






Impact of Pre-sepsis PTFV1 on Atrial Fibrillation in Older Adults
Older Patients with Elevated Pre-sepsis PTFV1 Demonstrate Greater Occurrence of Atrial Fibrillation and Worse In-Hospital Outcomes
Robert T. Mankowski, PhD1; Aisha Elfasi, MD3; Carlo Custodero, MD4; Yi Lin, PhD1; Gabriela L. Ghita, PhD5; Katelyn Villani, MSc2,8; Scott C. Brakenridge, MD5,6; Tyler J. Loftus, MD5; Lyle L. Moldawer, PhD5; Philip A. Efron, MD5; Frederick A. Moore, MD5; Alexis N. Simpkins, MD, PhD3,7.
- Department of Medicine, Division of Gerontology, Geriatrics, and Palliative Care, University of Alabama at Birmingham, Birmingham, AL, USA
- Department of Physiology and Aging, College of Medicine, University of Florida, Gainesville, FL, USA
- Department of Neurology, College of Medicine, University of Florida, Gainesville, FL, USA
- Department of Interdisciplinary Medicine, Clinica Medica Geriatria “Cesare Frugoni”, University of Bari Aldo Moro, Bari, Italy
- Department of Surgery, College of Medicine, University of Florida, Gainesville, FL, USA
- Department of Surgery, University of Washington, Seattle, WA, USA
- Department of Neurology and Neurosurgery, Cedars Sinai, Los Angeles, CA
- Department of Applied Physiology and Kinesiology, College of Health and Human Performance, University of Florida, Gainesville, FL, USA
* Authors contributed equally to this work
OPEN ACCESS
PUBLISHED: 30 September 2025
CITATION: Mankowski, R., Elfasi, A., et al., 2025. Older Patients with Elevated Pre-sepsis PTFV1 Demonstrate Greater Occurrence of Atrial Fibrillation and Worse In-Hospital Outcomes. Medical Research Archives, [online] 13(9).
https://doi.org/10.18103/mra.v13i9.6970
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i9.6970
ISSN 2375-1924
Abstract
Background: Elevated P-wave terminal force in lead V1 (PTFV1) >5000 μV*ms is a predictor of atrial fibrillation and stroke in a general population. The risk for atrial fibrillation and ischemic stroke is high in sepsis but predictors are lacking.
Objectives: Analysis of a prospective, observational cohort study with subjects categorized by PTFV1 (lower and higher than 5000 μV*ms) cutoffs and by age (older and younger than 60 years old).
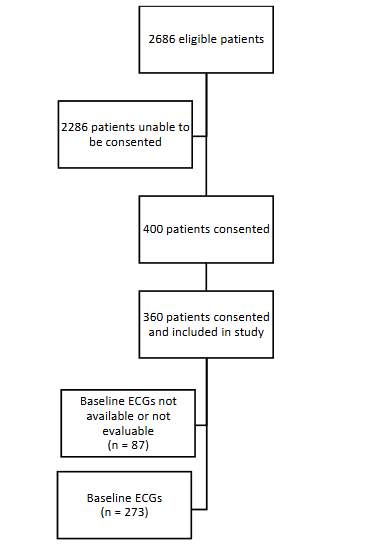
Methods: Of the 360 consented sepsis patients, 273 had evaluable pre-sepsis electrocardiograms (ECG). PTFV1 was measured by 3 independent and blinded assessors using the Mitutoyo 500-195-30CAL Absolute Digimatic Caliper on the last available ECG before sepsis onset. Patient characteristics and outcomes were compared between lower (PTFV1 < 5,000 μV*ms) and higher PTFV1 (PTFV1 > 5,000 μV*ms), and older and younger patients with elevated pre-sepsis PTFV1.
Results: The median age was 63 years [IQR 53, 71], 44% women. Median of the last ECG prior to sepsis-onset was 1 day [IQR, 0, 9]. 32% of individuals had pre-sepsis PTFV1 > 5,000 μV*ms, and were mostly females. Older patients with PTFV1 > 5,000 μV*ms had greater pre-sepsis left atrial diameter, more in-hospital new-onset atrial fibrillation, greater Charlson Comorbidity Index score, and worse clinical trajectory, compared to younger patients with PTFV1 > 5,000 μV*ms.
Conclusions: Older individuals with elevated pre-sepsis PTFV1 had greater occurrence of AF and worse outcomes during sepsis. Future studies will test pre-sepsis PTFV1 as a predictor of in-hospital and longitudinal outcomes in older sepsis patients at risk of atrial fibrillation, stroke and frailty.
Keywords: Sepsis, PTFV1, ECG, atrial fibrillation, arrhythmia, stroke
Introduction
Sepsis is one of the most common, expensive and inadequately managed syndromes in modern medicine. As a leading cause of death, sepsis accounts for >$20 billion of total hospital costs in the United States. Improved in-hospital mortality has yielded a rapidly expanding population of sepsis survivors who develop chronic critical illness characterized by the persistent organ dysfunction requiring prolonged intensive care unit (ICU) stay. Chronic critical illness frequently manifests thereafter as low-grade systemic inflammation, immunosuppression and muscle catabolic state. Our group has labeled this condition as the persistent inflammation, immunosuppression and catabolism syndrome (PICS). Sepsis survivors, especially older adults, are often discharged to long-term acute care facilities, where they experience dismal outcomes, sepsis recidivism, and ~40% post-discharge mortality in 1 year. Sepsis patients often suffer long-term new-onset and/or exacerbating health problems such as physical, cognitive and cardiovascular dysfunctions. Early detection of some of these dysfunctions during hospitalization, may result in better clinical management and alleviation of long-term health impairments. Sepsis patients are at high risk of acute and long-term cardiovascular events, such as ischemic stroke. Cardiac arrhythmias such as atrial fibrillation often occur during sepsis and persist after hospital discharge in approximately 50% of patients. Incidence of atrial fibrillation in sepsis patients has been reported to range from 5 to 23% and has been associated with increased cardioembolic risk. Occurrence of atrial fibrillation greatly increases the risk of stroke, especially in frail older adults. There is a need of predictors of atrial fibrillation in early sepsis in order to identify patients at risk of stroke. Atrial fibrillation electrocardiogram (ECG) markers of the left atrial abnormality, including the P-wave terminal force in lead V1 (PTFV1), have been recognized as easily accessible and clinically relevant predictors of the left atrial dysfunction. PTFV1 abnormalities are associated with the risk of ischemic stroke regardless of previous history of atrial fibrillation. PTFV1 >5000 μV*ms has been shown as a predictor of atrial fibrillation and ischemic stroke. According to The AtRial Cardiopathy and Antithrombotic Drugs In prevention After cryptogenic stroke (ARCADIA) trial, atrial cardiopathy was defined as the presence of 1 or more of the following: PTFV1>5000 μV*ms, serum NT-proBNP>250pg/mL or left atrial diameter index ≥3 cm/m2 on echocardiogram. These thresholds were chosen based on approximately doubled risk of stroke or stroke recurrence in observational studies. In this manuscript, we analyzed available pre-sepsis ECGs in a cohort of sepsis patients to characterize in-hospital outcomes of patients with elevated pre-sepsis PTFV1. We hypothesized that older patients with pre-sepsis PTFV1>5000 μV*ms will have worse in-hospital outcomes and greater occurrence of new-onset atrial fibrillation during sepsis.
Methods
SEPSIS COHORT.
We performed an analysis of a prospective, observational cohort study conducted over four years ending December 31, 2018 that enrolled surgical ICU patients with new onset sepsis. This study was conducted by the University of Florida Sepsis Critical Illness Research Center in collaboration with the UF Institute on Aging. Patients were recruited from the trauma and surgical ICUs (each with 24 beds) at the UF Health Shands Hospital (Gainesville, Florida; U.S.A.). Each ICU has a dedicated multidisciplinary ICU team that use established clinical protocols. The main study (Persistent Inflammation, Immunosuppression and Catabolism Syndrome (PICS): A New Horizon for Surgical Critical Care) was approved by the University of Florida Institutional Review Board (#IRB201400611) on 10/28/2014 and registered with clinicaltrials.gov (NCT02276417). Procedures were followed in accordance with the ethical standards of the responsible committee on human experimentation (institutional or regional) and with the Helsinki Declaration of 1975. All subjects signed a written informed consent before participation in the study. The patient or legally authorized representative provided informed consent within 96 hours after the patient qualified for study inclusion. If not obtained within 96 hours, all patient data and biological samples were destroyed. Details of the study design with inclusion and exclusion criteria as well as the clinical and laboratory standard operating procedure utilized have been previously documented. In brief, overall cohort inclusion criteria included (1) age ≥ 18 years; (2) clinical diagnosis of sepsis as defined by 2001 consensus guidelines; and (3) entrance into an electronic medical record evidence-based sepsis standard operating procedures. Exclusion criteria eliminated patients whose baseline immunosuppression, end-stage comorbidities, or severe injuries would be a primary determinant of their long-term outcomes and thus confound outcome assessment. The clinical course of study patients was prospectively documented by experienced research nurses using an established sepsis database. The diagnosis of sepsis, site of infection and initial sepsis severity of each case was adjudicated weekly by a team of bedside clinicians. Organ dysfunction progression was assessed by serial Sequential Organ Failure Assessment (SOFA) scores. Patients were classified by three pre-determined in-patient clinical trajectories: 1) early death, 2) rapid recovery and 3) chronic critical illness. Early death was defined as death within 14 days of sepsis onset. Chronic critical illness was defined as an ICU stay greater than or equal to 14 days with evidence of persistent organ dysfunction by SOFA. Rapid recovery patients were those not meeting criteria for early death or chronic critical illness. Our age cutoff of 60 years old was based on the evidence that mortality after trauma increases at the age of 60 years of age.
ELECTROCARDIOGRAM ANALYSES.
Electrocardiograms were analyzed before (most recent ECG prior to enrollment in the study) and after sepsis onset or the first ECG obtained during hospital admission). PTFV1 is defined as the measurement of the depth of the downward deflection of the P-wave in lead V1 multiplied by the duration of this downward wave in milliseconds. Measurements were conducted manually by three blinded investigators using Mitutoyo 500-195-30CAL Absolute Digimatic Caliper and PTFV1 was calculated standardizing it with an ECG correction factor based on printout parameters. PTFV1 values were averaged to yield the final PTFV1 average values. PTFV1 values greater than 5000 µV*ms have been designated as elevated PTFV1. We divided the cohort by the cutoff of 5000 μV*ms according to the ARCADIA trial. Charts were screened for occurrence of atrial fibrillation and atrial fibrillation with rapid ventricular response prior to or after enrollment in sepsis protocol. Transthoracic echocardiograms conducted after sepsis onset were identified to calculate the left atrial diameter.
STATISTICAL ANALYSES.
Fisher exact test and the Kruskal–Wallis test were used for comparison of categorical and continuous variables, respectively. All significance tests were 2-sided, with p-value ≤0.05 considered statistically significant. Statistical analyses were performed with SAS version 9.4 (SAS Institute, Cary, NC, U.S.A.).
Results
DEMOGRAPHIC AND IN-HOSPITAL INFORMATION.
Out of 360 patients, 273 patients had evaluable pre-sepsis ECGs (median age: 63 years old, 44% women, and 88% White) (Figure 1). Eighty-seven ECGs were not evaluable due to poor recording quality. The most recent ECG before sepsis onset was analyzed, median 1 day [interquartile range, IQR, 0, 9]. Sixty-three percent had hypertension, 12% had a pre-existing atrial fibrillation diagnosis, and 12% reported prior ischemic stroke. Median ICU stay was 8 days [IQR 3, 17] and hospital mortality was 9%. New-onset atrial fibrillation during sepsis occurred in 27 patients. There were in total 13 (5%) post-sepsis onset ischemic strokes.
PRE-SEPSIS PTFV1 COHORT CHARACTERISTICS.
There were 32% of individuals with pre-sepsis PTFV1>5000 μV*ms, mostly females. Only 17 % of patients with PTFV1>5000 μV*ms had history of coronary artery disease as compared to 31% of patients with PTFV1<5000 μV*ms. Individuals with PTFV1>5000 μV*ms had marginally shorter (p=0.06) hospital length of stay and lower (p=0.06) left atrial (LA) diameter index median 3.5 [IQR 3, 4] compared to median 3.8 [IQR 3.3, 4.2]. Among patients with pre-sepsis PTFV1> 5000 μV*ms, new-onset in-hospital atrial fibrillation occurred in 17% of patients as compared to 24% among those with PTFV1 < 5000 μV*ms (p=0.0007).
| Variables | Total Population (n=273) | PS PTFV1 > 5000 μV*ms (n=86) | PS PTFV1 < 5000 μV*ms (n=187) | P-value |
|---|---|---|---|---|
| Age – years (median, IQR) | 63 (53, 71) | 61 (53, 67) | 64 (53, 72) | 0.07 |
| Female sex – no. (%) | 121 (44) | 51 (59) | 70 (37) | 0.001 |
| Race or ethnic group – no. (%) | 0.52 | |||
| White | 240 (86) | 73 (85) | 167 (88) | |
| Black | 29 (10) | 13 (15) | 16 (8) | |
| American Indian | 1 (1) | 0 (0) | 1 (1) | |
| Asian | 1 (1) | 0 (0) | 1 (1) | |
| Other | 1 (1) | 0 (0) | 1 (1) | |
| Unknown | 1 (1) | 0 (0) | 1 (1) | |
| Hispanic – no. (%) | 6 (2) | 0 (0) | 6 (3.2) | 0.18 |
| Hypertension – no. (%) | 173 (63) | 54 (63) | 119 (64) | 0.95 |
| Diabetes – no (%) | 82 (30) | 26 (30) | 56 (30) | 1 |
| Coronary Artery Disease – no. (%) | 71 (26) | 14 (16) | 57 (31) | 0.02 |
| Congestive Heart Failure – no. (%) | 36 (13) | 10 (12) | 26 (14) | 0.70 |
| History of Stroke – no. (%) | 32 (12) | 7 (8) | 25 (13) | 0.21 |
| Tobacco Use – no. (%) | 114 (42) | 34 (40) | 80 (43) | 0.68 |
| Alcohol Use – no. (%) | 52 (19) | 15 (17) | 37 (20) | 0.76 |
| Atrial Fibrillation – no. (%) | 29 (12) | 7 (8) | 22 (13) | 0.40 |
| Body Mass Index (median, IQR) | 29.5 (24.8, 37.2) | 28.4 (25.1, 35.7) | 29.7 (24.7, 37.8) | 0.43 |
| Baseline LA diameter (cm) (median, IQR) | 3.7 (3.2, 4.2) | 3.5 (3, 4) | 3.8 (3.3, 4.2) | 0.06 |
| In-hospital Characteristics | ||||
| BNP (median, IQR) | 1397 (604, 4887) | 1397 (588, 4887) | 1420 (609.5, 4901.5) | 0.84 |
| Charlson Comorbidity Index (median, IQR) | 3 (2, 5) | 3 (1, 4) | 3 (2, 5) | 0.32 |
| Length of stay (days) (median, IQR) | 17 (8, 28) | 13 (7, 25) | 17 (9, 29) | 0.06 |
| ICU- Length of Stay (days) (median, IQR) | 8 (3, 17) | 6.5 (2, 17) | 9 (4, 18) | 0.08 |
| In-hospital Mortality – no. (%) | 24 (9) | 4 (5) | 20 (11) | 0.11 |
| Maximum SOFA Score (median, IQR) | 8 (5, 10) | 7 (5, 10) | 8 (6, 11) | 0.09 |
| Clinical trajectory – no. (%) | 0.71 | |||
| Early Death | 9 (3) | 2 (2) | 7 (4) | |
| CCI | 100 (37) | 29 (34) | 71 (38) | |
| RAP | 164 (60) | 55 (64) | 109 (58) | |
| Post enrollment atrial fibrillation – no. (%) | 59 (22) | 15 (17) | 44 (24) | 0.001 |
CHARACTERISTICS OF YOUNGER AND OLDER PATIENTS WITH ELEVATED PTFV1.
Individuals 60 years and older with PTFV1>5000 μV*ms had marginally higher SOFA score and higher Charlson Comorbidity Index and were marginally more often type 2 diabetic, and worse clinical trajectory i.e. more early death and chronic critical illness. Twenty-nine percent of older sepsis patients with pre-sepsis PTFV1>5000 μV*ms had new-onset post-sepsis atrial fibrillation compared to 3% among younger individuals. Pre-sepsis left atrial diameter was greater among older individuals compared to patients <60 years old.
| Variables | PS PTFV1 > 5000 μV*ms >60 years old (n=48) | PS PTFV1 > 5000 μV*ms <60 years old (n=187) | P-value |
|---|---|---|---|
| Age – years (median, IQR) | 66 (63, 71) | 51 (43, 56) | <0.0001 |
| Female sex – no. (%) | 25 (52) | 26 (68) | 0.18 |
| Race or ethnic group – no. (%) | 0.23 | ||
| White | 43 (90) | 30 (79) | |
| Black | 5 (10) | 8 (21) | |
| American Indian | 0 (0) | 0 (0) | |
| Asian | 0 (0) | 0 (0) | |
| Other | 0 (0) | 0 (0) | |
| Unknown | 0 (0) | 0 (0) | |
| Hispanic – no. (%) | 0 (0) | 0 (0) | 0.18 |
| Hypertension – no. (%) | 34 (71) | 20 (53) | 0.12 |
| Diabetes – no (%) | 19 (40) | 7 (18) | 0.06 |
| Coronary Artery Disease – no. (%) | 10 (21) | 4 (11) | 0.25 |
| Congestive Heart Failure – no. (%) | 8 (17) | 2 (5) | 0.17 |
| History of Stroke – no. (%) | 5 (10) | 2 (5) | 0.46 |
| Tobacco Use – no. (%) | 19 (40) | 15 (40) | 1 |
| Alcohol Use – no. (%) | 10 (13) | 5 (13) | 0.39 |
| Atrial Fibrillation – no. (%) | 6 (8) | 1 (3) | 0.13 |
| Body Mass Index (median, IQR) | 27.5 (24.3, 33.3) | 29.6 (25.6, 39.4) | 0.21 |
| Baseline LA diameter (cm/m2) (median, IQR) | 3.9 (3.4, 4.3) | 3.2 (2.8, 3.6) | 0.002 |
| In-hospital Characteristics | |||
| BNP (median, IQR) | 1741.5 (588, 5651) | 859 (475.5, 3121.5) | 0.34 |
| Charlson Comorbidity Index (median, IQR) | 4 (3, 6) | 1 (0, 2) | <0.0001 |
| Length of stay (days) (median, IQR) | 14 (8.5, 25.5) | 10.5 (7, 24) | 0.30 |
| ICU- Length of Stay (days) (median, IQR) | 9.5 (3, 18.5) | 5.5 (2, 14) | 0.15 |
| In-hospital Mortality – no. (%) | 3 (6) | 1 (3) | 0.63 |
| Maximum SOFA Score (median, IQR) | 8 (6, 10.5) | 6.5 (4, 9) | 0.06 |
| Clinical trajectory – no. (%) | 0.71 | ||
| Early Death | 2 (4.2) | 0 (0) | |
| CCI | 20 (42) | 9 (24) | |
| RAP | 26 (54) | 29 (76) | |
| New-onset atrial fibrillation – no. (%) | 14 (29) | 1 (3) | 0.001 |
Discussion
The main findings of this study were that PTFV1 was greater than 5000 μV*ms in approximately a third of individuals before sepsis onset (32%), which was nearly three-fold compared to a number of individuals with atrial fibrillation diagnosis (12%). In the total cohort, the occurrence of post-sepsis onset atrial fibrillation was greater among patients with PTFV1<5000 μV*ms. However, when comparing individuals >60 to <60 years old, older patients with elevated pre-sepsis PTFV1 had greater pre-sepsis left atrial diameter, more new-onset atrial fibrillation after sepsis onset, and worse in-hospital outcomes and clinical trajectory compared to individuals <60 years old. Twenty-two percent of new-onset atrial fibrillation in our cohort of mostly older sepsis patients are in line with others being between 2-26% in sepsis and 40% in septic shock. Recent results from the United Kingdom retrospective electronic health record study demonstrated that sepsis patients with a new-onset atrial fibrillation (n=7,691) were older, were mostly male and had more cardiovascular, renal and pulmonary comorbidities than sepsis patients without new-onset atrial fibrillation (n=24,506). Sepsis patients with atrial fibrillation had also longer hospital stay, greater risk for septic shock and in-hospital and post-discharge mortality. Thus, identification of clinically meaningful biomarkers would potentially improve early clinical management as well as alleviation of long-term health consequences. Our results demonstrating greater occurrence of atrial fibrillation and worse clinical outcomes in a cohort of patients who had pre-sepsis PTFV1<5000 μV*ms are not in line with the findings of others. Reports to date have shown that PTFV1>5000 μV*ms was an ECG biomarker predictive of atrial fibrillation and long-term ischemic stroke. These results were unexpected, but after dividing the cohort of patients with elevated pre-sepsis PTFV1 into older and younger than 60 years, because of a strong age effect on sepsis and atrial fibrillation risk, we found that older adults with elevated pre-sepsis PTFV1 have worse in-hospital outcomes and greater occurrence of new-onset atrial fibrillation compared to patients younger than 60 years old. Others have found that P wave duration at the upper fifth percentile was associated with long-term atrial fibrillation risk in older adults. Atrial fibrillation and stroke are more prevalent in older adults and overall in-hospital outcomes are worse in older age, thus our results indicate that in our cohort, older adults with elevated pre-sepsis PTFV1 had greater pre-sepsis left atrial diameter and occurrence of atrial fibrillation, and worse clinical outcomes in sepsis. To our knowledge, this is the first report suggesting that older adults with elevated pre-sepsis PTFV1 may be at risk of new-onset atrial fibrillation and poor outcomes in response to sepsis. Additionally, our general patient cohort with elevated pre-sepsis PTFV1 comprised majority of females. Females have a uniquely better response to sepsis than males, where protective effects of sex hormones and predominance of anti-inflammatory mediators may play a role. Sex differences in PTFV1 as a predictor of outcomes in sepsis warrant further investigation. Our findings should be interpreted in the light of recent evidence suggesting elevated PTFV1 values as a very early marker of atrial cardiomyopathy, but not indicative of the irreversible structural remodeling. Thus, given the recognized higher long-term risk of atrial fibrillation and ischemic stroke among older sepsis patients, PTFV1 might serve as a useful marker to guide clinical decision-making, for example anticoagulant therapy and modulating fluid overload during resuscitation. For example, in pre-dialysis patients, elevated PTFV1 was associated with higher thoracic fluid content. ECG-based markers of atrial function could be useful in sepsis because, for example, during hypovolemia related to septic shock, fluid overload while maintaining arterial pressures may cause atrial stretch which is associated with a higher incidence atrial fibrillation. Additionally, vasopressor therapy such as catecholamines used to maintain arterial blood pressure were also associated with a higher incidence of atrial fibrillation which could be through mechanisms such as adrenergic stimulation of alpha and beta receptors. This study has several limitations. First, the manual measurements of PTFV1 could introduce inter-assessor error, however having 3 independent assessors and a digital caliper reduce the inter-assessor error risk. Second, we have not accounted for the potential effect of other factors that may have contributed to acute hemodynamic changes during sepsis (e.g., fluid resuscitation) which might have had an effect PTFV1 values. In this study, we were focused on characterizing the sepsis patients based on their pre-sepsis PTFV1 values. Future studies will focus on pre-sepsis and early sepsis PTFV1 values as predictors of in-hospital and long-term atrial fibrillation and ischemic stroke outcomes as well as markers of clinical decision-making guiding fluid resuscitation and vasopressor therapy in sepsis-induced hypovolemia.
Conclusions
In conclusion, older individuals with elevated pre-sepsis PTFV1 had greater occurrence of new-onset atrial fibrillation and worse clinical outcomes during sepsis compared with younger patients with elevated pre-sepsis PTFV1. Future studies will test pre-sepsis PTFV1 as a predictor of in-hospital and longitudinal outcomes in older sepsis patients at risk of atrial fibrillation, ischemic stroke and frailty.
Clinical perspective
Atrial fibrillation is associated with increased morbidity and mortality as it is associated with the risk of heart failure and ischemic stroke. Identifying individuals at higher risk of developing atrial fibrillation is important to allow for early detection and optimization of medical management of the condition. Our study found that older patients diagnosed with sepsis were at higher risk of developing atrial fibrillation.
Conflicts of Interest Statement
The authors declare that they have no relevant conflicts of interests.
Funding Statement
This work was supported, in part, by the following National Institutes of Health grants: R01 GM-113945 (PAE), R01 GM-040586 and R01 GM-104481 (LLM), and P50 GM-111152 (FAM, LLM, PAE), awarded by the National Institute of General Medical Sciences (NIGMS). Finally, the work was supported, in part, by American Heart Association grant 18CDA34080001 (RTM).
Acknowledgments
We would like to thank the University of Florida Sepsis and Critical Illness Research Center for the access to the study database and patient electronic health records.
Author’s contribution:
Conceptualization, manuscript writing: RTM, AE, CC, ANS Data generation: AE, KV Statistical analyses: GLG Review: YL, SCB, TJL, LLM, PAE, FAM, ANS Clinical study registration: Clinicaltrials.gov (NCT02276417)
References
- Angus DC, van der Poll T. Severe sepsis and septic shock. N Engl J Med. 2013;369:2063. doi: 10.1056/NEJMc1312359
- Gaieski DF, Edwards JM, Kallan MJ, Carr BG. Benchmarking the incidence and mortality of severe sepsis in the United States. Crit Care Med. 2013;41:1167-1174. doi: 10.1097/CCM.0b013e31827c09f8
- Torio CM, Moore BJ. National Inpatient Hospital Costs: The Most Expensive Conditions by Payer, 2013: Statistical Brief #204. In: Healthcare Cost and Utilization Project (HCUP) Statistical Briefs. Rockville (MD); 2006.
- Gentile LF, Cuenca AG, Efron PA, Ang D, Bihorac A, McKinley BA, Moldawer LL, Moore FA. Persistent inflammation and immunosuppression: a common syndrome and new horizon for surgical intensive care. J Trauma Acute Care Surg. 2012;72:1491-1501. doi: 10.1097/TA.0b013e318256e000
- Horiguchi H, Loftus TJ, Hawkins RB, Raymond SL, Stortz JA, Hollen MK, Weiss BP, Miller ES, Bihorac A, Larson SD, et al. Innate Immunity in the Persistent Inflammation, Immunosuppression, and Catabolism Syndrome and Its Implications for Therapy. Front Immunol. 2018;9:595. doi: 10.3389/fimmu.2018.00595
- Mathias B, Delmas AL, Ozrazgat-Baslanti T, Vanzant EL, Szpila BE, Mohr AM, Moore FA, Brakenridge SC, Brumback BA, Moldawer LL, et al. Human Myeloid-derived Suppressor Cells are Associated With Chronic Immune Suppression After Severe Sepsis/Septic Shock. Ann Surg. 2017;265:827-834. doi: 10.1097/SLA.0000000000001783
- Hollen MK, Stortz JA, Darden D, Dirain ML, Nacionales DC, Hawkins RB, Cox MC, Lopez MC, Rincon JC, Ungaro R, et al. Myeloid-derived suppressor cell function and epigenetic expression evolves over time after surgical sepsis. Crit Care. 2019;23:355. doi: 10.1186/s13054-019-2628-x
- Stortz JA, Murphy TJ, Raymond SL, Mira JC, Ungaro R, Dirain ML, Nacionales DC, Loftus TJ, Wang Z, Ozrazgat-Baslanti T, et al. Evidence for Persistent Immune Suppression in Patients Who Develop Chronic Critical Illness After Sepsis. Shock. 2018;49:249-258. doi: 10.1097/SHK.0000000000000981
- Goodwin AJ, Rice DA, Simpson KN, Ford DW. Frequency, cost, and risk factors of readmissions among severe sepsis survivors. Crit Care Med. 2015;43:738-746. doi: 10.1097/CCM.0000000000000859
- Stortz JA, Mira JC, Raymond SL, Loftus TJ, Ozrazgat-Baslanti T, Wang Z, Ghita GL, Leeuwenburgh C, Segal MS, Bihorac A, et al. Benchmarking clinical outcomes and the immunocatabolic phenotype of chronic critical illness after sepsis in surgical intensive care unit patients. J Trauma Acute Care Surg. 2018;84:342-349. doi: 10.1097/TA.0000000000001758
- Brakenridge SC, Efron PA, Cox MC, Stortz JA, Hawkins RB, Ghita G, Gardner A, Mohr AM, Anton SD, Moldawer LL, et al. Current Epidemiology of Surgical Sepsis: Discordance Between Inpatient Mortality and 1-year Outcomes. Ann Surg. 2019;270:502-510. doi: 10.1097/SLA.0000000000003458
- Proietti M, Romiti GF, Raparelli V, Diemberger I, Boriani G, Dalla Vecchia LA, Bellelli G, Marzetti E, Lip GY, Cesari M. Frailty prevalence and impact on outcomes in patients with atrial fibrillation: A systematic review and meta-analysis of 1,187,000 patients. Ageing Res Rev. 2022;79:101652. doi: 10.1016/j.arr.2022.101652
- Mankowski RT, Yende S, Angus DC. Long-term impact of sepsis on cardiovascular health. Intensive Care Med. 2019;45:78-81. doi: 10.1007/s00134-018-5173-1
- Iwashyna TJ, Ely EW, Smith DM, Langa KM. Long-term cognitive impairment and functional disability among survivors of severe sepsis. JAMA. 2010;304:1787-1794. doi: 10.1001/jama.2010.1553
- Patel N, Bajaj NS, Doshi R, Gupta A, Kalra R, Singh A, Berra L, Arora G, Prabhu SD, Arora P. Cardiovascular Events and Hospital Deaths Among Patients With Severe Sepsis. Am J Cardiol. 2019;123:1406-1413. doi: 10.1016/j.amjcard.2019.01.038
- Induruwa I, Hennebry E, Hennebry J, Thakur M, Warburton EA, Khadjooi K. Sepsis-driven atrial fibrillation and ischaemic stroke. Is there enough evidence to recommend anticoagulation? Eur J Intern Med. 2022;98:32-36. doi: 10.1016/j.ejim.2021.10.022
- Walkey AJ, Hammill BG, Curtis LH, Benjamin EJ. Long-term outcomes following development of new-onset atrial fibrillation during sepsis. Chest. 2014;146:1187-1195. doi: 10.1378/chest.14-0003
- Walkey AJ, Wiener RS, Ghobrial JM, Curtis LH, Benjamin EJ. Incident stroke and mortality associated with new-onset atrial fibrillation in patients hospitalized with severe sepsis. JAMA. 2011;306:2248-2254. doi: 10.1001/jama.2011.1615
- Hancock EW, Deal BJ, Mirvis DM, Okin P, Kligfield P, Gettes LS, Bailey JJ, Childers R, Gorgels A, Josephson M, et al. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: part V: electrocardiogram changes associated with cardiac chamber hypertrophy: a scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society. Endorsed by the International Society for Computerized Electrocardiography. J Am Coll Cardiol. 2009;53:992-1002. doi: 10.1016/j.jacc.2008.12.015
- He J, Tse G, Korantzopoulos P, Letsas KP, Ali-Hasan-Al-Saegh S, Kamel H, Li G, Lip GYH, Liu T. P-Wave Indices and Risk of Ischemic Stroke: A Systematic Review and Meta-Analysis. Stroke. 2017;48:2066-2072. doi: 10.1161/STROKEAHA.117.017293
- Kamel H, Bartz TM, Elkind MSV, Okin PM, Thacker EL, Patton KK, Stein PK, deFilippi CR, Gottesman RF, Heckbert SR, et al. Atrial Cardiopathy and the Risk of Ischemic Stroke in the CHS (Cardiovascular Health Study). Stroke. 2018;49:980-986. doi: 10.1161/STROKEAHA.117.020059
- Jalini S, Rajalingam R, Nisenbaum R, Javier AD, Woo A, Pikula A. Atrial cardiopathy in patients with embolic strokes of unknown source and other stroke etiologies. Neurology. 2019;92:e288-e294. doi: 10.1212/WNL.0000000000006748
- Kamel H, Longstreth WT, Jr., Tirschwell DL, Kronmal RA, Broderick JP, Palesch YY, Meinzer C, Dillon C, Ewing I, Spilker JA, et al. The AtRial Cardiopathy and Antithrombotic Drugs In prevention After cryptogenic stroke randomized trial: Rationale and methods. Int J Stroke. 2019;14:207-214. doi: 10.1177/1747493018799981
- Loftus TJ, Mira JC, Ozrazgat-Baslanti T, Ghita GL, Wang Z, Stortz JA, Brumback BA, Bihorac A, Segal MS, Anton SD, et al. Sepsis and Critical Illness Research Center investigators: protocols and standard operating procedures for a prospective cohort study of sepsis in critically ill surgical patients. BMJ Open. 2017;7:e015136. doi: 10.1136/bmjopen-2016-015136
- Campbell-Furtick M, Moore BJ, Overton TL, Laureano Phillips J, Simon KJ, Gandhi RR, Duane TM, Shafi S. Post-trauma mortality increase at age 60: a cutoff for defining elderly? Am J Surg. 2016;212:781-785. doi: 10.1016/j.amjsurg.2015.12.018
- Hunter MD, Park Moon Y, DeCarli C, Gutierrez J, Wright CB, Di Tullio MR, Sacco RL, Kamel H, Elkind MSV. Electrocardiographic left atrial abnormality and silent vascular brain injury: The Northern Manhattan Study. PLoS One. 2018;13:e0203774. doi: 10.1371/journal.pone.0203774
- Huo Y, Yoshimura H, Gonzalez-Izquierdo A, Lip GYH, Schmidt F, Providencia R. Risk Factors and Prognosis of New-Onset Atrial Fibrillation in Sepsis: A Nationwide Electronic Health Record Study. JACC Adv. 2025;4:101681. doi: 10.1016/j.jacadv.2025.101681
- Kwon Y, McHugh S, Ghoreshi K, Lyons GR, Cho Y, Bilchick KC, Mazimba S, Worrall BB, Akoum N, Chen LY, et al. Electrocardiographic left atrial abnormality in patients presenting with ischemic stroke. J Stroke Cerebrovasc Dis. 2020;29:105086. doi: 10.1016/j.jstrokecerebrovasdis.2020.105086
- Ning Y, Wei M, Song W, Luo G. The Relationship Between Atrial Cardiopathy Biomarkers and Prognosis of Patients With Embolic Stroke of Undetermined Source. Front Cardiovasc Med. 2022;9:829361. doi: 10.3389/fcvm.2022.829361
- Kamel H, Hunter M, Moon YP, Yaghi S, Cheung K, Di Tullio MR, Okin PM, Sacco RL, Soliman EZ, Elkind MS. Electrocardiographic Left Atrial Abnormality and Risk of Stroke: Northern Manhattan Study. Stroke. 2015;46:3208-3212. doi: 10.1161/STROKEAHA.115.009989
- Magnani JW, Johnson VM, Sullivan LM, Gorodeski EZ, Schnabel RB, Lubitz SA, Levy D, Ellinor PT, Benjamin EJ. P wave duration and risk of longitudinal atrial fibrillation in persons >/= 60 years old (from the Framingham Heart Study). Am J Cardiol. 2011;107:917-921 e911. doi: 10.1016/j.amjcard.2010.10.075
- Barter J, Kumar A, Stortz JA, Hollen M, Nacionales D, Efron PA, Moldawer LL, Foster TC. Age and Sex Influence the Hippocampal Response and Recovery Following Sepsis. Mol Neurobiol. 2019;56:8557-8572. doi: 10.1007/s12035-019-01681-y
- Lopez MC, Efron PA, Ozrazgat-Baslanti T, Zhang J, Cuschieri J, Maier RV, Minei JP, Baker HV, Moore FA, Moldawer LL, et al. Sex-based differences in the genomic response, innate immunity, organ dysfunction, and clinical outcomes after severe blunt traumatic injury and hemorrhagic shock. J Trauma Acute Care Surg. 2016;81:478-485. doi: 10.1097/TA.0000000000001113
- Lebek S, Wester M, Pec J, Poschenrieder F, Tafelmeier M, Fisser C, Provaznik Z, Schopka S, Debl K, Schmid C, et al. Abnormal P-wave terminal force in lead V1 is a marker for atrial electrical dysfunction but not structural remodelling. ESC Heart Fail. 2021. doi: 10.1002/ehf2.13488
- Walkey AJ, Quinn EK, Winter MR, McManus DD, Benjamin EJ. Practice Patterns and Outcomes Associated With Use of Anticoagulation Among Patients With Atrial Fibrillation During Sepsis. JAMA Cardiol. 2016;1:682-690. doi: 10.1001/jamacardio.2016.2181
- Jaroszynski A, Jaroszynska A, Dabrowski W, Zaborowski T, Stepulak A, Ilzecki M, Zubilewicz T. Factors influencing P terminal force in lead V1 of the ECG in hemodialysis patients. Arch Med Sci. 2018;14:257-264. doi: 10.5114/aoms.2017.65926
- Dunser MW, Hasibeder WR. Sympathetic overstimulation during critical illness: adverse effects of adrenergic stress. J Intensive Care Med. 2009;24:293-316. doi: 10.1177/0885066609340519
- Schmittinger CA, Torgersen C, Luckner G, Schroder DC, Lorenz I, Dunser MW. Adverse cardiac events during catecholamine vasopressor therapy: a prospective observational study. Intensive Care Med. 2012;38:950-958. doi: 10.1007/s00134-012-2531-2