of internal predictions in guiding motor performance, rather than relying solely on real-time auditory feedback.
Under the Music Mode, our stroke participants could hear accompaniment music and use it as a sensory cue to predict and prepare for upcoming key presses. The accompaniment music may serve as an anticipatory guidance, enhancing motor planning. The connection between accompaniment music cues and anticipatory motor planning may facilitate improved motor performance by strengthening communication between auditory and motor brain regions. Previous studies have highlighted this key mechanism of MBT, noting that increased coherence in auditory-motor loops is associated with better brain function and stroke recovery. In contrast, under the Non-Music Mode, our participants had to rely solely on the visual cues and auditory feedback (i.e., the sound of the note they played), which may have provided less support for motor performance compared to the enriched sensory environment in Music Mode. Therefore, our findings further underscore the importance of accompaniment music in rehabilitation exercises.
In addition to our primary findings, this study provides further evidence that piano playing can inherently deliver a high dose of repetitive movements, such as finger flexion and extension, even during brief practice sessions. Over the two-week training period, our participants pressed an average of approximately 14,000 keys across a total of 4.51 hours of practice. This translates to roughly 1,555 repetitions involving fingers, wrist, or shoulder movements within a 30-minute session. This substantially exceeds the average 32 repetitions per session typically seen in outpatient clinics. Moreover, the repetition volume achieved through our app-assisted home MBT more closely aligns with the recommended 400-600 daily repetitions or even the 600-1,000 daily repetitions, which are considered necessary to induce structural and functional brain changes for motor recovery post-stroke. The melodic and rhythmic nature of song-based practice helps make these repetitions feel less monotonous, effectively embedding essential rehabilitation exercises into an enjoyable and motivating activity. These findings underscore the potential of our app-assisted home MBT to promote upper extremity recovery in stroke survivors.
Our study had several limitations. First and foremost, the sample size was small. Our team has been continuously refining the app through ongoing pilot testing and data collection. Although the findings from this study require further validation, they have been valuable in guiding modifications to the app for future testing and development. Second, our stroke participants were somewhat heterogeneous. Three had impairments on their dominant (right) side, while the remaining three presented varied combinations (e.g., right-hand dominance with left-side impairment; left-hand dominance with right-side impairment). In addition, participants’ piano experience ranged from none to 5-10 years. While half of the participants had never played the piano before, many had experience with other musical instruments. The impact of these factors on home rehabilitation compliance with our app-assisted MBT and on motor performance, particularly timing accuracy, remains unclear. Due to the small sample size, we were unable to conduct subgroup analyses based on these characteristics.
CONCLUSION
This pilot study demonstrated the potential benefits of accompaniment music in app-assisted, in-home MBT for stroke rehabilitation. Participants exhibited good compliance and motor performance, particularly in timing accuracy, when training with accompaniment music. These findings support the role of music as a motivating and enriching element in rehabilitation. Our data also highlight the value of high-dose, repetitive movement practice achievable through piano-based tasks. While the small and heterogeneous sample limits generalizability, the results provide promising evidence to guide future app refinements. Larger-scale studies with longer intervention periods and more diverse participant profiles are warranted to further evaluate the benefits of app-assisted MBT in promoting upper extremity recovery post-stroke.
CONFLICTS OF INTEREST STATEMENT
The authors have no relevant financial or non-financial interests to disclose.
FUNDING STATEMENT
This study was supported by TechSAge, which is funded by grant #90REGE0021 from the National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR), a Center in the Administration for Community Living (ACL), Department of Health and Human Services (HHS).
Acknowledgements: We would like to thank Evan Szypulski for assistance with musical content development.
REFERENCES
- Tsao CW, Aday AW, Almarzooq ZI, et al. Heart disease and stroke statistics-2023 update: A report from the American Heart Association. Circulation. 2023;147(8):e93-e621. doi:10.1161/cir.0000000000001123
- Martin SS, Aday AW, Almarzooq ZI, et al. 2024 heart disease and stroke statistics: A report of US and global data from the American Heart Association. Circulation. 2024;149(8):e347-e913. doi:10.1161/cir.0000000000001209
- Skolarus LE, Meurer WJ, Burke JF, Prvu Bettger J, Lisabeth LD. Effect of insurance status on postacute care among working age stroke survivors. Neurology. 2012;78(20):1590-5. doi:10.1212/WNL.0b013e3182563bf5
- Medford-Davis LN, Fonarow GC, Bhatt DL, et al. Impact of insurance status on outcomes and use of rehabilitation services in acute ischemic stroke: Findings from get with the guidelines-stroke. J Am Heart Assoc. 2016;5(11) doi:10.1161/jaha.116.004282
- Lohse KR, Lang CE, Boyd LA. Is more better? Using metadata to explore dose–response relationships in stroke rehabilitation. Stroke. 2014;45(7):2053-2058. doi:10.1161/STROKEAHA.114.004695
- Winstein C, Kim B, Kim S, Martinez C, Schweighofer N. Dosage Matters. Stroke. Jul 2019;50(7):1831-1837. doi:10.1161/strokeaha.118.023603
- Lang CE, Macdonald JR, Reisman DS, et al. Observation of amounts of movement practice provided during stroke rehabilitation. Arch Phys Med Rehabil. Oct 2009;90(10):1692-8. doi:10.1016/j.apmr.2009.04.005
- Young BM, Holman EA, Cramer SC. Rehabilitation therapy doses are low after stroke and predicted by clinical factors. Stroke. 2023;54(3):831-839. doi:10.1161/strokeaha.122.041098
- Mayo NE. Stroke rehabilitation at home. Stroke. 2016;47(6):1685-1691. doi:10.1161/STROKEAHA.116.011309
- Chen Y, Abel KT, Janecek JT, Chen Y, Zheng K, Cramer SC. Home-based technologies for stroke rehabilitation: A systematic review. Int J Med Inform. 2019;123:11-22. doi:10.1016/j.ijmedinf.2018.12.001
- Niyomyart A, Ruksakulpiwat S, Benjasirisan C, et al. Current status of barriers to mHealth access among patients with stroke and steps toward the digital health era: Systematic Review. JMIR Mhealth Uhealth. 2024;12:e54511. doi:10.2196/54511
- Cramer SC, Young BM, Schwarz A, Chang TY, Su M. Telerehabilitation following stroke. Phys Med Rehabil Clin N Am. 2024;35(2):305-318. doi:10.1016/j.pmr.2023.06.005
- Carraturo G, Pando-Naude V, Costa M, Vuust P, Bonetti L, Brattico E. The major-minor mode dichotomy in music perception. Phys Life Rev. 2025;52:80-106. doi:10.1016/j.plrev.2024.11.017
- Dimitriadis T, Della Porta D, Perschl J, Evers AWM, Magee WL, Schaefer RS. Motivation and music interventions in adults: A systematic review. Neuropsychol Rehabil. Jun 2024;34(5):649-678. doi:10.1080/09602011.2023.2224033
- Vigl J, Ojell-Järventausta M, Sipola H, Saarikallio S. Melody for the Mind: Enhancing Mood, Motivation, Concentration, and Learning through Music Listening in the Classroom. Music & Science. 2023;6:20592043231214085. doi:10.1177/20592043231214085
- Wu Q, Chen T, Wang Z, et al. Effectiveness of Music Therapy on Improving Treatment Motivation and Emotion in Female Patients with Methamphetamine Use Disorder: A Randomized Controlled Trial. Substance Abuse. 2020;41(4): 493-500. doi:10.1080/08897077.2019.1675117
- Hankinson K, Shaykevich A, Vallence AM, Rodger J, Rosenberg M, Etherton-Beer C. A Tailored Music-Motor Therapy and Real-Time Biofeedback Mobile Phone App (‘GotRhythm’) to Promote Rehabilitation Following Stroke: A Pilot Study. Neurosci Insights. 2022;17:26331055221100587. doi:10.1177/26331055221100587
- Wang Z, Xue Y, Sun G, et al. Effects of music-supported therapy for depression and cognitive disorders in people living with stroke and its impact on quality of life: A systematic evaluation and meta-analysis. Cerebrovasc Dis. 2025:1-26. doi:10.1159/000543361
- Huang WH, Dou ZL, Jin HM, Cui Y, Li X, Zeng Q. The effectiveness of music therapy on hand function in patients with stroke: A systematic review of randomized controlled trials. Frontiers in neurology. 2021;12:641023. doi:10.3389/fneur.2021.641023
- Zhang Y, Cai J, Zhang Y, Ren T, Zhao M, Zhao Q. Improvement in stroke-induced motor dysfunction by music-supported therapy: A systematic review and meta-analysis. Sci Rep. 2016;6:38521. doi:10.1038/srep38521
- Chen Y-A, Norgaard M. Important findings of a technology-assisted in-home music-based intervention for individuals with stroke: A small feasibility study. Disability and Rehabilitation: Assistive Technology. 2024;19(6):2239-2249. doi:10.1080/17483107.2023.2274397
- Tosto-Mancuso J, Tabacof L, Herrera JE, et al. Gamified Neurorehabilitation Strategies for Post-stroke Motor Recovery: Challenges and Advantages. Curr Neurol Neurosci Rep. Mar 2022;22(3):183-195. doi:10.1007/s11910-022-01181-y
- Sullivan KJ, Tilson JK, Cen SY, et al. Fugl-Meyer assessment of sensorimotor function after stroke: Standardized training procedure for clinical practice and clinical trials. Stroke. 2011;42(2):427-32. doi:10.1161/STROKEAHA.110.592766
- Woytowicz EJ, Rietschel JC, Goodman RN, et al. Determining Levels of Upper Extremity Movement Impairment by Applying a Cluster Analysis to the Fugl-Meyer Assessment of the Upper Extremity in Chronic Stroke. Archives of Physical Medicine and Rehabilitation. Mar 2017;98(3):456-462. doi:10.1016/j.apmr.2016.06.023
- Ansari NN, Naghdi S, Arab TK, Jalaie S. The interrater and intrarater reliability of the Modified Ashworth Scale in the assessment of muscle spasticity: Limb and muscle group effect. NeuroRehabilitation. 2008;23(3):231-237. doi:10.3233/nre-2008-23304
- Han CE, Kim S, Chen S, et al. Quantifying arm nonuse in individuals poststroke. Neurorehabilitation and Neural Repair. Jun 2013;27(5):439-47. doi:10.1177/1545968312471904
- Chen Y-A, Norgaard M, Albright R, Buchman E, Maitra K. A Home-Based, Mobile-Health-Assisted Piano Therapy to Improve Upper-Extremity Performance in Stroke Survivors: A Pilot Study. The American Journal of Occupational Therapy. 2020;74(4_Supplement_1):7411515391p1-7411515391p1. doi:10.5014/ajot.2020.74S1-PO4732
- Chen Y-A, Norgaard M. A Home-Based, mHealth-Assisted Piano Therapy to Improve Upper Extremity Performance in Stroke Survivors: A Pilot Study. Archives of Physical Medicine and Rehabilitation. 2020;101(11):e50. doi:10.1016/j.apmr.2020.09.148
- Grimm P. Social Desirability Bias. In J. Sheth, & N. Malhotra (Eds.) ed. Wiley International Encyclopedia of Marketing. Hoboken, NJ: John Wiley & Sons.; 2010.
- van de Mortel TF. Faking it: social desirability response bias in self-report research. Australian Journal of Advanced Nursing. 2008;25(4):40-48.
- Sedgwick P, Greenwood N. Understanding the Hawthorne effect. Bmj. Sep 4 2015;351:h4672. doi:10.1136/bmj.h4672
- Adair JG. The Hawthorne effect: A reconsideration of the methodological artifact. Journal of Applied Psychology. 1984;69(2):334-345. doi:10.1037/0021-9010.69.2.334
- Maidhof C. Error monitoring in musicians. Review. Frontiers in Human Neuroscience. 2013-July-26 2013;Volume 7 – 2013 doi:10.3389/fnhum.2013.00401
- Ruiz MH, Jabusch HC, Altenmüller E. Detecting wrong notes in advance: neuronal correlates of error monitoring in pianists. Cereb Cortex. Nov 2009;19(11):2625-39. doi:10.1093/cercor/bhp021
- Rojo N, Amengual J, Juncadella M, et al. Music-supported therapy induces plasticity in the sensorimotor cortex in chronic stroke: a single-case study using multimodal imaging (fMRI-TMS). Brain Inj. 2011;25(7-8):787-93. doi:10.3109/02699052.2011.576305
- Fujioka T, Ween JE, Jamali S, Stuss DT, Ross B. Changes in neuromagnetic beta-band oscillation after music-supported stroke rehabilitation. Ann N Y Acad Sci. Apr 2012;1252:294-304. doi:10.1111/j.1749-6632.2011.06436.x
- Amengual JL, Rojo N, Veciana de Las Heras M, et al. Sensorimotor plasticity after music-supported therapy in chronic stroke patients revealed by transcranial magnetic stimulation. PLoS One. 2013;8(4):e61883. doi:10.1371/journal.pone.0061883
- Grau-Sanchez J, Amengual JL, Rojo N, et al. Plasticity in the sensorimotor cortex induced by music-supported therapy in stroke patients: A TMS study. Front Hum Neurosci. 2013;7:494. doi:10.3389/fnhum.2013.00494
- Ripollés P, Rojo N, Grau-Sánchez J, et al. Music supported therapy promotes motor plasticity in individuals with chronic stroke. Brain imaging and behavior. 2016;10(4):1289-1307. doi:10.1007/s11682-015-9498-x
- Ghai S, Maso FD, Ogourtsova T, et al. Neurophysiological changes induced by music-supported therapy for recovering upper extremity function after stroke: A case series. Brain Sciences. 2021;11(5):666.
- Palumbo A, Groves K, Munoz-Vidal EL, et al. Improvisation and live accompaniment increase motor response and reward during a music playing task. Sci Rep. 2024;14(1):13112. doi:10.1038/s41598-024-62794-6
- Lang CE, MacDonald JR, Gnip C. Counting repetitions: an observational study of outpatient therapy for people with hemiparesis post-stroke. J Neurol Phys Ther. 2007;31(1):3-10. doi:10.1097/01.npt.0000260568.31746.34
- Kleim JA, Jones TA. Principles of experience-dependent neural plasticity: implications for rehabilitation after brain damage. Journal of Speech Language and Hearing Research. 2008;51(1):S225-39. doi:10.1044/1092-4388(2008/018)
- Nudo RJ, Milliken GW, Jenkins WM, Merzenich MM. Use-dependent alterations of movement representations in primary motor cortex of adult squirrel monkeys. The Journal of Neuroscience. 1996;16(2):785-807. doi:10.1523/JNEUROSCI.16-02-00785.1996