






Impact of SSA Autoantibodies on Thyroid Hormones in MCTD
SSA autoantibodies associated with severely decreased free thyroxine levels in systemic autoimmune mixed connective tissue disease
Dr. Ildikó Molnár, Ph.D.,1 Dr. Edit Bodolay, D.Sc.2
- Immunoendocrinology, EndoMed, Debrecen, Hungary
- University of Debrecen, Institute of Internal Medicine, Department of Clinical Immunology, Debrecen, Hungary
ORCID ID: 0000-0001-8375-0357
OPEN ACCESS
PUBLISHED: 31 December 2024
CITATION: Molnár, I., and Bodolay, E., 2024. SSA autoantibodies associated with severely decreased free thyroxine levels in systemic autoimmune mixed connective tissue disease. Medical Research Archives, [online] 12(12). https://doi.org/10.18103/mra.v12i12.6066
COPYRIGHT © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i12.6066
ISSN 2375-1924
Abstract
Background: Mixed connective tissue disease (MCTD) is a systemic autoimmune disease with variable symptoms and autoantibodies. Antinuclear antibody positivity is more common in autoimmune thyroid diseases with higher levels of antibodies to thyroid peroxidase (TPO) or thyroglobulin (Tg) leading to elevated TSH levels. Intracellular SSA autoantibodies have a direct role in tissue damage with a prevalence of 33% in MCTD.
Aims: To investigate the role of SSA autoantibodies in thyroid autoimmunity in MCTD patients. The effect of SSA autoantibodies on thyroid hormone levels was investigated in the presence and absence of thyroid autoimmunity.
Methods: Thirty-three patients with MCTD [41±10 years, 32 females and 1 male] and 34 healthy controls [33±14 years, 30 females and 4 males] were studied. Thyroid hormones (TSH, FT4 and FT3) were measured by luminescence immunoassay. Enzyme-linked immunosorbent assay was used for the detection of anti-TPO and anti-Tg autoantibodies. Biochemical data are presented as geometric mean with 95% confidence interval except for age and FT3/FT4 ratio, which are presented as mean±SD.
Results: Significant differences in age and serum FT4 levels were observed between MCTD patients and controls (41±10 vs. 33±14 years, p<0.0089 and 8.83(3.55-22) vs. 10.82(7.33-15.96) pmol/l, p<0.0229, respectively). The difference in serum TSH and FT4 levels was significant between SSA autoantibody positive MCTD patients and controls [2.43(0.42-13.96) vs. 1.63(0.75-3.53) mIU/ml, p<0.0405 for TSH, 6.59(2.22-19.53) vs. 10.82(7.33-15.96) pmol/l, p<0.0001 for FT4]. The greater decrease in serum FT4 levels could be demonstrated by the presence of SSA in combination with anti-Tg [3.74(1.37-10.18) vs. 11.05(8.57-14.24) pmol/l, p<0.001] or anti-TPO autoantibodies [4.68(1.65-13.28) vs. 11.75(6.05-22.8) pmol/l, p<0.0001] compared to those thyroid antibodies alone.
Conclusions: Our results showed that SSA autoantibodies together with anti-TPO and/or anti-Tg autoantibodies resulted in a greater decrease in serum FT4 levels than SSA autoantibodies alone. The effect of SSA autoantibodies on FT4 levels may be manifested in the absence of thyroid autoimmunity. These results highlight the importance of screening for thyroid hormone and autoantibody levels in MCTD patients regardless of thyroid autoimmunity.
Keywords: thyroid autoimmunity; mixed connective tissue disease; SSA autoantibodies; antibodies against thyroid peroxidase and thyroglobulin; decreased FT4 serum levels
Introduction
Mixed connective tissue disease (MCTD) is a systemic autoimmune disease with multiple symptoms and autoantibodies. MCTD is a chronic autoimmune disease characterized by Raynaud’s phenomenon, polyarthritis, polymyositis, sclerodactyly, swollen hands, esophageal dysmotility, pulmonary hypertension and interstitial lung fibrosis. The above non-specific symptoms of MCTD overlap with those of other systemic autoimmune diseases such as systemic lupus erythematosus (SLE), rheumatoid arthritis (RA), dermato-polymyositis (DM-PM) and scleroderma (SSc). Anti-U1-RNP autoantibodies are considered to be the most specific autoantibodies for MCTD, although several types of antinuclear autoantibodies (ANA) against double-stranded (ds) DNA, Sm, SSA/SSB, Jo1, Scl70 and phospholipids can be detected serologically.
Thyroid dysfunction is very common in systemic autoimmune diseases: 42% of patients with rheumatoid arthritis, 46% of patients with systemic lupus erythematosus, 27% of patients with scleroderma, 50% and 43% of patients with Sjögren’s syndrome (SS) and MCTD, respectively. Hashimoto’s thyroiditis (HT) could be considered as a dominant autoimmune thyroid disease besides Graves’ disease (GD). Hashimoto’s thyroiditis was more common than Graves’ disease in MCTD (21%), Sjögren’s syndrome (7%) and rheumatoid arthritis (6%); Graves’ disease was detected in 2.5%, 3% and 1.6%, respectively. Systemic autoimmune diseases were associated with 51% of Hashimoto’s thyroiditis and 16% of Graves’ disease. The association between MCTD and Hashimoto’s thyroiditis may be based on immune complex-mediated damage to thyroid follicular cells, resulting in subclinical or manifest hypothyroidism. However, some report has shown a high prevalence of hypothyroidism in systemic lupus erythematosus and polymyositis without underlying autoimmune disease.
Anti-SSA/SSB autoantibodies are intracellular antibodies to a cytoplasmic complex of small ribonucleic acid (RNA) nucleotides. They are most commonly associated with Sjögren’s syndrome (70-100%) and systemic lupus erythematosus (40-90%). The prevalence of SSA antibodies in MCTD was 33% in the work of Setty NY. Two Ro-ribonucleoproteins (RNP, Ro52 and Ro-60) form the SSA antigens, which are localized in different cell compartments. SSA autoantibodies [SSA/Ro60 (the target for classical detection) and SSA/Ro52] play a direct role in tissue damage and are involved in proteasomal degradation. SSB (La) is also part of the Ro heterogeneous antigen complex, which is an extractable nuclear complex. SSB autoantibodies are mainly associated with primary Sjögren’s syndrome. Tests for SSA autoantibodies generally provide a common target for Ro60 and Ro52. The separate detection of autoantibodies against Ro52 and Ro60 highlights their clinical relevance in autoimmune diseases. Ro52 autoantibodies are mainly associated with inflammatory myositis. Ro60 autoantibodies are often associated with the presence of antiphospholipid antibodies.
Antinuclear antibody positivity is more common in autoimmune thyroid disease than in controls (45% vs. 14%). Antinuclear antibody positivity was associated with higher levels of anti-thyroid peroxidase (TPO) autoantibodies or elevated TSH levels.
The role of SSA autoantibodies was investigated in relation to thyroid autoimmunity in MCTD patients. The effect of SSA autoantibodies on thyroid hormone levels was investigated in the presence and absence of thyroid autoimmunity.
Patients and Methods
PATIENTS
Thirty-three patients with MCTD [41±10 years, 32 females and 1 male] and 34 healthy controls [33±14 years, 30 females and 4 males] were studied. The patients with MCTD were diagnosed and followed-up at the special clinic of the Department of Immunology, University of Debrecen. All clinical and immunological parameters were investigated at the University, except thyroid hormones and anti-TPO and anti-Tg autoantibodies. These parameters were measured from the patients’ sera at the Kenezy Hospital in 2007. The diagnosis of MCTD was based on the classification criteria of the American College of Rheumatology. Autoimmune thyroid diseases in 12 patients [10 cases of Hashimoto’s thyroiditis and 2 cases of Graves’ disease] were associated with MCTD. The diagnosis of Hashimoto’s thyroiditis was based on the presence of anti-TPO and/or anti-Tg autoantibodies. The presence of anti-TPO antibodies in 17 cases and anti-Tg antibodies in 7 cases was detected in 33 patients with MCTD. Diffuse goitre with hyperthyroidism at onset was characterized by Graves’ disease (none of the patients had ophthalmopathy). The non-specific symptoms were as follows: arthralgia in 26 cases, hand swelling in 16 cases, skin lesions in 7 cases, arthritis in 9 cases, myositis in 16 cases (confirmed by electromyography (EMG) and biopsy), Raynaud’s phenomenon in 20 cases, vasculitis in 9 cases. The presence of SSA autoantibodies was demonstrated in 12 cases and cardiac disease (all heart failure) in 12 cases. All patients with MCTD had anti-U1-RNP autoantibodies. None of the patients had SSB autoantibodies. Disease duration at the time of the study was 9±4 years.
Disease-specific therapies included methylprednisolone (2-12 mg/day), methotrexate (10-25 mg/week) and cyclophosphamide (500-1000 mg/3 weeks), as well as adalimumab, chloroquine and immunoglobulin therapies. Non-specific therapies included pentoxifylline, NSAIDs with proton pump inhibitors, acenocoumarol and low molecular weight (LMW) heparin. Patients with Hashimoto’s thyroiditis were treated with levothyroxine (50-75 ug/day), but all patients with Graves’ disease were euthyroid at the time of the study and did not require treatment.
METHODS
DETERMINATION OF SERUM THYROID HORMONE LEVELS
Thyroid hormones (TSH, FT4 and FT3) were measured by fully automated luminescence immunoassay (LIA-MAT, Byk Sangtec, Germany). Normal values were as follows: 0.3-3 mIU/l for TSH, 7.72-23.18 pmol/l for FT4 and 2.5-4.5 pg/ml for FT3. FT3 values were converted from pg/ml to pmol/l before calculation of the FT3/FT4 ratio. Anti-TPO and anti-Tg antibodies were detected by enzyme-linked immunosorbent assay (ELISA) (SIGMA, USA) at Kenézy Hospital. Autoantibodies to SSA/SSB (including both Ro60 and Ro52 proteins/La protein) and U1-RNP were detected by ELISA (Cogent Diagnostics, UK) at the University. The results were expressed as positive and negative antibody forms for SSA, anti-TPO and anti-Tg antibodies. The calculation gave a ratio of optical density for MCTD patient sera to mean optical density + 2 SD for controls. Ratios greater than 0.64 for anti-Tg antibodies and greater than 0.73 for anti-TPO antibodies were considered positive.
STATISTICS
Biochemical data are presented as geometric mean with 95% confidence interval except for age and FT3/FT4 ratio, which are presented as mean±SD. The presence of autoantibodies against TPO, Tg and SSA was considered as positive and negative. Thyroid hormones, such as serum levels of TSH, FT4 and FT3 were skewed, so their logarithms were used, which showed an approximately normal distribution. Chi-squared tests were used to compare categorical data. Two-way and three-way ANOVA were used to show the effect of SSA autoantibodies together with anti-TPO and/or anti-Tg autoantibodies on the changes in logFT4 levels, which were presented as mean with 95% confidence interval after conversion from logarithm. The general linear model was used to estimate the relationship between FT4 levels as the dependent variable and SSA, anti-TPO and anti-Tg autoantibodies as independent variables, as well as between their interactions. P values less than 0.05 were considered significant. Statistical analyses were performed using Medcalc 17.9.7. and SPSS 26.0.0. softwares.
Results
THYROID HORMONE STATUS IN PATIENTS WITH MIXED CONNECTIVE TISSUE DISEASE AND CONTROLS
The difference in age and serum FT4 levels between patients with MCTD and controls was significant (41±10 vs. 33±14 years, p<0.0089 and 8.83(3.55-22) vs. 10.82(7.33-15.96) pmol/l, p<0.0229, respectively). There was no significant difference in serum TSH and FT3 levels or FT3/FT4 ratio. The presence of SSA autoantibodies was detected in 12 out of 33 MCTD patients. Only 4 out of 12 patients with thyroid autoimmunity showed SSA autoantibodies. The presence of anti-TPO antibodies in 12 cases and anti-Tg antibodies in 6 cases was not associated with autoimmune thyroid diseases. Six cases with anti-TPO antibody positivity and 8 cases with anti-Tg antibody positivity showed SSA autoantibodies in patients with MCTD. The cut-off value of serum FT4 levels was based on the categories of SSA autoantibody positivity and negativity using receiver operating characteristic (ROC) curve analysis. The cut-off value was given at <7.91 pmol/l for FT4, Younden index: 0.6905, p<0.0013 for the area under the ROC curve (AUC).
The results showed an association between serum FT4 levels and SSA autoantibodies, the main presence of which affected FT4 levels independently of thyroid autoimmunity in MCTD.
THE EFFECT OF SSA AUTOANTIBODIES ON THYROID HORMONE LEVELS IN PATIENTS WITH MIXED CONNECTIVE TISSUE DISEASE
Serum thyroid hormone levels (TSH, FT4, FT3) and the ratio of FT3/FT4 between patients with MCTD and controls in relation to the presence of SSA autoantibodies are shown in Figure 1. The difference in serum TSH and FT4 levels, as well as the ratio of FT3/FT4, was significant between SSA autoantibody positive patients with MCTD and controls [2.43(0.42-13.96) vs. 1.63(0.75-3.53) mIU/ml for TSH, p<0.0405, 6.59(2.22-19.53) vs. 10.82(7.33-15.96) pmol/l for FT4, p<0.0001 and 0.55±0.47 vs. 0.29±0.1 for the ratio of FT3/FT4, p<0.0033]. The difference in serum FT3 levels was significantly lower in SSA autoantibody negative patients compared to controls [2.42(1.36-4.29) vs. 4.79(1.71-13.48) pg/ml, p<0.0106]. The ratio of FT3/FT4 was significantly higher in MCTD patients with SSA autoantibody positivity than negativity.
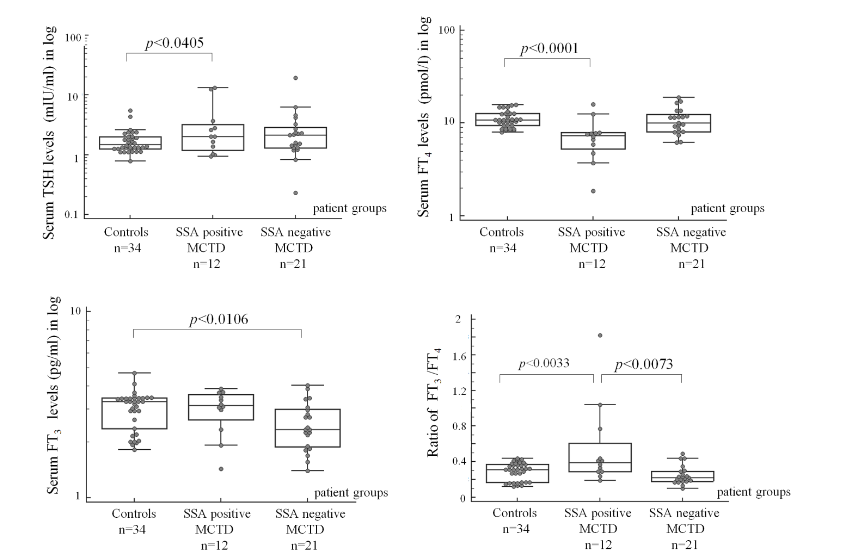
The patients with MCTD without autoimmune thyroid diseases, who were SSA autoantibody positive had slightly higher serum FT4 levels than controls [11.19(5.78-21.64) vs 10.82(7.33-15.96) pmol/l]. In MCTD, the presence of SSA autoantibodies in patients without thyroid diseases was associated with lower serum FT4 levels compared to patients with thyroid diseases who were SSA autoantibody negative [5.91(1.71-20.44) vs. 9.35(5.84-14.98) pmol/l, p<0.0762*]. The difference in FT4 levels was significant between patients with SSA autoantibody positivity and thyroid disease negativity and controls [vs. 10.82(7.33-15.96) pmol/l, p<0.0001] or patients with SSA autoantibody negativity and thyroid disease negativity (p<0.0069). Patients who were both SSA autoantibody positive and thyroid disease positive had significantly lower FT4 levels compared to controls (p<0.0164).
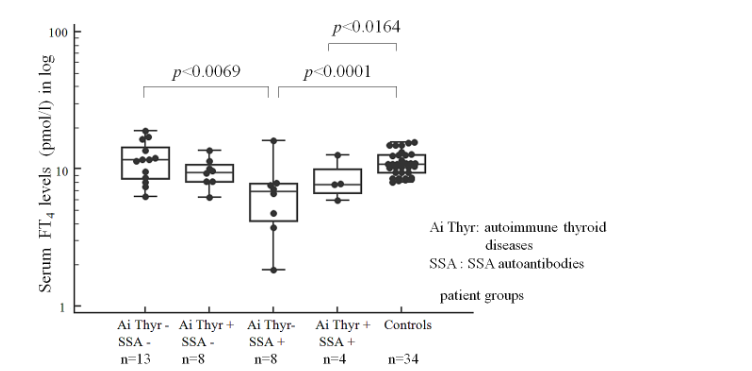
The results showed that the presence of SSA autoantibodies primarily affected serum FT4 levels, lowering them, while simultaneously increasing TSH levels and the FT3/FT4 ratio. The presence of SSA autoantibodies resulted in a greater decrease in serum FT4 levels compared to those who were negative for SSA autoantibodies and negative for autoimmune thyroid diseases, and borderline significance in MCTD patients who were positive for thyroid diseases only.
THE EFFECT OF SSA AUTOANTIBODIES ALONE AND WITH ANTI-THYROID PREOXIDASE AND/OR ANTI-THYROGOBULIN AUTOANTIBODIES ON FT4 LEVELS IN PATIENTS WITH MIXED CONNECTIVE TISSUE DISEASE
The effect of SSA autoantibodies alone and together with anti-Tg or anti-TPO antibodies on serum FT4 levels in patients with MCTD was investigated using two-way ANOVA. The relationship between SSA and anti-Tg or anti-TPO autoantibodies is shown in Figure 3. The presence of SSA autoantibodies alone was associated with lower serum FT4 levels compared to their absence [8.71(4.68-16.2) vs. 10.38(5.32-20.25) pmol/l]. Their association with anti-Tg antibodies represented the greater decrease in FT4 levels compared to anti-Tg positive cases alone [3.74(1.37-10.18) vs. 11.05(8.57-14.24) pmol/l, p<0.001], and cases with SSA autoantibody positivity (p<0.002) or SSA autoantibody negativity (p<0.0001).
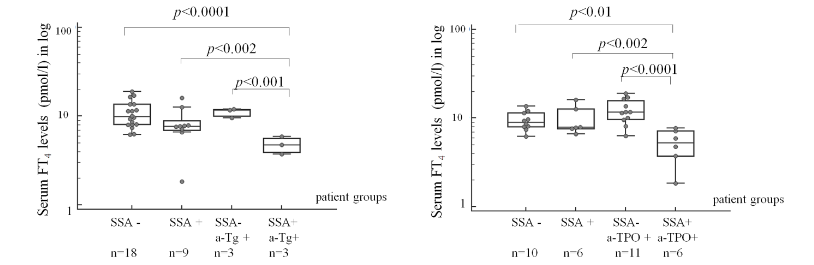
The presence of SSA or anti-TPO autoantibody positivity alone did not significantly decrease serum FT4 levels, but their association resulted in significantly lower FT4 levels [9.23(4.64-18.35) and 11.75 (6.05-22.8) vs. 4.68(1.65-13.28) pmol/l, p<0.014 and p<0.0001, respectively].
Three-way ANOVA was used to examine the relationship between SSA, anti-Tg and anti-TPO autoantibodies and FT4 levels in patients with MCTD. The results are limited by the small number of patients. The strength of the relationship between FT4 as the dependent variable and independent variables such as SSA, anti-Tg, and anti-TPO autoantibodies, and their interactions was evaluated using general linear model. The presence of all three autoantibodies resulted in a greater decrease in serum FT4 levels compared to those with SSA autoantibodies alone, or with the presence of anti-TPO antibodies alone, or with the combination of SSA and anti-TPO autoantibodies, or with the combination of anti-TPO and anti-Tg antibodies [3.74 (1.37-10.18) vs. 9.23(4.64-18.35) pmol/l, p<0.0001 or 13.27(7.18-24.53) pmol/l, p<0.007 or 7.91(4.69-13.3) pmol/l, p<0.023 or 10.59(7.9-14.2) pmol/l, p<0.046, respectively].
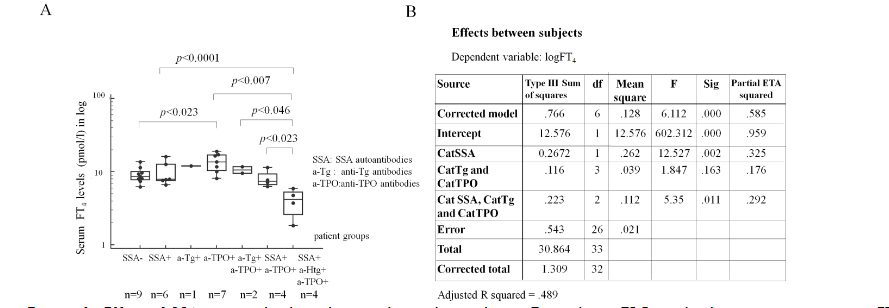
The model was significant: p<0.0001, adjusted R squared: 0.489. In this model, the results showed that the combined effect of anti-TPO and anti-Tg antibodies was not sufficient to significantly reduce serum FT4 levels. In contrast, SSA autoantibodies alone and in the combination with anti-TPO and anti-Tg antibodies showed a significant decrease in FT4 levels in the model.
Discussion
The presence of anti-TPO and anti-Tg antibodies is more commonly associated with antinuclear antibodies and elevated IgG immunoglobulin levels independent of thyroid autoimmunity. Sjögren’s syndrome is frequently associated with autoimmune thyroid diseases (Hashimoto’s thyroiditis in 17% and Graves’ disease in 5%) highlighting the risk of developing lymphoma in both diseases. Genetic factors, infections and cytokine-mediated inflammation represent a multistep process for the induction of B cell activation and proliferation. SSA autoantibodies have been detected in 30-60% of patients with Sjögren’s syndrome. The study of the adjuvant activity of U1-RNP demonstrated both B- and T-cell activation and dendritic cell maturation, suggesting that U1-RNP may play an endogenous adjuvant role. Systemic sclerosis also shows a high association with autoimmune thyroid diseases (33%) resulting in hypothyroidism (50%).
Hypothyroidism is more common sign in the association between systemic and organ specific autoimmune thyroid diseases, especially by Hashimoto’s thyroiditis. Thyroid autoantibodies were present in 6 patients out of 33 in MCTD without thyroid autoimmunity highlighting that thyroid autoantibodies can occur independently of thyroid autoimmunity. The presence of SSA autoantibodies was associated with significantly decreased serum FT4 and concomitantly increased TSH levels in MCTD patients. Surprisingly, in the absence of SSA autoantibodies, serum FT3 levels were significantly lower in MCTD patients compared to controls. This rules out the causative role of non-thyroidal illness in thyroid hormone changes by SSA autoantibody positivity. The low T3 levels characterize the non-thyroidal illness syndrome, are due to the inhibitory effect of cytokines on deiodinase enzymes (type 1 and type 2) as observed in critically ill patients. Maternal SSA autoantibodies can be transferred to the foetus during pregnancy. The presence of maternal SSA/SSB autoantibodies can be transmitted a danger in utero by activating the type 1 interferon system, leading to congenital heart block. A Chinese study showed a strong association between thyroid autoimmunity and the prevalence of antinuclear antibodies (ANA) in pregnancy. They found that high ANA titres associating with high anti-TPO antibody levels (in 30%) were connected to the risk of neonatal damage in pregnancy. Congenital heart block (14-42%) has two main aetiologies: AV septal defects and anomalies of the great arteries. Neuromyelitis optica spectrum disorder (NMOST) is an autoimmune inflammatory disease characterized by astrocytopathy leading to blindness. Neuromyelitis optica spectrum disorder is most commonly associated with the systemic autoimmune diseases Sjögren’s syndrome (35%) and systemic lupus erythematosus (51%). Estrogen plays an immune enhancing role. In these diseases, the SSA autoantibodies alone can be considered to be the cause of the tissue damage.
Our results showed that SSA autoantibodies in combination with anti-TPO and/or anti-Tg autoantibodies led to a greater decrease in serum FT4 levels than SSA antibodies alone. In mixed connective tissue disease, hypothyroidism may develop in the absence of thyroid autoimmunity, so measurement of thyroid hormones and autoantibodies must be routine. Endothelial cell dysfunction is associated with MCTD and plays a role in atherosclerotic complications such as cardiovascular disease and pulmonary arterial hypertension. In turn, hypothyroidism promotes the development of endothelial dysfunction. Hypothyroidism is associated with decreased cardiac output, increased capillary permeability and vascular resistance, and decreased insulin sensitivity. The above pathomechanisms are involved in the symptoms of MCTD. In euthyroid patients with Hashimoto’s thyroiditis, non-specific rheumatic symptoms such as polyarthralgia and myalgia/fibromyalgia were observed in 62%. The exact mechanism by which SSA autoantibodies can interfere with thyroxine (T4) synthesis is not yet understood. Both proteins, SSA antigen and T4 synthesis, are located in the nucleolus, so the role of proteasomes may be a common factor. Nuclear autoantigens and T4 are degraded by proteasomal pathways. Proteasomal events play a role in systemic autoimmunity by antigen processing and influencing the activity of inflammatory processes.
Limitations of the study could be the small number of patients and categorizing the levels of SSA, anti-Tg and anti-TPO autoantibodies. The relationships between the effect of SSA autoantibodies and decreased serum FT4 levels may represent a real clinical conditions using multiple statistical analyses.
Conclusions
The presence of SSA autoantibodies was associated with significantly lower serum FT4 levels compared to controls in MCTD with concomitant elevated TSH levels. The effect of SSA autoantibodies on FT4 levels can also be observed in the absence of thyroid autoimmunity. SSA autoantibody positive MCTD patients, together with anti-TPO and anti-Tg antibody positivities showed the greatest decrease in serum FT4 levels. The results highlight the importance of screening for thyroid hormone and autoantibody levels in MCTD patients independently of thyroid autoimmunity, especially by the co-occurrence of SSA, anti-TPO and anti-Tg antibody positivity and pregnancy.
Conflicts of interest statement:
The authors declare no conflicts of interest.
Funding statement:
No funding.
Acknowledgements:
None
References
- Zöld E, Bodolay E, Dezső B, Soos Gy, Nakken B, Szodoray P. Mixeted connective tissue disease associated with autoimmune hepatitis and pulmonary fibrosis. IMAJ 2014;16:733-734.
- Wanzenried A, Garaiman A, Jordan S, Distler O, Maurer B. The enigma of mixed connective tissue disease-challenges in routine care. Clin Rheumatol 2022;41: 3503-3511. doi:10.1007/s’0067-022-06286-w.
- Sapkota B, Khalili Y. Mixed connective tissue disease. StatPearls Publishing, 2024. https://www.ncbi.nlm.nih.gov/books/NBK542198/
- Jones D, Anjanappa JC, Hiremath S, et al. The prevalence of thyroid dysfunction in patients with connective tissue disorders. Asian Journal of Med Sci 202;12(7):33-36. doi:10.3126/ ajms.v12i7.34998.
- Bíró E, Szekanecz Z, Czirják L, et al. Association of systemic and thyroid autoimmune diseases. Clin Rheumatol 2006; 25:240-245.doi:10.1007/s1006-005-1165-y.
- Calder EA, Irvine WJ. Cell-mediated immunity and immune complexes in thyroid disease. Clin Endocrinol and Metab 1975;4(2):287-318. doi:10.1016/S0300-595X(75)80023-5.
- Dominiques SL, Gonçalves FT, Jorge MLMP, Limongi JE, Ranza R, Jorge PT. High prevalence of hypothyroidism in systemic lupus erythematosus patients without and increase in circulating antithyroid antibodies. Endocr Pract 2017; 23(11): 1304-1310. doi:10.41586/EP161664.
- Garga A, Helbig M, Schauer M, Nguyen M. A complex case of polymyositis overlapping with hypothyroid myopathy without underlying autoimmune thyroid disorder. Cureus 2020;12(6):1-5. doi:10. 7759/cureus.8629.
- Setty YN, Pittman CB, Mahale AS, Greidinger EL, Hoffman RW. Sicca symptoms and anti-SSA/Ro antibodies are common in mixed connective tissue disease. J Rheumatol 2002;29(3):487-489. https://www.jrheum.org/content/29/3/487.
- Yoshimi R, Ueda A, Ozato K, Ishigatsubo Y. Clinical and pathological roles of Ro/SSA autoantibody system. Clin Dev Immunol 2012; Vol 2012, Article ID: 606196, 12 pages. doi:10.1155/2012/ 606195.
- Robbins A, Hentzien M, Toquet S, et al. Diagnostic utility of separate anti-Ro60 and anti-Ro52/TRIM21 antibody detection in autoimmune diseases. Front Immunol 10:444. doi:10.3389/fimmu.2019.00444.
- Lazúrová I, Benhatchi K. Autoimmune thyroid diseases and nonorgan-specific autoimmunity. Pol Archiv Med Wewn 2012; 122(Suppl 1):56-58. https://pubmed.ncbi.nlm.nih.gov/23222800/.
- Pedro ABP, Romaldini JH, Americo C, Takei K. Association of circulating antibodies against double-stranded and single-stranded DNA with thyroid autoantibodies in Graves’ disease and Hashimoto’s thyroiditis patients. Exp Clin Endocrinol Diabetes 2006;114(1):35-38. doi:10.1055/s2005-873005.
- Liu YJ, Miao Hb, Lin S, Chen Z. Association between rheumatoid arthritis and thyroid dysfunction: A meta-analysis and systemic review. Front Endocrinol 13:1015516. doi: 10.3389/fendo.2022. 1015516.
- Alercón-Segovia D, Villareal M. Classification and diagnostic criteria for mixed connective tissue disease, In: Kasukawa R, Sharp GC: Mixed Connective tissue disease and antinuclear antibodies, eds. by Toyo T, Miyawaki S, Elsevier Science Publishers B.V. (Biomedical Division), Amsterdam, 1987:33-40.
- Bodolay E, Csiki Z, Szekanecz Z, et al. Five-year follow-up of 665 Hungarian patients with undifferentiated connective tissue disease (UCTD). Clin Exp Rheumatol 2003;21:313-320. https://pubmed.ncbi.nlm.nih.gov/12846049/
- Bodolay E, Csípő I, Gál I, et al. Anti-endothelial cell antibodies in mixed connective tissue disease: Frequency and association with clinical symptoms. Clin Exp Rheumatol 2004; 22:409-415. https://pubmed.ncbi.nlm.nih.gov/15301236/
- Ruan Y, Heng Xp, Yang Lq, et al.. Relationship between autoimmune thyroid antibodies and anti-nuclear antibodies in general patients. Front Endocrinol 15: 1368088. doi:10.3389/ fendo.2024.1368088.
- Baldini C. Ferro F, Mosca M, Fallahi P, Antonelli A. The association of Sjögren syndrome and autoimmune thyroid disorders. Front Endocrinol 9:121. doi:10.3389/fendo. 2018.00121.
- Goëb V, Salle V, Duhaut P, et al. Clinical significance of autoantibodies recognizing Sjögren’s syndrome A (SSA), SSA, calpastatin and alpha-fodrin in primary Sjögren’s syndrome. Clin Exp Immunol 2007; 148:281-287. doi:10.1111 /j.1365.2249.2007.03337.x.
- Kelly-Scumpia KM, Nacionales DC, Scumpia PO, et al. In vivo adjuvant activity of the RNA component the Sm/RNP lupus autoantigen. Arthritis Rheum 2007;56(10): 3379-3386. doi:10.1002/art.2294.
- Fallahi P, Ruffilli I, Giuggioli D, et al. Associations between systemic sclerosis and thyroid diseases. Front Endocrinol 8:266. doi: 10.3389/fendo.2017.00266.
- Wajner SM, Maia AL. New insights toward the acute non-thyroidal illness syndrome. Front Endocrinol 2012;3, 1-7. doi:10.3389/fendo.2012.00008.
- Molnár I, Czirják L. Euthyroid sick syndrome and inhibitory effect of sera on the activity of thyroid 5’-deiodinase in systemic sclerosis. Clin Exp Rheumatol 2000;18:719-724. https://pubmed.ncbi.nlm.nih.gov/11138334/.
- Hedlund M, Thorlacius GE, Ivanchenko M, et al. Type I IFN system activation in newborns exposed to Ro/SSA and La/SSB autoantibodies in utero. RMD 2020; 6: e00989.doi:10.1136/mdopen-2019-00989.
- Wu M, Wan Y, Zhao L, et al. Association between thyroid autoimmunity and antinuclear antibody prevalence among pregnant women: a cross-sectional study in Qingdao, China. Front Endocrinol 15: 1403917.doi:10.3389/fendo.2024.1403917.
- Brito-Zerón P, Izmirly PM, Ramos-Casals M, Buyon JP, Khamashta MA. The clinical spectrum of autoimmune congenital heart block. Nat Rev Rheumatol 2015;11(5): 301-312. doi:10.1038/nrrheum.2015.29.
- Lin L, Hang H, Zhang J, Lu J, Chen D, Shi J. Clinical significance of anti-SSA/Ro antibody in Neuromyelitis optica spectrum disorders. MSARD 2022;58:1-6. doi:10. 1016/j.msard.2022.103494.
- Soltesz P, Bereczki D, Szodoray P, et al. Endothelial cell markers reflecting endothelial cell dysfunction in patients with mixed connective tissue disease. Arthritis Res Ther 2010; 12:R78-R88. doi: 10.1186/ar2999.
- Tudoran M, Tudoran C. Particularities of endothelial dysfunction in hypothyroid patients. Kardiol Pol 2015;5:337-343. doi:10.5603/Kpa2014.0241.
- Udovcic M, Pena RH, Patham B, Tabatabai L, Kansara A. Hypothyroidism and the heart. MDCVJ 2017;XIII(2):55-59.
- Giuffrida G, Bagnato G, Campenni A, et al. Non-specific rheumatic manifestations in patients with Hashimoto’s thyroiditis: a pilot cross-sectional study. J Endocrinol Invest 2020;43(1):87-94. doi: 10.1007/s40618-019-01083-w.
- Mountz JD. Significance of increased circulating proteasome in autoimmune disease. J Rheumatol 2022;29(10):2027-2030. https://www.jrheum.org/content/29/10/2027.long.
- Egerer K, Kuckelkorn U, Rudolph PE, et al. Circulating proteasomes are markers of cell damage and immunologic activity in autoimmune diseases. J Rheumatol 2020; 29(10):2045-2052. https://www.jrheum.org/content/jrheum/29/10/2045.
- Chen M, von Mikecz A. Proteasomal processing of nuclear autoantigen: systemic autoimmunity. Autoimmun Rev 2005;4(3): 117122. doi:10.1016/j.autrev. 2004.08.038.