





Impact of Supplements on Levothyroxine Administration
Vitamins, Supplements, and Dietary Habits Contribute to Incorrect Levothyroxine Administration – A Sub-Analysis of the CONTROL Surveillance II Study
Kayla Reid¹, Duni Cummings-John¹, Walter Sandulli¹, Doreen Clark²
- IBSA USA, Parsippany, NJ, USA
- Way to Goal Business Insights, Phoenix, AZ, USA
OPEN ACCESS
PUBLISHED: 30 April 2026
CITATION: Reid, K., Cummings-John, D., et al., 2026. Vitamins, Supplements, and Dietary Habits Contribute to Incorrect Levothyroxine Administration – A Sub-Analysis of the CONTROL Surveillance II Study. Medical Research Archives, [online] 14(4).
COPYRIGHT: © 2026 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
ISSN 2375-1924
ABSTRACT
Introduction:
Levothyroxine has a narrow therapeutic window, and its absorption is highly sensitive to food and supplements, making precise dosing and adherence to administration guidelines critical. The CONTROL Surveillance II study evaluated real-world patient awareness and adherence to FDA-labeled levothyroxine administration instructions, including timing and avoidance of interfering substances. This sub-analysis assessed patient ingestion of foods, vitamins, and supplements known to affect absorption, the effectiveness of physician communication, and patient comprehension and recall, as well as demographic and socioeconomic characteristics associated with lower awareness.
Methods:
CONTROL Surveillance II was an online survey of 1,000 U.S. adults aged 19–90 years who self-reported a clinician diagnosis of hypothyroidism. Participants were randomly selected from a proprietary, consented research panel developed and maintained by Harmon Research Inc., a U.S.-based research firm (https://www.harmonresearch.com). Pregnant patients were excluded. Qualified subjects had been taking levothyroxine monotherapy for ≥ 1 year. Survey questions were reviewed by board certified endocrinology experts, and the survey was initiated in December 2023 and completed in January 2024.
Results:
This CONTROL Surveillance II sub-analysis assessed patient awareness of food, vitamin, and supplement interactions with levothyroxine, provider communication, and factors associated with nonadherence. Key findings include: 1. Overall, 49% of participants reported using dietary supplements, most commonly multivitamins (57%), followed by calcium (30%) and iron (15%). 2. Most patients recalled receiving physician guidance on dosing timing, but only 45% remembered discussions about food, vitamin, or supplement interactions with levothyroxine. 3. Supplement use was higher among older adults (29% vs 14%, P≤ 0.05), non-Hispanic white patients (27% v 18%, P≤ 0.05), and higher income participants, with the latter reporting greater multivitamin and calcium use than lower-income groups (63% vs 54% and 39% vs 28%, P≤ 0.05).
Conclusions:
Suboptimal levothyroxine administration due to supplement and food co-administration is widespread. This sub-analysis highlights persistent gaps in counseling and comprehension influenced by sociodemographic factors, underscoring the need for improved patient education.
Keywords:
levothyroxine, hypothyroidism, dietary supplements, patient education, medication adherence
INTRODUCTION
Hypothyroidism is a common endocrine disorder resulting from thyroid hormone deficiency and has a higher prevalence among female and older patients. The clinical presentation can include a wide variety of non-specific symptoms that differs with age, sex, and time between onset and diagnosis defined by thyroid stimulating hormone (TSH) concentrations. The standard of care for treating hypothyroidism is levothyroxine, a synthetic form of thyroxine (T4), which is the body’s natural thyroid hormone and is usually used as a lifelong treatment. Levothyroxine is a medication with a narrow therapeutic index; therefore, small changes in the levothyroxine dose can lead to substantial variation in serum TSH levels. Ensuring proper dosage and maximum absorption is critical to therapeutic success. Leading endocrine thyroid bodies including the American Thyroid Association (ATA) and the European Thyroid Association (ETA) are aligned in recommending levothyroxine be taken with water 30–60 minutes before breakfast or before bedtime with at least a 3-hour interval from the evening meal and avoiding the concomitant ingestion of foods, supplements, and medications that are known to inhibit absorption. Given that patient behaviors can significantly compromise levothyroxine performance, identifying and having a deeper understanding of the factors that influence patient awareness of and adherence to levothyroxine’s strict administration guidance may help optimize its clinical performance. The CONTROL Surveillance II study sought to confirm the earlier findings from the original CONTROL Surveillance study which quantified the prevalence of factors adversely affecting levothyroxine therapy and to explore the reasons why patients adhere or do not adhere to FDA-recommended administration guidance for levothyroxine. The study confirmed widespread low awareness of FDA-recommended levothyroxine administration guidance. Up to 21% of study participants reported taking levothyroxine within 30 minutes of eating breakfast, and 26.6% reported using over-the-counter (OTC) or prescription acid blockers that can influence the dissolution and absorption of levothyroxine tablet therapies. Patient awareness of medications, vitamins, and supplements known to interfere with levothyroxine was low despite physician efforts to provide education about their potentially negative impact on levothyroxine therapy, indicating a need to better understand the factors that shape patient awareness and adherence specific to these topics.
AIMS AND SCOPE
The current sub-analysis further explores the results of the CONTROL Surveillance II study, specifically the effectiveness of efforts to educate patients about FDA-recommended administration guidance for levothyroxine. Correlation between populations based on age, ethnicity, and socioeconomic variables, comprehension and adherence to levothyroxine administration guidance, and therapy satisfaction were also assessed. This manuscript follows the Quality Assessment Criteria for Survey Research Reports guidelines.
METHODS
IBSA Pharma USA was the sponsor of the study. In conjunction with the study administrator, Way to Goal Inc., it developed the survey and was responsible for all aspects of the study. Survey questions were reviewed by board certified endocrinology experts. Participants were selected from a proprietary panel research of subjects maintained by Harmon Research Inc. of Anaheim, California. Each subject had previously agreed and consented to be a part of a panel to take surveys on various health-related topics. Recruitment into the panel is conducted across multiple digital channels, including major social media platforms such as LinkedIn, Facebook, Instagram, and TikTok, as well as through Google Ads. This multichannel approach allows Harmon to reach a broad and diverse population. (More information can be obtained by visiting https://www.harmonresearch.com). Study participants were informed of their data’s confidentiality and were given a statement indicating that their participation was voluntary and that withdrawal from the survey was possible at any point. The sponsor did not have access to patient-identifying information. The study enrolled 1,000 patients between the ages of 19 and 90 years old who self-reported to have been diagnosed with hypothyroidism by their clinician. Participants were chosen randomly. The invitation process incorporates randomization by selecting every nth eligible record to receive an email alert about a new survey opportunity. Once notified, panel members can log into their personal portal where they see a list of available surveys for which they may qualify, typically four to five surveys at any given time. This method of randomized email distribution and participant self-selection is a standard practice among commercial research panels and is designed to balance reach, feasibility, and diversity of response within target demographic criteria. Those who indicated interest were sent a link to a set of screening questions that evaluated their qualification for study inclusion. Participant identity was verified via double opt-in, digital fingerprinting, and validation of contact information. Respondents were provided with all pertinent information related to the study including estimated survey duration, technology requirements such as a mobile phone, tablet or desktop/laptop, and honoraria for survey completion. Once qualified, respondents had the option to participate in the study and could click on a link that provided access. Participants could opt out at any time. Each was assigned a unique ID, and their entire participation history was recorded including inclusion and exclusion criteria. Duplicates were not allowed. Post-survey responses underwent manual review to ensure data quality, geographic eligibility, and the absence of duplicates or suspicious patterns. Persons who partially completed the survey were allowed to resume at any time. Prospective study subjects completed 9 screener questions. If a participant passed the screening criteria, he/she was asked to answer approximately 20 study questions (see Appendix: Hypothyroid Patient Survey). Time to complete the online survey was approximately 12-15 minutes. Quality control included pre-survey identity verification, in-survey screening for bots and low-effort responses, and post-survey manual review to remove incomplete, invalid, or duplicate entries. The survey was initiated in December 2023 and was completed in January 2024.
COMPENSATION
Subjects were paid an honorarium of $25 upon completion of the survey and confirmation of contact information.
Inclusion Criteria
- 19-90 years of age
- Formally diagnosed with hypothyroidism by a healthcare provider
- Currently taking levothyroxine monotherapy to treat hypothyroidism
- Taking levothyroxine for ≥1 year
- Not currently pregnant
- A US resident
- Voluntary agreement to provide informed consent
Exclusion Criteria
- Not taking levothyroxine to treat hypothyroidism
- Taking prescription medication to treat hypothyroidism for ≤ 1 year
- Taking Cytomel or generic liothyronine in addition to levothyroxine
- Currently pregnant
Statistical methods
Demographic characteristics were presented using frequency and descriptive statistics. Frequency and descriptive statistics were also used to analyze categorical and continuous response sets. Cross-tabulation tables were created to present pertinent data across multiple survey questions of interest. Parametric and non-parametric between-subject analyses were performed in an exploratory fashion. Frequency and percentage statistics were used to analyze the survey questions using categorical and “select all that apply” response sets. Descriptive statistics (mean, median, standard deviation, and interquartile range) were used for questions using continuous level response sets, such as a five-point scale. Cross-tabulation tables were created to present the frequencies and percentages of survey responses across multiple questions of interest. Parametric (independent samples t-test, one-way ANOVA, and post hoc tests) and/or non-parametric (chi-square, Mann-Whitney U, Kruskal-Wallis, and Dunn’s test) between-subjects analyses were performed based on the meeting of statistical assumptions. These inferential analyses were all exploratory in nature. No adjustments were made to account for multiple comparisons. The frequency, descriptive, and inferential statistics were presented in tabular and visual formats. All analyses were performed using Q Professional Version 5.16.4.0 and statistical significance was assumed at a non-adjusted, two-sided alpha value of 0.05.
SAMPLE SIZE
Using a 95% confidence interval, a 3% margin of error, and a prevalence of 15-40% in the general population for GERD and H. pylori infections, a total sample size of n = 1,000 participants was needed to have adequate statistical power for purposes of yielding a generalizable measure of prevalence within the population of interest. There were no a priori hypotheses stipulated for the proposed inferential analyses.
Key Findings of the Primary Study
The results of the CONTROL Surveillance II study highlight that a significant percentage of levothyroxine-taking patients may not be taking levothyroxine in a way that is consistent with FDA-approved administration guidance. This lack of compliance may be a result of incomplete patient awareness, indicating an opportunity for enhanced prescriber-patient dialogue.
KEY FINDINGS ARE AS FOLLOWS:
- Between 55 and 60% of participants do not recall receiving instructions regarding avoidance of interfering vitamins, supplements, or medications.
- Over 36% administer levothyroxine outside of instructions contained in FDA approved labeling.
- A large percentage (54%) of participants report taking proton pump inhibitors (39%) or antacids (15%) concomitantly with levothyroxine.
- Most patients (72%) recalled physician instructions to take levothyroxine in the morning ≥30 minutes before breakfast with water. However, 55% did not recall instructions regarding the consumption of interfering vitamins/supplements.
- Patients who reported difficulty adhering to administration guidance were more likely to report having stopped their prescribed medication for >1 month (25% vs. 10%; P≤0.05).
Reporting of Results
Way to Goal organized and analyzed the results, highlighting relevant research findings and implications.
STUDY ETHICS
Institutional Review Board
The protocol and appropriate related documents were reviewed and approved by Advarra of Columbia, MD, which was constituted and is functioning in accordance with ICH E6, 3. A signed letter of study approval from the IRB Chairman was sent to the study administrator (Way to Goal Business Insights) with a copy sent to the sponsor (IBSA) prior to study initiation.
ETHICAL CONDUCT OF THE STUDY
This study was conducted in accordance with the standard operating practices of IBSA, which are designed to ensure adherence to GCP guidelines.
SUBJECT INFORMATION AND CONSENT
Each subject was informed that participation in the study was voluntary and that he/she may withdraw from the study at any time. A Waiver of Informed Consent was issued by Advarra.
CONFIDENTIALITY OF INFORMATION
Way to Goal and IBSA followed all national, regional, and local laws with respect to privacy and data protection to ensure that the survey complied with all applicable industry standards. This included observing the following guidelines, among others:
- Voluntary cooperation of subjects
- Protection of researchers’ and respondents’ identities
- Terms & Conditions and privacy policies compliant with local laws
- State-of-the-art data security policies and measures
- Reliable and validated data procedures
- Strict adherence to rules governing the interviewing of children and young people
Survey Completion Rates
More than three thousand respondents (3,029) requested to take the survey. Of these, 58% (1,759) did not meet the study’s inclusion criteria. Of the 1,270 who met the study’s criteria and initiated the survey, 79% (1,000) successfully completed it.
Demographics
The median age of participants was 62 and respondents to the survey were predominantly female (74%). Non-Hispanic whites represented 84% of study participants; Hispanic and black non-Hispanics represented 14%, and 2% reported as “other”. Most respondents were under the care of a primary care physician (PCP) for the treatment of their hypothyroidism (70%), followed by those treated by an endocrinologist (19%). The majority (81%) reported taking levothyroxine to treat their hypothyroidism for six years or more; 61% for more than 10 years. Regarding household income, 63% reported annual income <$60,000, 29% $60,000-$120,000, and 8%>$120,000.
| Patient Reported Prescribers of Levothyroxine | Gender Identity |
|---|---|
| Primary Care Physician (Family Doctor, IM) | 70% Female |
| Endocrinologist | 26% Male |
| Nurse Practitioner | 0% Non-binary |
| Physician Assistant | |
| Thyroid Specialist |
| Total Annual Household Income | Age |
|---|---|
| $0-$30,000 | 19-44 years old 16% |
| $31,000-$60,000 | 45-64 years old 40% |
| $61,000-$90,000 | 65+ years old 44% |
| $91,000-$120,000 | Median age 62 years old |
| $120,000+ |
Results of Sub-analysis
This sub-analysis of the CONTROL Surveillance II study evaluated patient awareness of the potential for foods, vitamins, and supplements to interfere with levothyroxine therapy and the information received by patients from their prescribers about such interactions. It also documented lack of adherence to administration guidance and correlating factors to lack of adherence.
KEY FINDINGS INCLUDE THE FOLLOWING:
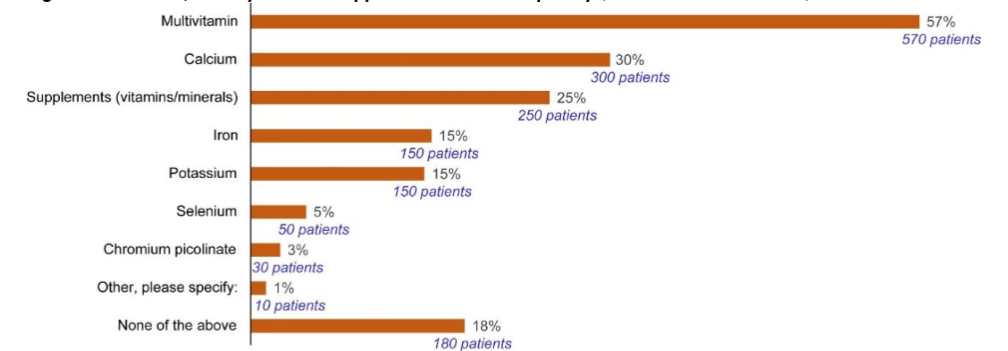
Supplement Use Varies by Patient Demographics Overall, 49% of participants in the CONTROL Surveillance II study indicated that they take dietary supplements, with multivitamins being the most commonly used supplements taken concomitantly with levothyroxine (57%) followed by calcium (30%) and iron (15%).
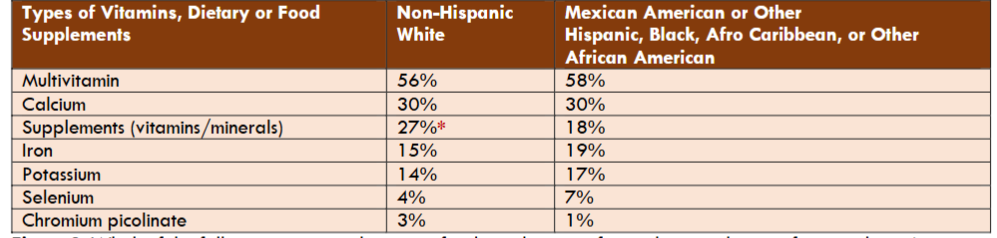
Supplement use patterns varied significantly by demographic characteristics. Non-Hispanic white patients were more likely to report vitamin and mineral use compared to other racial or ethnic groups (27% vs 18%, P≤ 0.05).
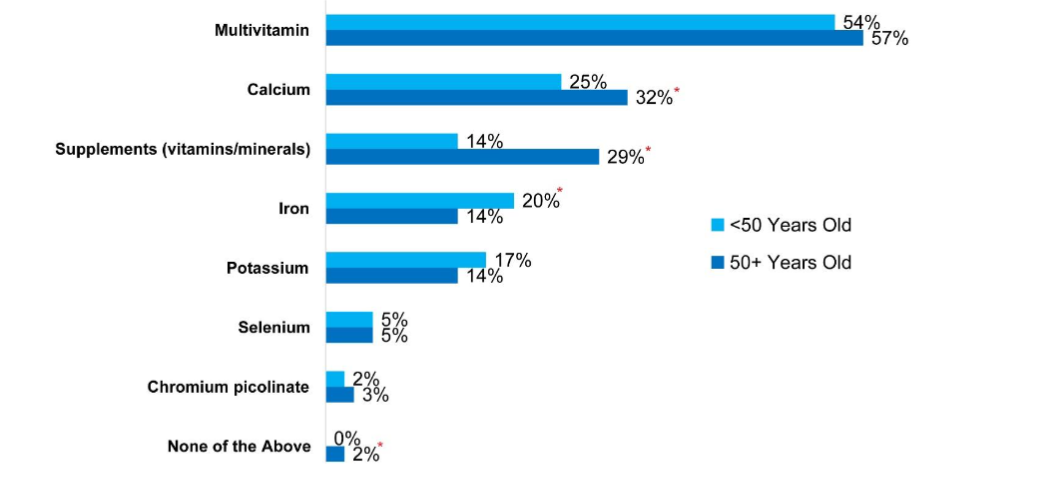
Age was associated with greater supplement use, with older patients (>50 years) reporting higher rates of vitamin and supplement consumption compared to younger patients (<50 years) (29% vs 14%, P≤ 0.05). While older patients reported higher use of calcium than younger patients (32% vs 25%, P≤ 0.05), younger patients reported higher use of iron (20% vs 14%, P≤ 0.05). With regard to timing of supplement and vitamin administration, 33% of patients reported taking vitamins and supplements concomitantly with levothyroxine therapy “sometimes”, “always” or “often”; such behavior differs between older and younger patients. Younger patients (< 50 years) were more likely than older patients (> 50 years) to report such behavior (53% vs 37%, P ≤ 0.05). The coadministration of levothyroxine with calcium supplements was reported equally among all ethnicities.
However, there appears to be an association between income and frequent calcium and multivitamin use. Patients with income greater than $120,000 annually were more likely to report taking more multivitamins and calcium compared to patients with income less than $60,000 annually (63% vs 54% and 39% vs 28%, P≤ 0.05, respectively).
Strong Demographic Trends Relative to the Use of Interfering Foods and Liquids In the CONTROL Surveillance II study, 36% of participants reported taking levothyroxine outside of FDA-recommended guidance: daily on an empty stomach at least 30 minutes before eating. The sub-analysis identified that while all age groups were comparable in following recommended guidance for hypothyroid administration time before eating, older patients (>50 years) were better at following after eating guidance versus younger patients. Compared with younger patients, older patients were more likely to report taking levothyroxine 2 or more hours after eating (35% vs 9%, P≤ 0.05). Patients reporting with low income were more likely to be less compliant with after-eating guidance, with 24% reporting that they take their medication within 10 minutes after eating. This compares with 5% of patients with moderate levels of income ($60,000-$120,000) and 11% of patients with higher reported levels of income ($120,000+). There were no statistical differences or trends identified by ethnicity in terms of the timing of administration before or after meals.
Even though most study subjects recalled some instruction about the need to administer levothyroxine 30 minutes before breakfast (64%), many were unaware of the need to take their medication with water alone (19%).
Figure 4: Vitamins, Dietary or Food Supplements Taken at Same Time as Hypothyroid Medication by Income
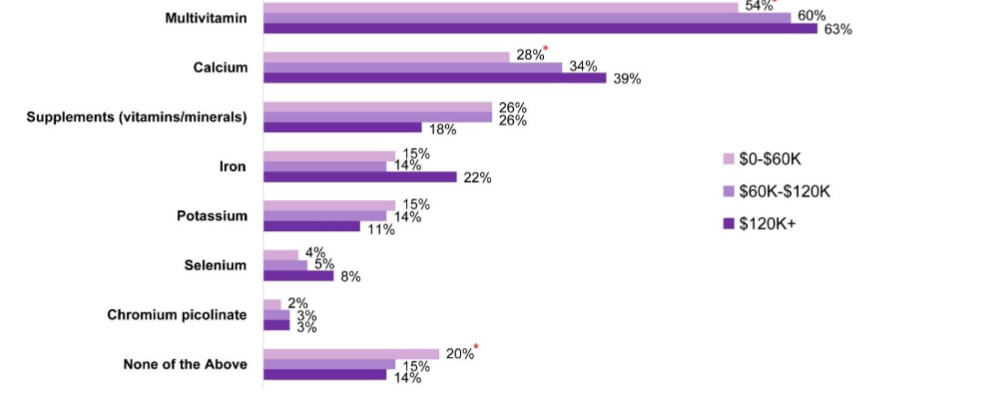
Figure 4: Which of the following vitamins, dietary or food supplements, if any, do you take on a frequent basis (i.e., more than 2 times per week)?
* means statistically significant (P < 0.05) at 95% CI; “$0–$60K” n = 630, “$60K–$120K” n = 291, “$120K+” n = 79
Strong Demographic Trends Relative to the Use of Interfering Foods and Liquids
In the CONTROL Surveillance II study, 36% of participants reported taking levothyroxine outside of FDA-recommended guidance: daily on an empty stomach at least 30 minutes before eating breakfast¹. The sub-analysis identified that while all age groups were comparable in following recommended guidance for hypothyroid administration time before eating, older patients (>50 years) were better at following after-eating guidance versus younger patients. Compared with younger patients, older patients were more likely to report taking levothyroxine 2 or more hours after eating (35% vs 9%, P < 0.05). Patients reporting with low income were more likely to be less compliant with after-eating guidance, with 24% reporting that they take their medication within 10 minutes after eating. This compares with 5% of patients with moderate levels of income.
($60,000–$120,000) and 11% of patients with higher reported levels of income ($120,000+). There were no statistical differences or trends identified by ethnicity in terms of the timing of administration before or after meals.
Even though most study subjects recalled some instruction about the need to administer levothyroxine 30 minutes before breakfast (64%), many were unaware of the need to take their medication with water alone (19%) (Table 2). Younger patients (<50 years) were more likely to report taking levothyroxine with liquids other than water compared to older patients (24% vs 17%, P ≤ 0.05).
| How Hypothyroid Medication is Taken | With Food/Water | With Vitamins/Supplements |
|---|---|---|
| <50 Years Old | 76% | Always 22% |
| 50+ Years Old | 83%* | Often 15%* |
* Means statistically significant (P<0.05) at 95% CI; “<50” group is defined by those younger than 50 years of age (n=234); “50+” group is defined by those 50 years of age or older (n=766)
Patient Characteristics Strongly Correlate with Recall about Physician Guidance
Physician discussions about nutrition were reported by 21% of study respondents. Older patients (>50 years) were twice as likely not to recall having any discussions with their care providers about dietary habits, nutrition, and levothyroxine administration versus younger patients (34% vs 17%, P≤ 0.05). Younger patients (<50 years) were more likely to recall discussing proper administration of their hypothyroid medication (timing, need to take with water only) with their doctor (43% vs 33%, P≤ 0.05) and were almost twice as likely to recall discussing nutrition with their doctor than older patients (32% vs 17%, P ≤ 0.05). Our sub-analysis identified that age is not correlated with incorrect recall of these physician instructions about levothyroxine administration. There was no significant difference between how and when younger participants (<50 years old) and older participants take their hypothyroid medicine – with water or at the same time as vitamins, dietary or food supplements.
While there was little difference between the ethnicity of study respondents and recall of such discussions about recommended levothyroxine administration, there was a strong correlation between patient income and patient recall of nutrition-focused discussions. Patients with incomes greater than $120,000 annually were more likely to recall nutrition-focused discussions with their providers versus those with incomes less than $60,000 annually (38% vs 19%, P≤ 0.05). Higher income patients were also more likely to recall vitamin, dietary, or food supplement focused discussions with their providers as compared to those in lower income groups ($60,000-$120,000 and <$60,000), (46% vs 35% and 33%, P≤ 0.05), respectively.
Low Recall about Food Sensitivities and Levothyroxine Utilization
In the CONTROL Surveillance II study, 7% of participants reported having food allergies or sensitivities. Our sub-analysis reveals that non-Hispanic white respondents are less likely to have had food allergy or sensitivity focused discussions with their providers than other ethnicities (5% vs 12%, P ≤ 0.05). Patients with higher income (>$120,000) were more likely to discuss allergies to excipient ingredients or fillers (gluten, lactose, dyes, etc.) compared to those in the middle-income range ($60,000-$120,000) or those in the lower (<$60,000) income range (17% vs 7%, P≤ 0.1; 17% vs 5%, P≤ 0.05). Higher income patients were also more likely to report having discussions about stomach or gastrointestinal (GI) conditions compared to patients in lower income groups (33% vs 21%; 33% vs 24%, P<0.05 for each). 4). Higher income patients were also more likely to report having discussions about stomach or gastrointestinal (GI) conditions compared to patients in lower income groups (33% vs 21%; 33% vs 24%, P ≤ 0.05 for each; Table 4). Younger patients were more likely to discuss allergies to excipient ingredients or “fillers” (gluten, lactose, dyes,
etc.) than older patients (>50 years) (9% vs 5%, P ≤ 0.05; Table 3).
Table 3: Topics Discussed With Doctor Who Prescribed Hypothyroid Medication by Age
| Topics Discussed | <50 Years Old | 50+ Years Old |
|---|---|---|
| Use of other prescription medications | 34% | 39% |
| Hypothyroid medication administration (i.e., the proper way to take hypothyroid medication) | 43%* | 33% |
| Vitamins, dietary, or food supplements | 37% | 34% |
| Use of over-the-counter (OTC) medications | 29% | 23% |
| Stomach or gastrointestinal conditions | 29% | 22% |
| Nutrition | 32%* | 17% |
| Allergies to excipient ingredients or “fillers” (gluten, lactose, dyes, etc.) | 9% | 5% |
| None of the above | 17% | 34%* |
* means statistically significant (P < 0.05) at 95% CI
Age: <50 n = 234, Age 50+ n = 766
Which of the following topics, if any, have you ever discussed with the doctor who currently prescribes your hypothyroid medication?
Table 4: Topics Discussed With Doctor Who Prescribed Hypothyroid Medication by Income
| Topics Discussed | $0–$60K (a) | $60–$120K (b) | $120K+ (c) |
|---|---|---|---|
| Use of other prescription medications | 36% | 38% | 47% |
| Hypothyroid medication administration (i.e., the proper way to take hypothyroid medication) | 34% | 35% | 39% |
| Vitamins, dietary, or food supplements | 33% | 35% | 46%ᵇ |
| Use of over-the-counter (OTC) medications | 24% | 26% | 29% |
| Stomach or gastrointestinal conditions | 24% | 21% | 33%ᵇ |
| Nutrition | 19% | 20% | 38%ᵃᵇ |
| Allergies to excipient ingredients or “fillers” (gluten, lactose, dyes, etc.) | 5% | 7% | 17%ᵃᵇ |
| None of the above | 32%ᶜ | 30% | 5% |
ᵃ, ᵇ, ᶜ means statistically significant at 95% CI compared with the corresponding lettered column
“$0–$60K” n = 630, “$60K–$120K” n = 291, “$120K+” n = 79
Which of the following topics, if any, have you ever discussed with the doctor who currently prescribes your hypothyroid medication?
Table 5: Topics Discussed With Doctor Who Prescribed Hypothyroid Medication by Ethnicity
| Topics Discussed | Non-Hispanic White | Mexican American or Other Hispanic, Black, Afro Caribbean, or Other African American |
|---|---|---|
| Use of other prescription medications | 39% | 32% |
| Hypothyroid medication administration (i.e., the proper way to take hypothyroid medication) | 35% | 37% |
| Vitamins, dietary, or food supplements | 34% | 37% |
| Use of over-the-counter (OTC) medications | 24% | 29% |
| Stomach or gastrointestinal conditions | 23% | 26% |
| Nutrition | 20% | 26% |
| Allergies to excipient ingredients or “fillers” (gluten, lactose, dyes, etc.) | 5% | 12%* |
| None of the above | 31% | 24% |
* means statistically significant (P < 0.05) at 95% CI
“Non-Hispanic White” n = 836
“Mexican American or other Hispanic, Black, Afro Caribbean or other African American” n = 164
Which of the following topics, if any, have you ever discussed with the doctor who currently prescribes your hypothyroid medication?
Younger patients were also more likely to experience concomitant GI conditions than older age groups, specifically reporting greater rates of Gastroesophageal Reflux Disease (GERD), irritable bowel syndrome (IBS), lactose intolerance, ulcerative colitis, food allergies, gastroparesis, Crohn’s Disease, and H. pylori infection. Not surprisingly, they were also more likely to report taking antacids or acid reducers (Table 6).
Table 6: Concomitant GI Disease/Conditions and Frequency of Antacids/Acid Reducers by Age
Concomitant Disease/Conditions
| Condition | <50 Years Old | 50+ Years Old |
|---|---|---|
| Acid reflux or GERD | 35%* | 28% |
| IBS (irritable bowel syndrome) | 13%* | 7% |
| Lactose intolerance | 7%* | 3% |
| Gastric bypass or bowel resection | 3% | 3% |
| Ulcerative colitis | 5%* | 2% |
| Food allergies | 5%* | 2% |
| Gastroparesis | 4%* | 1% |
| Crohn’s disease | 3%* | 1% |
| Celiac disease | 1% | 0% |
| Atrophic gastritis | 1% | 0% |
| H. pylori infection | 2%* | 0% |
| Hyperthyroidism | 0% | 0% |
| None | 0% | 0% |
Antacids/Acid Reducers On a Frequent Basis
| Usage | <50 Years Old | 50+ Years Old |
|---|---|---|
| I take antacids or acid reducers on a frequent basis | 63%* | 51% |
| I do not take antacids or acid reducers on a frequent basis | 37% | 49%* |
* means statistically significant (P < 0.05) at 95% CI
“<50” group is defined by those younger than 50 years of age (n = 234); “50+” group is defined as those 50 years or older (n = 766)
For which of the following, if any, are you currently taking medication(s) prescribed by your doctor?
Please indicate which of the following antacid or acid reducers, if any, you take on a frequent basis (i.e., more than 2 times per week)
DISCUSSION
The findings of the Control Surveillance II sub-analysis highlight the common use of nutritional supplements and vitamins known to interfere with levothyroxine absorption among patients taking levothyroxine. A lack of adherence to labeled guidance reported in the original CONTROL Surveillance II study has been further revealed to vary by age and sociodemographic variables, including income and ethnicity.
Of note are the following findings:
- Widespread coadministration of foods and supplements containing calcium and iron
The Control Surveillance II sub-analysis reveals limited patient awareness of nutrient–levothyroxine interactions, along with the widespread use of multivitamin preparations as well as their coadministration with levothyroxine. Specifically, awareness of the potential of multivitamins to interfere with levothyroxine absorption appears to be low. Clinicians often underappreciate the presence of iron, calcium, or other interfering minerals and vitamins found in “fortified” foods which are common in the daily diet of adult Americans. This finding is concerning as these are often consumed without provider or patient recognition of their adverse effects on medication. It is also important to note that the minerals in supplements and fortified foods vary widely across products and formulations.
The extent of multivitamin consumption is not surprising when viewed against the findings of large-scale epidemiology studies. According to Bailey et al, in an analysis of the 2003-2006 National Health and Nutrition Examination Survey (NHANES), multivitamins are the most widely consumed dietary supplement in the United States, with more than one-third of the population reporting daily use. This widespread use across the general population indicates that levothyroxine taking patients are engaging in supplementation practices consistent with the general population yet have unique clinical implications due to drug nutrient interactions.
Several studies have shown that calcium and iron can cause malabsorption of levothyroxine sodium when co-administered. This is due to the binding of iron or calcium with thyroid hormone to form an insoluble or non-absorbable complex. From a clinical perspective, the ill effects of calcium and iron co-administration were demonstrated by Irving and colleagues in a retrospective population analysis of 1,491 levothyroxine-taking patients. In this analysis, the influence of calcium and iron supplements on levothyroxine were notable, with increased serum TSH concentrations of 0.27 mU/l and 0.22 mU/l (P<0.001), respectively.
Clinicians often are not aware of the correlation between the duration of iron and supplement use and the extent of their ability to interfere with levothyroxine. Mehuys et al highlight that the duration of supplement use may further complicate the clinical picture. Patients receiving long-term iron or calcium supplementation may have suboptimal or fluctuating thyroid hormone levels and progressive levothyroxine dose escalation that can be challenging to attribute to the underlying cause.
Despite the available data demonstrating reduced bioavailability with concurrent administration of interfering vitamins and nutritional supplements and FDA labeling requirements that clearly instruct patients to separate levothyroxine from calcium and iron, a substantial proportion of the participants reported simultaneous use. This disconnect suggests a knowledge gap where patients may not receive adequate counseling about these interactions during treatment initiation as patient counseling may lack specificity about which supplements to avoid or provide adequate explanation about timing requirements. It may be important to consider that even the well-informed patient may struggle with applying complex administration instructions to their daily routines and regimens. With the widespread availability of vitamins and supplements, as well as fortified foods, patient education about their effects on levothyroxine absorption is critical and highlights the importance of the role of health care providers in advising patients about how to avoid these interactions.
Patient demographics and the use of interfering foods and supplements Both regulatory and professional bodies recognize the significance of food-drug interactions which are reflected in clinical guidance regarding levothyroxine administration. Despite clear recommendations, our analysis reveals that older patients and patients with higher income were more likely to follow guidance surrounding taking levothyroxine medication after eating while younger patients and patients in lower income groups were less compliant with taking their medication at appropriate timing after eating. The analysis also highlights that younger patients with hypothyroidism may be more likely to take levothyroxine with liquids other than water and to take vitamins and supplements concomitantly with levothyroxine compared with older hypothyroid patients. This suggests that, beyond professional guidelines, clear product labeling in addition to practical and comprehensive counseling are needed to change patient behavior regarding food–levothyroxine interactions.
Managing these interactions is further complicated by widespread, often unrecognized sources of dietary calcium and iron in fortified and nutrient-dense foods (for example, milk substitutes, cereals, breads, and calcium-fortified juices). Patients may recognize obvious sources such as dairy but overlook less common natural sources (for example, sardines or leafy greens) and medication-based sources of minerals, underscoring the need for education on reading food labels and understanding both common and uncommon mineral sources. Coordinating care across the patient’s healthcare team, including nutrition specialists, may be required to manage food, supplement, and drug interactions while respecting the recommended 30–60-minute pre-meal and 4-hour post-dose timing, which may conflict with daily schedules. Even when patients understand that levothyroxine should be taken on an empty stomach, limited clarity about food composition and timing can lead to unrecognized nutrient-based interactions despite sincere efforts to adhere to instructions.
Awareness of administration guidance correlates with patient demographics Our sub-analysis findings confirm a widespread lack of patient awareness of clinical guidance that appears to be associated with patient demographics. Non-Hispanic white patients and higher income individuals show greater rates of supplement use and higher income individuals were more likely to have dietary and nutrition-focused discussions with their physicians than lower income individuals. The observed patterns mirrored national trends reported from the 2011-2014 NHANES conducted by Cowan et al. In that survey, over half of U.S. adults (52%) used at least one or more dietary supplements, which were most commonly multivitamins, and identified higher use among non-Hispanic whites, older adults, and individuals with greater income. While this is merely an association, the consistency across studies is noteworthy. These findings suggest that these patients, rather than being disengaged in their health, may rather be engaged in well-intended behaviors that create unintended medication interactions that undermine the efficacy of levothyroxine. Our results may reflect varying exposure to nutrition information by socioeconomic status with differential access to supplements, and diverse approaches to health and wellness stratified by age, ethnicity, and income. The focus for interventions to improve levothyroxine adherence should therefore consider these factors and be tailored to different patient populations in order to manage health within the context of their specific wellness routines.
Suboptimal patient counseling regarding dietary habits The sub-analysis suggests persistent gaps in counseling about levothyroxine–food and levothyroxine–supplement interactions at multiple points of care, even though these interactions are well documented. A relatively low percentage of overall study participants reported having a discussion with their healthcare provider relative to the need to administer levothyroxine in the absence of certain vitamins and nutritional supplements. The analysis shows higher coadministration rates among younger patients when supplements are used, and lower awareness of iron’s impact on levothyroxine. In our study, older participants seemingly adhered to levothyroxine administration guidance more than younger patients. However, this is not necessarily because they recall receiving those instructions from their doctors more than younger people. While younger patients in this analysis reported less supplement use, they had higher rates of coadministration when supplements were used and were also more likely to discuss proper administration and nutrition compared to older patients, suggesting a different medication knowledge gap. Although the lower overall use of vitamins and supplements can be expected in younger patients, iron being the exclusion, this potentially points to a lack of awareness of the impact of iron on levothyroxine. Even with higher rates of important HCP-patient discussions taking place, gaps in knowledge and the translation to proper administration are still missing and remain an area for improvement.
With younger participants, an important point to consider is that hypothyroidism is a chronic condition that requires daily medication adherence, medication timing precision, and the navigation of drug-supplement interactions. While not always the case, some younger adults with hypothyroidism may struggle more with daily adherence, precise timing, and managing drug and supplement interactions because they lack prior experience integrating complex medication regimens into their daily routines. In contrast, older adults already managing multiple chronic conditions may have developed practical strategies to manage proper medication administration.
Our analysis shows that higher-income patients, often assumed to have greater health literacy, demonstrate patterns of higher supplement use but lower coadministration with levothyroxine suggesting more effective medication management and more frequent nutrient-focused discussions with providers. This likely reflects greater resources to purchase supplements and to access comprehensive, prevention-oriented care with longer visits, where providers have more opportunity to recommend and contextualize supplements and proactively address supplement–medication interactions. This is in contrast to the discussion that may take place in settings with shorter, acute care focus. Supplement focused discussions with providers offer up natural opportunities to address supplement-medication interactions and allow for provider oversight of recommended supplements compared to over-the-counter items independently purchased by patients with little provider oversight.
Health literacy, though not measured in this study, is pivotal for effective management of chronic diseases like hypothyroidism as it underpins patients’ ability to understand levothyroxine use, adhere to treatment, and interpret follow-up monitoring. Low health literacy has been shown to disproportionately affect those from lower income, racial and ethnic minority groups, and lower educational backgrounds who often struggle with complex regimens. These patients may experience reduced adherence and worsened clinical outcomes.
Among hypothyroid participants in our sub-analysis, non-Hispanic White patients were less likely than other ethnic groups to discuss food allergies or sensitizing excipients in levothyroxine with their physicians, whereas higher-income patients were more likely to raise these issues than lower-income patients. This pattern suggests that even when patients show good supplement use and timing practices, they may still underreport relevant health information to their providers, creating missed opportunities to identify clinically important dietary factors.
The overall low patient reported recall of discussions with their healthcare provider about nutrition and levothyroxine use suggests that the prevalence of widespread coadministration of levothyroxine with interfering nutrients reflects a fundamental gap in how medication information is communicated. This counseling deficit is particularly evident when it comes to the use of supplements, as patients may initiate supplements with little understanding of how they may affect medication regimens. As with these over-the-counter medications, patients often overlook providing prescribers with details of their supplement use. In a survey of 31,044 patients, only 33.4% reported telling a conventional healthcare provider about their herb or nutritional supplement use. Without systematic processes for comprehensive medication reconciliation that considers use of dietary supplements and vitamins, the potential for unintended food-medication interactions can remain invisible to the patient’s care team. Addressing the widespread gaps in levothyroxine counseling identified in this sub-analysis requires changes to how information is communicated across the healthcare system.
Strategies for Improvement
The sub-analysis highlights the ongoing need to optimize patient counseling particularly as it relates to dietary habits. A relatively low percentage of overall study participants reported having a discussion with their healthcare provider relative to the need to administer levothyroxine in the absence of certain foods, vitamins, and nutritional supplements. These findings align with the broad clinical literature. Given the multifactorial nature of therapy which encompasses supplement use, dietary patterns, formulation selection, dosing, adherence, and ongoing monitoring, collaborative care among physicians, pharmacists, nurses, and dietitians is essential to avoid unintended interference with levothyroxine therapy. Pharmacists, who frequently engage with patients during medication refills, are uniquely positioned to conduct comprehensive medication reviews to identify supplement interactions, reinforce prescriber recommendations, and monitor adherence. Dietitians contribute critical expertise in tailoring dietary strategies, particularly for individuals with food intolerances, cultural considerations, or complex nutritional requirements, and can provide depth of dietary guidance beyond the scope of most physicians or pharmacists. Integrating dieticians into endocrinology practices or making them accessible through telehealth platforms could increase patient adherence to levothyroxine administration guidance. Nurses and medical assistants can further support care coordination by systematically assessing supplement use and medication timing during intake and documenting these findings within electronic health records. Overall, clear role delineation, structured communication pathways, and shared access to patient information remain foundational to achieving effective, integrated management of levothyroxine therapy.
While verbal counseling during clinical encounters is essential, accessible written materials serve as critical reinforcements that patients can reference at home or share with caregivers. However, available levothyroxine instructions are often inadequate, particularly for individuals with limited English proficiency or low health literacy. Effective educational resources should clearly name interfering substances (e.g., calcium, iron, antacids, fiber, soy products), explain their relevance to absorption, and include visual aids illustrating proper medication timing relative to meals and supplements. Materials should be written at an appropriate literacy level (approximately 6th–8th grade), use plain language and active voice, and be available in multiple languages with culturally relevant dietary examples. The development and dissemination of such standardized, multilingual, and multimodal materials made freely available through handouts, videos, and digital platforms should be coordinated by professional societies and patient advocacy organizations rather than relying on individual practices.
While these standardized improvements have been demonstrated to optimize adherence and patient outcomes, tailored interventions should be considered to improve outcomes as well. Although medication management may appear intuitive, young adults often require explicit counseling on foundational principles such as taking medication on an empty stomach, timing for optimal absorption, identifying interfering substances, and navigating real-world barriers to adherence. As patients vary in their information needs, preferences, and processing styles, education should be individualized to ensure understanding and promote effective management of hypothyroid therapy in the context of concurrent supplement and dietary use.
Regular follow-up visits provide essential opportunities to assess treatment response, address patient concerns, and reinforce adherence to levothyroxine therapy. Fluctuating thyroid function tests or persistent symptoms may indicate issues with medication timing or dietary interference rather than treatment failure, underscoring the importance of ongoing monitoring. During these visits, providers should evaluate changes in diet, supplement use, or concomitant medications and review how such factors influence therapeutic outcomes. Standardized education on the timing of levothyroxine relative to food and supplements, delivered across multiple touchpoints including prescribing, pharmacy dispensing, and regular follow-up visits can enhance patient understanding and adherence. Achieving this consistency requires systematic workflows, focusing healthcare systems on prioritizing medication optimization, interprofessional collaboration, and standardized counseling protocols to ensure every patient receives comprehensive, evidence-informed guidance regardless of care setting.
STUDY LIMITATIONS
This post hoc sub-analysis offers exploratory, real-world insight into how foods, vitamins, and supplements that may interfere with levothyroxine are used across age, ethnic, and socioeconomic groups but has several important limitations. The study relies on self-reported survey data that were not validated against medical or pharmacy records. The study did not collect thyroid hormone levels, levothyroxine dose, body weight, or indication (replacement vs TSH suppression), and excluded pregnant and pediatric patients which limits generalizability. The assessment of counseling did not capture the quality, specificity, or comprehensiveness of counseling received and did not distinguish between different counseling sources (physician, pharmacist, online source, written material). The study did not directly measure health literacy, so it cannot quantify or compare health literacy between groups. Lastly, the study was not originally powered or designed to test specific hypotheses, and overall findings regarding levothyroxine co-administration and counseling should be considered hypothesis-generating rather than confirmatory.
CONCLUSIONS
Levothyroxine has been the gold-standard treatment for hypothyroidism for over 60 years and is among the most commonly prescribed medications in the United States, with more than 110 million prescriptions dispensed in 2020. Many patients remain unaware or only partially aware that timing levothyroxine on an empty stomach with water and avoiding interacting foods, drugs, or vitamins is critical to its effectiveness, as highlighted by this sub-analysis and prior CONTROL Surveillance study findings. This analysis uniquely calls attention to the complex interactions among dietary habits, age, income, ethnicity, and chronic disease management. Its findings support the conclusion that there is room for improvement in patient counseling efforts regarding FDA recommended levothyroxine administration and the use of interfering dietary supplements, foods, and liquids, with considerations for the influence of sociodemographic variables on counseling effectiveness and patient understanding. While this study provides some useful information, additional studies may be needed to further explore these possible patterns, their causes, and clinical implications.
Conflicts of Interest:
K.R., D.C-J., and W.S. are employees of IBSA Pharma Inc. D.C. is an outside consultant for IBSA Pharmaceuticals. Way to Goal staff are paid consultants of IBSA pharmaceuticals. The authors have no other conflicts of interest to declare.
Funding Sources:
This study was supported by IBSA Pharma for the completion of the investigation.
Acknowledgements:
The authors would like to thank Carolyn Kong, Pharm.D., at IBSA USA (Parsippany, NJ, USA) for her review of the manuscript and Aesculapius Consulting, Inc. (East Brunswick, NJ, USA) for their editorial support.
References
- Chaker L, Bianco AC, Jonklaas J, Peeters RP. Hypothyroidism. Lancet. 2017;390(10101):1550-1562. doi:10.1016/S0140-6736(17)30703-1.
- American Thyroid Association, “Thyroid Hormone Treatment,” American Thyroid Association, 2024, https://www.thyroid.org/thyroid-hormone-treatment. Accessed October 21, 2024.
- Donnelly M, Fang L, Madabushi R, et al. Narrow Therapeutic Index Drugs: FDA Experience, Views, and Operations. Clin Pharmacol Ther. 2025;117(1):116-129. doi:10.1002/cpt.3460.
- Jonklaas J, Bianco AC, Bauer AJ, et al. Guidelines for the treatment of hypothyroidism: prepared by the American Thyroid Association task force on thyroid hormone replacement. Thyroid. 2014;24:1670-1751.
- Centanni M, Duntas L, Feldt-Rasmussen U, et al. ETA guidelines for the use of levothyroxine sodium preparations in monotherapy to optimize the treatment of hypothyroidism. Eur Thyroid J. 2025;14(4):e250123. doi: 10.1002/cpt.3460.
- McMillan M, Rotenberg KS, Vora K, et al. Comorbidities, concomitant medications, and diet as factors affecting levothyroxine therapy: results of the CONTROL Surveillance Project. Drugs R D. 2016;16:53-68. doi: 10.1007/s40268-015-0116-6.
- Cummings-John D, Sandulli W, Castano M, Clark D, Heidel RE. Drug administration as a factor affecting levothyroxine therapy—results of the CONTROL surveillance II study. Ann Thyroid. 2025;10:4.
- Ward LS. The difficult patient: drug interaction and the influence of concomitant diseases on the treatment of hypothyroidism. Arq Bras Endocrinol Metabol. 2010;54:435-442. doi: 10.1590/s0004-27302010000500002.
- Badillo R, Francis D. Diagnosis and treatment of gastroesophageal reflux disease. World J Gastrointest Pharmacol Ther. 2014;5:105-112. doi: 10.4292/wjgpt.v5.i3.105.
- Cohen E, Bolus R, Khanna D, et al. GERD symptoms in the general population: prevalence and severity versus care-seeking patients. Dig Dis Sci. 2014;59:2488-2496.
- Ruchala M, Szczepanek-Parulska E, Zybek A. The influence of lactose intolerance and other gastrointestinal tract disorders on L-thyroxine absorption. Endokrynol Pol. 2012;63:318-323.
- Moraga Franco CR, Falbe J, Arnold CD, Engle-Stone R. The Food Fortification Landscape in the United States: Identification and Prevalence of Fortified Food Purchases Using National Household Scanner Data. J Nutr. 2025;155(10):3321-3335. doi:10.1016/j.tjnut.2025.08.015.
- American Dietetic Association. Position of the American Dietetic Association: fortification and nutritional supplements. J Am Diet Assoc. 2005;105(8):1300-1311. doi:10.1016/j.jada.2005.06.009.
- Sadovsky R, Collins N, Tighe AP, Brunton SA, Safeer R. Patient use of dietary supplements: a clinician’s perspective. Curr Med Res Opin. 2008;24(4):1209-1216. doi:10.1185/030079908×280743.
- Bailey RL, Gahche JJ, Lentino CV, Dwyer JT, Engel JS, Thomas PR, Betz JM, Sempos CT, Picciano MF. Dietary supplement use in the United States, 2003-2006. J Nutr. 2011;141:261-266.
- Singh N, Singh PN, Hershman JM. Effect of calcium carbonate on the absorption of levothyroxine. JAMA. 2000;283(21):2822-2825. doi:10.1001/jama.283.21.2822.
- Mehuys E, Lapauw B, T’Sjoen G, et al. Investigating Levothyroxine Use and Its Association with Thyroid Health in Patients with Hypothyroidism: A Community Pharmacy Study. Thyroid®. 2023;33(8):918-926. doi:10.1089/thy.2023.0066.
- Irving SA, Vadiveloo T, Leese GP. Drugs that interact with levothyroxine: an observational study from the Thyroid Epidemiology, Audit and Research Study (TEARS). Clin Endocrinol (Oxf). 2015;82:136-141. doi: 10.1111/cen.12559.
- Shkembi B, Huppertz T. Calcium Absorption from Food Products: Food Matrix Effects. Nutrients. 2021;14(1):180. doi:10.3390/nu14010180.
- Cowan AE, Jun S, Gahche JJ, et al. Dietary Supplement Use Differs by Socioeconomic and Health-Related Characteristics among U.S. Adults, NHANES 2011-2014. Nutrients. 2018;10(8):1114. doi:10.3390/nu10081114.
- Gahche JJ, Bailey RL, Potischman N, Dwyer JT. Dietary Supplement Use Was Very High among Older Adults in the United States in 2011-2014. J Nutr. 2017;147(10):1968-1976. doi:10.3945/jn.117.255984.
- McGilton KS, Vellani S, Yeung L, et al. Identifying and understanding the health and social care needs of older adults with multiple chronic conditions and their caregivers: a scoping review. BMC Geriatr. 2018;18(1):231. doi: 10.3945/jn.117.255984.
- Gualtieri L, Rigby M, Wang D, Mann E. Medication Management Strategies to Support Medication Adherence: Interview Study With Older Adults. Interact J Med Res. 2024;13:e53513. doi:10.2196/53513.
- Coughlin SS, Vernon M, Hatzigeorgiou C, George V. Health Literacy, Social Determinants of Health, and Disease Prevention and Control. J Environ Health Sci. 2020;6(1):3061.
- Kwon DH, Kwon YD. Patterns of health literacy and influencing factors differ by age: a cross-sectional study. BMC Public Health. 2025;25(1):1556. doi:10.1186/s12889-025-22838-6.
- Kennedy J. Herb and supplement use in the US adult population. Clin Ther. 2005;27(11):1847-58. doi: 10.1016/j.clinthera.2005.11.004.
- McFarland MS, Finks SW, Smith L, et al. Medication Optimization: Integration of Comprehensive Medication Management into Practice. Am Health Drug Benefits. 2021;14(3):111-114.
Appendix
Hypothyroid Patient Survey
SURVEY LENGTH: 12-15 MINUTES (~20 QUESTIONS)
QUOTA: 1000 PATIENTS
SCREENER QUESTIONS
- Have you been formally diagnosed with hypothyroidism by a physician?
- Yes
- No TERMINATE IF SELECTED
- For which of the following, if any, are you currently taking medication(s) prescribed by your doctor? (Select all that apply)
- Acid reflux or GERD
- Atrophic gastritis
- Celiac disease
- Crohn’s disease (inflammation affecting the digestive tract)
- Food allergies
- Gastric bypass or bowel resection
- Gastroparesis (slows/stops the movement of food from the stomach)
- H. pylori infection (a bacteria that infects the stomach)
- Hypothyroidism (underactive thyroid) TERMINATE IF NOT SELECTED
- Hyperthyroidism (overactive thyroid) I & J ARE MUTUALLY EXCLUSIVE
- IBS (irritable bowel syndrome)
- Lactose intolerance
- Ulcerative colitis (inflammation affecting the colon/large bowel)
- Except I and J, none of the above MUTUALLY EXCLUSIVE
- Which of the following hypothyroid medications are you currently taking? (Select all that apply)
- Armour® Thyroid TERMINATE IF SELECTED
- Cytomel® or generic liothyronine TERMINATE IF SELECTED
- Ermeza®
- Generic levothyroxine
- Levoxyl®
- NP Thyroid® TERMINATE IF SELECTED
- Synthroid®
- ThyQuidity®
- Tirosint® (Gel capsules)
- Tirosint®-SOL (liquid solution)
- Unithroid®
- WP Thyroid® TERMINATE IF SELECTED
- Other (specify:___________) TERMINATE IF “OTHER” IS SELECTED OR IF NO SELECTION IS MADE
- What type of doctor currently prescribes your hypothyroid medication? (Select one)
- Primary Care Physician (Family doctor, Internal Medicine)
- Endocrinologist
- Thyroid Specialist
- Nurse Practitioner
- Physician Assistant
- Other (specify:___________)
- Since your diagnosis of hypothyroidism, how long have you been taking medication for hypothyroidism?
- Less than 1 year TERMINATE IF YES
- More than 1 year
- Are you currently pregnant?
- Yes. TERMINATE IF YES
- No
- What is your age?
- ___________________years (OE – number range 1-99 – MUST BE 18 OR OLDER OTHERWISE TERMINATE)
- Which of the following best represents your racial or ethnic heritage? (Select all that apply)
- Mexican American or other Hispanic MINIMUM OF 8.5% OF COMPLETES
- Non-Hispanic Black MINIMUM OF 4.2% OF COMPLETES
- Non-Hispanic White
- Other (please specify)___________________________
- Prefer not to answer
- Which of the following best represents your gender identity? (Select one)
- Male MINIMUM OF 20% OF COMPLETES
- Female
- Non-binary
- Prefer not to answer
MAIN QUESTIONNAIRE
- Since you were first diagnosed with hypothyroidism, how long have you been taking prescription hypothyroid medication(s) to treat the condition? (Select one)
- About 1-2 years
- About 3-5 years
- About 6-10 years
- More than 10 years
- How many times in the past year has your current doctor changed your prescribed hypothyroid medication to a different hypothyroid medication? (Select one)
- Never
- One time
- Two times
- Three times
- More than three times
- How many times in the past year, has your current doctor either increased or decreased the dose of your current hypothyroid medication? (Select one)
- Never
- One time
- Two times
- Three times
- More than three times
- How consistent are you in taking your medication at the same time of day, every day over the last 6 months?
- I always take it at the same time of day every day
- Most days I take it at the same time of day every day
- Sometimes I take it at the same time of day every day SKIP Q5 IF SELECTED
- I rarely take it at the same time of day every day SKIP Q5 IF SELECTED
- I never I take it at the same time of day every day SKIP Q5 IF SELECTED
- What time of day do you typically take your hypothyroid medication?
- SHOW CONTINUUM, ALLOW RESPONDENT TO SELECT AT ANY TICK MARK; ALLOW UP TO TWO SELECTIONS
- Wake up
- Breakfast
- Mid-morning
- Lunch
- Afternoon
- Dinner
- After Dinner
- Bedtime
- [ASK IF Q4 c. Breakfast, f. Lunch or h. Dinner SELECTED] When do you usually take your hypothyroid medication? (Select one.)
- Before eating
- After eating
- While eating
- [ASK IF Q5 = a. Before Eating SELECTED] How much time BEFORE eating do you typically take your hypothyroid medication? (Select one.)
- Less than 10 minutes before eating
- 10-19 minutes before eating
- 20-29 minutes before eating
- 30-39 minutes before eating
- 40-49 minutes before eating
- 50-59 minutes before eating
- 1-2 hours before eating
- More than 2 hours before eating
- [ASK IF Q5 = b. After Eating SELECTED] How much time AFTER eating do you typically take your hypothyroid medication? (Select one.)
- Less than 10 minutes after eating
- 10-19 minutes after eating
- 20-29 minutes after eating
- 30-39 minutes after eating
- 40-49 minutes after eating
- 50-59 minutes after eating
- 1-2 hours after eating
- More than 2 hours after eating
- How do you typically take your hypothyroid medication? (Select one)
- With water
- With black coffee
- With coffee and milk/cream
- With coffee and non-dairy creamer
- With tea
- With tea and milk/cream
- With milk
- With soy milk
- With juice
- With food
- With other liquid: _____ [OPEN END]
- With no liquid or food
- Which of the following vitamins, dietary or food supplements, if any, do you take on a frequent basis (i.e., more than 2 times per week)? (Select all that apply)
- Calcium
- Chromium picolinate
- Iron
- Selenium
- Potassium
- Multivitamin
- Other: _____ [OPEN END]
- None of the above [MUTUALLY EXCLUSIVE]
- [DO NOT ASK IF THEY ANSWER Q7h., “None of the above”] How often do you take vitamins, dietary, or food supplements at the same time that you take your hypothyroid medication? (Select one)
- Always
- Often
- Sometimes
- Rarely
- Never
- How often do you take any other prescription medications at the same time that you take your hypothyroid medication? (Select one)
- Always
- Often
- Sometimes
- Rarely
- Never
- I do not take any other prescription medications
- Please indicate which of the following antacid or acid reducers, if any, you take on a frequent basis (i.e., more than 2 times per week). (Select all that apply)
- AcipHex® PRESCRIPTION ACID REDUCERS
- Alka-Seltzer® NON-PRESCRIPTION ANTACIDS
- Gaviscon® NON-PRESCRIPTION ANTACIDS
- Maalox® NON-PRESCRIPTION ANTACIDS
- Nexium®, non-prescription NON-PRESCRIPTION ACID REDUCERS
- Nexium®, prescription PRESCRIPTION ACID REDUCERS
- Omeprazole, prescription PRESCRIPTION ACID REDUCERS
- Omeprazole, non-prescription NON-PRESCRIPTION ACID REDUCERS
- Pepto-Bismol® NON-PRESCRIPTION ANTACIDS
- Prevacid®, non-prescription NON-PRESCRIPTION ACID REDUCERS
- Prevacid®, prescription PRESCRIPTION ACID REDUCERS
- Prilosec®, non-prescription NON-PRESCRIPTION ACID REDUCERS
- Prilosec®, prescription PRESCRIPTION ACID REDUCERS
- Protonix® PRESCRIPTION ACID REDUCERS
- Rolaids® NON-PRESCRIPTION ANTACIDS
- Tagamet HB 200® NON-PRESCRIPTION ACID REDUCERS
- Tums® NON-PRESCRIPTION ANTACIDS
- Other non-prescription antacid or acid reducers (specify:___________) TBD, POST CODING
- Other prescription antacid or acid reducers (specify:___________) TBD, POST CODING
- I do not take any antacid or acid reducers on a frequent basis MUTUALLY EXCLUSIVE
- Has your doctor ever instructed you about the following?
- Take hypothyroid medicine each morning on an empty stomach with water before eating
- Yes
- No
- Don’t Recall
- Do not take hypothyroid medication at the same time as vitamins, dietary or food supplements
- Yes
- No
- Don’t Recall
- Do not take hypothyroid medication at the same time as other prescription medications
- Yes
- No
- Don’t Recall
- Take hypothyroid medicine each morning on an empty stomach with water before eating
- Which of the following statements best describes your attitude toward taking hypothyroid medicine each morning on an empty stomach with water before eating as instructed by your doctor? (Select all that apply)
- I have no problem doing this
- It is inconvenient for me
- I have a hard time remembering to take my hypothyroid medicine each morning before eating or drinking (coffee, tea etc.)
- I don’t have time to wait before I eat breakfast or have my morning drink (coffee, tea etc.)
- I prefer to take my medication the way that I want
- Other (specify:______)
- Have you ever stopped taking your prescribed hypothyroid medication for more than one month? (Past or present prescription)
- Yes IF YES, ASK Q12a
- No
- Which of the following were reason(s) you stopped taking your hypothyroid medication for more than one month? (Select all that apply)
- Felt better, no need to take medicine
- Medicine didn’t seem to help me
- Medication was too expensive
- My brand was not available at pharmacy
- Medication was difficult and inconvenient to take
- Insurance company wouldn’t cover my medication
- Prefer a non-drug remedy
- Medication made me feel worse
- Other (specify:______)
- Which of the following topics, if any, have you ever discussed with the doctor who currently prescribes your hypothyroid medication? (Please check all that apply)
- Vitamins, dietary or food supplements
- Allergies to excipient ingredients or “fillers” (gluten, lactose, dyes etc.)
- Nutrition
- Use of Over-the-counter (OTC) medications
- Use of other prescription medications
- Stomach or gastrointestinal conditions
- Hypothyroid medication administration (i.e., the proper way to take hypothyroid medication). IF YES, THEN QUESTION 13a
- None of the above
- Thinking back to discussions you’ve had with your doctor about how to take your hypothyroid medicine, how would you characterize those discussions?
- Not very helpful -2 -1 0 1 2 Very Helpful
- Did not receive enough information -2 -1 0 1 2 Received sufficient information
- Information was NOT new to me -2 -1 0 1 2 Information was new to me
- Confusing -2 -1 0 1 2 Clear
- Frustrating. Doctor did not answer my questions -2 -1 0 1 2 Satisfying. Doctor answered my questions
- Thinking of your overall experience of being treated for hypothyroidism, please indicate your level of agreement with the following statements:
- Nobody seems to understand or care about how I feel
- I don’t know where to get reliable information about my hypothyroid condition
- It’s hard to control my hypothyroid symptoms
- My hypothyroid condition reduces my quality of life causing me not to be able to do the things I used to do
- I am able to take on anything without being limited by my hypothyroid condition
- I am satisfied with my hypothyroid medication
- I can live life normally
- If your doctor were to recommend a liquid hypothyroid medicine, how would you feel about it? (Select one)
- I would prefer to take a tablet or capsule instead of a liquid
- If it works, I don’t care about the form of the medication
- I follow what my doctor recommends, even if it is not my preference
- I prefer liquid medications instead of other forms of medication
- What is your interest level in a liquid hypothyroid medication, on a scale of 1 to 5, where 1 means not at all interested, and 5 means extremely interested?
- 1=Not at all interested, 5= Extremely interested
- 1 Completely uninterested
- 2 Somewhat uninterested
- 3 Neither/no opinion
- 4 Somewhat interested
- 5 Completely interested
- Which category best describes your total annual household income? (Select one)
- $0-$30,000
- $31,000-$60,000
- $61,000-$90,000
- $91,000-$120,000
- $120,000+
Thank you for participating.