






Impact of Neoliberalism on Global Health Systems
Global Health in the Grip of Neoliberalism: A Combined Retrospective Comparative Stages Heuristic Policy Analysis
Wafa Abuelkheir Mataria ¹, Sungsoo Chun ²
- Institute of Global Health and Human Ecology, American University in Cairo
- Institute of Global health and Human Ecology, American University in Cairo
OPEN ACCESS
PUBLISHED: 30 November 2024
CITATION:AbuElKheir-Mataria, W., and Chun, S., 2024. Global Health in the Grip of Neoliberalism: A Combined Retrospective Comparative Stages Heuristic Policy Analysis. Medical Research Archives, [online] 12(11). https://doi.org/10.18103/mra.v12i11.5843
COPYRIGHT © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i11.5843
ISSN 2375-1924
Abstract
Background: The COVID-19 pandemic revealed critical weaknesses in global health systems, many of which have roots in the neoliberal policies that have dominated global health governance since the 1980s. Neoliberalism, characterized by market-driven policies, privatization, and reduced government intervention, has profoundly impacted healthcare access, equity, and quality worldwide.
Objective: This study aims to analyze the impact of neoliberal reforms on health systems in various countries, focusing on the interplay between governance, policy formulation, and stewardship in the health sector. By examining the outcomes of these reforms, the study seeks to understand how different approaches to neoliberalism have shaped health system performance and equity.
Methods: The study employs the Stages Heuristic Model (SHM) to conduct a retrospective comparative analysis of health policy reforms in ten countries, including the United States, Chile, New Zealand, Ecuador, and China. The research synthesizes data from peer-reviewed articles to assess the outcomes of neoliberal policies on healthcare systems.
Results: The analysis reveals that in countries such as the United States and Chile, neoliberal reforms led to increased health inequities and a tiered healthcare system, where access to quality care became increasingly dependent on socioeconomic status. In contrast, countries like Taiwan, which balanced neoliberal reforms with strong public health initiatives, managed to maintain more equitable health systems. China and Venezuela, both of which initially adopted more interventionist healthcare policies, made notable early strides in improving access to healthcare and addressing inequities, particularly for underserved populations. However, Venezuela’s progress was undermined by economic challenges and insufficient support for higher-level care, leading to a decline in health outcomes over time.
Conclusion: The study underscores the need for governance models that prioritize equity and public health in healthcare systems. It suggests that while neoliberal policies can drive economic efficiency, they often do so at the cost of health equity, necessitating a re-evaluation of global health governance and policy approaches.
Keywords: Neoliberalism, health reform, economic reform, health inequity, social safety net, austerity measures, privatization.
Introduction
During the COVID-19 pandemic, health systems were criticized for their inadequate performance. Health systems’ lack of preparedness, overwhelmed infrastructure, and healthcare access inequities opened many discussions concerning the underlying reasons for these shortcomings. Issues were raised, mainly that current health systems are the result of the long trend of concentrating on efficiency, underinvestment in the public health sector, and pushing for the privatization of health services. These trends are directly related to neoliberalism and its proliferation as a dominant reform paradigm in the last decades.
“Neoliberalism” is an economic and political approach that advocates for limited government intervention in the economy, free-market capitalism, deregulation, and reducing social safety nets. In many places of the world, it has been a prominent economic and political doctrine. Originating in the late 20th century, neoliberalism gained prominence as a reaction to the perceived failures of Keynesian economics and state-led welfare models. Initially, after World War II, many newly independent and developing nations adopted state-led development and nation-building strategies, with governments heavily involved in managing demand, stabilizing markets, and promoting social welfare. However, the economic challenges of the 1970s, particularly the stagflation crises characterized by economic stagnation, high inflation, and high unemployment, led many countries to seek alternative economic approaches. Key principles of neoliberalism include prioritizing economic efficiency, privatization of public services, and fostering competition. Adopting a neoliberal ideology does not only affect the economy of a country but also its social aspects including health, education, and even the social structure. Neoliberalism has reshaped policies across various sectors, including health. Governments called for privatization, marketization, deregulation, and austerity measures, which gave rise to deep implications for healthcare access, equity, and quality.
This study examines how neoliberal reforms in healthcare have been applied across various national contexts and integrated into institutional frameworks. Through case studies from different countries, it provides a comparative overview of these policies’ socioeconomic and public health impacts on healthcare services. The analysis spans from the 1980s to the COVID-19 pandemic, exploring how long-term neoliberal reforms have shaped healthcare systems’ effectiveness and equity. The pandemic response is an example of these policies’ cumulative effects. The study also addresses the complexities of implementing neoliberal reforms in distinct socio-political environments and their long-term implications for healthcare delivery and public health outcomes.
Methods
DATA SOURCE AND COLLECTION
This study’s data collection was conducted in two steps to ensure a rigorous and comprehensive analysis of the impact of neoliberalism on healthcare reforms. The first step involved a systematic search in the Scopus database using the keywords “neoliberalism” and “health reform.” The primary goal was to identify relevant cases for analysis. Collected studies were organized using Zotero, a citation management tool, to eliminate duplicates. Each study’s title and abstract were reviewed for eligibility, focusing on studies written in English and relevant to neoliberalism and health reforms. Studies meeting these criteria were included a full-text review, aiding in selecting the most pertinent cases.
- Search Term: (TITLE-ABS-KEY (“neoliberalism” AND “health reform”)) AND (LIMIT-TO(LANGUAGE, “english”))
The initial search provided a foundational set of cases, but the information available was sometimes limited. To supplement the initial data, a second step was done where a search was conducted using Google Scholar. This supplementary search aimed to gather more detailed information on each identified case, including aspects related to healthcare systems, equity, and responses to the COVID-19 pandemic. Keywords such as country names, healthcare, equity, and COVID-19 were used to expand the scope of data collection, providing a more comprehensive understanding of the contextual factors influencing health outcomes.
POLICY ANALYSIS METHODS
This study employs an analytical framework of two steps. The Stages Heuristic Model (SHM) to understand the policy process and healthcare system and health equity changes in different countries. And, a comparative analysis to compare the experiences of different countries in adopting neoliberal reforms and their effects on health. Policy implications and recommendations for better more equitable health future outcomes in the context of neoliberalism were drawn from the results of the analysis.
The Stages Heuristic Model (SHM), as proposed by Lasswell and further developed by Brewer and DeLeon is known as the policy cycle framework. SHM is a multipurpose framework that has been used in political science, policy analysis, and public administration. It is a widely used policy analysis tool as it allows for understanding the policy process and analyzing policy accompanying changes and their implications. The SHM has five main steps:
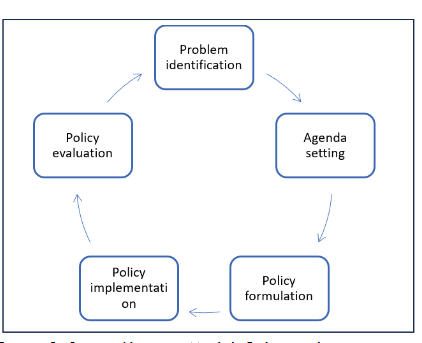
- Problem identification: This stage involves identifying the issues that led to the adoption of neoliberal reforms, considering all relevant factors such as economic challenges (e.g., high inflation and low growth rates), social tensions, and inefficiencies in the healthcare system. It also accounts for the broader context, including the dominance of neoliberalism as a hegemonic ideology influencing policy decisions and shaping the understanding of these issues as problems requiring intervention.
- Agenda setting, where policy options including neoliberal reforms are considered. It involves assessing these options within the context of the hegemonic influence of neoliberalism, which often prioritizes market-oriented solutions. The agenda-setting process considers the political and economic environment, stakeholders’ influence, and the extent to which neoliberal ideology has permeated policy discourse and decision-making processes.
- Policy formulation is where a decision is made and a policy is chosen often reflecting the neoliberal emphasis on privatization, deregulation, and reducing public sector involvement.
- Policy implementation to assess how neoliberal reforms were implemented in healthcare delivery.
- Policy evaluation which is an analysis of the outcomes of neoliberal reforms in terms of their impact on health including equity among socio-economic groups.
Comparative analysis is a powerful methodology within political science that allows for political systems, institutions, or processes comparison. Comparative analysis in this case deepens the understanding of the patterns, trends, commonalities and differences in the adoption of neoliberal reform and its impact on health outcomes in different countries giving valuable insight into the effectiveness of neoliberal reforms and their implication in a country’s healthcare system. For this study, the comparative analysis was done through cross-case synthesis where stages of the policy process were compared among country cases followed by a thematic analysis where overarching themes related to the impact of the adoption of neoliberal ideology on healthcare systems are discussed taking into consideration the trade-offs between economic liberalization and its immediate and long-term impact on health access, equity and outcomes.
The combination of the SHM and comparative analysis not only provides a comprehensive framework for examining the intricacies of policy development but also enables the identification of unique national responses to neoliberal reforms. This dual approach is crucial in uncovering the underlying factors that influence the variation in healthcare system transformations and their subsequent impacts on equity and access.
Results
SEARCH RESULTS
The systematic search in the Scopus database resulted in 29 studies within which there are 2 books and 27 peer-reviewed articles within which there were 11 studies covering specific countries (Senegal(1), Chile (4), New Zealand (2), Colombia(1), Turkey(1), Ecuador(2), Taiwan(1), China (2), Venezuela(1), Guyana (1), USA (2)), three studies covered specific areas (Latin America (2), Latin America and Africa (1)) and five of them are general (not country-specific).
STAGES HEURISTIC MODEL
The second part of the results is divided by countries where each country’s neoliberal reform and its effect on health are analyzed using the SHM and its five steps.
Chile
Problem identification: Before the 1970s, Chile faced social and political tension due to unequal land distribution, where land ownership was concentrated in the hands of the wealthiest portion of the population, leading to stagnation of a highly potential agricultural sector. Chile faced economic challenges, including high inflation, low growth rates, and fiscal deficits. Moreover, the government perceived inefficiencies in the healthcare system, characterized by inequities in access and quality of care, and rising healthcare costs.
Agenda setting: To face the economic problems, Pinochet, in the 1970s brought a group of economists “Chicago Boys” from Chicago University to implement economic reform. They called mainly for the privatization of state-owned companies, trade Liberalization opening of the Chilean economy for foreign competition, and export-oriented growth where the industrial focus shifted toward productivity for export.
Policy formulation: Under the leadership of Augusto Pinochet, in the 1980s Chile adopted an economic reform highly influenced by the neoliberal doctrine. The reform encompassed the healthcare system. The 1981 Health Sector Reform aimed to increase efficiency, competition, and consumer choice in healthcare provision.
Policy implementation: The implementation of the healthcare reform led to the privatization of healthcare services, the introduction of a private health insurance system and user fees and decreased public spending on health.
Policy evaluation: Although Pinochet’s reforms led to economic growth, they came at the expense of social aspects, particularly in the public sector. The austerity measures and reduction of state intervention resulted in a tiered healthcare system characterized by user fees, with a higher quality private healthcare sector and a lower quality public sector. This system disproportionately benefited wealthier individuals who could afford private care, while the public sector, burdened by limited resources, offered lower quality services. Additionally, the reforms decentralized healthcare responsibilities, shifting them to localities. This shift meant that areas rich in resources could provide better quality healthcare services, while poorer regions suffered from fewer and lower-quality provision points. As a result, there were significant socioeconomic inequalities in access to services based on wealth, gender, and place of residence. Key social aspects, such as equitable access to healthcare and strong public health infrastructure, were neglected. Following Pinochet’s era, from the 1990s to the present, Chile’s policy focus shifted towards maintaining economic growth while also addressing social disparities. This period saw an increase in social spending aimed at poverty reduction and improving healthcare accessibility.
Ecuador
Problem Identification: In Ecuador, the adoption of neoliberal policies manifested as a hegemonic shift towards a market-oriented economy, which affected various sectors, including health. This shift was characterized by a reduction in state intervention, an emphasis on privatization, and an increased reliance on market mechanisms. The country’s economic trajectory was significantly influenced by its dependence on oil revenue, particularly after the discovery of oil in the 1960s. This dependence became problematic when falling oil prices led to economic crises marked by high inflation, unsustainable public debt, currency devaluation, and stagnant growth.
These broader economic challenges, driven by neoliberal economic policies, had direct repercussions on the healthcare system. The market-oriented approach resulted in significant fragmentation within the healthcare system, inequitable access to services, and financial barriers for the population. Specifically, out-of-pocket payments for healthcare reached as high as 61%, imposing a heavy financial burden on many citizens. This environment fostered a healthcare landscape where access and quality of care were increasingly determined by market forces rather than equitable public provision.
Agenda setting: These economic challenges along with other factors including the pressure to adopt the International Monetary Fund (IMF) suggested solution which concentrated on privatization, trade liberalization and austerity measures created pressures to adopt a more neoliberal approach to stabilize the economy and promote growth. In the period (2007-2017) during Rafael Correa’s presidency, the government recognized the presence of these problems in the healthcare system and considered the National Plan for Good Living and healthcare reform.
Policy formulation: the Ecuadorian government enacted the Organic Law of Health, and implemented various initiatives to operationalize the reform. The declared objective was to concentrate on the social determinants of health, equity and inclusion.
Policy implementation: Correa’s government started a centralized state approach to health reform. The reform included an increase in the budget for the Ministry of Health (MoH), increased investment in infrastructure, equipment and human resources for health and extended the social protection scheme making it tax-based financed and supported by oil revenue.
Policy evaluation: although the healthcare reform implemented before Correa has never been declared to be neoliberal reforms, they were criticized to be a “silent” neoliberal reform as it was accompanied by limited public spending, increased government engagement with private health service providers, the limited access to certain healthcare services such as access to specialists and the high out-of-pocket expenses. Correa’s government transformation plan intended to reverse these effects however, the transformation was criticized to be slow. Fragmentation persisted and It appeared far-fetched that an effective taxation system would ever be implemented.
Colombia
Problem identification: several challenges were identified in the Colombian healthcare system mainly: accessibility, quality, and equity which needed to be addressed.
Agenda setting: in the 1990s under the guidance of IMF and the World Bank, Colombia was one of the countries that were forced to adopt a more neoliberal approach limiting their interventionist role. This approach was extended to reach the healthcare sector and a neoliberal reform for health reached the agenda.
Policy formulation: the neoliberal reform was introduced through Law 100/93 which emphasized market competition and privatization in Colombia’s healthcare system with the aim of improved efficiency and expanded access.
Policy implementation: the reform implementation resulted in the proliferation of private health providers, increased competition between insurers and increased workload on health professionals leading to dissatisfaction.
Policy evaluation: the reform increased the concentration on profit over care resulting in a dehumanized and fragmented healthcare system with unequal access to healthcare services as patients with limited resources might have difficulty accessing quality care under this system. Moreover, the focus shifted towards tasks rather than holistic care coordination limiting the health workforce’s ability to utilize their full skill set.
Venezuela
Problem identification: Before Chávez’s administration, Venezuela’s healthcare system faced significant challenges, including inequitable access to services and resource shortages. High proportion of the population lacked access to high-quality care, although the country was regionally recognized for advancements in specialized fields like heart surgery and infectious diseases such as polio were largely controlled. Neoliberal policies in the 1980s and 1990s, emphasizing privatization and reduced public spending, led to a weakening of public healthcare infrastructure, contributing to growing inequalities in access to services.
Agenda setting: In contrast to the prevailing neoliberal trend in other Latin American countries, President Hugo Chávez advocated for a reform model centered on social justice, equity, and universal access to healthcare. His administration sought to address the shortcomings of the previous neoliberal policies by increasing state involvement in the healthcare sector and ensuring that all citizens, regardless of socioeconomic status, could access quality healthcare services.
Policy adoption: Barrio Adentro was introduced as a cornerstone healthcare reform, designed to address inequities in access by deploying Cuban health workers to underserved areas. The program established a network of primary care clinics (Consultorios Médicos Populares) and Comprehensive Diagnostic Centers (CDIs) to provide free, community-level care. Despite its focus on accessibility, concerns about the qualifications of the foreign professionals and the sustainability of the program arose, with some arguing that strengthening the existing health infrastructure would have been a more effective strategy.
Policy implementation: Barrio Adentro was successful in expanding access to primary care, especially in marginalized areas, but the focus on basic services left higher-level care underfunded. The program did not invest sufficiently in hospitals and specialized services, which led to a collapse of tertiary care infrastructure. Consequently, while primary care services expanded, the system struggled to manage more complex health needs.
Policy evaluation: Initially, Barrio Adentro helped improve access to healthcare in underserved communities, but long-term outcomes revealed a deterioration of the public healthcare system. Key health indicators, such as child growth parameters, declined, and shortages of medical staff and supplies became pervasive. Despite the government’s commitment to a state-led model, economic mismanagement and underfunding of healthcare during periods of high oil revenues weakened the system.
Guyana
Problem identification: Throughout the post-independence period, the Guyanese government has had relatively low resources, leaving it with little to spend on health. Guyana’s healthcare system has significant constraints, including limited access to healthcare services, inadequate infrastructure, and inequities in health outcomes, all of which required government intervention.
Agenda setting: in 1970s, the socialist government decided to act upon the healthcare system limitations making health a primary issue on the agenda. The government had a strong dedication of resources to public health.
Policy adoption: accordingly, the government introduced a clause into the development of the new Republican constitution that would guarantee “the right to free medical attention”. Emphasizing the provision of free healthcare as a fundamental principle of the new Republic.
Policy implementation: while implementing “the right to free medical attention” the government declared its inability to provide complete coverage of health service and advocated for the nation’s central principle of self-help through preventative care and the use of local resources in order to decrease the load on the health system and increase efficiency.
Policy evaluation: national economic difficulties continued and insufficient spending on the healthcare system continued leading to health workforce understaffing, and frozen salaries. The discussion of underspending and efficiency continued in the 1980s, reinforced by the World Bank structural adjustment loan introduced as a new vehicle to promptly transfer funds to numerous postcolonial countries, including Guyana.
New Zealand
Problem identification: New Zealand had a Universal taxpayer-funded health system that was supposed to cover the whole population. However, this system did not provide equitable access to healthcare services, especially for the indigenous Maori people. Furthermore, within this system, the government was supposed to cover two-thirds to three-quarters of the cost of healthcare services within this system. With time the government contribution value to the system eroded and patients covered most of the cost in the 1970s.
Agenda setting: Efforts to improve equity in access, particularly for the Maori, began in the 1970s when the Treaty of Waitangi was incorporated into legislation as a measure to affirm Maori rights. However, significant changes to the healthcare system were not observed until the 1980s and 1990s, when neoliberal policies were introduced by the elected market-driven government. During this period, the Treasury was strongly influenced by American ideas regarding the role of competition in the healthcare system, advising the government to adopt these policies.
Policy formulation: in the early 1990s significant changes were introduced to the healthcare system through the Green and White paper and the Youth Health and Public Health paper. Mainly, New Zealand embraced elements of corporatization as a solution for the healthcare system challenges.
Policy implementation: the adoption of these policy changes resulted in the increased role of the private sector, individuals became more financially responsible for their healthcare, and charges were introduced in secondary care in public hospitals. As for the Maori population, there was an increase in Maori health providers.
Policy evaluation: the reforms did not acknowledge the social determinants of health and cultural diversity in New Zealand. The neoliberal approach in New Zealand increased income and health inequities among the population. Despite the Maori increased access to health services through increased providers, Maori population health deteriorated due to the severe economic effects of neoliberal reforms on Maori families’ economic situation resulting in persisting health inequities. Since 1997, there has been a retreat from neoliberal free-market approach towards a more in between neoliberal social approach in healthcare system policies.
China
Problem identification: in 2003, The fourth-generation government of China acknowledged several healthcare system issues, including inequities in the distribution of health resources among different geographical areas, inadequate government spending on health, rising overall health expenditures resulting in a high rate of households experiencing catastrophic health expenses, and the lack of insurance coverage for around 45% of urban residents and 80% of rural residents.
Agenda setting: Although some scholars link China’s health reforms to the 2003 SARS outbreak, evidence suggests that the reform process had already begun earlier, notably with the issuance of the ‘Decision on the Further Improvement of Rural Health Work’ in October 2002. The government was facing increasing social discontent due to the implementation of neoliberal policies before the early 2000s and saw health reform as a way to address this tension.
Policy formulation: the government decided to expand several urban and rural government-administered health insurance programs.
Policy implementation: between 2003 and 2009 several modifications took place, namely: the establishment of the New Rural Cooperative Medical Insurance (NRCMI) for China’s rural population, the expansion of the Urban Employees Basic Medical Insurance (U-Employee) for urban employees, the establishment of the ‘rural medical assistance’ for rural residents in poverty, the ‘urban medical assistance’ for urban residents in poverty, and the Urban Residents Basic Medical Insurance (U-Resident) for urban residents. Finally, the development of a national essential drug list, reform of the primary health care system, and reform of public hospitals.
Policy evaluation: Although the uninsured proportion of the population fell from more than 70% to 5%, significant inequalities in the distribution of health resources between geographical areas persisted. Additionally, out-of-pocket spending increased, and the proportion of households experiencing catastrophic health expenses did not decline. These mixed outcomes indicate that while coverage expanded, issues related to equitable access and financial protection remained unresolved. In response, the Chinese government continued to refine its policies, seeking a balance between neoliberal market-driven approaches and the need for broader social protection.
United States
Problem Identification: The United States has faced persistent issues with increasing healthcare costs and limited access to healthcare services. Despite being a wealthy nation, a significant portion of the population remains uninsured or underinsured, limiting their ability to access necessary healthcare services. This lack of coverage has led to negative health outcomes, as individuals often forgo care due to cost, resulting in preventable illnesses and more severe health conditions.
Agenda Setting: The U.S. healthcare system has historically been influenced by neoliberal values, emphasizing market efficiency and individual responsibility over collective social responsibility. This ideology has made comprehensive healthcare reform challenging, as powerful stakeholders, including the insurance and pharmaceutical industries, have significant influence in shaping policy. The absence of strong social solidarity movements further complicates efforts to prioritize healthcare as a public good. However, despite these challenges, Barack Obama successfully brought healthcare reform to the forefront of the national agenda during his 2008 presidential campaign, culminating in the passage of the Affordable Care Act. This marked a significant, though contested, shift towards expanding healthcare access within a predominantly market-driven system.
Policy formulation: The Affordable Care Act (ACA) was enacted in 2010. ACA aimed to expand health insurance coverage to millions of Americans. ACA mandated American citizens to have health insurance or pay a penalty. ACA also aimed to improve healthcare outcomes and reduce costs through promoting preventive care and improving healthcare quality.
Policy implementation: The ACA implementation was in the form of a tiered system of health insurance plans. Four main health insurance plans “metal tiers” were offered through the state and federal exchanges: Bronze, Silver, Gold, and Platinum. They differ in the average percentage of total healthcare expenses that the plan will cover.
Policy evaluation: ACA did not increase access to healthcare services. ACA was not based on a single-payer healthcare system, where the government acts as the sole insurer. Instead, ACA expanded health insurance coverage by creating marketplaces (exchanges) where individuals and small businesses can shop for private health insurance plans. Thus, having a tiered system with access that depends on the individual job status and his ability to pay premiums.
Senegal
Problem identification: Senegal experienced social, economic, and political disparities, which resulted in health inequities based on factors such as place of residence, gender, and age.
Agenda setting: Senegal government which represented itself as the protective caretaker of its citizens recognized these disparities and decided to act upon its healthcare system deficiencies. The government was backed up by international organizations mainly the WHO and UNICEF who conducted a meeting in 1987 to increase the availability of essential medicines and to improve drug procurement systems through resale of pharmaceuticals at health centers.
Policy formulation: In the 1990s, the Senegalese government initiated the Bamako Initiative, which encompassed health reforms, including the implementation of a new financing plan.
Policy implementation: the implementation of the health reform had three cornerstones: decentralization where responsibilities including managing health spending and budgeting were transferred to regional and municipal officials. The introduction of minimal user fees for primary care services at government health structures and higher fees for care at secondary and tertiary care were introduced. Community involvement in the health sector was ensured through the establishment of health committees. And “responsibilization” which claims that the healthcare system would be of limited effect on health outcomes as long as citizens do not know how to take care of their health shifting the health responsibility from the state to the individuals.
Policy evaluation: the health reform resulted in increased access to healthcare systems where primary care services were available in rural and urban areas, and generic pharmaceuticals were available for patients in these structures at a wholesale price. Although healthcare services were provided at minimal fees these fees constituted a financial barrier for rural areas citizens causing them to delay healthcare services. Also, primary care services were limited leading to referrals to secondary care units which had higher fees. Community involvement resulted in the creation of a new political arena dominated by senior politically affiliated men leading to the further marginalization of women and children as stakeholders in decision-making. Decentralizing the health system aimed at increasing accountability and responsiveness created problems in money disbursement from central to local levels.
Taiwan
Problem identification: Before fully embracing neoliberal reforms, Taiwan’s National Health Insurance (NHI) system aimed to provide universal healthcare coverage. However, the NHI faced financial challenges, raising concerns about its sustainability and efficiency.
Agenda setting: Unlike many nations, Taiwan was not directly influenced by the World Bank or IMF but was instead shaped by global economic trends and its trade relationship with the United States. The push towards neoliberal reforms was driven by internal aspirations for economic growth, democratization, and the privatization of public sector enterprises. Despite these pressures, there was significant resistance from the public health liberation movement, which prioritized maintaining robust public health services. This resistance helped limit the extent of neoliberal influence on Taiwan’s healthcare system.
Policy formulation: Policies were formulated to promote market openness, fiscal austerity, and privatization, aligning with neoliberal principles.
Policy implementation: The implementation of these neoliberal policies introduced increased market mechanisms in healthcare. However, Taiwan’s National Health Insurance (NHI) system played a crucial role in counteracting potential inequities, focusing on both equity and efficiency.
Policy evaluation: The neoliberal reforms in Taiwan emphasized privatization and market efficiency, which posed challenges to prioritizing public health. Despite these, Taiwan’s commitment to universal coverage and the active efforts of the Public Health Liberation Movement successfully mitigated the negative impacts, ensuring that public health priorities remained above purely capitalist interests.
COMPARATIVE ANALYSIS
To facilitate the comparison among cases, the results of the first step of analysis are summarized in Table 1 where each column (except for the first column) provides a comparison criterion among cases. Starting with problem identification which is mainly the driver behind the adoption of a health reform be it based on a neoliberal ideology or not, all the countries included faced some kind of healthcare system challenge. The common healthcare system challenge among all cases was the presence of one or more of the socioeconomic inequitable access to healthcare services (financial, geographic, gender, etc.) which resulted in disparities in health outcomes. Other healthcare system challenges found in these cases and which are related to access inequity were; the rising cost of healthcare services (USA), the high percentage of uninsured population (USA, China), and the catastrophic health expenditure (China). Moreover, healthcare systems deficits were accompanied by financial challenges in the health sector in Taiwan and reduced governmental expenditure in New Zealand, China and Guyana.
Policy adoption in healthcare reform during the neoliberal era is deeply intertwined with agenda setting, contextual factors, stakeholder influence, and prevailing ideologies. In many cases, policies reflect the vision of the dominant agenda setter, resulting in manifestations of neoliberal ideology such as privatization, market competition, and individual responsibility towards health. During the period from the 1970s onwards, marked by the rise of neoliberal doctrine, countries globally faced economic challenges, notably the stagflation crises of economic stagnation, high inflation, and high unemployment. This crisis was one of the drivers for countries to seek change in their economic approaches from interventionism to a more neoliberal approach. After WWII, western countries went to adopt a more interventionist approach to the economy and the welfare of their countries. Governments were deeply involved in managing demands, stabilizing markets and promoting social welfare in their countries. However, the stagflation crises made governments look for ways out of the crises, and the neoliberal doctrine was on the rise. At the time, many scholars criticized the interventionism approach to be ineffective and recommended the neoliberal approach to face the stagflation. They argued that limited government intervention, free markets and individual freedom would end the crises and lead to economic prosperity.
The United States was the pioneer in adopting the neoliberal doctrine and advocating for it, had already incorporated the neoliberal philosophy into its policymaking approach. So, when the government was faced with challenges in the healthcare sector, the neoliberal and individual responsibility model was already on the agenda as an approach to address whatever challenge rise to the government agenda including the challenges in the healthcare sector. Another neoliberal country was New Zealand. A neoliberal government was elected to power. This government embraced the advice of its treasury and pursued neoliberal approaches to healthcare reform.
Non-neoliberal countries were pushed to adopt neoliberalism through the influence of the US as in the case of Chile or under the pressure of certain international financial organizations mainly the IMF and World Bank such as Ecuador and Colombia. The rest of the cases were more resilient to the neoliberal doctrine. They tried either to balance its effects such as the case of Taiwan or adopted an interventionalist non-neoliberal approach such as Venezuela, Guyana, China and Senegal.
In most cases, the policies adopted mirror the vision of the winner in setting the agenda thus for the USA the ACA essentially created private health insurance schemes allowing the private sector to expand and emphasizing the individual responsibility towards health which are basically neoliberal manifestations. For New Zealand, the corporatization of the healthcare sector, the increased number of private providers and the introduction of secondary healthcare fees were also manifestations of the neoliberal ideology of the neoliberal government elected. Chili’s policies of decreased public spending on health, privatization of healthcare services and the introduction of a private health insurance system and user fees were also the result of the interest of Pinochet in the neoliberal economy and the effect of the Chicago boys who came from the US university. Ecuador’s and Colombia’s policies were similarly a result of an influential stakeholder, the IMF and World Bank. However, Colombia’s policy was through a law (100/93) that emphasized market competition and privatization while Ecuador’s policies were through a national plan (National Plan for Good Living). Taiwan’s policy adopted increased market mechanisms while sticking to universal coverage as a result of both external neoliberal pressure and internal interventionalist pressure. Venezuela, Guyana, Senegal and China’s policies were more affected by their governments’ social interests. Venezuela’s adopted policy was the introduction of a decentralized community-based healthcare system. Guyana’s policy was through the right to free medical attention. Senegal’s adopted policy was through the Bamako initiative and the new financing plan and finally, China’s adopted policy was through a governmental decision to expand health insurance coverage.
Table 1 Intercountry Comparative Health Reform Policy Analysis
| Country | Problem identification | Agenda setting | Policy adoption | Policy implementation | Policy evaluation |
|---|---|---|---|---|---|
| Chile | Inefficiencies in the healthcare system: inequities in access and quality of care, and rising healthcare costs. Economic challenges: high inflation, low growth rates, and fiscal deficits. | Discussion of economic reform with economists from Chicago University who called for a neoliberal reform. | Adoption of a neoliberal-influenced reform to increase efficiency, competition, and consumer choice in healthcare provision. | Decreased public spending on health. Privatization of healthcare services. Introduction of a private health insurance system and user fees. A tiered healthcare system with user fees. Low-quality public sector vs. higher quality private healthcare sector. Socioeconomic inequality in access to services according to wealth, gender and place of residence. | |
| Ecuador | Fragmented healthcare system. Financial barriers- high out-of-pocket payments. Inequitable access to services. Economic crises, high inflation, unsustainable levels of public debt, currency devaluation, and stagnant growth. | Pressure by the IMF for privatization, trade liberalization and austerity. | National Plan for Good Living including healthcare reform with a concentration on the social determinants of health, equity and inclusion. | Increase in the budget for the MoH, investment in infrastructure, equipment and human resources for health and extension of the social protection scheme. | Fragmentation persists and It appeared far-fetched that an effective taxation system will ever be implemented. |
| Colombia | Inequity in accessibility and quality, were the main problems in the healthcare system. | The IMF and the World Bank pushed for the adoption of a neoliberal reform. | Law 100/93 was introduced emphasizing market competition and privatization in Colombia’s healthcare to improve efficiency and expand access. | Increased number of private health providers. Increased workload on health professionals. | Dehumanized and fragmented healthcare system. Unequal access to healthcare services. |
| Venezuela | Inequitable access to healthcare services, poor health outcomes, and a lack of resources. | A reform model that emphasized social justice, equity, and universal access to healthcare was advocated for by President Hugo Chávez. | A decentralized community-based healthcare system was introduced. Prioritized preventative healthcare. | Access to healthcare services was increased. Health outcomes ameliorated. | |
| Guyana | Limited resources for the healthcare system resulting in limited access to healthcare services, inadequate infrastructure, and disparities in health outcomes. | Socialist government pushed towards investing in public health. | The new Republican constitution encompassed “the right to free medical attention” which emphasized the provision of free healthcare. | The government could not provide full coverage and called for self-help through preventative care and the use of local resources. | Overloaded health workforce. Frozen salaries. Self-help through preventative care and the use of local resources. |
| New Zealand | Inequitable access to healthcare services. Decreased public spending on health. | Legislation changed to protect the rights of minorities. | A neoliberal government was elected. Treasury advice to adopt a market-driven approach. | The Green and White paper and the Youth Health and Public Health paper were produced. Both embraced corporatization as a solution for the healthcare system challenges. | Increased number of private providers. Introduction of secondary care charges. Increased inequalities. |
| China | High percentage of uninsured population. Geographical health inequities. Insufficient government spending on health. Catastrophic health expenditure. | 2003 SARS outbreak. Increased social discontent. | Expansion of several urban and rural government-administered health insurance programs. | Expansion of insurance coverage. Reform of public hospitals. Reform of PHC system. | Reduced geographical inequities. Increased out-of-pocket expenditure. |
| United States | Increased healthcare costs. Large percentage of the uninsured population. Limited access to healthcare service. | Neoliberal model and individual responsibility. | Presidential campaign for health reform. | Affordable Care Act (ACA) was enacted. A tiered system of health insurance plans. | Inequitable access to healthcare system. Access depended on individual’s ability to pay premiums. |
| Senegal | Place of residence, gender and age-based health inequities. | The government wanted to address these disparities. | Bamako Initiative; health reform with a new financing plan. | Decentralization to regional and municipal levels. Minimal user fees for primary care services at government health structures and higher fees for care at secondary and tertiary levels were introduced. Establishment of health committees. | Increased access to PHCs and generic pharmaceuticals. Financial barriers remained due to high user fees in secondary care. Marginalization of women in decision-making. Central to peripheral money transfer problems. |
| Taiwan | Financial challenges pressure to adopt neoliberal reforms. | Market openness, fiscal austerity and privatization policies. | Increased market mechanisms in healthcare. | The negative effects of the neoliberal reforms were balanced by the commitment to universal coverage and the collective efforts. |
Discussion
This study concentrated on the effect of neoliberalism on healthcare systems and health equity. Neoliberalism has been a dominant doctrine shaping economic and social policies in many countries since the 1980s. This ideology aims to foster economic growth and improve GDP by promoting free markets, encouraging private sector growth, and limiting government spending. However, it often neglects critical social dimensions, such as social welfare, safety nets, healthcare accessibility, and equity. The long-term impact of these neoliberal policies has significantly influenced health outcomes and healthcare systems globally, particularly during crises like the COVID-19 pandemic.
Countries’ capacities and strategies for managing the COVID-19 pandemic varied widely, reflecting the influence of neoliberal policies over time. Scholars have even referred to COVID-19 as a “neoliberal disease,” highlighting how these policies have shaped healthcare systems’ preparedness and response. The ability of countries to respond effectively to health crises is often linked to their healthcare systems’ structure, funding, and accessibility, which are, in turn, shaped by the adoption of neoliberal or more interventionist approaches.
Countries that adopt neoliberal approaches tend to depend on the private sector for service delivery, limit expenditure on health and shy away from UHC resulting in persistent healthcare challenges and pronounced health inequities leading to challenges in managing health emergencies. In our study, neoliberal countries (i.e., the USA, Chile, Ecuador, Colombia, and New Zealand) had these challenges and exhibited inadequate responses during the COVID-19 pandemic.
The USA healthcare system has its own strengths such as having well-trained workforce and high-quality medical specialists. Nonetheless, it is frequently criticized for inadequate healthcare coverage leaving citizens without protection with high health cost resulting in poor health outcomes and increased health inequities. Apparently, these US healthcare systems deficiencies attributed to the US response to the pandemic and its outcomes. USA response to COVID-19 and the resultant COVID-19 morbidity and mortality were severe compared to other countries. In 2021, US COVID-19 attributable cumulative mortality was 15% of that of the global total. COVID-19 has also highlighted the inequalities in the US healthcare system. These inequalities have their roots in neoliberalism. The neoliberal governance of the healthcare system concentrated on market-based policies leading to these inequities. The neoliberal US healthcare system failed to concentrate on public health and prioritized corporate profit resulting in poor preparedness for the pandemic and protection of the health workforce. Scholars indicated the need for government intervention and adequate social services to overcome these widened inequities.
New Zealand’s case is somewhat different. Although neoliberal principles, such as privatization and deregulation affected the healthcare system in New Zealand and resulted in social inequalities, the government of New Zealand responded to the pandemic with great acclaim, enacting a “go hard, go early” policy and offering assistance to both individuals and businesses which helped in mitigating the effects of neoliberal policies.
The other three countries in this category: Chile, Ecuador and Colombia response to COVID-19 did not have better outcomes. According to our Worldmeter data on COVID-19, the percentage of death cases in these countries was relatively high especially in Chile where the percentage of death cases can be compared to that of the US. Chile’s neoliberal policies resulted in social inequities that have been made worse by the COVID-19, especially in the capital, where lower-class communities have seen greater rates of infection and mortality as a result of comorbidities and restricted access to healthcare. Ecuador’s response to COVID-19 was also marked by high inequalities, where the government prioritized the private sector leading to the exacerbation of existing inequalities that are rooted in neoliberalism. COVID-19 had similarly exposed and exacerbated health inequalities in Colombia, a consequence of neoliberal policies. The neoliberal governance model in Colombia which is characterized by decreased governmental expenditure on social services was a main obstacle for the implementation of Universal Health coverage which led to health inequities in access to healthcare services. In Colombia, health inequity was observed in the lower socioeconomic groups and indigenous people through greater rates of COVID-19 mortality. The epidemic has caused an additional 3.5 million people to live in poverty, making the residents of lower-income neighborhoods to have a ten-fold higher risk of hospitalization or COVID-19-related death than residents of wealthy neighborhoods.
Table 2: COVID-19 mortality
| Country | Population | Deaths | %D |
|---|---|---|---|
| US | 334805269 | 1219487 | 0.364237697 |
| New Zealand | 4898203 | 5697 | 0.11630796 |
| Chile | 19250195 | 64497 | 0.335045957 |
| Colombia | 51512762 | 143200 | 0.277989365 |
| Ecuador | 18113361 | 36043 | 0.19898571 |
| Venezuela | 29266991 | 5856 | 0.02000889 |
| Senegal | 17653671 | 1971 | 0.011164817 |
| Guyana | 794045 | 1300 | 0.163718681 |
| China | 1448471400 | 5272 | 0.00036397 |
| Taiwan | 23888595 | 19005 | 0.079556793 |
On the other hand, there are the more interventionalist countries, including China, Guyana, Senegal, and Venezuela. During COVID-19, although their responses varied, some were praised while others were criticized. China, although, was criticized for implementing strict control measures such as complete lockdowns, which were considered unsuitable for other nations was praised for its socialist economic and political system which prioritized saving millions of lives over protecting economic growth. And responded to the COVID-19 pandemic by putting in place a robust social safety net that combined welfare, support, and social insurance.
Guyana had originally planned to take an interventionist stance, but it finally gave in to external pressure to cut back on government health spending. Major disparity in access and insufficient healthcare coverage were the outcomes of this choice. These flaws were exposed during the COVID-19 pandemic, which made it necessary for foreign agencies like the World Bank, GAVI, and the Pan American Health Organisation (PAHO) to provide support in order to obtain necessary COVID-19 medical supplies and rectify uneven access to healthcare.
In Senegal, the government pursued a multi-sectoral approach to managing the pandemic while maintaining healthcare services. The Ministry of Health collaborated with the private sector to enhance access to testing services, including establishing partnerships for manufacturing COVID-19 rapid diagnostic tests, which were crucial for timely detection and patient isolation. However, underlying socio-economic factors continued to significantly impact Senegal’s healthcare system, leading to unequal health outcomes among certain communities during COVID-19 due to limited access to healthcare services.
Venezuela’s already fragile healthcare system has been made even more vulnerable by the COVID-19 outbreak and socioeconomic unrest. Medicine is being practiced in a precarious manner due to healthcare workers leaving the industry due to unfavorable working conditions, low pay, as well as shortages of supplies, equipment, and necessities like water and electricity. These problems are exacerbated by the pandemic, highlighting the country’s struggle to provide adequate healthcare services amid ongoing crises.
Conclusion
In conclusion, the influence of neoliberalism on healthcare systems is profound, often deepening existing disparities in access and outcomes. Countries embracing neoliberal policies typically face heightened healthcare challenges and inequities due to their emphasis on market-driven solutions and limited expenditure. While interventionist countries like China and Taiwan demonstrate more effective crisis management through their prioritization of universal healthcare, economic instability, as observed in Venezuela, can hinder such efforts. To mitigate neoliberalism’s adverse impact on health, healthcare must be treated as a common good, necessitating robust governmental intervention and regulation to ensure equitable access and address negative externalities. While neoliberalism has long-term effects and is a significant factor, it’s essential to recognize that countries’ responses to health crises like COVID-19 are multifaceted, influenced by factors beyond neoliberal ideology alone, including strong leadership, prior experience, and economic resources. Therefore, a comprehensive understanding of healthcare systems must consider a diverse range of influences, recognizing both the role of neoliberalism and the broader contextual factors at play.
Conflicts of Interest
The authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Acknowledgement
We would like to express our gratitude to Dr. Amr Adly for his valuable comments and insightful feedback, which greatly enriched this work. We also acknowledge the support of the ‘Pathways from Neoliberalism: Voices from the Middle East and North Africa’ project, which provided a fellowship that supported this research.
References
- Haldane V, De Foo C, Abdalla SM, et al. Health systems resilience in managing the COVID-19 pandemic: lessons from 28 countries. Nat Med. 2021;27(6):964-980.
- Almeida A. The trade-off between health system resiliency and efficiency: evidence from COVID-19 in European regions. Eur J Health Econ. 2024;25(1):31-47. doi:10.1007/s10198-023-01567-w
- Maani N, Galea S. COVID-19 and underinvestment in the public health infrastructure of the United States. Milbank Q. 2020;98(2):250.
- David Williams O, Yung KC, Grépin KA. The failure of private health services: COVID-19 induced crises in low- and middle-income country (LMIC) health systems. Glob Public Health. 2021;16(8-9):1320-1333. doi:10.1080/17441692.2021.1874470
- Vallier K. Neoliberalism. Published online 2021. Accessed March 30, 2024. https://plato.stanford.edu/entries/neoliberalism/?ref=amonle.com
- Evans P, Sewell WH. The neoliberal era: Ideology, policy, and social effects. Soc Resil Neoliberal Era. Published online 2013:35-68.
- McGregor S. Neoliberalism and health care. Int J Consum Stud. 2001;25(2):82-89.
- Lasswell HD. The political science of science: An inquiry into the possible reconciliation of mastery and freedom. Am Polit Sci Rev. 1956;50(4):961-979.
- Brewer GD, DeLeon P. The Foundations of Policy Analysis. Brooks/Cole Publishing Company; 1983. https://books.google.com.eg/books?id=Vq7uAAAA MAAJ
- Adelle C, Jordan A, Turnpenny J. Policy making. In: Environmental Policy in the EU. Routledge; 2012:235-252. Accessed April 2, 2024. https://www.taylorfrancis.com/chapters/edit/10.4324/9780203109823-25/policy-making-camilla-adelle-andrew-jordan-john-turnpenny
- Collier D. The comparative method. Polit Sci State Discip II Ada W Finifter Ed Am Polit Sci Assoc. Published online 1993. Accessed April 14, 2024. https://papers.ssrn.com/sol3/papers.cfm?abstract_id=1540884
- Stafford A. Comparative analysis within political science. E-Int Relat. 2013;1(4).
- Levy FD. Chile: an economy in transition. World Bank Ctry Study USA. Published online 1983.
- Gideon J. Counting the cost of privatised provision: Women, rights and neoliberal health reforms in Chile. IDS Bull. 2008;39(6):75-82. doi:10.1111/j.1759-5436.2008.tb00514.x
- Rotarou ES, Sakellariou D. Neoliberal reforms in health systems and the construction of long-lasting inequalities in health care: A case study from Chile. Health Policy. 2017;121(5):495-503.
- Taylor M. The reformulation of social policy in Chile, 1973-2001: Questioning a neoliberal model. Glob Soc Policy. 2003;3(1):21-44. doi:10.1177/1468018103003001009
- Tsai TC, Jl J. Neoliberalism and its discontents: Impact of health reforms in Chile. Harv Int Rev. 2009;31(2):32-36.
- López-Cevallos DF, Chi C. Health care utilization in Ecuador: a multilevel analysis of socio-economic determinants and inequality issues. Health Policy Plan. 2010;25(3):209-218.
- De Paepe P, Tapia RE, Santacruz EA, Unger JP. Ecuador’s silent health reform. Int J Health Serv. 2012;42(2):219-233. doi:10.2190/HS.42.2.e
- Friederic K, Burke BJ. La Revolución Ciudadana and social medicine: Undermining community in the state provision of health care in Ecuador. Glob Public Health. 2019;14(6-7):884-898. doi:10.1080/17441692.2018.1481219
- Mahmood Q, Muntaner C. Theoretical underpinnings of state institutionalisation of inclusion and struggles in collective health in Latin America. Glob Public Health. 2019;14(6-7):863-874. doi:10.1080/17441692.2018.1455886
- Muntaner C, Salazar RMG, Rueda S, Armada F. Challenging the neoliberal trend: The Venezuelan health care reform alternative. Can J Public Health. 2006;97(6):1-19.
- Misir P. Health care in guyana. Soc Med. 2015;9(1):36-47.
- Seoane‐Vazquez E, Rodriguez‐Monguio R. Access to essential drugs in Guyana: a public health challenge. Int J Health Plann Manage. 2010;25(1):2-16. doi:10.1002/hpm.949
- Walker A. Narrating health and scarcity: Guyanese healthcare workers, development reformers, and sacrifice as solution from socialist to neoliberal governance. Soc Sci Med. 2017;187:225-232.
- Barnett R, Barnett P. Back to the Future? Reflections on past reforms and future prospects for health services in New Zealand. GeoJournal. 2004;59(2):137-147. doi:10.1023/B:GEJO.0000019972.22425.8d
- Brown H, Bryder L. Universal healthcare for all? Māori health inequalities in Aotearoa New Zealand, 1975–2000. Soc Sci Med. 2023;319. doi:10.1016/j.socscimed.2022.115315
- Zhang W, Navarro V. Why hasn’t China’s high-profile health reform (2003-2012) delivered? An analysis of its neoliberal roots. Crit Soc Policy. 2014;34(2):175-198. doi:10.1177/0261018313514805
- Duckett J, Langer AI. Populism versus Neoliberalism: Diversity and Ideology in the Chinese Media’s Narratives of Health Care Reform. Mod China. 2013;39(6):653-680. doi:10.1177/0097700413492602
- Epperson B. Challenging narratives to neoliberalism in media representations of American health reform: Lessons from the United States. In: Neoliberal Contentions: Diagnosing the Present. ; 2022:133-155.
- Waitzkin H, Hellander I. The History and Future of Neoliberal Health Reform: Obamacare and Its Predecessors. Int J Health Serv. 2016;46(4):747-766. doi:10.1177/0020731416661645
- Foley EE. The anti-politics of health reform: Household power relations and child health in rural Senegal. Anthropol Med. 2009;16(1):61-71. doi:10.1080/13648470802426243