






Impact of Person-Centered Care on Nursing Home Mental Health
Does Person-Centered Care Improve Nursing Facility Residents’ Mental Health? A Review and Commentary
Linda Hermer, Ph.D.1,2* and Anusha Natarajan, M.A.3
- Vantage Precision Health, 6200 Westchester Drive, Suite 803, College Park, MD 20740
- Amnon Labs, 35 E. Blancke Street, Linden, NJ 07036
- Institute for Social and Economic Research and Policy (ISERP), 61 Claremont Avenue, Suite 503, Mail Code 3355, New York, NY 10115
OPEN ACCESS
PUBLISHED 31 December 2025
CITATION Hermer, L., and Natarajan, A., 2025. Does Person-Centered Care Improve Nursing Facility Residents’ Mental Health? A Review and Commentary. Medical Research Archives, [online] 13(12). https://doi.org/10.18103/mra.v13i12.7050
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i12.7050
ISSN 2375-1924
ABSTRACT
Loneliness, social isolation, and depression are prevalent among nursing home residents worldwide, causing mortality risks that rival those of major chronic diseases. Over the past three decades, the person-centered care movement has sought to replace the institutional medical model with care prioritizing residents’ individuality, dignity, and meaningful relationships. This review and commentary traces the evolution of person-centered care models and evaluates the evidence regarding whether person-centered care improves resident mental health. As part of our review, we consider evidence gathered from nursing home residents and staff during the COVID-19 pandemic, which led to the removal of major elements of person-centered care from daily life. Older, pre-pandemic studies yielded mixed but increasingly positive results, with higher-quality designs showing that thorough person-centered care adoption improves quality of life and reduces depressive and neuropsychiatric symptoms. Our own research has clarified mechanisms by which person-centered care improves residents’ mental wellbeing. In a comparative observational study of homes differing in levels of person-centered care adoption, residents in high-person-centered care settings displayed greater positive affect, engagement, and social connection. In a follow-up longitudinal study, higher person-centered care scores predicted significant Patient Health Questionnaire-9 (PHQ-9) reductions and increased expressions of pleasure, mediated by stronger aide–resident relationships and timely depression treatment. Statewide analyses of Kansas’s Medicaid program to incentivize person-centered care adoption (the Promoting Excellent Alternatives in Kansas 2.0, or PEAK 2.0, program) showed that residents whose facilities were strong person-centered care adopters had strikingly lower odds of depression and better clinical outcomes overall. Pandemic disruptions provided a stress test for person-centered care. When social contact and autonomy were curtailed, resident mental health declined sharply, underscoring the protective mechanisms person-centered care fosters. Emerging post-pandemic evidence reaffirms that comprehensive person-centered care improves psychological wellbeing and stabilizes the workforce through enhanced job satisfaction and lower turnover. Yet under 15% of U.S. facilities have fully implemented person-centered care, hindered by workforce instability and structural financial disincentives. Facilities should pursue thoroughly person-centered care adoption to transform themselves into communities where elders can live with dignity, purpose, and connection.
Keywords: person-centered care, nursing homes, mental health, loneliness, social isolation, depression
Introduction
Nursing homes remain a critical part of long-term care in the United States and many other nations, yet they have long been criticized for their institutional design and neglect of residents’ psychosocial wellbeing. This review and commentary aim to clarify whether and how person-centered care (PCC)—a movement to replace the traditional medical model with one that honors residents’ individuality, autonomy, dignity, and relationships—improves mental health and quality of life for long-stay residents. For readers unfamiliar with the health consequences of chronic loneliness and social isolation, or with U.S. systems for long-term care and nursing home PCC, we start with an overview of those concepts. Then we trace the evolution of PCC from its international, philosophical roots to commonly implemented models; evaluate pre-, during-, and post-pandemic evidence linking PCC to better psychosocial outcomes; and summarize our own empirical findings from multi-site and statewide studies of PCC’s effects on depression, the experience of pleasure, and resident and family satisfaction. We also highlight our efforts to provide insight into the mechanisms by which PCC impacts resident mental health. Finally, we discuss barriers to adoption, including workforce instability and financial incentives, and outline policy and research directions necessary for PCC to realize its full potential in transforming institutional care.
AGING AND LONG-TERM CARE GLOBALLY AND IN THE UNITED STATES
Globally, populations are aging at an unprecedented pace. By 2050, nearly one in four people in Europe will be aged 65 and older, with similar surges in elder populations occurring across North America and Asia. In the U.S., from 2023 to 2030, the percentage of adults 80 years and older is expected to grow from 3.3% to 4.1% of the total population — a nearly 30% increase. How societies respond to this demographic shift varies dramatically. European societies generally support aging-in-place (remaining at home), with families and communities as the primary caregivers. In the United States, while there is increasing support for aging-in-place, over 1.2 million elders were institutionalized as “long-stay” residents in 2024—those receiving nursing home care for over 100 days, typically until the end of their lives.
LONELINESS, SOCIAL ISOLATION, AND DEPRESSION AMONG NURSING HOME RESIDENTS
The subjective feeling of “loneliness” and the objective state of being socially isolated occur at alarming rates among community-dwelling older adults, with high-quality studies of community-dwelling seniors in the U.S. finding rates of ~30-40% for loneliness and 15-25% for social isolation (L/SI). Unfortunately, nursing home residents report experiencing these conditions even more often; e.g., for loneliness (moderate to severe): ~50-90% of residents in the U.S. and abroad, and for social isolation: ~30-40% of residents. The prevalence of L/SI in U.S. nursing facilities peaked during the pandemic when facilities were locked down, resulting in no visitations by family, friends, or volunteers. Additionally, the requirement to wear personal protective equipment (PPE) by staff and residents shielded social signals like facial expressions and generally led facility leadership to halt group activities. Mandated social distancing further limited social engagement among residents and staff. For nursing homes, these stipulations lasted a minimum of several months, and for facilities in certain states, well over a year. In resident surveys, these factors markedly increased their sense of L/SI. Post-pandemic, it appears that nursing home residents have not fully recovered, as their rates of loneliness and social isolation have remained above pre-pandemic levels.
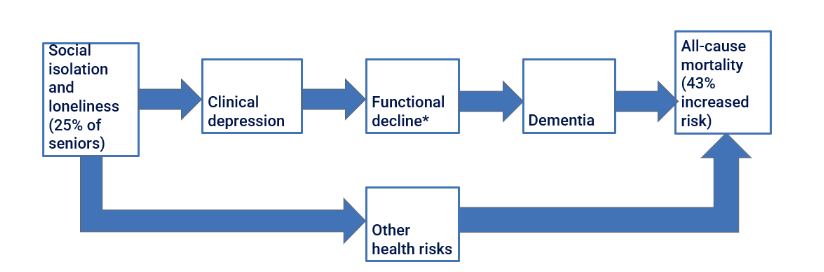
The rising rates of loneliness and social isolation among older adults are considered a mounting public health crisis in the U.S.—particularly for nursing home residents. The health consequences of experiencing L/SI can be severe. Feeling chronically alone raises the risk of clinical depression, functional decline, and dementia by ~50%. Moreover, experiencing these conditions is not just correlated with L/SI. As is seen so often in nursing facility residents, depression, functional decline, and dementia often stem from L/SI—occurring in the above sequence, and culminating in a heightened risk of death—with one high-quality study indicating an increase in one-year, all-cause mortality rate of 43%, as depicted in Figure 1. Not all of the mortality risk is explained by L/SI leading to functional decline and dementia, so we suggest there is a second pathway leading from L/SI to death from other causes. The consequences of experiencing both loneliness and social isolation are grave—comparable to the increased mortality caused by chronically smoking 15 cigarettes per day. Consistent with these findings and hypotheses, post-pandemic studies of nursing facility residents have found elevated prevalences of functional decline, dementia, and death.
TRADITIONAL NURSING FACILITIES
Historically, loneliness, social isolation, and clinical depression have been most pronounced in traditional “medical-model” nursing homes, which are facilities designed similar to hospitals, consisting of long corridors, regimented routines, and limited opportunities for resident choice. In such settings, the staff who interact most with residents—certified nursing aides (CNAs or aides)—are instructed to prioritize clinical tasks, such as bathing and dressing residents, without guidance to form close bonds with residents or otherwise advance their psychosocial wellbeing. Residents and frontline aides alike have little autonomy; e.g., residents can seldom choose which activities they participate in or what they are given to eat, and aides are generally not authorized to make care decisions. Especially for the long-stay residents in traditional facilities, the hospital-like building layout and dehumanizing operating principles are thought to cause social isolation and loneliness, boredom, a lack of meaning in daily life, and poor quality of life.
PERSON-CENTERED CARE FOR NURSING HOME RESIDENTS
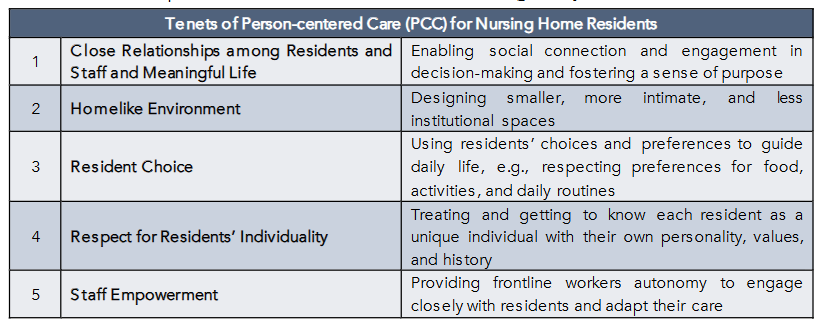
We and our colleagues at Kansas State University, LeadingAge, and Rutgers University have been assessing the long-term benefits for residents and staff of an alternative to the medical model for nursing homes: person-centered care (PCC). In healthcare more generally—and as addressed by other contributions to this special issue—PCC holds that providers should respect patients’ values, preferences, and choices. In the case of nursing facilities, PCC (in reference to nursing homes, also known as “culture change”) shifts priorities away from the medical model toward fostering residents’ and staff’s mental wellbeing and quality of life. Nursing home PCC (henceforth “PCC”) doesn’t deemphasize providing high-quality medical care, but prioritizes their mental wellbeing just as highly. This means respecting individual residents’ values, preferences, and needs, recognizing residents as active partners in making care choices, and emphasizing building relationships, promoting autonomy, fostering dignity, and creating a homelike environment, as outlined in Table 1.
Purpose
In this review, we evaluate whether PCC implementation improves nursing home residents’ psychosocial health, drawing on pre- and post-pandemic studies and our own research. We conclude with implications for practice, policy, and the future of person-centered long-term care.
The Movement Toward, and Models of, Person-Centered Care
PCC is best understood not as a single model, but as a philosophy of care meant to address the longstanding harms of institutional nursing home life—social isolation, loneliness, and the subsequent mental and physical decline. This movement began over three decades ago and is supported by diverse international stakeholders, including policymakers, nursing home leadership, staff, residents, and families. Although the movement was sometimes led by different people or groups in different countries, these individuals were united by a common goal of transforming nursing homes into communities that felt homelike, facilitated residents’ quality of life, and brought more job satisfaction to frontline care staff.
MODELS OF PCC: FROM PHILOSOPHY TO PRACTICE
To operationalize these ideals, a number of PCC models have been developed in the United States and abroad. Among the earliest and most influential was the Eden Alternative, created in 1991–1992 by geriatrician William Thomas to combat what he termed the “three plagues” of nursing homes: loneliness, helplessness, and boredom. Eden transformed traditional institutions into vibrant communities by integrating plants, animals, and intergenerational activities into daily life—restoring spontaneity and companionship. Building on this foundation, Thomas and colleagues developed the Green House model, which took deinstitutionalization a step further. Green House homes were purpose-built, small-scale residences—typically housing 10–12 residents—with private rooms, open kitchens serving residents’ preferred foods, and self-directed staff teams working without rigid hierarchies. The design emphasized autonomy and intimacy, replacing traditional long corridors and nurse stations with shared living spaces and flexible daily routines.
While the Eden and Green House models indicated specific changes that facilities should make, the state of Kansas pioneered a more systemic approach: Promoting Excellent Alternatives in Kansas (PEAK) 2.0. Launched in 2011–2012, PEAK 2.0 became the first large-scale, statewide initiative to incentivize PCC adoption across all nursing facilities. Its design took advantage of the U.S. financing structure for long-term care, in which most long-stay residents are covered by Medicaid, the U.S.’s public insurance program for people with low incomes. Because Medicaid reimburses facilities for the majority of long-stay care, states can influence facility practices through their payment models.
Under PEAK 2.0, Kansas replaced uniform Medicaid reimbursement with a pay-for-performance (P4P) system: Facilities demonstrating successively higher levels of PCC adoption received higher payment rates. From 2014 to 2017, the Kansas State University Center on Aging, which administered the program, conducted annual on-site assessments of PCC implementation for each of the state’s 349 nursing homes, scored from 0 (no adoption) to 4 (thorough adoption). Using data from those years, we found that PEAK 2.0 succeeded in facilitating large-scale PCC adoption, with most facilities in the state achieving at least partial implementation. The PEAK 2.0 program continues to expand. Its funding and bonus payments have increased as facilities meet higher standards, and its framework has inspired at least seven additional U.S. states— including Maryland, Illinois, Maine, New Jersey, Ohio, Colorado, and Minnesota, as of 2022—to develop value-based payment systems linking Medicaid reimbursement to quality indicators such as staffing stability and PCC adoption.
What is daily life like in a nursing home that has comprehensively adopted PCC as its founders intended?
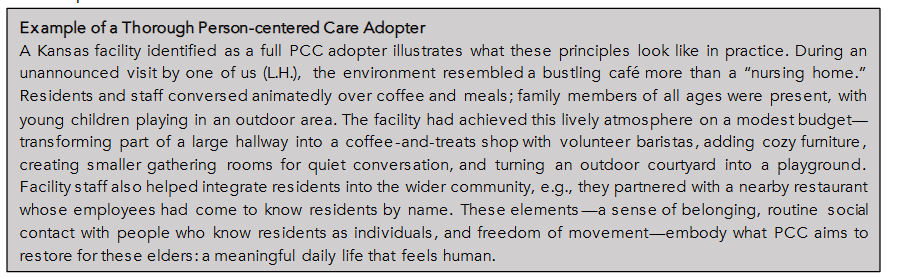
Box 1 below describes the lively atmosphere in a facility that thoroughly and successfully implemented PCC. Residents, staff, intergenerational visitors and even the surrounding community are benefiting richly from it. Furthermore, implementing it successfully didn’t require a large, initial capital outlay and led to higher occupancy and greater resident and family satisfaction.
EVIDENCE LINKING PERSON-CENTERED CARE TO REDUCED DEPRESSION AND BETTER PSYCHOSOCIAL HEALTH
INTRODUCTION
Many facilities have adopted PCC, and several states are incentivizing its adoption systemically in facilities throughout their states. But does PCC achieve one of its major goals: improving residents’ psychosocial wellbeing? PCC has obvious face validity, as most people recognize that all individuals regardless of age would like their values and preferences to be respected and to engage in meaningful relationships and activities; likewise, they understand that frontline staff would rather find their jobs satisfying than frustrating, exhausting, and even denigrating. But does PCC actually improve residents’ mental health and quality of life? And if it does so, what are the mechanisms by which these improvements take place? This second question has critical implications about which elements of PCC are most important to adopt, especially given that most U.S. facilities adopt PCC only partially and in individualistic ways.
PRE-PANDEMIC EVIDENCE
The pre-pandemic evidence on whether PCC improved residents’ mental health and wellbeing tilted slightly positive overall. Some studies revealed seemingly powerful benefits, but study quality issues, variations in the models examined, and a few prominent failures to find benefits in high-quality studies limited drawing any definitive conclusions. The earliest studies were particularly inconclusive. For example, in a review of the quality and results of 36 studies published between 2005 and 2012, there were few clearly positive associations between PCC and residents’ mental or physical wellbeing. However, it was difficult to synthesize the evidence across studies because of variations in the domains of PCC evaluated (e.g., homelike environment vs. resident-centeredness) and a general lack of implementation assessments, among other issues. Another early study found that compared to a traditional control facility, residents in an experimental Eden Alternative home had a higher rate of falls and nutritional deficiencies. Nevertheless, potential benefits to resident mental wellbeing—a major goal of implementing Eden—were not well-assessed. In fact, residents in the Eden home may have experienced better mental health and quality of life, but in the early stages of implementing the new model (the study examined outcomes only one year after the start), staff may have focused more on residents’ mental wellbeing than their safety and nutrition. Indeed, another study from roughly that time found that residing in an Eden home was associated with an improvement in residents’ quality of life.
As subsequent studies addressed the earlier studies’ limitations, evidence of PCC’s benefits to resident mental wellbeing accumulated. For example, Grabowski et al. (2014) undertook the first large-scale study of whether PCC improves care quality using a design allowing for causal inference, a difference-in-difference (DID) design—examining pre-/post- outcomes in a nationally recognized group of “expert” PCC adopters and comparing them to outcomes at the same two times in facilities not identified as expert adopters. They found 15% fewer survey deficiencies, a set of measures related to the quality of care, in expert adopters compared to controls, but no observed improvements in the 13 more direct measures of resident mental and physical health they examined. The lack of more clearly positive findings might have arisen because the degree of PCC adoption was not assessed in the control facilities, i.e. some control homes may have partially adopted PCC over the study period but without being recognized as expert adopters, thus biasing the results toward the null hypothesis. Another notable study focused on whether PCC improved mental wellbeing specifically in nursing home residents with dementia, who comprise the majority of residents in many U.S. homes. Importantly, given the inclusion of so many RCTs, they found that residents in PCC settings experienced better quality of life and were less agitated and depressed. Both Grabowski et al.’s DID study and Kim and Park’s meta-analysis of RCTs allowed causal inference, with Kim and Park’s analysis providing especially compelling evidence that PCC improved residents’ mental health and wellbeing. Multiple other well-designed studies during this period revealed that PCC enhanced residents’ quality of life.
Our Contributions to Evidence on Person-Centered Care and Resident Mental Health
Critical Elements of PCC, and Mechanisms for Improved Mental Health
With a few exceptions, most pre-pandemic studies did not investigate how PCC improves psychosocial health. To some, it might seem obvious that respecting residents’ individuality, forming closer bonds with them, and treating them with dignity in a comfortable, homelike environment would bring social and emotional benefits, and mounting evidence suggested that this was the case. But we argue that there are multiple pathways by which PCC can improve psychosocial wellbeing, and we provide evidence regarding this. One reason it matters so much to illuminate how PCC improves mental wellbeing is that some aspects of PCC are more expensive or otherwise difficult to implement than others (e.g., environmental renovations can be costly). Also, over an extended time, most facilities nationally have undertaken partial—not full—PCC adoption and have implemented PCC in idiosyncratic ways. If many facilities were going to implement PCC only partially, which elements were the je-ne-sais-quois that led to successes like the Kansas facility described earlier? From a practical perspective, answers to these questions would help facility leadership decide which aspects of PCC were most important to adopt.
Critical Elements of Person-Centered Care
To probe how person-centered care (PCC) improves residents’ mental wellbeing, we began by conducting a comparative observational study of three nursing homes that varied in their degree of “culture change” adoption: a “household-model” facility with entirely new, homelike buildings that had comprehensively implemented PCC, and two control homes that had partially adopted it within traditional, institutional layouts. At baseline, we matched residents across facilities on demographics, presence or absence of a dementia diagnosis, and depression severity, and observed each resident’s visible affect, engagement, and activities for eight hours at five-minute intervals, at baseline and a one-year follow-up. In parallel, staff were observed and rated for person-centeredness of care. These methods produced one of the most fine-grained behavioral data sets of nursing-home life to date. We also assessed PCC implementation at the outset of the study across environmental, organizational, and policy domains.
Results showed that residents in the household-model home spent less time idle or parked in hallways, more time actively engaged in meaningful activities, and exhibited more positive affect during meals, particularly while interacting with staff. Staff themselves were observed providing more person-centered care, engaging residents in conversation and shared tasks. Markedly higher levels of pleasure, engagement, and social connection in the dining area than at control sites. These findings suggest that the mechanisms linking PCC to psychosocial wellbeing include richer resident–staff interactions and emotionally resonant shared spaces—especially mealtimes that foster “place attachment” (as their former family homes might have) and daily social rhythms. Importantly, the data also implies that facilities might achieve many of these psychosocial benefits through selective, targeted modifications focused on dining redesign, resident-choice policies, and the quality of resident-staff relationships—without incurring the full capital costs of complete architectural transformation.
Pathways Linking Person-Centered Care to Depression Reduction (Unpublished Data)
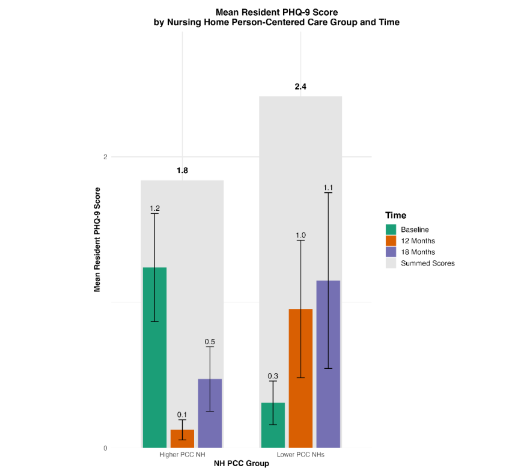
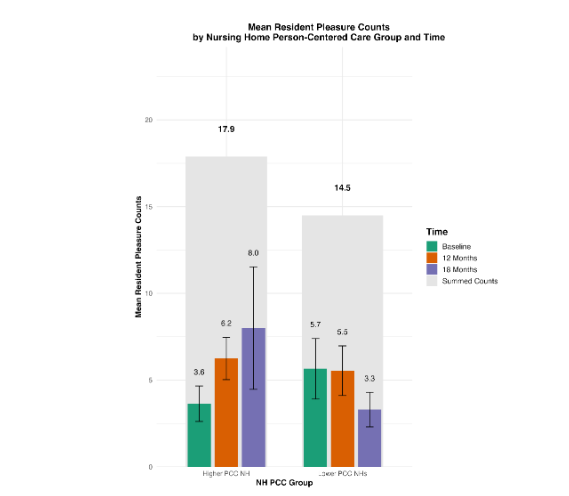
Thus, higher degrees of PCC implementation were associated with more expressions of pleasure, greater engagement in activities, and potentially more meaningful relationships between residents and aides. This study was part of a larger, 18-month prospective cohort study we were conducting to evaluate whether PCC reduced depressive symptoms. Drawing on the findings from the 2017 study, we hypothesized that there were at least two pathways by which PCC would lead to reductions in depressive symptoms: 1. Detection and treatment pathway – Close aide–resident relationships improve staff sensitivity to subtle mood changes, allowing earlier detection and treatment (e.g., timely antidepressant initiation). 2. Meaning and relationship pathway – Residents experience daily routines tailored to them, and more dignity and social meaning through mutual relationships.
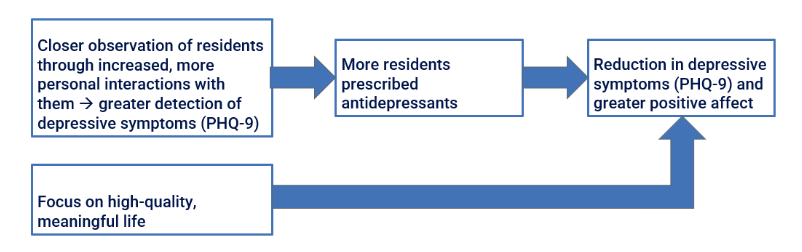
To evaluate these pathways, we conducted an 18-month longitudinal study using repeated PHQ-9 measures and observational coding of affect. General linear mixed-effects models indicated that compared to baseline, at 12- and 18-month follow-ups residents in higher-PCC facilities showed marked declines in depressive symptoms and parallel increases in observed smiling and laughing. The figures depicting PHQ-9 trajectories suggest both direct and indirect effects consistent with our hypothesized model: reduced depressive symptomatology was partly mediated by increases in antidepressant initiation (the detection/treatment pathway) and partly by increased engagement in conversations and other activities (the meaning/relationship pathway). We plan to perform structural equation modeling (SEM) to formally test these mediational relationships, linking organizational PCC domains to resident-level emotional health.
Statewide Evidence: Kansas PEAK 2.0 Program
We also investigated whether systemic mechanisms to incentivize PCC adoption led to improved mental and physical health. We assessed whether a statewide pay-for-performance initiative could both scale PCC and improve outcomes. As described in the section on models of PCC, the Kansas program Promoting Excellent Alternatives in Kansas Nursing Homes (PEAK 2.0) incentivizes facilities to advance through progressively higher PCC implementation stages, verified by annual onsite implementation assessments. Our analysis of 349 Kansas nursing homes linked program stage (0, non-adoption, to 3 and 4, highest adoption) to 13 Minimum Data Set 2.0 long-stay resident mental and physical outcomes. Residents living in facilities at higher stages of PCC exhibited a sharply lower prevalence of major depressive symptoms—approximately 49% lower than non-adopters—and better outcomes on six of the other health indicators, including pressure ulcers and restraint use. A composite health index also improved in a clear dose-response fashion: the more advanced the PCC implementation, the better the overall resident health. These results are especially striking given that PEAK 2.0 incentivized adoption of PCC rather than direct clinical performance, yet meaningful clinical benefits emerged as a byproduct of culture change.
Resident and Family Satisfaction
Finally, our survey of residents and families across Kansas nursing homes demonstrated that greater PCC implementation predicted higher satisfaction across nearly all domains—care quality, staff responsiveness, respect for preferences, and perceived autonomy. Families of residents in high-PCC facilities were more likely to recommend the facility and reported stronger trust in staff, echoing the emotional-connection mechanisms identified in our observational and depression studies.
Summary of Our Contributions
Together, these convergent findings—obtained from a combination of fine-grained behavioral observation, longitudinal depression tracking, statewide outcomes, and satisfaction surveys—indicate that PCC improves psychosocial wellbeing through both interpersonal relationship-related and systemic mechanisms. The benefits extend beyond affective health to encompass clinical quality and stakeholder satisfaction. These findings suggest that PCC not only humanizes care but also enhances its effectiveness and sustainability.
The Pandemic as a Stress Test of PCC Mechanisms
COVID-19 disrupted core elements of PCC. For the first several months, CMS mandates to reduce infection rates included no outside visitors or group activities and minimal interactions with staff. As documented by staff surveys, throughout the pandemic there were enormous barriers to PCC including continued constraints on resident choice and visitors, staff anxiety, severe short-staffing, and expanded staff duties that limited their ability to provide individualized care. Thus, like the Kansas PEAK 2.0 program levels with resident health outcomes, the pandemic and its disruptions of daily nursing home life allowed a dose-response test of the effects of PCC on mental health, but a more dramatic one: What happens when almost all elements of PCC are removed? While some pre-pandemic evidence indicated that PCC improved resident wellbeing, did the curtailment of close relationships, lack of visitors, and other abrogation of PCC tenets worsen resident psychosocial wellbeing?
IN RESIDENTS’ OWN VOICES
Disruptions to administering PCC during the pandemic are well-documented. Surveys of residents in nursing facilities across 36 states showed sharp drops in visits and activities and marked increases in loneliness; many residents remained uninfected and yet they experienced malaise, weight loss, and worsened mental health, implicating isolation and lost PCC practices as drivers. Qualitative accounts captured residents’ profound distress at their loss of freedom and meaning in daily life. For example, many shared feelings of hopelessness and even a desire to die, making comments like “If the virus doesn’t kill me the loneliness will” and “I have depression—why keep living? It’s not living and it’s barely existing.” The pandemic period thereby illuminated several of the mechanisms PCC targets: When autonomy and relationships are all but forbidden, mood, engagement, and health decline.
Facility Adaptations and Evidence on Person-Centered Care and Resident Mental Health since the Pandemic
As restrictions eased, facilities re-established PCC with staff support, technology-mediated connection, and environmental adaptations. Recent evidence mostly reaffirms that PCC improves psychological wellbeing, especially when implemented comprehensively and in a sustained manner. As the acute phase of the COVID-19 pandemic ended in 2022-2023, nursing facilities have worked to restore and enhance person-centered care (PCC) practices, incorporating lessons learned from the crisis. For example, Morgan et al. (2023) surveyed 379 staff across 11 nursing homes in Georgia, finding that while COVID-19 precautions initially created barriers to PCC implementation— including (as with earlier studies) reduced resident choice, staff anxiety, and expanded duties for direct care workers—facilities also developed important facilitations. These included enhanced staff engagement, provision of mental health resources, increased supervisor support, staff empowerment measures, and technological innovations. Industry reports indicated that nursing homes were increasingly leveraging telehealth platforms and remote monitoring systems to maintain person-centered connections while keeping infection risks low. The post-pandemic era has seen facilities prioritizing flexible staffing models, enhanced environmental design for both safety and creating a homelike atmosphere, and strengthened family engagement strategies that balance infection control with meaningful relationships.
Recent high-quality studies support the earlier findings that person-centered care significantly improves resident mental health and wellbeing. Across countries and designs (including high-quality studies), a majority of the evidence converges that PCC reduces depressive symptoms and enhances psychosocial wellbeing; effect sizes are largest under comprehensive, sustained implementation. For instance, a systematic review of reviews synthesized evidence from 11 studies with strong designs, identifying six core principles of patient-centered mental health services, with particular emphasis on psychological well-being outcomes including reduced anxiety, depression, and improved mood regulation. Further recent studies support the linkage between PCC and enhanced resident mental health.
More mixed evidence comes from a systematic review and meta-analysis of 17 randomized controlled trials examining person-centered care interventions for people living with dementia. This rigorous analysis found that person-centered care implementation significantly improved cognitive function (pooled standardized mean difference: 0.22; 95% CI [0.04, 0.41], p = .02), a not only significant but clinically meaningful effect. However, the review found mixed results across studies for depression and quality of life outcomes. Additionally, a cluster randomized controlled trial comparing team-based versus problem-based approaches to resident-centered dementia care found that comprehensive facility-wide training approaches led to staff viewing previously problematic behaviors (such as wandering) as positive coping strategies, suggesting important shifts in care philosophy. However, like Saragih et al.’s study, this study also revealed some mixed outcomes, with trends toward increased behavioral symptoms in the team-based intervention arm, highlighting the complexity of implementing person-centered approaches and the need for careful monitoring of unintended consequences.
The cumulative evidence from these recent studies mostly reinforces earlier findings that person-centered care improves psychological well-being among nursing facility residents. We note that the strongest effects observed when the interventions were implemented comprehensively and sustained over time.
The recent literature largely demonstrates that post-pandemic, nursing homes adopted new strategies, including use of telehealth and other technologies and flexible staffing, to restore person-centered care.
Strong evidence shows PCC improves mental health, cognition, and well-being, especially when implemented comprehensively. However, some studies highlight implementation challenges and mixed outcomes, emphasizing the need for careful monitoring.
Person-Centered Care and Staff Outcomes
PCC also positively impacts staff. For example, nursing assistants in high-PCC environments report greater job satisfaction, stronger resident relationships, and lower burnout. A further example is Sköldunger et al. (2020), who found that PCC reduces aides’ job strain. Consistent staffing models—where aides care for the same residents over time—appear especially effective in reducing aide stress and turnover. These effects matter: PCC findings demonstrated that aide consistency and closeness were key factors driving resident wellbeing and satisfaction. These and many other findings imply that aide turnover is among the most significant threats to nursing home quality. By improving job satisfaction and relationships, PCC indirectly benefits residents through workforce stabilization.
Systemic Barriers to Implementation
UNEVEN ADOPTION
Despite evidence of its benefits, full PCC implementation remains rare in the U.S. The Centers for Medicare and Medicaid Services (CMS) requires nursing homes to assess resident preferences for daily routines and activities (Minimum Data Set 3.0, Section F), institutionalizing the recognition of individuality in care. Yet surveys show that most facilities (85%) report only partial adoption of culture-change practices, with under 15% having fully implemented them. Therefore, thorough PCC appears to be more the exception than the rule. However, many facilities make their environment more homelike without entirely renovating their buildings and might have underreported their extent of adoption. It is also possible that in recent years, especially since the pandemic, further facilities have implemented all tenets of PCC.
MECHANISMS UNDERLYING UNEVEN ADOPTION
In another Kansas PEAK 2.0 program study, our team examined why transforming institutional nursing homes’ culture to adopt PCC fully is so difficult. We conducted a multi-arm, pre-post intervention study during 2014-2015, comparing nursing homes that were “pre-adopters” (just beginning PEAK 2.0’s foundational year) to “adopters” (facilities that had already implemented PCC for a year). We compared staff perceptions of PCC implementation across seven domains at two critical times—just before versus after a year of education and exposure. The study revealed a key barrier to comprehensive PCC transformation: Pre-adopters initially rated their PCC implementation significantly higher than adopters did, but after a year of education and exposure to true PCC practices, pre-adopters’ self-ratings decreased significantly while adopters’ ratings increased. This counterintuitive finding suggests that many nursing homes believe they are already implementing PCC when they are not, creating a false sense of accomplishment that prevents deeper transformation. This misperception appeared to serve as a major source of resistance to change. For example, one facility reported that by celebrating residents’ birthdays—without asking residents whether they would like to—they had adopted PCC. To understand and truly adopt PCC, they had to “unlearn” inaccurate definitions of PCC through education, and experience “aha moments” when they recognized the gap between their current practices and true person-centered care. This educational process helped break down organizational resistance and improve adoption rates.
Leadership at the thoroughly adopting Kansas facility described earlier reported how they transitioned from early misconceptions to a deep understanding of PCC. Initially—and without asking residents what they wanted—the staff began celebrating residents’ birthdays, thinking this was a major step toward full adoption. However, this did not seem to improve morale in the nursing home. When they actually interviewed residents to find out more about what they wanted, they were surprised to learn that most residents did not care about (or even disliked) birthday celebrations, and instead asked for changes that would facilitate meaningful, intimate and enjoyable interactions with others and a continued intellectual life. The result was the lively atmosphere noted in Box 1, with some residents reading newspapers in the coffee shop and people of all ages happily immersed in conversation or playing in the playground.
WORKFORCE INSTABILITY AND WAGES
Workforce instability is a critical barrier. Nursing aide turnover averages 40-60% per year in U.S. facilities and approaches 100% in many of them. This undermines continuity of care and the close resident–aide relationships that are at the heart of PCC. Wages, though improved since the pandemic, remain a challenge. Pre-pandemic estimates suggested that wages were as low as $22,000 annually, though these may have been underestimated. The U.S. Bureau of Labor Statistics (BLS) reported that the median across industries was closer to $38,000 in 2019. By 2024, the median wage for NH nursing assistants had risen to approximately $39,610. While this represents some progress, pay still lags behind other entry-level healthcare roles, such as medical assistants or hospital-based aides, and turnover remains high. Chronic under-compensation and difficult working conditions foster churn, making it economically easier for facilities to accept turnover than to invest in retention.
STRUCTURAL AND FINANCIAL INCENTIVES
Multiple studies have found that over time (roughly one to several years), PCC does not increase resource use. Some studies have found that it is cost-neutral or even modestly cost-saving. Initially it requires more resources, but within a few years it results in higher occupancy, especially in private-pay facilities. There is evidence that some for-profit facilities may tolerate or even prefer high staff turnover because retaining aides would require higher wages and better conditions. Studies also suggest that profits in some facilities may be higher than reported in cost statements, raising questions about whether sufficient resources are directed to frontline staff.
Conclusion
Person-centered care represents one of the most effective strategies for counteracting the psychosocial harms of institutional nursing home life. By empowering frontline staff, fostering close resident–staff relationships, honoring personal preferences, and creating homelike environments, PCC helps circumvent the loneliness and social isolation → depression → functional decline → dementia pathway. Evidence from U.S. longitudinal studies and European clinical trials shows that PCC reduces depressive symptoms and improves psychosocial wellbeing.
However, adoption remains uneven, with only 13% of facilities fully committed to PCC. Until the U.S. significantly expands home- and community-based services (HCBS) to support aging in place—as many European countries have done—nursing homes will remain a central setting for elder care. In this context, advancing PCC is not optional but essential.
Crucially, this requires stabilizing the NH workforce. Adequate staffing levels, improved compensation, and supportive conditions are critical to enabling the close resident–aide relationships that PCC depends on. Without addressing the structural disincentives that make turnover profitable, PCC will remain out of reach for most facilities.
In short, PCC offers a path to transform U.S. nursing homes into places where older adults can live their final months or years not in isolation, but in dignity, connection, and contentment. The aging population makes this an urgent imperative: how we care for our elders today will help shape the humanity of our societies tomorrow.
Conflict of Interest Statement: None.
Funding Statement: None.
Acknowledgements: None.
References
- Andre C, Gal P, Schief M. Enhancing Productivity and Growth in an Ageing Society: Key Mechanisms and Policy Options. Organisation for Economic Co-operation and Development; 2024:1-55. https://www.oecd.org/content/dam/oecd/en/publications/reports/2024/06/enhancing-productivity-and-growth-in-an-ageing-society_68a94c77/605b0787-en.pdf
- The Impending Age Wave. NIC MAP. Accessed September 20, 2025. https://www.nicmap.com/blog/the-impending-age-wave-navigating-the-urgent-need-for-senior-housing/#:~:text=To%20understand%20the%20opportunity%20ahead,senior%20housing%20and%20care%20facilities
- Rau J. What Long-Term Care Looks Like Around the World. KFF Health News. November 14, 2023. Accessed August 21, 2025. https://kffhealthnews.org/news/article/dying-broke-long-term-care-other-countries/
- Harris R. Aging Alone: Elder Care Infrastructure in the EU. Harvard International Review. February 28, 2024. https://hir.harvard.edu/elder-care-infrastructure/#:~:text=Given%20new%20research%20establishing%20the,Europe’s%20disproportionately%20solitary%20elder%20population.
- New AARP Report: Majority of Adults 50-plus Want to Age in Place, But Policies and Communities Must Catch Up. AARP. December 10, 2024. https://press.aarp.org/2024-12-10-New-AARP-Report-Majority-Adults-50-plus-Age-Place-Policies-Communities-Catch-Up#:~:text=Dec%2010%2C%202024,of%20their%20income%20on%20housing
- Quality measures for nursing homes. Medicare.gov. https://www.medicare.gov/care-compare/resources/nursing-home/quality-of-resident-care
- Simard J, Ladislav V. Loneliness and Isolation in Long-term Care and the COVID-19 Pandemic. Journal of the American Medical Directors Association. 2020;21(7):966-967. doi:10.1016/j.jamda.2020.04.004
- Social Isolation and Loneliness in Older Adults: Opportunities for the Health Care System Social Isolation and Loneliness in Older Adults Opportunities for the Health Care System. National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Division of Behavioral and Social Sciences and Education; Board on Health Sciences Policy; Board on Behavioral, Cognitive, and Sensory Sciences; Committee on the Health and Medical Dimensions of Social Isolation and Loneliness in Older Adults; 2020. https://nap.nationalacademies.org/catalog/25663/social-isolation-and-loneliness-in-older-adults-opportunities-for-the
- Gardiner C, Laud P, Heaton T, Gott M. What is the prevalence of loneliness amongst older people living in residential and nursing care homes? A systematic review and meta-analysis. Age and Aging. 2020;49(5):748-757.
- Span P. Just What Older People Didn’t Need: More Isolation. The New York Times. April 13, 2020. Accessed October 18, 2025. https://www.nytimes.com/2020/04/13/health/coronavirus-elderly-isolation-loneliness.html
- Abbasai J. Social Isolation—the Other COVID-19 Threat in Nursing Homes. Journal of the American Medical Association. 2020;324(7):619-620. doi:10.1001/jama.2020.13484
- Montgomery A, Slocum S, Stanik C. Experiences of Nursing Home Residents During the Pandemic. Altarum; 2020:1-46.
- San Martín-Erice I, Escalada-Hernández P, García-Vivar C, Furtado-Eraso S, San Martín-Rodríguez L, Soto-Ruiz N. How did COVID-19 lockdown impact the health of older adults in nursing homes? A scoping review. BMC Geriatrics. 2024;24(1):760. doi:10.1186/s12877-024-05356-9
- Our Epidemic of Loneliness and Isolation: The U.S. Surgeon General’s Advisory on the Healing Effects of Social Connection and Community. Department of Health and Human Services; 2023:1-82.
- Egbujie BA, Betini G, Ochwat S, et al. Cross-National Evidence on Risk of Death Associated with Loneliness: A Survival Analysis of 1-Year All-Cause Mortality among Older Adult Home Care Recipients in Canada, Finland, and Aotearoa j New Zealand. Journal of the American Medical Directors Association. 2025;26(7):1-8. doi: https://doi.org/10.1016/j.jamda.2025.105687
- Holt-Lunstad J, Smith TB, Baker M, Harris T, Stephenson D. Loneliness and social isolation as risk factors for mortality: a meta-analytic review. Perspectives on Psychological Science. 2015;10(2):227-237. doi:10.1177/1745691614568352
- Freedman A, Nicolle J. Social isolation and loneliness: the new geriatric giants. Can Fam Physician. 2020;66(3):176-182.
- Kitwood T. Dementia Reconsidered: The Person Comes First. Open University Press
- Koren MJ. Person-Centered Care For Nursing Home Residents: The Culture-Change Movement. Health Affairs. 2010;29(2):312-317. doi:10.1377/hlthaff.2009.0966
- Brownie S, Nancarrow S. Effects of person-centered care on residents and staff in aged-care facilities: a systematic review. Clin Interv Aging. 2013;8:1-10. doi:10.2147/CIA.S38589
- White-Chu EF, Graves WJ, Godfrey SM, Bonner A, Sloane P. Beyond the medical model: the culture change revolution in long-term care. Journal of the American Medical Directors Association. 2009;10(6):370-378. doi:10.1016/j.jamda.2009.04.004
- Neves B, Sandra A, Kokanović R. “It’s the worst bloody feeling in the world”: Experiences of loneliness and social isolation among older people living in care homes. Journal of Aging Studies. 2019;49:74-84. doi: https://doi.org/10.1016/j.jaging.2019.100785
- Pomeroy ML, Cudjoe TKM, Cuellar AE, et. al. Association of Social Isolation With Hospitalization and Nursing Home Entry Among Community-Dwelling Older Adults. JAMA Internal Medicine. 2023;183(9):955-962. doi:10.1001/jamainternmed.2023.3064
- Hermer L, Bryant NS, Pucciarello M, Mlynarczyk C, Zhong B. Does Comprehensive Culture Change Adoption via the Household Model Enhance Nursing Home Residents’ Psychosocial Well-being? Innov Aging. 2017;1(2):igx033. doi:10.1093/geroni/igx033
- Thomas WH. Evolution of Eden. Journal of Social Work in Long-Term Care. 2008;2(1-2):141-157. doi: https://doi.org/10.1300/J181v02n01_10
- Hermer L, Cornelison L, Kaup ML, Poey JL, Stone R, Doll G. The Kansas PEAK 2.0 Program Facilitates the Diffusion of Culture-Change Innovation to Unlikely Adopters. The Gerontologist. 2018;58(3):530-539. doi:10.1093/geront/gnw210
- Thomas WH. The Eden Alternative: Nature, Hope and Nursing Homes. Eden Alternative Foundation; 1994.
- Pioneer Network. https://www.pioneernetwork.org
- Rabig J, Thomas W, Kane R, Cutler LJ, McAlilly S. Radical redesign of nursing homes: Applying the Green House concept in Tupelo, Mississippi. Gerontologist. 2006;46(4):533-539. doi:10.1093/geront/46.4.533
- Promoting Excellent Alternatives in Kansas. Kansas State University Center on Aging. https://www.hhs.k-state.edu/aging/research/peak20/
- Doll GA, Cornelison LJ, Rath H, Syme ML. Actualizing culture change: The Promoting Excellent Alternatives in Kansas Nursing Homes (PEAK 2.0) program. Psychological Services. 2017;14(3):307-315. doi: https://doi.org/10.1037/ser0000142
- Cohen LW, Zimmerman S, Reed D, et al. The Green House Model of Nursing Home Care in Design and Implementation. Health Services Research. 2016;51(S1):352-377. doi: https://doi.org/10.1111/1475-6773.12418
- Verbeek H, van Rossum E, Zwakhalen SMG, Kempen GIJM, Hamers JPH. Small, homelike care environments for older people with dementia: a literature review. International Psychogeriatrics. 2009;21(2):252-264. doi:10.1017/S104161020800820X
- Hodges K, Kaye N, Fox-Grage W. State Medicaid Value-Based Payment Incentivizes Staffing in Nursing Homes. National Academy for State Health Policy; 2025. https://nashp.org/state-medicaid-value-based-payment-incentivizes-staffing-in-nursing-homes/#:~:text=The%20incorporation%20of%20staffing%20metrics,for%20other%20states%20to%20consider.
- Nursing Facility Pay For Performance. Maryland Department of Health. https://health.maryland.gov/mmcp/longtermcare/pages/pay-for-performance.aspx
- Lima JC, Schwartz ML, Clark MA, Miller SC. The Changing Adoption of Culture Change Practices in U.S. Nursing Homes. Innovation in Aging. 2020;4(3):1-10. doi:10.1093/geroni/igaa012
- Miller SC, L SM, C LJ, et al. The Prevalence of Culture Change Practice in US Nursing Homes: Findings from a 2016/17 Nationwide Survey. Med Care. 2019;56(12):985-993. doi:10.1097/MLR.000000000000993
- Shier V, Khodyakov D, Cohen LW, Zimmerman S, Saliba D. What Does the Evidence Really Say About Culture Change in Nursing Homes? The Gerontologist. 2014;54(1):6-16. doi: https://doi.org/10.1093/geront/gnt147
- Coleman MT, Looney S, O’Brien J, Ziegler C, Pastorino CA, Turner C. The Eden Alternative: findings after 1 year of implementation. Journals of Gerontology Series A: Biological Sciences and Medical Sciences. 2002;57(7):422-427. doi:10.1093/gerona/57.7.m422
- Grabowski DC, O’Malley AJ, Afendulis CC, Caudry, DJ, Elliot A, Zimmerman S. Culture Change and Nursing Home Quality of Care. The Gerontologist. 2014;54(1):35-45. doi: https://doi.org/10.1093/geront/gnt143
- Kim SK, Park M. Effectiveness of person-centered care on people with dementia: a systematic review and meta-analysis. CIA. 2017; Volume 12:381-397. doi:10.2147/CIA.S117637
- Mukamel DB, Saliba D, Ladd H, Konetzka RT. Dementia Care Is Widespread In US Nursing Homes; Facilities With The Most Dementia Patients May Offer Better Care. Health affairs (Project Hope). 2023;42(6):795-803. doi:10.1377/hlthaff.2022.01263
- Ballard C, Corbett A, Orrell M, et al. Impact of person-centred care training and person-centred activities on quality of life, agitation, and antipsychotic use in people with dementia living in nursing homes: A cluster-randomised controlled trial. PLOS Medicine. 2018;15(2):1-18. doi:https://doi.org/10.1371/journal.pmed.1002500
- Sköldunger A, Sandman PO, Backman A. Exploring person-centred care in relation to resource utilization, resident quality of life and staff job strain – findings from the SWENIS study. BMC Geriatrics. 2020;20(1):1-9. doi: https://doi.org/10.1186/s12877-020-01855-7
- Li J, Porock D. Resident outcomes of person-centered care in long-term care: A narrative review of interventional research. International Journal of Nursing Studies. 2014;51(10):1395-1415. doi:10.1016/j.ijnurstu.2014.04.003
- LTCCC Brief for Policymakers: Consumer Perspectives on Nursing Home Culture Change. Long Term Care Community Coalition; :1-19. https://nursinghome411.org/wp-content/uploads/2022/03/LTCCC-Brief.Consumer-Perspectives-Culture-Change.pdf
- Poey JL, Hermer L, Cornelison L, et al. Does Person-Centered Care Improve Residents’ Satisfaction With Nursing Home Quality? Journal of the American Medical Directors Association. 2017;18(11):974-979. doi:10.1016/j.jamda.2017.06.007
- Morgan JC, Ahmad W, Chen YZ, Burgess EO. The Impact of COVID-19 on the Person-Centered Care Practices in Nursing Homes. J Appl Gerontol. 2023;42(7):1582-1587. doi:10.1177/07334648231154544
- Levere M, Rowan P, Wysocki A. The Adverse Effects of the COVID-19 Pandemic on Nursing Home Resident Well-Being. Journal of the American Medical Directors Association. 2021;22(5):948-954. doi:10.1016/j.jamda.2021.03.010
- Crespo-Martín A, Palacios-Ceña D, Huertas-Hoyas E, Güeita-Rodríguez J, Fernández-Gómez G, Pérez-Corrales J. Emotional Impact and Perception of Support in Nursing Home Residents during the COVID-19 Lockdown: A Qualitative Study. International Journal of Environmental Research and Public Health. 2022;19(23):1-13. doi: https://doi.org/10.3390/ijerph192315712
- Iyamu I, Plottel L, Snow ME, et al. Culture Change in Long-Term Care-Post COVID-19: Adapting to a New Reality Using Established Ideas and Systems. Canadian Journal on Aging. 2023;42(2):351-358. doi:10.1017/S0714980822000344
- Bergeron P. Long Term Care 2025 Trends and Outlook. Provider Magazine. January 14, 2025. https://www.providermagazine.com/Articles/Pages/Long%20Term%20Care%202025%20Trends%20and%20Outlook.aspx
- Siddiqi Z. Top Skilled Nursing Trends for 2025. Skilled Nursing News. January 3, 2025. https://skillednursingnews.com/2025/01/top-skilled-nursing-trends-for-2025/
- Khosravi M, Azar G, Izadi R. Principles and elements of patient-centredness in mental health services: a thematic analysis of a systematic review of reviews. BMJ Open Quality. 2024;13(3):1-11. doi: https://doi.org/10.1136/bmjoq-2023-002719
- Bäckman H, Lindkvist M, Niklasson J, Backman A. Health and Quality of Life in Nursing Homes: A Repeated Cross-Sectional Study on the Impact of Leadership and Person-Centred Care. Nursing Open. 2025;12(7):1-11. doi: https://doi.org/10.1002/nop2.70283
- Lorber M, Reljić NM, McCormack B, Kmetec S. Person-Centred Care in Association with Psychological Well-Being of Older Adults. Healthcare. 2025;13(12):1-12. doi: https://doi.org/10.3390/healthcare13121379
- Saragih ID, Suarilah I, Saragih IS, et al. A meta-analysis of person-centered care interventions for improving health outcomes in persons living with dementia. Worldviews on Evidence-Based Nursing. 2024;22(1). doi: https://doi.org/10.1111/wvn.12746
- Shier V, Bae-Shaaw YH, Sood N, et al. A Cluster Randomized Trial: Mixed Methods Comparison of 2 Approaches to Promote Nonpharmacologic, Resident-Centered Dementia Care in Nursing Homes. Journal of the American Medical Directors Association. 2024;25(10). doi:10.1016/j.jamda.2024.105216
- Lepore M, Scales K, Anderson RA, et al. Person-directed care planning in nursing homes: A scoping review. International Journal of Older People Nursing. 2018;13(4):1-12. doi:10.1111/opn.12212
- Barbosa A, Sousa L, Nolan M, Figueiredo D. Effects of Person-Centered Care Approaches to Dementia Care on Staff: A Systematic Review. American Journal of Alzheimer’s Disease & Other Dementias. 2014;30(8):713-722. doi: https://doi.org/10.1177/1533317513520213
- FastFacts: Consistent Assignment: A Key Step to Individualized Care. California HealthCare Foundation; 2007:1-2. https://www.chcf.org/wp-content/uploads/2017/12/PDF-FF21ConsistentAssignment.pdf
- Castle NG. Consistent assignment of nurse aides: association with turnover and absenteeism. Journal of aging & social policy. 2013;25(1):48-64. doi:10.1080/08959420.2012.705647
- Gandhi A, Yu H, Grabowski DC. High Nursing Staff Turnover In Nursing Homes Offers Important Quality Information. Health Affairs. 2021;40(3):384-391. doi:10.1377/hlthaff.2020.00957
- Castle NG, Engberg J. Staff turnover and quality of care in nursing homes. Medical Care. 2005;43(6):616-626. doi:10.1097/01.mlr.0000163661.67170.b9
- Sjögren K, Lindkvist M, Sandman PO, Zingmark K, Edvardsson D. Person-centredness and its association with resident well-being in dementia care units. Journal of Advanced Nursing. 2013;69(10):2196-2205. doi:10.1111/jan.12085
- U.S. Nursing Assistants Employed in Nursing Homes: Key Facts. Paraprofessional Healthcare Institute; 2019:1-12. https://www.phinational.org/wp-content/uploads/2019/08/US-Nursing-Assistants-2019-PHI.pdf
- Nursing Assistants. U.S. Bureau of Labor Statistics. May 2023. https://www.bls.gov/oes/2023/may/oes311131.htm
- Shield RR, Looze J, Tyler D, Lepore M, Miller SC. Why and How Do Nursing Homes Implement Culture Change Practices? Insights From Qualitative Interviews in a Mixed Methods Study. Journal of Applied Gerontology. 2013;33(6):737-763. doi: https://doi.org/10.1177/0733464813491141
- Jenkens R, Sult T, Lessell N, Hammer D, Ortigara A. Financial Implications of THE GREEN HOUSE® Model Overview. Seniors Housing & Care Journal. 2011;19(1). https://www.nic.org/news-press/paper-examines-green-house-models-financial-viability/
- PEAK 2.0. Kansas State University Center on Aging; 2020. https://www.hhs.k-state.edu/aging/research/peak20/times/202002.pdf
- Gandhi A, Olenski A. Tunneling and Hidden Profits in Health Care. Published online June 2024. https://www.nber.org/system/files/working_papers/w32258/revisions/w32258.rev1.pdf