





Impact of PDE-5 Inhibitors on Rat Hearing: A Study
The Effect of Phosphodiesterase Type 5 Inhibitors on the Hearing of Rats
Gürcan Sünnetci MD¹, Güven Yıldırım MD², Ziya Saltürk MD³, Tolgar Lütfi Kumral MD¹, Yavuz Uyar MD¹
- Otorhinolaryngology Specialist, Private Practice, İstanbul, Türkiye
- Okan University, Medical Faculty, Department of Otorhinolaryngology, Istanbul, Türkiye
- University of Health Sciences, Prof. Dr. Cemil Taşcıoğlu Hospital, Department of Otorhinolaryngology, Istanbul, Türkiye
OPEN ACCESS
PUBLISHED: 31 May 2026
CITATION: Sünnetci, G., et al., 2026. The Effect of Phosphodiesterase Type 5 Inhibitors on the Hearing of Rats. Medical Research Archives, [online] 14(5).
COPYRIGHT: © 2026 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
ISSN 2375-1924
Abstract
There have been reports of sudden hearing loss under treatment for erectile dysfunction with phosphodiesterase type-5 inhibitors. This study investigated the possible damaging effect on the cochleae in rats using the otoacoustic emission method. Wistar albino rats were divided into four groups. Each group received Sildenafil, Vardenafil, Tadalafil, or saline orally for 28 days. Distortion product otoacoustic emission measurements were conducted at the beginning of the study and on the 14th and 28th days (stimulation 65/55 decibels). Paraffin block serial sections of the mid-modiolar area (up to 5 µm thick) were prepared, stained with hematoxylin and eosin, and evaluated using light microscopy. A statistically significant decrease in the distortion product was observed in group 1 (sildenafil) on day 28 at stimulus intensities of 65/55 dB (p < 0.05). Conversely, a statistically significant increase was detected in group 3 (tadalafil). No statistically significant change was noted in group 2 (vardenafil). When comparing the three groups, we found no statistically significant difference in the number of outer ciliated cells. Differences in stria vascularis and spiral ganglion were statistically insignificant among the three groups (p>0.05). Sildenafil has an ototoxic effect on cochleae. This effect was not observed in the tadalafil and vardenafil groups. This study also revealed that the ototoxic side effect of sildenafil was dependent on exposure time.
Keywords:
Otoacoustic Emissions, Spontaneous, Hearing Loss, Sudden, Phosphodiesterase Type 5 Inhibitors
Introduction
Phosphodiesterase type 5 (PDE-5) inhibitors sildenafil, vardenafil, and tadalafil are widely prescribed oral medications for treating erectile dysfunction. These drugs are well-tolerated, but the most common side effects reported include headache, flushing, abnormal vision, and nasal obstruction. Although reliable data is currently lacking, reports of sudden hearing loss associated with PDE-5 inhibitors exist. The US Food and Drug Administration (FDA) has documented 29 reports of sudden hearing loss potentially related to PDE-5 inhibitor use. While the precise causal relationship between PDE5 inhibitors and sensorineural hearing loss remains to be established, existing epidemiological data and case reports suggest a potential negative impact on auditory function. For instance, a case study detailed bilateral profound sensorineural hearing loss in a 44-year-old male following a two-week regimen of sildenafil. The hearing loss is sensorineural and may be accompanied by dizziness, tinnitus, or nausea. Most hearing losses were unilateral (88-96%) and occurred within 24 hours of the intake of PDE-5 inhibitors (66.7-88%). After discontinuing the medication, it was partially reversible in some patients. However, some individuals experience permanent profound sensorineural hearing loss despite treatment with corticosteroids. This underscores the critical need for further investigation into the ototoxic mechanisms of PDE5 inhibitors, especially given their widespread clinical application for conditions beyond erectile dysfunction, including pulmonary hypertension and benign prostatic hyperplasia.
PDE-5 inhibitors inhibit the enzymes that degrade cyclic guanosine monophosphate (cGMP), thereby increasing cGMP levels. Alterations in the nitric oxide pathway, including cGMP and downstream second messenger molecules, have been previously linked to cochlear pathophysiology in conditions such as aminoglycoside ototoxicity. The increase in cGMP augments the effect of nitric oxide, leading to increased smooth muscle relaxation and penile erection. However, this mechanism also contributes to the systemic vasodilatory effects, which may alter cochlear blood flow and oxygenation, potentially inducing cellular stress within the inner ear. This vascular alteration, combined with the presence of PDE5 in inner ear structures, suggests a plausible pathway through which these inhibitors could mediate auditory dysfunction. Numerous case reports and observational studies have documented the occurrence of sudden sensorineural hearing loss temporally associated with PDE5 inhibitor use, further highlighting this potential adverse effect.
While the FDA has noted missing data in patient records, such as medical history and conclusive cause of death, precluding a direct causal link, a growing body of evidence, including experimental studies in rats and cohort studies in humans, points to a higher incidence of hearing loss among PDE-5 inhibitor users. Few studies have examined the effects of PDE-5 inhibitors on the cochlea to date. In this study, we investigated the potential effects of the currently prevalent PDE-5 inhibitors on the cochlea using otoacoustic emissions (OAEs) and pathological examination. Given the established presence of PDE-5 in inner ear structures, understanding the specific molecular mechanisms by which PDE-5 inhibitors modulate cochlear homeostasis is crucial for elucidating their ototoxic potential.
Material and Methods
This study was conducted at the Istanbul University Experimental Medicine Research Institute, with approval number 2012-133 from the local animal studies ethical committee. International standards for animal care and handling were followed during the experiments.
Healthy adult Wistar Albino rats weighing between 261 and 386 g were used in the study. They were housed in temperature-controlled rooms with 12-hour light/dark cycles. The animals had free access to food and water. The rats were intraperitoneally anesthetized with 30 mg/kg of ketamine hydrochloride and 4 mg/kg of xylazine before sacrifice. All rats were examined otoscopically before inclusion in the study; those with outer cerumen, acute otitis, or adhesive otitis media were excluded. Also, rats lacking pre-study distortion product otoacoustic emissions (DPOAE) were excluded.
The rats in the study were divided into four groups. Group 1 (n=8) received 1 mg/kg/day of oral sildenafil citrate (Viagra; Pfizer, Istanbul, Turkey) dissolved in 1 cc of normal saline for 28 days. Group 2 (n=8) received 0.5 mg/kg/day of oral vardenafil monohydrochloride trihydrate (Levitra; Istanbul, Turkey), dissolved in saline, for 28 days. Group 3 (n=8) received 2.5 mg/kg/day of oral tadalafil (Cialis; Lilly, Istanbul, Turkey) dissolved in 1 cc of normal saline for 28 days. Group 4 (n=8) received 1 cc of oral normal saline for 28 days. The doses given to the animals were calculated based on human therapeutic doses.
The DPOAE measurements were performed on all rats on days 0, 14, and 28. Otomicroscopic examination of the rats was performed before DPOAE recordings. Animals with middle ear pathology that may impair DPOAE recordings were excluded from the study. The DPOAE recordings were made using the smallest probe (Otodynamics Ltd, London, United Kingdom). The DPOAEs were measured as a function of sound pressure level using stimuli with constant intensity and frequency. The frequencies (f1 and f2) were adjusted to the f2:f1 ratio of 1.22 and stimulus intensity levels of 65/55 dB. Distortion product measurements were performed, recorded, and traced at 4004, 4358, 4761, 5188, 5652, 6165, 6726, 7336, and 7996 Hz.
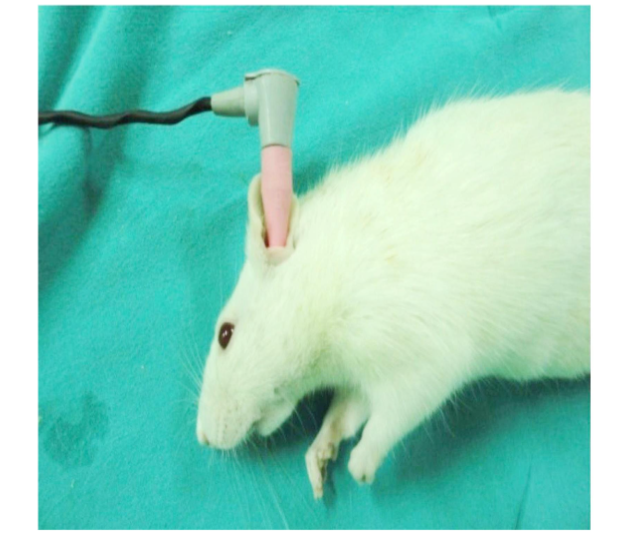
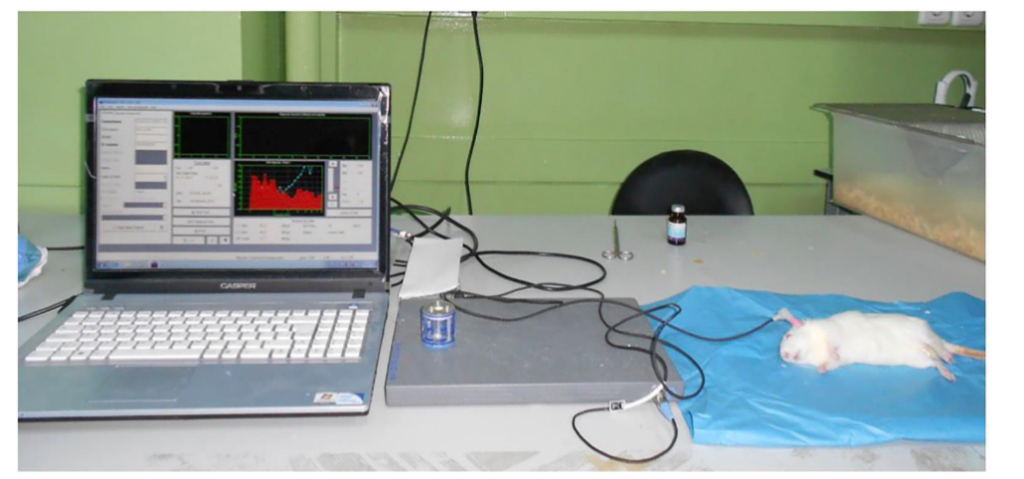
Figure 2: Otoacoustic Emission Recording Setup in the Rat Model
Animals were sacrificed on day 28 by decapitation while under anesthesia (ketamine/xylazine, as described above). The temporal bones were carefully dissected out. Under the dissecting microscope (S1, 300 mm lens; Carl Zeiss, Oberkochen, Germany), the bony capsule of the cochlea was carefully removed, and the lateral wall was removed to reveal the organ of Corti. The corresponding groups of the samples were unknown to the pathologist. Samples were fixed with 10% buffered formaldehyde for 3 days, and decalcification was performed using 10% ethylenediaminetetraacetic acid disodium salt (pH 7.4). After 3 hours, running tap water was used to wash away the decalcification solution, and the tissue was fixed in formaldehyde for 2 more days. An automated tissue tracking device was used for routine processing. Paraffin block serial sections of the modiolar area (up to 5 µm thick) were prepared, stained with hematoxylin and eosin, and evaluated using light microscopy by a pathologist blinded to the treatment groups.
The organ of Corti, stria vascularis, and spiral ganglion were visualized by light microscopy (Olympus CX 31) at 400x magnification and photographed using an Olympus digital camera. Four-point scoring systems were developed to grade injury to the organ of Corti, stria vascularis, and spiral ganglion. Injury to the outer ciliated cells was graded using a four-point scoring system. A score of zero indicates the presence of three rows of outer ciliated cells with intact nuclei, and one, two, and three indicate cochleae with injury to one, two, or three rows of outer ciliated cells, respectively. A four-point scoring system was used to grade stria vascularis injury, with a score of 0 indicating no shrinkage of the intermediate cells and scores of 1, 2, and 3 indicating slight, moderate, and severe shrinkage, respectively. Spiral ganglion cells, vacuolization, and nuclear degeneration were also subjectively evaluated and categorized based on the severity of the changes (i.e., no change, 0; mild, 1; moderate, 2; and severe changes, 3).
NCSS (Number Cruncher Statistical System) 2007 and PASS (Power Analysis and Sample Size) 2008 Statistical Software (Utah, USA) programs were used for statistical analysis. When the study data were evaluated, descriptive statistics (mean, standard deviation) were calculated, and the Kruskal-Wallis test was employed for intergroup comparisons of data that were not normally distributed. The Mann-Whitney U test was used to assess differences between groups. The Wilcoxon Signed Ranks test was utilized for intra-group comparisons of data that were not normally distributed. Results were evaluated at a 95% confidence interval, with a significance level set at p < 0.05. Histopathological evaluation included assessment of cellular degeneration, apoptosis, and cytoplasmic vacuolization in various cochlear structures.
Results
The experimental rats tolerated the oral medication well, with no weight loss or extreme weight gain. Additionally, there was no change in food and water consumption. The mean hearing thresholds for 65/55 dB stimuli showed no significant difference between the groups on days 0 and 14 (p=0.228; p=0.075). However, a substantial difference in mean frequencies was observed between the groups on day 28 (p=0.003).
As determined by the Mann-Whitney U Test, which was used to identify differences between groups, the mean hearing thresholds of group 1 were significantly lower than those of groups 2, 3, and 4 (p=0.010; p=0.002; p=0.010). Group 1 showed no statistically significant change in the day 14 measurements compared to day 0 (p>0.05), but it did show significant decreases in the day 28 measurements compared to day 0 (p<0.05). Group 2 exhibited no statistically significant change in the day 14 and 28 measurements compared to day 0 (p>0.05; p>0.05). Group 3 showed no statistically significant change in the day 14 measurements (p>0.05), but significant increases were noted on day 28 compared to day 0 (p<0.05). Group 4 revealed no statistically significant change in the day 14 and 28 average frequency measurements at 65/55 dB compared to day 0 (p>0.05; p>0.05).
There was no statistically significant difference in the number of outer ciliated cells between the three groups. Changes in stria vascularis and spiral ganglion were also statistically insignificant among the groups (p>0.05).
| Group 1: Sildenafil | Group 2: Vardenafil | Group 3: Tadalafil | Group 4: Saline | + 65/55 dB Mean Frequency, Hz | p |
|---|---|---|---|---|---|
| Day 0 16.23±8,04 (17.00) | 23.14±9.61 (27.56) | 22.31±8.88 (23.16) | 20.02±7.38 (21.26) | 0.228 | |
| Day 14 12.74±7.16 (12.48) | 20.45±11.83 (22.15) | 22.81±8.36 (26.45) | 20.54±6.83 (21.53) | 0.075 | |
| Day 28 10.87±8.27 (8.74) | 22.65±7.24 (26.4) | 27.0±5.71 (28.79) | 21.1±6.98 (18.93) | 0.003** | |
| ++Day 0-14 0.093 | 1.000 | 1.000 | 0.327 | ||
| ++Day 0-28 0.050* | 0.484 | 0.050* | 0.484 |
There was no significant difference between the groups at days 0 and 14 (p=0.228; p=0.075). However, there was a significant difference between the groups in the mean frequencies at the 28 (p=0.003).
| 65/55 dB Mean Frequencies Day 28 | P |
|---|---|
| Group 1 Group 2 | 0.010* |
| Group 1 Group 3 | 0.002** |
| Group 1 Group 4 | 0.010* |
| Group 2 Group 3 | 0.105 |
| Group 2 Group 4 | 0.959 |
| Group 3 Group 4 | 0.130 |
| Groups | n | Mean±SD | P |
|---|---|---|---|
| Outer Ciliated cells | 1: Sildenafil | 8 1.00±0.54 | 0.103 |
| 2: Vardenafil | 8 0.50±0.54 | ||
| 3: Tadalafil | 8 0.38±0.52 | ||
| 4: Saline | 8 0.38±0.42 | ||
| Stria vascularis | 1: Sildenafil | 8 0.75±0.87 | 0.580 |
| 2: Vardenafil | 8 0.50±0.54 | ||
| 3: Tadalafil | 8 0.38±0.52 | ||
| 4: Saline | 8 0.25±0.46 | ||
| Spiral ganglion | 1: Sildenafil | 8 0.5000±0.76 | 0.866 |
| 2: Vardenafil | 8 0.25±0.46 | ||
| 3: Tadalafil | 8 0.25±0.46 | ||
| 4: Saline | 8 0.38±0.52 |
Kruskal Wallis Test p>0.05
There was no statistically significant difference in the numbers of outer ciliated cells, changes in the stria vascularis, or changes in spiral ganglia between the three groups.
Discussion
The present investigation aimed to determine the potential ototoxic effects of vardenafil and tadalafil administered orally, focusing on their impact on DPOAE responses and cochlear histopathology. This study specifically explored whether phosphodiesterase-5 inhibitors induce ototoxicity, a concern raised by reports of sudden hearing loss and subsequent regulatory announcements. The findings of the current study indicate no statistically significant changes in DPOAE measurements or cochlear histopathology following administration of vardenafil and tadalafil, suggesting a limited ototoxic effect at the tested dosages. This outcome contrasts with some clinical observations in which PDE5 inhibitors, including sildenafil, vardenafil, and tadalafil, have been associated with hearing impairment, particularly sudden sensorineural hearing loss.
However, previous research has indicated that sildenafil may induce cochlear bleeding, which could result in sensorineural hearing loss, although this is posited to be secondary to physical exertion rather than a direct ototoxic pharmacological effect. Sudden hearing loss is defined as a greater than 30 dB reduction in hearing, over at least three consecutive frequencies, occurring within a period of 72 hours or less. Studies have shown that OAE has a high predictive value in diagnosing sudden hearing loss and can be used for differential diagnosis and follow-up of this condition. In the context of ototoxicity research, evaluating cochlear structural integrity is paramount, as demonstrated by studies analyzing degeneration in spiral ganglion cells, stria vascularis, and spiral ligament.
The most common side effects of PDE-5 inhibitors include headaches, dyspepsia, flushing, nasal congestion, dizziness, visual problems, and back and muscle pains. Currently, there have been case reports of sudden hearing loss associated with these medications used for erectile dysfunction. The source of otoacoustic emissions is the outer hair cells. Damage to these cells due to ototoxic drugs, hypoxia, and acoustic trauma inhibits the production of otoacoustic emissions. A drug that causes cochlear damage can be immediately detected with OAE. In our study, we used DPOAE to assess the effects of sildenafil, vardenafil, and tadalafil on the inner ear and hearing, evaluating cochlear damage.
The pathophysiology of sudden hearing loss due to PDE-5 inhibitors remains unclear. However, PDE-5 inhibitors block the degradation of cGMP. By doing so, they induce gene expression via transcription factors by phosphorylating proteins with specific kinases. These processes have been associated with damage to cochlear hair cells due to increased nitric oxide levels. It has also been hypothesized that PDE-5 inhibitors might cause hearing loss by affecting nasal physiological characteristics and, thus, Eustachian tube function. Recently, sensorineural hearing loss has been reported in association with these drugs. However, the published case reports of sudden sensorineural hearing loss attributed to PDE-5 inhibitors may simply reflect the natural incidence of this condition rather than an increased risk posed by these medications. Although our study supported the ototoxic effect of sildenafil. In a population-based study, patients aged 40 years or older with self-reported hearing impairment were more than twice as likely to report taking PDE-5 inhibitors compared with those without hearing loss. It has also been reported that this relationship was limited to sildenafil intake and was not encountered with other PDE-5 inhibitors. These findings are compatible with ours.
Most cases of hearing loss have been reported in the early stages of drug usage. They performed audiometric tests on 18 patients before vardenafil and 1, 5, and 72 hours after drug ingestion. They detected decreases consistent with reversible ototoxicity in four patients. Khan et al. identified 47 cases of sudden hearing loss attributable to PDE-5 inhibitor use. 66.7% of cases developed within 24 hours of PDE-5 inhibitor intake, and over 50% were due to sildenafil. Our study, in contrast to previous studies, evaluated both short- and long-term hearing loss. We observed ototoxicity after day 14 and only in the sildenafil group. The data in this study do not support the previously described early hearing loss. This discrepancy underscores the necessity for comprehensive, long-term studies to ascertain the chronic effects of PDE5 inhibitors on auditory function.
Rats were given high doses of sildenafil for 105 days, and their hearing was evaluated. As in our study, they found decreases in OAE values. However, they did not compare the measurements with other PDE-5 inhibitors. The present study revealed a higher ototoxic effect of sildenafil than vardenafil and tadalafil. These PDE-5 inhibitor drugs have the same therapeutic efficacy and side effects, except for tadalafil, which has a longer onset of action and a longer therapeutic half-life. Our study revealed a significant improvement in hearing levels at day 28 compared with day 0 in the tadalafil group. No significant effect of tadalafil on auditory function was observed, except for an isolated increase in hearing thresholds in a few patients. They hypothesized that long-term sildenafil use causes hearing loss in rats via increased apoptosis. Histological findings showed cochlear apoptosis in the examined rats. Light microscopy of modiolar longitudinal sections allows observation of changes in cilia and identification of alterations in the stria vascularis and the spiral ganglion. According to our results, there was a decrease in the number of outer ciliated cells in the sildenafil group. However, there was no statistically significant difference in the number of outer ciliated cells among the three groups. The tadalafil group showed physiological effects similar to those in the normal saline group. This suggests that sildenafil may have an ototoxic effect. Changes in the spiral ganglion and stria vascularis were not significant.
Sildenafil has an ototoxic effect on the cochlea, which was not observed in the tadalafil and vardenafil groups. This study also revealed that the ototoxic side effect of sildenafil was time-related. It is possible that when PDE-5 inhibitors are used intermittently, the risk for ototoxicity is much lower than during continuous therapy.
Conclusion
This study, therefore, concludes that while sildenafil demonstrates a discernible ototoxic potential, particularly with prolonged administration, tadalafil and vardenafil do not exhibit comparable effects. This differential ototoxicity among PDE-5 inhibitors warrants further investigation into their molecular mechanisms, particularly their differential effects on cochlear physiology and cellular viability. Future research should focus on elucidating the specific biochemical pathways and genetic predispositions that contribute to sildenafil-induced ototoxicity, while also exploring potential protective mechanisms or interventions.
Acknowledgment:
This manuscript is based on the postgraduate thesis conducted by Gürcan Sünnetçi.
References:
- Maddox PT, Saunders JE, Chandrasekhar SS. Sudden hearing loss from PDE-5 inhibitors: a possible cellular stress etiology. Laryngoscope. 2009;119(8):1586. doi:10.1002/lary.20511
- Barreto MASC, Bahmad F. Phosphodiesterase type 5 inhibitors and sudden sensorineural hearing loss. Braz J Otorhinolaryngol. 2013;79(6):727. doi:10.5935/1808-8694.20130133
- Hatzopoulos S. Advances in clinical audiology. In: InTech. 2017. doi:10.5772/63685
- Szczepek AJ. Ototoxicity: old and new foes. In: InTech. 2017. doi:10.5772/66933
- Chandanshive C, Rangasayee R. A follow-up study of effect of PDE5i drugs on extended high-frequency hearing. Indian J Otolaryngol Head Neck Surg. 2025;77(3):1537. doi:10.1007/s12070-025-05372-0
- AlRuwaili R, Al-Kuraishy HM, Alruwaili M, Khalifa AK, Alexiou A, Papadakis M, et al. The potential therapeutic effect of phosphodiesterase 5 inhibitors in acute ischemic stroke. Mol Cell Biochem. 2023;479(5):1267. doi:10.1007/s11010-023-04793-1
- Hayashi Y, Okada M, Yamada H, Hato N. A case of sudden sensorineural hearing loss associated with phosphodiesterase type 5 inhibitors. Pract Otorhinolaryngol. 2017;110(8):505. doi:10.5631/jibirn.110.505
- Khan AS, Sheikh Z, Khan S, Dwivedi RC, Benjamin E. Viagra deafness: sensorineural hearing loss and phosphodiesterase-5 inhibitors. Laryngoscope. 2011;121(5):1049. doi:10.1002/lary.21450
- Sarris AB, Nakamura MC, Fernandes LGR, Staichak RL, Pupulim AF, Sobreiro BP. Pathophysiology, evaluation and treatment of erectile dysfunction: review article. Rev Med. 2016;95(1):18. doi:10.11606/issn.1679-9836.v95i1p18-29
- Öntepeli S, Muluk NB, Tuğlu D, Şipal T. Audiometry results and TEOAE and DPOAE amplitudes in men taking a phosphodiesterase type 5 inhibitor. Ear Nose Throat J. 2017;96(7). doi:10.1177/0145561370960070
- Mittal R, Bencie N, Shaikh N, Mittal J, Liu XZ, Eshraghi AA. Role of cyclic nucleotide phosphodiesterases in inner ear and hearing. Front Physiol. 2017;8. doi:10.3389/fphys.2017.00908
- Terzi S, Özgür A, Çeliker M, Mercantepe T, Yılmaz A, Tümkaya L, et al. The protective effect of astaxanthin on cisplatin-induced ototoxicity. Adv Clin Exp Med. 2021;30(3):315. doi:10.17219/acem/133081
- Okuyucu Ş, Güven O, Akoğlu E, Uçar E, Dağ S. Effect of phosphodiesterase-5 inhibitor on hearing. J Laryngol Otol. 2009;123(7):718. doi:10.1017/S002221510900423X
- Zhang X, Xia L, Yang Q, Tang P. Phosphodiesterase type 5 inhibitors-related hearing impairment: a real-world study based on the FDA adverse event reporting system. Sci Rep. 2024;14(1):9743. doi:10.1038/s41598-024-60493-w
- Cook AM, Patuzzi R. One mechanism of sudden sensorineural hearing loss after sildenafil and sexual activity. Int J Audiol. 2024;64(1):94. doi:10.1080/14992027.2024.2368577
- Abd-Elhakim YM, Abdel-Motal SM, Malhat SM, Mostafa HI, Ibrahim WM, Beheiry RR, et al. Curcumin attenuates gentamicin and sodium salicylate ototoxic effects by modulating NF-κB and apoptotic pathways in rats. Environ Sci Pollut Res. 2022;29(60):89954. doi:10.1007/s11356-022-21932-1
- Chaplan SR, Bach FW, Pogrel JW, Chung JM, Yaksh TL. Quantitative assessment of tactile allodynia in the rat paw. J Neurosci Methods. 1994;53(1):55. doi:10.1016/0165-0270(94)90144-9
- Hong BN, Yi T, Kim SY, Kang TH. High dosage sildenafil induces hearing impairment in mice. Biol Pharm Bull. 2008;31(10):1981. doi:10.1248/bpb.31.1981
- Thakur JS, Thakur S, Sharma D, Mohindroo NK, Thakur A, Negi PC. Hearing loss with phosphodiesterase-5 inhibitors. Laryngoscope. 2013;123(6):1527. doi:10.1002/lary.23865