






Impact of Tech on Nursing Students’ IV Skills
Simulation-Based Learning: The Impact of Technology-Enhanced Education on Peripheral Vascular Access Skills
Melissa A. Bathish, PhD, RN, CPNP-PC 1; Valerie Marsh, DNP, RN, CNOR 1; Julie A. Thompson, PhD 2,3; Thomas Hopkins, MD, MBA, CPE 3; Elizabeth Weathers, PhD, RN, RGN, PGCertTLHE, FAAN 3,4
- University of Michigan School of Nursing, Ann Arbor, MI, USA
- Duke University School of Nursing, Durham, NC, USA
- AccuVein Inc., Medford, NY, USA
- School of Nursing, Midwifery, and Health Sciences, University College Dublin, Belfield, Dublin, Ireland
OPEN ACCESS
PUBLISHED: 31 August 2025
CITATION: BATHISH, Melissa A. et al. Simulation-Based Learning: The Impact of Technology-Enhanced Education on Peripheral Vascular Access Skills. Medical Research Archives. Available at: <https://esmed.org/MRA/mra/article/view/6987>.
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i9.6987
ISSN 2375-1924
Abstract
Aims and objectives: To assess the impact of a technology-enhanced teaching program on students’ knowledge, confidence, and attitudes toward peripheral intravenous catheter (PIVC) insertion and ability to select optimal insertion sites.
Background: Near-infrared technology enhances venous assessment and can reduce the number of insertion attempts. Yet, adoption of near-infrared technology is limited.
Design: A randomized, controlled, interventional study design (Phase 1) and an observational design (Phase 2) were used.
Methods: Data on knowledge, confidence, and attitudes toward the technology were collected, along with assessments of students’ ability to select optimal PIVC sites on patients with diverse skin tones.
Results: The program increased students’ knowledge and confidence. Near-infrared technology improved students’ ability to visualize vasculature in patients with dark skin and enabled objective assessment and adherence to evidence-based practices.
Conclusions: Technology-enhanced education improves nursing students’ PIVC skills and promotes equitable care by enhancing insertion outcomes for patients with diverse skin tones.
Keywords: peripheral intravenous catheter insertion, vascular access, vein visualization technology, nursing student, education.
Introduction
Each year in the United States (US), more than 300 million peripheral intravenous catheters (PIVCs) are inserted, marking it the most frequently performed invasive healthcare procedure. Placing a single PIVC typically requires an average of 2.18-2.35 attempts, with success influenced by patient characteristics, provider experience, and confidence. Multiple access attempts not only increase the utilization of healthcare resources but also elevate the risk of adverse outcomes such as venous depletion, nerve damage, paresthesia, hematomas, phlebitis, and arterial puncture. Furthermore, the incidence of hospital-acquired PIVC site infections can reach up to 60%, with the insertion technique being a crucial factor associated with infection rates.
Nurses—often new graduates or those with limited experience—frequently undertake the placement of PIVCs. The first-attempt success rates for newly qualified nurses range from 44-76.9%, in contrast to the 91-98% success rates observed in more experienced nurses. Across the US, significant variability exists in PIVC education and training within nursing programs. Interviews with undergraduate nursing students revealed that the current university curriculum provides limited foundational knowledge about PIVC assessment, management, and removal. Inconsistencies between the curriculum and clinical practice create uncertainty, impacting nurses’ ability to follow evidence-based guidelines. This inconsistency in PIVC education for nurses contributes to a knowledge deficit in clinical practice.
Vandenhouten et al. emphasized the importance of nursing students being acquainted with PIV skills in nursing school, as nurses constitute the largest group responsible for the placement and oversight of peripheral intravenous (PIV) therapy. Existing literature highlights that many newly graduated nurses often lack the confidence, knowledge, and proficiency to place and maintain PIVC insertion sites successfully. Addressing this knowledge gap is crucial for avoiding PIVC complications, improving the quality of care, and enhancing patient safety.
Over the past decade, technologies like near-infrared (NIR) vein visualization, which enhance venous assessment and improve PIVC placement, have become widely accessible. Evidence suggests that NIR technology can significantly enhance clinical practice by enabling a swift and thorough venous assessment. This includes the identification of valves and bifurcations, as well as the observation of vein patency and refill speed. NIR technology can potentially reduce the number of attempts and the time required for successful PIVC placement, particularly in patients with challenging venous access. A study by van der Woude and colleagues explored the application of NIR technology in the operating room for IV cannulations in children with dark skin. The findings revealed a 68% success rate in the group utilizing NIR technology compared to 51% in the control group. The study highlighted the inherent difficulty of initiating IV cannulations in children, further exacerbated in individuals with dark skin due to the limited contrast between vein visibility and skin color. This underscores the potential of NIR technology as a valuable tool to improve success rates in challenging scenarios.
Consequently, professional organizations, such as the Emergency Nurses Association, the Infusion Nurses Society, and the Association for Vascular Access, now recommend using vein visualization technology during PIVC placement. Despite these recommendations, the adoption of this advantageous technology remains limited. The hypothesis is that educating student nurses about the benefits of NIR technology and providing them with the opportunity to use it in a simulated environment will enhance the learning experience. This, in turn, is expected to increase students’ perceived confidence and comfort with PIV assessment and placement, ultimately leading to improvements in patient care and further adoption of vein visualization technology.
STUDY PURPOSE
This study addressed the current knowledge gap by introducing an innovative, technology-enhanced PIVC teaching program for baccalaureate nursing students at an academic institution in the US. The purpose of the educational initiative was to evaluate whether technology-enhanced education improves procedural competence and preparedness in peripheral vascular access.
The primary aims were to: (1) evaluate students’ knowledge and confidence of PIVC placement, (2) improve students’ proficiency in performing a comprehensive pre-insertion site assessment and selecting an optimal insertion site, and (3) assess students’ attitudes toward the use of NIR vein visualization technology for successful PIVC placement.
Methods
To achieve the objectives of this study, an exploratory intervention study was conducted. The Standards for Quality Improvement Reporting Excellence (SQUIRE 2.0) health research reporting guidelines were adhered to.
SETTING AND SAMPLE
The study was conducted at a prestigious academic university in the Midwest of the US. Research participants included fourth-year baccalaureate nursing students enrolled in a 12-week capstone course. The course featured a weekly 3-hour didactic lecture and 224 hours of clinical immersion experience in either a pediatric or adult high-acuity/critical care unit.
STUDY DESIGN AND INTERVENTION
The didactic portion of the capstone course included a comprehensive PIVC curriculum which outlined the indications for PIVC insertion, the procedural steps for insertion and removal, catheter management, potential complications, and appropriate patient education. The educational content on NIR vein visualization technology (AccuVein®, Inc.; Medford, NY, USA) was integrated into the existing PIVC placement educational curriculum. An overview of the study design and research questions is shown in
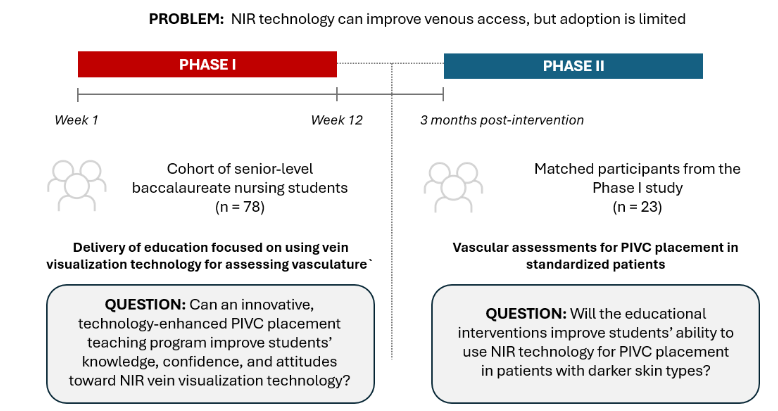
. All participants were required to complete pre-readings for the standard PIVC session and respond to a pre-education survey. Following this, participants were randomly assigned to either the intervention or control group and directed to the respective room, as illustrated in
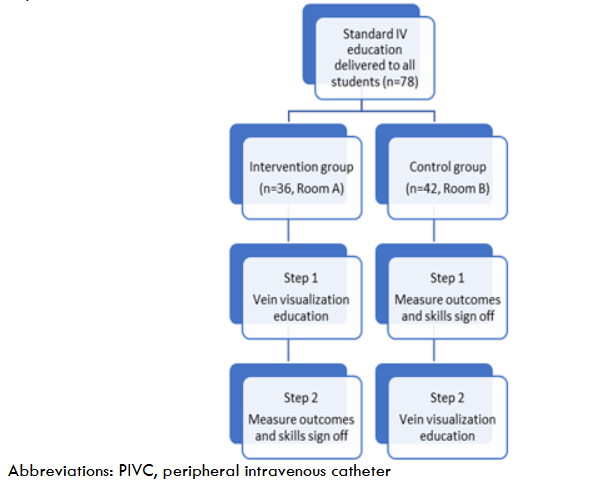
.
Phase 1.
The intervention group was provided with specific content that included both a theoretical component and a skills station. The theoretical aspect consisted of a concise presentation along with an animated video demonstrating the application of vein visualization technology for assessing vasculature. During the simulated skills session using arm task trainers, nursing students had the opportunity to practice using the device to assess vasculature, select a site, and perform actual PIVC placement. Students in the control group only received the didactic instruction followed by a skills competency assessment. Subsequently, students in the control group crossed over to engage in the technology-enhanced component of the intervention. This approach ensured that all students received faculty sign-off on PIVC competency and had equal exposure to the technology-enhanced education session. Outcomes were assessed immediately after the education and three months later.
Phase 2.
Three months after the educational intervention, all students were invited to participate in an observational assessment to evaluate their competence in performing a vascular site assessment and choosing an optimal site for PIVC insertion. Each student was evaluated on their ability to successfully place a PIVC across four scenarios (i.e., in a light-skinned and dark-skinned standardized patient (SP), with or without the assistance of NIR vein visualization technology). All students had to perform two assessments: one on the light-skinned patient and one on the dark-skinned patient. The assignment to use NIR or no NIR was random. Four evaluators performed evaluations of student ability. Two evaluators were with the light-skinned SP and two were with the dark-skinned SP. All evaluators were trained on the assessment tool immediately before the study. The two evaluators at each station had to agree on the scores assigned to each student.
DATA COLLECTION
Following approval from the Institutional Review Board (HUM00233818), data collection was conducted electronically using Qualtrics Survey Software (Qualtrics, 2020). Participants were provided with QR codes that enabled them to access study consent and pre- and post-education surveys using their personal devices. Before each survey, participants were instructed to create a unique, de-personalized identifier. They were guided to devise easily memorable identifiers that did not contain sufficient information for personal identification. In this study, the individual’s identifier was constituted by the last four digits of their phone number, followed by their middle initial.
SURVEY DESIGN
The pre-education survey was distributed to both study groups before the PIVC curriculum. Demographic data were collected first (see Appendix 1). The knowledge and confidence questionnaire, which was adapted from Indarwati et al. featured seven multiple-choice items assessing prior knowledge of PIVC insertion (see Appendix 2) and 14 questions assessing students’ confidence related to PIVC placement on a five-point Likert scale (see Appendix 3). Participants self-rated their confidence, ranging from 1 = Strongly Disagree to 5 = Strongly Agree.
The post-survey was administered to both study groups to reassess PIVC insertion knowledge and confidence following the educational intervention. For the intervention group, the outcome measurement occurred after participating in both the standard and enhanced education sessions. Apart from the core questions, the intervention group responded to seven additional questions evaluating their attitudes toward NIR vein visualization technology for PIVC insertion using a 5-point Likert scale (see Appendix 4). The control group underwent outcome measurement immediately after completing the standard education session.
KNOWLEDGE AND CONFIDENCE SCORING
To evaluate knowledge, the cumulative score for each participant on the 14-item knowledge survey was computed before and after the intervention. Each correct answer was awarded one point, while incorrect responses received zero points, resulting in a maximum achievable score of 15. Internal consistency was evaluated using Kuder-Richardson (KR) 20 values, which indicated very low reliability at pre, KR20 = .094, and fair reliability at post, KR20 = .509. The low consistency values were likely due to the 14 knowledge questions assessing various constructs within PIVC insertion, including education, documentation, steps for insertion, and risk factors. To evaluate confidence, the sum scores of confidence items were calculated, with a maximum achievable score of 70 points derived from 14 items utilizing a 5-point Likert scale ranging from 1=Strongly Disagree to 5=Strongly Agree. Higher scores indicated higher confidence levels. Internal consistency was evaluated using Cronbach’s alphas and indicated strong reliability, α= .945 for pre, α = .957 for post, and α = .924 at 3 months.
STATISTICAL ANALYSIS
Data were analyzed using IBM SPSS version 29, with the significance level set at .05. Demographic variables between the control and intervention groups were compared using chi-square tests. For the Phase 1 analysis, descriptive statistics (percent change calculations) and a mixed model ANOVA, with control/intervention as the between-groups variable, were employed to explore changes in knowledge and confidence scores over time. Descriptive statistics (mean, standard deviation, median) were used to analyze attitudes toward utilizing NIR vein visualization technology for PIVC placement. The assessment of ability involved chi-square tests for each skill related to PIVC insertion attempts. Exploratory analyses were conducted to examine whether variables such as prior experience with PIVs or previous training were associated with changes in knowledge and confidence over time. The initial analysis included univariate tests to identify potential associations. In cases where a significant association was detected in the univariate testing, general linear models were applied, introducing prior experience and/or previous training as additional factors.
During Phase 2, the confidence levels of matched participants were evaluated through repeated measures analysis of variance (ANOVA) across three time points (pre-, post-, and Phase 2). Subsequently, independent samples t-tests were conducted to confidently examine the association between PIVC placement experience (yes/no) and prior PIVC insertion training (yes/no).
Results
Table 1 presents demographic information, including age, sex, and prior training or experience in PIVC insertion or venipuncture. A total of 78 senior baccalaureate nursing students participated in the study, with 36 in the intervention group and 42 in the control group.
| Control | n = 42 | Intervention | n = 36 | P-value |
|---|---|---|---|---|
| Age | .593 | Mean (SD) | 20-29 years, n (%) 41 (97.6) 34 (94.4) | 30-39 years, n (%) 1 (2.4) 5 (2.6) |
| Sex | .460 | Female | 39 (92.9) 31 (86.1) | Male 3 (7.1) 5 (13.9) |
| Education and Experience | Previous PIVC insertion or venipuncture training 11 (26.2) 10 (27.8) .999 | Previous PIVC insertion or venipuncture experience 7 (16.7) 9 (25.0) .409 |
Phase 1
Knowledge scores.
The intervention group had 35 participants, and the control group had 40 participants, with complete data at both time points. A mixed-model ANOVA, incorporating control/intervention as the between-groups variable, was utilized to examine the change in mean knowledge scores over time. Detailed ANOVA results are presented in
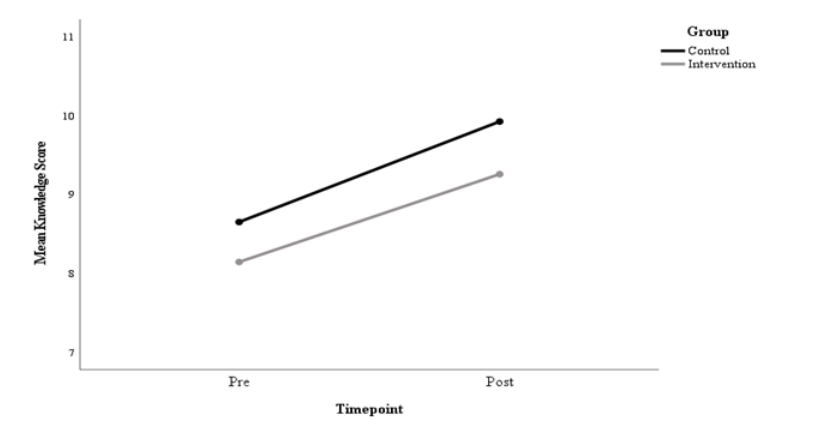
.
Mixed Model ANOVA Summary for Knowledge
Group Pre Post F (1, 73) p ηp2
Control 8.65 (1.99) 9.93 (2.30) 18.03 <.001 .965
Intervention 8.14 (1.85) 9.26 (2.28)
Note: Time (Pre/Post) x Group p = .77
The overall ANOVA test indicated a significant impact of time on knowledge. However, the group-by-time interaction did not achieve significance, suggesting that both groups exhibited significant knowledge improvement at a comparable rate. Additionally, there were no statistically significant differences between the groups in knowledge scores at pre- (P = .206) and post- (P = .212) assessments. The intervention group’s knowledge scores improved by 13.8%, and the control group’s improved by 14.8%.
Univariate analyses were conducted to examine potential relationships between demographic variables, specifically prior experience with PIVCs and previous training with knowledge. The findings revealed no significant associations between prior experience (P = .518) and previous training (P = .881) with knowledge. As a result, a general linear model (GLM) incorporating these factors was not pursued for knowledge.
Confidence scores.
Confidence scores in the intervention group improved by 30.2% from baseline, and scores in the control group improved by 26.8%, although this difference was not statistically significant. The results of the ANOVA are presented in

.
Mixed Model ANOVA Summary for Confidence
Group Pre Post F (1, 73) p ηp2
Control 46.34 (10.09) 58.76 (5.75) 173.64 <.001 .701
Intervention 46.66 (10.13) 60.74 (6.74)
Note: Time (Pre/Post) x Group p = .409
In contrast to knowledge scores, when examining confidence, univariate analyses revealed associations with both prior experience (P = .046) and previous training (P = .035). These variables were found to be highly correlated (p = .009). Consequently, a general linear model (GLM) was implemented, incorporating baseline confidence as a covariate and introducing prior experience (yes/no) as an additional factor to determine if the intervention influenced confidence when considering these additional variables and accounting for baseline confidence. The outcomes revealed that baseline confidence significantly predicted post-education confidence, but neither prior experience (P = .526) nor “group” (control vs intervention, P = .905) significantly impacted post-education confidence.
NIR technology evaluation.
Participants in the intervention group evaluated NIR technology education using eight items on a 5-point Likert scale. Possible responses to these items ranged from 1 (Strongly Disagree) to 5 (Strongly Agree). The descriptive statistics for the NIR technology evaluation are presented in
| Item | M | Mdn | SD | Min | Max |
|---|---|---|---|---|---|
| I found the near-infrared education session helpful | 4.49 | 5 | 0.56 | 3 | 5 |
| I received useful information today on how to use near-infrared technology | 4.57 | 5 | 0.56 | 3 | 5 |
| I would recommend the near-infrared education session to my colleagues/peers | 4.57 | 5 | 0.50 | 4 | 5 |
| I found the near-infrared device easy to use | 4.60 | 5 | 0.50 | 4 | 5 |
| I would feel more confident placing a PIVC using the near-infrared device | 4.60 | 5 | 0.50 | 4 | 5 |
| I would like to use the near-infrared device on all my patients | 4.57 | 5 | 0.56 | 3 | 5 |
| I think the near-infrared device would enhance my ability to select an optimal site for PIVC insertion | 4.60 | 5 | 0.50 | 4 | 5 |
| I think the near-infrared device would enhance my ability to insert a PIVC | 4.60 | 5 | 0.50 | 4 | 5 |
.
Likert scale response options: 1 -Strongly Disagree to 5- Strongly Agree
Abbreviations: Mdn = median; M = mean; PIVC = peripheral intravenous catheter; SD = standard deviation.
Qualitative assessment of the educational sessions.
Participants were invited to provide additional comments regarding their experience with the education session (Table 3). Comments from both groups highlighted the usefulness of the education and their satisfaction with the overall experience. Other students commented on the perceived benefits of the technology in clinical practice and provided topics for additional education (i.e., phlebotomy training).
| Intervention group | Theme | Examples |
|---|---|---|
| Applicability | “it was fun and educational” | “I believe it would be very helpful in practice” |
| Positive learning experience | “loved it” | “such a cool experience” |
| Clinical benefit of technology | “I believe it would be very helpful in practice” | “Highly recommend [near infrared] device to minimize risk for PIV” |
| Control group | Theme | Examples |
|---|---|---|
| Applicability | “very informational and helpful” | |
| Positive learning experience | “it was a great session” | “great learning experience” |
| Areas of educational need | “a phlebotomy class would be really beneficial” |
Phase 2
Demographics.
At each time point in the study, the students were asked to provide their unique identifiers so that their results could be tracked. However, some of the students entered an incorrect identifier or did not enter one at all. Of the 35 respondents in Phase 1, a total of 23 participants were matched from Phase 1 to Phase 2 based on their unique identifiers. There were 20 females (87%) and three males (13%), and most (96%) were between the ages of 20 and 29 years of age.
PIVC insertion experience post-education.
When asked if they had an opportunity to place a PIVC in clinical practice after completing the education, 12 (52%) of the nursing students reported they did not, and 11 (48%) reported they did. Of the 11 that did have an opportunity to place a PIVC, six (55%) had one placement, and five (45%) had more than one placement.
Confidence scores.
Mean confidence scores improved by 20.9% from pre- to post-education. This improvement was generally sustained at Phase 2, with a 9.5% improvement over pre-education scores. Repeated measures ANOVA was conducted to examine changes in confidence from Phase 1 (pre, post) to Phase 2. Figure 5 shows the mean confidence scores across all three measurement points. The overall findings showed a statistically significant improvement in confidence F (2, 42) = 24.41, P < .001. Pairwise comparisons showed a statistically significant improvement from Phase 1 pre to Phase 1 post (P < .001) and then a significant decline from Phase 1 post to Phase 2 (P = .002). However, despite the considerable decline in Phase 2, the mean was still significantly higher than Phase 1 pre-confidence scores (P = .003).

Notably, real-world practice in utilizing NIR vein visualization technology influenced confidence scores. An independent samples t-test was executed to compare the confidence scores of 11 participants with at least one PIVC placement with the scores of 12 participants who did not have an opportunity for a PIVC placement in practice. The results indicated a slightly higher mean confidence score for those with at least one PIVC placement compared to those without, though the observed difference did not achieve statistical significance (P = .487).
PIVC objective site assessment.
A total of 68 PIVC insertion site assessments were performed by the phase 2 cohort of 35 students. Chi-square tests were employed to assess each skill involved in PIVC insertion attempts, and the outcomes are presented in Table 4. The sample sizes for each scenario varied from 12 to 18 based on available data. Skills such as locating bifurcations, distinguishing between superficial and deep veins, locating valves, determining vein patency, and selecting an optimal vein for insertion were significantly less successful without NIR technology in the light-skinned and dark-skinned SP compared to the other three scenarios. With regard to selecting an optimal vein for insertion, the success rate without NIR was 73% lower in the dark-skinned standardized patient compared to 29% lower in the light-skinned SP. This suggests that practitioners performing insertions on individuals with dark skin tones may achieve better outcomes by utilizing NIR technology for these specific procedures.
| Skill | Scenario A: Pale Skin SP with NIR Technology | Scenario B: Pale Skin SP without NIR Technology | Scenario C: Dark Skin SP with NIR Technology | Scenario D: Dark Skin SP without NIR Technology | N | % Successful | |||
|---|---|---|---|---|---|---|---|---|---|
| Correctly assess veins with wipe technique | 17 | 94% | 16 | 0% | 14 | 86% | 17 | 0% | <.001 |
| Locate bifurcations | 17 | 100% | 17 | 100% | 15 | 93% | 18 | 39% | <.001 |
| Identify superficial vs deep veins | 17 | 88% | 17 | 82% | 15 | 100% | 18 | 22% | <.001 |
| Locate valves | 17 | 94% | 17 | 0% | 15 | 93% | 18 | 22% | <.001 |
| Determine vein patency | 17 | 94% | 17 | 0% | 15 | 100% | 18 | 6% | <.001 |
| Select an optimal vein for insertion | 17 | 100% | 17 | 71% | 15 | 73% | 18 | 0% | <.001 |
| Tourniquet use | 17 | 29% | 17 | 100% | 12 | 33% | 17 | 94% | <.001 |
Abbreviations: NIR = near-infrared; PIVC = peripheral intravenous catheter; SP = standardized patient.

Skills like accurately assessing veins with the wipe technique, locating valves, determining vein patency, and utilizing a tourniquet were performed with greater success in the light-skinned SP versus the dark-skinned patient, regardless of whether NIR technology was used. This suggests that individuals equipped with NIR technology, irrespective of the SP’s skin tone, demonstrated a higher proficiency in locating valves than those without NIR technology. For both the light-skinned and dark-skinned SPs, tourniquet utilization was notably higher when NIR-assisted technology was not used.
Discussion
This study aimed to enhance students’ knowledge, skills, and confidence by implementing an innovative, technology-enhanced PIVC teaching program for baccalaureate nursing students in a US academic institution. As technology continues to shape the healthcare landscape, its integration into nursing education is crucial for preparing competent and skilled nursing professionals.
Due to the invasive nature of peripheral vascular access insertion and the morbidity associated with complications, practitioners must demonstrate competency before performing the phlebotomy or PIVC placement without supervision. Currently, there is no universal guidance for training on PIVC assessment and placement. The Infusion Therapy Standards of Practice (Standards) recognize the importance of using blended learning methods to improve learner knowledge and competence regarding peripheral vascular assessment and PIVC placement procedures. Furthermore, the Standards recommend using simulation methods to develop and cultivate skills in performing invasive procedures such as PIVC insertion.
This study investigated the impact of a comprehensive peripheral vascular access education program on nursing students’ knowledge of PIVC insertion, confidence with PIVC insertion skills, attitudes toward using NIR vein visualization technology for PIVC placement, as well as participants’ ability to perform a thorough pre-insertion site assessment and their ability to select an optimal site for insertion. Data from the current study aligns with available evidence supporting the integration of simulation-based training into the modern nursing education curriculum to enhance nursing students’ knowledge, competence, and confidence.
The ability to visualize veins accurately is fundamental to successful phlebotomy and PIVC placement. NIR visualization technology offers real-time imaging of superficial and subcutaneous veins, providing nursing students with enhanced visibility compared to traditional methods of assessment. Prior research has demonstrated a significant improvement in the speed and precision of vein selection among nurses exposed to NIR technology. Furthermore, this technology promotes a deeper understanding of anatomical variations in vein structures, contributing to a more comprehensive knowledge base and skill set among nursing students. As educators, we recognize the importance of accelerated skill acquisition, and NIR technology has emerged as a valuable tool in achieving this goal.
In the current study, students’ ability to perform a pre-insertion assessment and identify a suitable vein was significantly improved when NIR technology was used compared with traditional methods. This study builds on available evidence demonstrating that dark-skinned patients are at a disadvantage when it comes to PIVC placement, as darker skin makes it more difficult to find an appropriate site to perform phlebotomy or place a PIVC. Also, the current findings support using NIR technology to address this clinical practice gap. When using NIR on dark skin, students’ ability to identify venous bifurcations, differentiate between superficial and deep veins, locate valves, and determine the patency of veins was greater than when using the traditional technique of using a tourniquet and palpating the veins. Although the use of NIR also improved vascular assessment in the light-skinned simulated patient, the improvement observed with the dark-skinned simulated patient was significantly more pronounced. Globally, nursing school initiatives focus on building a culture of diversity, equity, and inclusion (DEI) to advance health care. These findings suggest that integrating NIR training into curricula may serve as a practical strategy to operationalize diversity, equity, and inclusion commitments within nursing education.
Ensuring patient safety and providing equitable care are paramount in nursing education. The integration of NIR technology not only promoted equitable and safe practices for peripheral vascular assessment but also enriched the learning experience for students. NIR has been shown to decrease unsuccessful insertion attempts and venous puncture-related complications. Reducing complications related to PIVC insertion has far-reaching implications, including minimizing patient discomfort and mitigating the risk of infections associated with multiple insertion attempts. NIR technology’s enhanced visualization ultimately enhances patient safety. This aspect underscores the importance of technology not only in skill development but also in promoting patient-centered and equitable care. Equity in vascular access enhances the patient’s experience and reduces disparities in healthcare outcomes. By adopting NIR technology, nurses become advocates for equitable care, fostering a healthcare environment that prioritizes the unique needs of patients.
The economic considerations of integrating technology into nursing education are pertinent to the discussion. While initial costs may be associated with adopting NIR visualization technology, the potential long-term benefits may justify this investment. The potential reduction in procedure-related complications and improved skill acquisition contribute to overall cost-effectiveness. Additionally, financial benefit may be realized in terms of reduced PIV access supply use (secondary to improved first attempt access success) and reduced staff and care escalations. Finally, it is possible to enhance revenue generation for vascular access teams by reallocating high-value resources away from phlebotomy and PIVC placement and toward billable procedures such as midline and PICC placement.
It is important to acknowledge the challenges associated with integrating this technology. Ongoing updates, faculty training, and financial considerations are crucial factors. Moreover, faculty training and curriculum alignment are imperative to ensure that technology is integrated in a substantial manner and that students continue to develop traditional assessment skills, rather than becoming overly reliant on devices.
Simulation-based learning has become a cornerstone of nursing education, bridging theoretical knowledge and clinical practice. NIR technology seamlessly integrates into simulation education, offering a realistic environment for students to practice PIV catheter insertion. The implications of this integration extend beyond skill acquisition, impacting the students’ confidence and readiness for real-world application. While simulation-based improvements are encouraging, an important question is whether these skills transfer to clinical environments characterized by patient comorbidities, time constraints, and variable supervision. Confidence gains were partially sustained at three months, but real-world opportunities to practice PIVC insertion were limited for many students. This underscores the need to link simulation exposure with repeated clinical practice opportunities to maintain competence and ensure translation of skills to bedside performance.
This study is subject to certain limitations. It was conducted at a single academic institution with a relatively small sample size, which may limit generalizability. Confidence was also self-reported and may not fully reflect objective competence. Future research should examine patient-centered outcomes such as comfort, satisfaction, and trust, as well as conduct cost-effectiveness analyses in real-world settings to provide more substantial justification for the adoption of NIR technology in both education and practice. In addition, longitudinal and multi-institutional studies are needed to determine whether simulation-based improvements translate into sustained clinical performance and to inform the development of a standardized nursing curriculum for vascular access training.
Conclusion
The integration of NIR visualization technology into nursing education for PIVC placement enhanced students’ knowledge, confidence, and ability to perform comprehensive vascular assessments in a simulated care setting. Notably, the findings highlight the potential of NIR technology to reduce disparities in vascular access by improving site selection among patients with darker skin tones, thereby advancing equity in care. Beyond skill acquisition, NIR-supported simulation offers a valuable pathway to strengthen clinical preparedness, promote patient safety, and align nursing curricula with evidence-based standards. Future work should focus on translating these educational gains into clinical outcomes and evaluating cost-effectiveness to guide broader adoption. Embracing technology-enhanced education represents an important step toward preparing competent, confident nurses and ensuring safe, equitable vascular access for all patients.
Conflicts of Interest and Source of Funding
We, the authors of the manuscript titled “Simulation-Based Learning: The Impact of Technology-Enhanced Education on Peripheral Vascular Access Skills”, would like to disclose the following potential conflicts of interest:
- Three authors, Elizabeth Weathers, Thomas Hopkins, and Julie A. Thompson, currently hold consultancy roles with AccuVein Inc. This company specializes in vein visualization technology.
- This technology is related to the subject matter discussed in the manuscript.
The other authors do not have a conflict of interest to disclose.
Every effort has been made to ensure that the research and findings presented in this manuscript are objective and unbiased, and we have taken measures to mitigate any influence this affiliation may have had on the design, conduct, analysis, and reporting of the research. The data and conclusions presented in this manuscript are based on thorough and rigorous research procedures. This was a collaborative study in which all authors had input and oversight of every research study step, including study design, IRB application and approval, data collection and analysis, write-up, and dissemination.
We are committed to transparency and the integrity of the research process. As such, we felt it necessary to declare this potential conflict of interest to ensure that readers, reviewers, and editors have all the necessary information to assess the objectivity and credibility of our work.
We are willing to provide additional information to the editors and reviewers to address any concerns regarding the influence of the conflict of interest on the research outcomes and conclusions presented in this manuscript.
Disclosure Statement: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- Alexandrou E, Ray-Barruel G, Carr PJ, et al. Use of short peripheral intravenous catheters: characteristics, management, and outcomes worldwide. J Hosp Med. 2018;13(5): doi: 10.12788/jhm.3039
- Marsh N, Webster J, Ullman AJ, et al. Peripheral intravenous catheter non-infectious complications in adults: a systematic review and meta-analysis. J Adv Nurs. 2020;76(12):3346-3362. doi: 10.1111/jan.14565
- Carr PJ, Rippey JCR, Budgeon CA, Cooke ML, Higgins N, Rickard CM. Insertion of peripheral intravenous cannulae in the emergency department: factors associated with first-time insertion success. J Vasc Access. 2016;17(2):182-190. doi: 10.5301/jva.5000487
- Keleekai NL, Schuster CA, Murray CL, et al. Improving nurses’ peripheral intravenous catheter insertion knowledge, confidence, and skills using a simulation-based blended learning program: a randomized trial. Simul Healthc. 2016;11(6):376-384. doi: 10.1097/SIH.0000000000000186
- Loon FHJV, Puijn LAPM, Houterman S, Bouwman ARA. Development of the A-DIVA Scale: a clinical predictive scale to identify difficult intravenous access in adult patients based on clinical observations. Medicine (Baltimore). 2016;95(16):e3428. doi: 10.1097/MD.0000000000003428
- Helm RE, Klausner JD, Klemperer JD, Flint LM, Huang E. Accepted but unacceptable: peripheral IV catheter failure. J Infus Nurs. 2015;38(3):189-203. doi: 10.1097/NAN.0000000000000100
- Brown RA, Crookes PA, Iverson D. An audit of skills taught in registered nursing preparation programmes in Australia. BMC Nurs. 2015;14:68. doi: 10.1186/s12912-015-0113-7
- Massey D, Craswell A, Ray-Barruel G, et al. Undergraduate nursing students’ perceptions of the current content and pedagogical approaches used in PIVC education. A qualitative, descriptive study. Nurse Educ Today. 2020;94:104577. doi: 10.1016/j.nedt.2020.104577
- Vizcarra C, Cassutt C, Corbitt N, Richardson D, Runde D, Stafford K. Recommendations for improving safety practices with short peripheral catheters. J Infus Nurs. 2014;37(2):121-124. doi: 10.1097/NAN.0000000000000028
- Etafa W, Wakuma B, Tsegaye R, Takele T. Nursing students’ knowledge on the management of peripheral venous catheters at Wollega University. PLoS One. 2020;15(9):e0238881. doi: 10.1371/journal.pone.0238881
- Simonetti V, Comparcini D, Miniscalco D, Tirabassi R, Di Giovanni P, Cicolini G. Assessing nursing students’ knowledge of evidence-based guidelines on the management of peripheral venous catheters: a multicentre cross-sectional study. Nurse Educ Today. 2019;73:77-82. doi: 10.1016/j.nedt.2018.11.023
- Vandenhouten CL, Owens AK, Hunter MR, Raynak A. Peripheral intravenous education in North American nursing schools: a call to action. J Nurs Educ. 2020;59(9):493-500. doi: 10.3928/01484834-20200817-03
- Hunter MR, Vandenhouten C, Raynak A, Owens AK, Thompson J. Addressing the silence: a need for peripheral intravenous education in North America. JAVA. 2018;23(3):157–165. doi: 10.1016/j.java.2018.06.001
- Indarwati F, Munday J, Keogh S. Nurse knowledge and confidence on peripheral intravenous catheter insertion and maintenance in pediatric patients: a multicentre cross-sectional study. J Pediatr Nurs. 2022;62:10-16. doi: 10.1016/j.pedn.2021.11.007
- Ahlin C, Klang-Söderkvist B, Johansson E, Björkholm M, Löfmark A. Assessing nursing students’ knowledge and skills in performing venepuncture and inserting peripheral venous catheters. Nurse Educ Pract. 2017;23:8-14. doi: 10.1016/j.nepr.2017.01.003
- Osti C, Khadka M, Wosti D, Gurung G, Zhao Q. Knowledge and practice towards care and maintenance of peripheral intravenous cannula among nurses in Chitwan Medical College Teaching Hospital, Nepal. Nurs Open. 2019;6(3):1006-1012. doi: 10.1002/nop2.288
- Pitts S, Ostroff M. The use of visualization technology for the insertion of peripheral intravenous catheters. JAVA. 2019;24(3):10–14. doi: 10.2309/j.java.2019.003.007
- Aulagnier J, Hoc C, Mathieu E, Dreyfus JF, Fischler M, Le Guen M. Efficacy of AccuVein to facilitate peripheral intravenous placement in adults presenting to an emergency department: a randomized clinical trial. Acad Emerg Med. 2014;21(8):858-863. doi: 10.1111/acem.12437
- Eren H, Caliskan N. Effect of a vein imaging device and of fist clenching on determination of an appropriate vein and on catheter placement time in patients receiving chemotherapy: a randomized controlled trial. Cancer Nurs. 2022;45(2):105-112. doi: 10.1097/NCC.0000000000000931
- Guillon P, Makhloufi M, Baillie S, Roucoulet C, Dolimier E, Masquelier A-M. Prospective evaluation of venous access difficulty and a near-infrared vein visualizer at four French haemophilia treatment centres. Haemophilia. 2015;21(1):21-26. doi: 10.1111/hae.12513
- Kanipe W, Shobe K, Li Y, Kime M, Smith-Miller CA. Evaluating the efficacy and use of vein visualization equipment among clinical nurses in an intermediate care environment. J Infus Nurs. 2018;41(4):253-258. doi: 10.1097/NAN.0000000000000286
- Parker SIA, Benzies KM, Hayden KA, Lang ES. Effectiveness of interventions for adult peripheral intravenous catheterization: a systematic review and meta-analysis of randomized controlled trials. Int Emerg Nurs. 2017;31:15-21. doi: 10.1016/j.ienj.2016.05.004
- Sriparkdee C, Sawangwong S, Curry P, Tatiyanupunwong S. A randomized controlled trial comparing the AccuVein AV400 device to standard insertion technique for peripheral intravenous cannulation by experienced nurse anesthetists in obese patients undergoing elective surgery. Thammasat Medical Journal. 2016;16(4):546–552.
- van der Woude OCP, Cuper NJ, Getrouw C, Kalkman CJ, de Graaff JC. The effectiveness of a near-infrared vascular imaging device to support intravenous cannulation in children with dark skin color: a cluster randomized clinical trial. Anesth Analg. 2013;116(6):1266-1271. doi: 10.1213/ANE.0b013e31828e5bde
- Nickel B, Gorski L, Kleidon T, et al. Infusion therapy standards of practice, 9th edition. J Infus Nurs. 2024;47(1S Suppl 1):S1-S285. doi: 10.1097/NAN.0000000000000532
- Adhikari S, Schmier C, Marx J. Focused simulation training: emergency department nurses’ confidence and comfort level in performing ultrasound-guided vascular access. J Vasc Access. 2015;16(6):515-520. doi: 10.5301/jva.5000436
- Awad MS, Abdullah MK, Ibrahim RH, Abdulla RK. Nursing students’ attitudes toward simulation technology in nursing education. Int J Eng Technol. 2019;14(14):31–45. doi: 10.3991/ijet.v14i14.10571
- Fukuroku K, Narita Y, Taneda Y, Kobayashi S, Gayle AA. Does infrared visualization improve selection of venipuncture sites for indwelling needle at the forearm in second-year nursing students? Nurse Educ Pract. 2016;18:1-9. doi: 10.1016/j.nepr.2016.02.005
- Marchionni C, Connolly M, Gauthier M, Lavoie-Tremblay M. Innovative approaches to teaching vascular access to nursing students in the COVID-19 era. Br J Nurs. 2021;30(14):S34-S41. doi: 10.12968/bjon.2021.30.14.S34
- Mulyadi M, Tonapa SI, Rompas SSJ, Wang R-H, Lee B-O. Effects of simulation technology-based learning on nursing students’ learning outcomes: a systematic review and meta-analysis of experimental studies. Nurse Educ Today. 2021;107:105127. doi: 10.1016/j.nedt.2021.105127
- Demir D, Inal S. Does the use of a vein visualization device for peripheral venous catheter placement increase success rate in pediatric patients? Pediatr Emerg Care. 2019;35(7):474-479. doi: 10.1097/PEC.0000000000001007
- El –Aziz RAE-RA, Osman YM. Effectiveness of AccuVein AV400 device versus ultrasound-guided cannulation of the great saphenous vein at the ankle in infants: a randomized controlled trial. Int J Anesthesiol Res. 2020;594–599. doi: 10.19070/2332-2780-20000118
- Zhang Z, Wang X, Zhang L, et al. Infrared vein imaging for insertion of peripheral intravenous catheter for patients requiring isolation for Severe Acute Respiratory Syndrome Coronavirus 2 Infection: a nonrandomized clinical trial. J Emerg Nurs. 2022;48(2):159-166. doi: 10.1016/j.jen.2021.10.001
- Glover KR, Stahl BR, Murray C, et al. A simulation-based blended curriculum for short peripheral intravenous catheter insertion: an industry-practice collaboration. J Contin Educ Nurs. 2017;48(9):397-406. doi: 10.3928/00220124-20170816-05
- Goff DA, Larsen P, Brinkley J, et al. Resource utilization and cost of inserting peripheral intravenous catheters in hospitalized children. Hosp Pediatr. 2013;3(3):185-191. doi: 10.1542/hpeds.2012-0089
- Hallam C, Weston V, Denton A, et al. Development of the UK Vessel Health and Preservation (VHP) framework: a multi-organisational collaborative. J Infect Prev. 2016;17(2):65-72. doi: 10.1177/1757177415624752
- Pinelli F, Pittiruti M. The integrated short peripheral cannula: a new peripheral venous access device? J Vasc Access. 2023;24(3):353-357. doi: 10.1177/11297298211034023
- Reddy VK, Lavoie MC, Verbeek JH, Pahwa M. Devices for preventing percutaneous exposure injuries caused by needles in healthcare personnel. Cochrane Database Syst Rev. 2017;11(11):CD009740. doi: 10.1002/14651858.CD009740.pub3
- Zhang M, Lee M, Knott S. Is clinical performance adversely affected by wearing gloves during paediatric peripheral intravenous cannulation? Emerg Med Australas. 2014;26(5):455-460. doi: 10.1111/1742-6723.1227
Appendix 1
Demographic Questionnaire
Participants Demographic Data (Tick ( √ ) that apply to you)
- What age group are you in?
- ☐1≤ 19 years
- ☐2 20 – 29 years
- ☐3 30 – 39 years
- ☐4 40 – 49 years
- ☐5 50 – 59 years
- ☐6 ≥ 60 years
- What gender was assigned to you at birth?
- ☐1 Male
- ☐2 Female
- Other than the education today, have you had any previous peripheral intravenous catheter (PIVC) insertion or venipuncture training?
- ☐1 Yes
- ☐2 No
- If yes to question 3, where was the training conducted?
- ☐1 University
- ☐2 Hospital
- ☐3 Other, please specify: ___________
- Do you have previous PIVC insertion or venipuncture experience?
- ☐1 Yes
- ☐2 No
- If yes to question 5, please indicate duration of experience:
- ☐ Years
- ☐ Months
- If yes to question 5, please indicate where the experience was gained:
- ☐1 University
- ☐2 Hospital
- ☐3 Other, please specify: ___________
Appendix 2
Knowledge of PIVC Insertion Questionnaire
Please answer the question by choosing/ticking (√) the option available
- What factors would support placement of a PIVC? (Please select one)
- ☐ a. To deliver Mannitol 20%
- ☐ b. Anticipated duration of IV medication of 14 days
- ☐ c. To deliver 0.45% Sodium chloride + 5% Glucose
- ☐ d. To obtain blood sample*
- As a general guideline, what type of peripheral IV catheter should be selected when considering routine peripheral venous access?
- ☐ a. The smallest gauge catheter the vein will accommodate to deliver prescribed therapy
- ☐ b. The longest length catheter the vein will accommodate to deliver prescribed therapy
- ☐ c. The smallest gauge and longest length catheter the vein will accommodate to deliver prescribed therapy
- ☐ d. The smallest gauge and shortest length catheter the vein will accommodate to deliver prescribed therapy
- Please indicate which veins below are most appropriate for routine PIVC placement in adult patients: (Please select all that apply)
- ☐1 Veins of the wrist
- ☐2 Mid-forearm basilic vein
- ☐3 Vein of the ankle
- ☐4 Mid-forearm cephalic vein
- ☐5 Veins in areas of joint flexure
- ☐6 Antecubital fossa cephalic vein
- ☐7 Veins without bifurcations
- ☐8 Veins of the lower extremities
- ☐9 Vein section that does not have valves
- Place the following PIVC catheter insertion steps in correct order from start to finish by putting number (1-9) in the box.
- ☐ 1 Occlude blood vessel [8]
- ☐ 2 Wash hands [1]
- ☐ 3 Remove stylet [7]
- ☐ 4 Thread catheter [5]
- ☐5 Release tourniquet [6]
- ☐6 Stabilize vein [3]
- ☐7 Connect to an IV administration set or saline lock [9]
- ☐8 Insert needle and catheter [4]
- ☐10 Don gloves [2]
- Nurse A will insert a PIVC to adult patient who was admitted to the hospital one hour ago. Prior to the PIVC insertion, nurse A gives health education to the adult patient. What educational topics should be included in the health education? (please select one)
- ☐ a. Purpose, expected outcomes potential & complications/risks and benefits
- ☐ b. Type of the infusion therapy & the insertion procedure
- ☐ c. Infusion-device related care to prevent complications *
- ☐ d. All of the above
- From the following examples, select the most appropriate documentation for a PIVC insertion procedure?
- ☐ a. Date, time, & name of the inserter
- ☐ b IV catheter & infusion characteristics
- ☐ c. Site insertion characteristics & patient responses
- ☐ d. All of the above
- The greatest risk for contamination of the vascular access device after catheter placement is associated with failure to (Please select one)
- ☐ a. Perform routine site care
- ☐ b. Rotate the PIVC
- ☐ c. Disinfect the needleless connector
- ☐ d. Stabilize the catheter
Appendix 3
Confidence with PIVC Insertion Questionnaire
Please choose a response that best represents your confidence in PIVC insertion
- 1=strongly disagree
- 2=disagree
- 3=neither disagree nor agree
- 4=agree
- 5=strongly agree
- No Statement Response
- 1 2 3 4 5
- I am confident I can…
- 1 Perform a pre-insertion PIVC site assessment
- 2 Insert a PIVC within 1 or 2 attempts
- 3 Select the most appropriate PIVC device for the prescribed treatment plan
- 4 Assist my peers with difficult PIVC insertion
- 5 Select an ideal vein for PIVC insertion
- 6 Prepare the insertion site according to hospital protocol
- 7 Insert the PIVC correctly
- 8 Advance the PIVC correctly
- 9 Remove the needle/stylet with minimal blood exposure
- 10 Dress and secure the PIVC and tubing according to hospital protocol
- 11 Document PIVC insertion according to hospital protocol
- 12 Give patient education related to PIVC insertion and care
- 13 Document the results of site assessment according to the hospital protocol
- 14 Recognise signs and symptoms of PIVC complications
Appendix 4
- Please indicate your level of agreement with the following statements:
- Strongly agree
- Agree
- Neither agree nor disagree
- Disagree
- Strongly disagree
- I found the near infrared education session helpful
- I received useful information today on how to use near infrared technology
- I would recommend the near infrared education session to my colleagues/peers
- I found the near infrared device easy to use
- I would feel more confident placing a PIVC using the near infrared device
- I would like to use the near infrared device on all my patients
- I think the near infrared device would enhance my ability to select an optimal site for PIVC insertion
- I think the near infrared device would enhance my ability to insert a PIVC
- Have you used an AccuVein near infrared device before?
- ☐1 Yes
- ☐2 No
- If yes to question 2, how long have you been using the device?
- ☐1 0-3 months
- ☐2 4-6 months
- ☐3 7-12 months
- ☐4 Over 12 months
- If yes to question 2, please indicate whether you gained additional insights from the education session today about using the AccuVein near infrared device efficiently:
- ☐1 Strongly agree
- ☐2 Somewhat agree
- ☐3 Neither agree nor disagree
- ☐4 Somewhat disagree
- ☐5 Strongly disagree
- Please share any other comments about your experience of the education session today and using the near infrared device: