

Improving ADHD Assessment: Quebec’s Clinical Insights
Improving the Psychosocial Assessment of Young People with ADHD: Clinical and Ethical Issues from the Quebec Experience (I)
Joël Monzée, Ph.D 1*; Anne-Isabelle Dionne, M.D., IFMCP 1
- Joël Monzée, PhD Institut du développement de l’enfant et de la famille, Quebec, Canada
- Anne-Isabelle Dionne, M.D., IFMCP Institut du développement de l’enfant et de la famille, Quebec, Canada
OPEN ACCESS
PUBLISHED: 30 June 2025
CITATION:Monzee, J., and Dionne, A., 2025. Improving the Psychosocial Assessment of Young People with ADHD: Clinical and Ethical Issues from the Quebec Experience (I). Medical Research Archives, [online] 13(6).
https://doi.org/10.18103/mra.v13i6.6536
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i6.6536
ISSN 2375-1924
ABSTRACT
Attention Deficit Hyperactivity Disorder is a neurodevelopmental disorder that is often diagnosed in childhood and can persist into adulthood. This disorder is characterized by inattention, hyperactivity, and impulsivity that significantly interfere with daily functioning. In Quebec, there is a problem of overdiagnosis and overprescription of psychostimulants compared to the usual global statistics. In fact, the diagnosis of attention deficit hyperactivity disorder is normally based on a detailed clinical assessment, including analysis of medical, family, and environmental history, as well as the use of validated rating scales and structured clinical interviews that understand their limitations. However, the differential diagnosis is challenging due to the presence of various comorbidities, such as mood disorders, anxiety disorders, sleep disorders, and learning disabilities. In addition, some modern environmental factors, such as excessive screen exposure, have been associated with symptoms of inattention, agitation, and impulsivity in children. Since secure attachment relationships play a crucial role in a child’s development, things like family instability, high parental stress, lack of emotional availability, or inconsistent parenting practices can weaken attachment and lead to “Attention-Deficit-Hyperactivity-Disorder-Like” behaviors. Beyond the clinical issues, it is also an ethical concern to ensure that the therapeutic direction is optimized for the benefit of the patient. This article examines the issues related to the diagnostic process by emphasizing the importance of a comprehensive and integrative assessment that considers environmental and relational factors. Such an approach makes it possible to better distinguish attention deficit hyperactivity disorder from other pathologies and to develop appropriate therapeutic strategies, ranging from conventional pharmacological treatments to interventions focused on managing exposure to screens and strengthening secure attachment bonds. This comprehensive diagnostic framework offers large potential to improve patient care and optimize long-term clinical outcomes.
Keywords: children, adolescents, ADHD, psychostimulants, psychosocial assessment, clinical ethics
Introduction
Ethics and clinical judgment are at the heart of mental health practice, while the definition of psychiatric conditions is based on clinical consensus and not biological markers. Each physician or health care professional must make the best use of their clinical expertise, but an ongoing reflective process, to adequately guide the treatment plan of a person in distress. This is even more important for a young patient, when his parents must make sometimes difficult decisions. Medication may be a preferred option based on the information available to the physician. He listens to the parents or the young adult and may use the results of a standardized test, a psychometric assessment or a history. However, it is questionable whether this diagnostic process is still in line with good medical practice.
According to the psychiatric consensus, ADHD is a neurodevelopmental disorder of genetic origin that produces alterations in personal, social, school or occupational functioning. While there are certainly ADHD patients, there are also other individuals affected by various psychosocial or medical problems that manifest themselves with symptoms resembling ADHD without it being a neurodevelopmental disorder of genetic origin. In such a case, these would be ADHD-like patients who require therapeutic interventions that are different from treatments for ADHD patients. This is the principle of differential diagnosis that carefully explores the origin of symptoms, to ensure the right direction of clinical intervention. This first article questions the traditional model of psychiatric intervention around ADHD, as well as the different psychosocial avenues that must be considered to better differentiate and better treat ADHD-like patients. Similarly, the second article explores how metabolic problems affect the regulation of behaviors associated with ADHD.
Basically, it is a question of exploring the different clinical indicators to optimize patient management to better distinguish and better treat ADHD patients or ADHD-like patients. In addition, psychostimulants can improve cognitive performance, which leads to an ethical issue in terms of equity between students in a context of academic performance. As was the case to counter doping in sport, it is necessary to ensure that the prescription of a psychostimulant responds to a possible neurological disorder, to avoid tipping over into a form of undue optimization of academic performance or to overlook other psychosocial problems, while parents and students are sometimes under great pressure to have a medication prescribed.
Of course, it is possible that, individually, the pharmacological treatment plan is the only option to help the young patient meet school and social standards. The problem, both clinical and ethical, stems from the increasing number of young patients diagnosed and treated with psychotropic drugs. This phenomenon has been exposed for more than twenty years in Quebec, but there has never been a real questioning of the model for evaluating symptoms associated with ADHD by health authorities or institutions regulating the work of health professionals. While good practice guidelines require that health professionals use a differential diagnostic process, assessment process is rarely performed often because of the conceptualization of ADHD described as a genetic neurodevelopmental disorder.
Finally, the only longitudinal study comparing two groups of ADHD students to determine whether it was preferable to prescribe psychostimulants or to offer psychosocial therapy concluded that, if medication is faster than a psychosocial intervention, but that in the medium and long term educational and psychotherapeutic strategies are more effective. However, it is not clear to many health professionals that they can intervene psychosocially. By considering the avenues of intervention based on a differential diagnosis, this offers levers for therapists to intervene with young patients-ADHD, as well as patients-ADHD-like. Thus, this first article and a second companion article draw up a broad portrait of the different clinical hypotheses which should be evaluated in the diagnostic process to guide the therapeutic process.
Methods
In the complete study, we analyze the number of prescriptions of psychotropic molecules for young people aged 0 to 26 years grouped by age groups (0-5, 6-10, 11-15, 16-20, 21-26 years) from 2003 to 2022. However, Intuniv® is segregated because guanfacine was only marketed in 2013, and normally prescribed in exceptional situation. Data has been provided by the Régie de l’Assurance médicament publique du Québec (RAMQ) which covers 29.5% of citizens. Health authorities don’t have data for the entire population, even if the people are compulsorily covered by a private program or RAMQ. While the Access to Information Act requires public institutions to provide statistical data, they are presented in a way that makes it difficult to accurately count the number of patients. Indeed, they concern the ‘number of pharmacy services’ (PS). According to clinical experience, one PS is generally equivalent to the monthly consumption of one drug, or 12 PS/person/year. However, it is possible for an individual to receive two psychotropic drugs concomitantly, as a long-term (before school) and a short-term (return home) psychostimulant pills every day. Similarly, it is possible that – over the course of the year – some people start taking psychotropic drugs, while others start withdrawal and stop them. Thus, we can estimate, but not determine with certainty the number of patients from the number of PS. In this article, we focus only on data of psychostimulant, and non-stimulant drugs used as a therapeutic treatment for ADHD with the aim of reflecting on ways of clinically intervening with young people who have received a diagnosis.
Prevalence of TDAH
According to the DSM, the diagnosis must be made before the age of seven. However, non-specific-ADHD may be suspected in people over the age of seven. Yet, it is very common for the diagnosis to be made when entering school or in very demanding university programs. While the prevalence of ADHD was 3.5% in 1996 and 5-7% in 2000, it is now estimated at 10%. Curiously, Quebec health authorities still report that ADHD is present in 3-5% of students, while French authorities speak of a maximum of 6% in minors and 3% in adults based on a consensus emerging from a collaboration between 400 European university laboratories.
Parents, teachers, and health care professionals are commonly concerned that ADHD can occur when students have difficulty paying attention or finishing what they start, are easily distracted or procrastinate, and when they are unruly or impulsively moving. This suggests that this psychopathology is located on a continuum of psychosocial dysfunctions. While the intensity of symptoms differs from person to person, ADHD can lead to academic problems, relationship problems, and self-esteem problems. However, there are no biological markers. Certainly, psychometric tests can be used, but clinical judgment is essential to guide the treatment plan, as these tests do not distinguish ADHD from ADHD-like.
The Quebec experience
To facilitate the reflective process required in mental health, we will discuss the process of evaluating and prescribing psychostimulants when a young patient is suspected of having ADHD in Quebec.
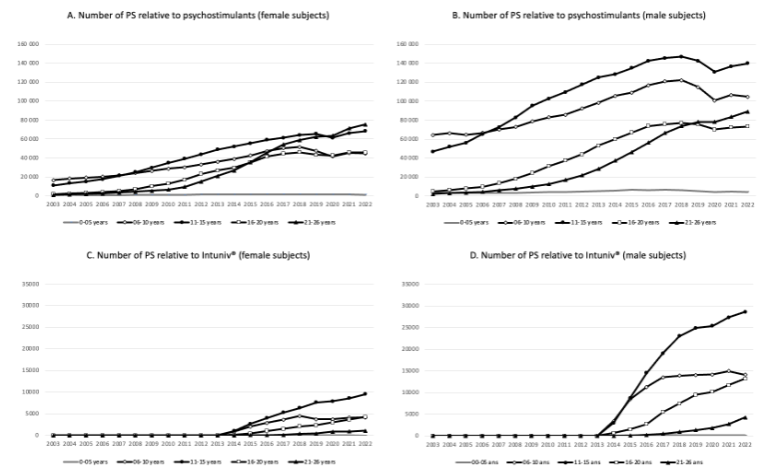
The prescription of psychotropic drugs has been steadily increasing for 20 years. Regarding ADHD, the estimate of the number of young patients receiving psychostimulants increased from 8.27 to 12.18% between 2005 and 2022 among boys (6-10 years), while the proportion of young adolescents (11-15 years) increased from 6.15 to 16.27%. During the same period, adolescent girls (16-20 years) saw their proportion increase from 0.37 to 5.88 and young women (21-26 years) from 0.17 to 7.17%. Previously, it was revealed that there were two to four times more students on psychostimulants in Quebec as in other provinces in Canada.
The Institut national de la santé publique du Québec (INSPQ) explains that psychotropic drugs that relieve ADHD symptoms are prescribed by family physicians (53.2%), pediatricians (30.5%) and psychiatrists (10.3%), as well as other specialists (6%). The Quebec guidelines result from a collaboration between the Collège des médecins and the Ordre des psychologues, but they have not been adjusted since 2000. However, the Institut national de l’excellence en santé et en services sociaux (INESSS) recommends making a differential diagnosis, but this is rarely considered, because the symptoms are sometimes very pervasive and jeopardize academic success. Finally, INSPQ and INESSS have drawn up a portrait of the situation. They acknowledge the continued increase in the prescription of psychostimulants, but they do not question the diagnostic criteria or guidelines used by clinicians.
In 2019, the Association des pédiatres du Québec adopted the recommendations proposed by Labbé and collaborators. At the same time, the Ministry of Health and Social Services and the Ministry of Education and Higher Studies published a clinical pathway protocol for interdisciplinary and intersectoral assessment and intervention with students. They mention the need to make a differential diagnosis, without this applying in the field. As a result, the Parliamentary Committee on Health and Social Services investigated the phenomenon of overconsumption of psychostimulants in Quebec. To reverse the trend, their report recommended (1) documenting the situation of overdiagnosis and overuse of psychostimulants, (2) evaluating the side effects of psychostimulants, (3) improving practice guidelines to increase rigour during evaluations, (4) promoting psychosocial interventions, (5) adapting questionnaires to the Francophone culture, and (6) ensuring the clinical validity of psychometric tests. Six years later, none of these mandates have been carried out. However, these various documents have raised awareness among doctors, leading to a decrease in the rate of prescriptions in 2019 and 2020, which seems to support the hypothesis of a lack of rigor and confusion between ADHD and ADHD-like. Moreover, the increase resumed in 2021, while the health crisis due to SARS-CoV-2 disrupted the schooling of students. Thus, there is concern that many cases of ADHD-like are not adequately treated in Quebec, but this has already been reported in other countries, while researchers fear a lack of objectivity and rigor in the diagnostic process.
Are the criteria for identifying symptoms too inclusive?
The estimated prevalence are similar across countries, notwithstanding Quebec. However, the increase in the prescription of psychotropic drugs is observed in Europe and USA. The question is whether ADHD is being diagnosed better than before. However, there is concern that the criteria for ADHD are too inclusive, which would increase the number of ADHD-like patients. It should be noted that, as early as 1998, Swanson and his collaborators had already demonstrated that by increasing the rigor during the diagnostic process, the frequency fell to 1%. As a result, it is likely that many ADHD-like patients do not receive the appropriate treatment plan, as the ease with which a patient meets the criteria for ADHD and receives medication tends to short-circuit the necessary differential diagnosis. On the one hand, the family and the patient are convinced, thanks to popular literature, that he or she has ADHD, and the origin of the symptoms is not questioned, while, on the other hand, the doctor has a few minutes to diagnose.
To reduce the number of ADHD-like patients, clinicians should assess the impact of lifestyle habits, psychosocial vulnerability factors and the quality of the determinants of health. First, our way of life has become sedentary over the centuries, while access to digital life has increased the number of hours spent sitting in front of screens. Therefore, is it possible that children need to move more intensely when they are in a stimulating environment and without screens to slow them down? Could a lack of interest in school or any subject lead to a lack of concentration, without it being an ADHD? What links can be made between unhealthy lifestyle habits and symptoms of ADHD?
The criteria for ADHD are becoming more and more broad, without determining the degree of adaptive stress of the students, or their environment. Yet, clinical experience shows that the number of authority figures at home and at school can disrupt the attachment bond, which can complicate the brain’s normal developmental process. Similarly, the structure of families sometimes creates a context that increases vulnerability factors: separation conflicts, single parenthood, blended families, dysfunctional families, etc. According to Shore and Porges, these common situations can induce normal and invasive adaptive behaviors. Thus, it’s not due to a disorder of genetic origin (ADHD), but rather to living conditions (ADHD-Like).
Finally, some criteria are highly dependent on the perceptions and expectations of the adults who assess the young person, such as “has difficulty complying with instructions from others”, “has difficulty remaining seated when asked” or “often interrupts others or imposes their presence”. What is the difference between the relevant judgment of an adult and that of another who is physically or mentally tired? Couldn’t an adult with adjustment difficulties in his or her own life be less tolerant if he or she must continually repeat disciplinary instructions? And what about the feeling overwhelm?
Inclusive criteria encourage confusion between ADHD and ADHD-like. E.g., the normal immaturity of young students in a class may be confused with the symptoms of ADHD. Indeed, ADHD is a neurodevelopmental disorder of genetic origin, so there should be a homogeneous distribution of rate throughout the year. However, it has been shown in Quebec that the rate of ADHD diagnosis was 25% more frequent in students born during the summer (22%) than those born during the fall. The distribution is not homogeneous according to the months of the year: the youngest are more likely to have an ADHD diagnosis. Similar results are reported in France where, again, the youngest students in a class are more likely to get an ADHD diagnosis and psychostimulants to regulate symptoms.
Thus, the ethical question would be to ask whether the prescription of psychostimulants would not compensate for a less great, but natural, maturity in the young students of a class to reduce the workload of adults? Wouldn’t such a use of medication obscure the need to reorganize the school curriculum? Why has no study ever really looked at the neurological impacts of psychostimulants on the natural development of the attentional system? If the nature of the personal perception of the assessor and the prescriber is influenced to this extent, shouldn’t we question the international consensus?
In addition, the rate of prescriptions for psychostimulants in Quebec is systematically higher than in the “rest of Canada”. However, these are the same psychometric tests that are used across Canada. While there are cultural differences between Quebec and the ROC, there are few genetic differences. Could it be that lifestyle habits and disciplinary strategies differ between Quebec and the ROC and that, as a result, there are more young people who meet ADHD indices in Quebec than elsewhere? Could the translation of psychometric tests initially written in English induce errors in understanding the words translated?
A great heterogeneity of the ADHD-population
Currently, the definition of ADHD is based on a circular logic: “if an individual suffers from ADHD, it is because he or she is inattentive, disorganized and hyperactive-impulsive; if an individual is inattentive, disorganized and hyperactive-impulsive, it is because he or she suffers from ADHD”. On the other hand, ADHD is suspected if, according to the DSM-5-TR, the symptoms “cause clinically significant distress or impairment in social, occupational, or other important areas of functioning predominate but do not meet all the criteria for ADHD or any of the disorders in the diagnostic class of neurodevelopmental disorders.” In other words, a person can be diagnosed even if they do not meet the diagnostic criteria for ADHD if their suffering requires prompt medical intervention.
Factually, does this distress reflect a neurological disorder, opposition or the impact of a lack of discernment on the part of the young patient’s entourage? To avoid this confusion, the clinician must assess the student in two different locations. For example, the patient may act differently if they are at school or at home, but if the issues are the same, is this clinically valid? Activities or times of day should also be varied, as stress and fatigue can interfere with the efficiency of the assessment. E.g., a child concentrates easily during creative activities, but is easily distracted during homework. A teenager procrastinates to study, but is cautiously involved in his paid work on weekends or when he tinkers with his grandfather. A student gets involved in mathematics, but encounters difficulties during his French lessons. However, a neurological disorder works continuously, and not in an alternative way depending on external expectations or the affordance of activities.
In addition, psychometric tests do not evaluate the quality of the attachment bonds between young patients and adults, even though this can weaken the availability for social and academic learning. The intensity of the mental load during certain academic tasks or certain times of the day is not evaluated. We don’t look at the affordance of educational activities or the subject taught. We don’t question the ability of teachers to interest, mobilise and regulate a group. In addition, statistical averages erase the dynamic issues of child or adolescent development. The levels of certain hormones, vitamins and other trace elements are not considered. These tests do not look at lifestyle habits and do not measure the number of hours spent in front of screens or those spent on restful sleep. Who addresses relational challenges in the family or in the classroom? Why not take into account socio-economic protective factors or vulnerability? Can we really ensure that psychometric tests target the real difficulties encountered by the student before assuming that he or she needs a psychotropic drug to regulate his or her behaviours?
Despite appearances, the claim that ADHD is a neurodevelopmental disorder is not really supported by the DSM. Although it is classified as such, the authors of the DSM-5-TR explicitly admit that research confirming the definition of ADHD as a neurodevelopmental disorder is not yet conclusive. In addition, the theory associating ADHD with a genetic problem has long been criticized. As discussed in the second article, it is still difficult to identify which genes are specific, while metabolic problems, as well as psychosocial difficulties, could also explain the symptoms observed.
The conclusions of a meta-analysis of the brain organization of ADHD patients recall that, in most cases, symptoms result from several genetic and environmental risk factors. Each factor may have a small individual effect, but these factors interact in such a way that they increase the body’s susceptibility and manifest themselves in symptoms associated with ADHD. The ADHD-like concept therefore takes on its full importance, because it allows us to accept the consensus theory (ADHD), while ensuring that the symptoms are not confused with other health problems (ADHD-like).
The first challenge for clinicians is to avoid confusion to properly orient the therapeutic direction. The second challenge is to avoid standardized educational or therapeutic intervention protocols aimed at erasing symptoms without acting on the environment (house, school, or neighborhood) or the environment (family, friends, teachers, coaches, and community). Finally, it must be remembered that research methods are based on very rigorous criteria for selecting subjects in the hope of obtaining evidence that eventually validates a psychometric test or a therapeutic protocol. The third challenge for clinicians is to generalize these findings to guide intervention with a much more heterogeneous population.
Could these three challenges explain why parents and caregivers face so much difficulty in helping children and adolescents who are too often distracted, hyperactive or impulsive? Is it still ADHD? Can we examine the presence of ADHD-like associated with other psychological conditions, including the manifestation of stress, anxiety, lack of motivation, lack of reassuring relationships, unstimulating classes, low self-esteem, lack of confidence, inappropriate organization of school days, poor screen management, etc.? In the case of ADHD-like, most of the reactivities would be normal, but disturbing for those around them or disruptive for school perseverance. However, the treatment plan will be different for each of these conditions.
Finally, many health problems affect attentional skills, emotion regulation, and motor drive inhibition. However, they are rarely regarded in the evaluation of mental disorders, because most theoretical models offer a reductionist view of psychiatric disorders. These theories appear worrying and inconsistent about the systemic definition of health proposed by the WHO, but even more so regarding the real needs, deemed in terms of global development, of children and adolescents, and even young adults, to promote educational success and their integration into family, school or social life, and, sooner or later, professional. It is a clinical problem, but also an ethical one.
Improving the rigour of the evaluation
The current consensus defining ADHD hypothesizes a genetic condition that induces slower maturation in the prefrontal cortex or a dysfunction affecting the dopaminergic pathway that allows the striatum to modulate the areas of the prefrontal cortex involved in the regulation of attention, inhibitory control, and social behaviors. E.g., a study using fMRI showed that the prefrontal cortex was significantly less active in the group of ADHD subjects than those in the comparison group. However, the maturation process of the prefrontal cortex depends, of course, on biochemical efficiency, but also on the conditions in which the child evolves in the family, social and school factors. To avoid clinical errors and ethical misguidance, it is therefore necessary to explore the living conditions of young patients.
Various elements related to health and lifestyle must be better considered to ensure a fair and equitable diagnosis for the young patient, to prevent the treatment plan from obscuring the real problem or inducing cognitive doping. This is the founding principle of the differential diagnostic process. In other words, what could explain the symptoms without it necessarily being a genetic neurodevelopmental disorder?
First, it is important to know that the emotions experienced by the mother during pregnancy can influence the quality of mental health. It is known, e.g., that maternal stress during pregnancy can disrupt neuropsychological development, as has been shown for certain forms of schizophrenia and language problems, as well as academic learning difficulties. In addition, a complicated birth could have behavioral repercussions that are unfortunately rarely assessed when a student is evaluated for possible ADHD. In fact, three studies have shown that birth by caesarean section may increase the risk of an ADHD diagnosis.
Second, the first few months of life can also have some influence, such as the consequences of postpartum depression or when parents have difficulty adjusting to the new family reality. However, it is often difficult to talk about the issues of attachment to parents, because certain psychoanalytic theories have sometimes hurt mothers. Today, we are witnessing the opposite dynamic, we avoid making parents feel guilty. This poses a problem both clinically and ethically, since attachment issues or the low quality of parental presence have a dynamic influence on the brain maturation process of children and teenagers. In addition, research on the consequences of adverse childhood experiences (ACEs) – e.g. violence, neglect, parental abandonment, adaptation to a parent’s psychiatric conditions, etc. – has attracted attention, as they can induce health problems at both the metabolic and psychiatric levels.
A study to measure the effect of ACEs on brain maturation was done in England. Brain volume was measured in young adults, even though they had all been adopted after a stint in an orphanage. In one group, these were English children abandoned shortly after birth. In the second group, they were Romanian children who had been housed in orphanages from a few weeks to four years of age during Ceauşescu’s dictatorship. Children lived large ACEs before being adopted by English parents. Twenty years later, the brain volume of Romanian youth was significantly lower than that of English youth. In addition, the longer they had been placed in an orphanage, the smaller the brain volume. Since subcortical structures are relatively mature from the first months of life, the reduction in brain volume is mainly associated with the prefrontal areas of the brain essential for attentional skills, inhibitory control and executive functions.
All in all, adversity disrupts the maturation process of the prefrontal cortex. Clinicians should therefore take the ACE-Score into account. To access relevant information, a strong bond of trust must be created with the patient and his or her parents. Secondly, it is a question of supporting them to ensure a reassuring quality of presence with children and to reduce the frequency of ACEs as much as possible. The same is true in schools where there are sometimes people who act abusively to ensure discipline. There are also teachers who encounter personal difficulties and unintentionally create a negative school climate. And there is bullying between students. Consequently, the clinical evaluation must consider the vulnerability factors in the students’ family and school life before concluding that ADHD is present.
Third, clinical experience shows that the reactive behaviours of children and adolescents when they must adapt to too many expectations are like several symptoms of ADHD. Rather, these behaviours are associated with the various manifestations of adjustment disorder. Indeed, stress hormones accumulate during the school day to meet academic and social expectations, which can induce different impulsive reactions or distraction. The same is true for children whose parents are separated and travel from one house to another or who no longer have contact with one of the parents, which is one of the ten conditions deemed to be ACE. Consequently, we can imagine that students experiencing family or social difficulties, without there even being an ACE, can behave in a way that is like ADHD, and therefore develop an ADHD-Like.
These different phenomena must therefore be regarded by the medical doctor before establishing with certainty that it is an ADHD. The DSM-5-TR and PDM-2 recognize the importance of social context. In the DSM-5-TR, the authors mention that “signs of the disorder may be minimal or absent when the individual receives frequent rewards for appropriate behavior, is under close supervision, is in a novel environment, is engaged in particularly interesting activities, is receiving constant external stimulation [e.g., via electronic screens], or interacts in individual situations [singular as in the office of the clinician who evaluates it].” Thus, the behavioural indices of ADHD should be assessed in two different places, but these two places must be different not in terms of space (home and school), but in terms of different emotional load and socio-emotional context (different activities, affordante tasks, bond of trust, safe place, etc.) to avoid misunderstanding the behavioural reactions of young people. Yet, the time of day must also be considered, since a student may meet the expectations of adults at certain times of the day or for certain specific activities, while he or she could become disorganized at other times, especially in the afternoon, especially if he or she has made extensive efforts previously.
Thus, it must be remembered that there is not necessarily a correspondence between the result of a psychometric test and what is happening in the individual’s brain. The test measures the frequency of a behavior, but cannot accurately determine what is happening in the person’s brain given the multifactorial aspects of ADHD and ADHD-like. In addition, psychometric assessments offer a succession of individual tests. We cannot ignore the fact that each of which could influence the taking of subsequent tests. The patient, especially youngers, will be less cognitively available if he accumulates physical fatigue, resists to the lack of affordance of diagnostic tools, and misregulates the increasing mental load or performance anxiety. Finally, PDM-2 adds that indices of normality of behaviours must be pondered in relation to their mentalization skills and abilities in relation to their affective maturity.
Fourth, various social factors seem to be correlated with the manifestation of inattentive, compulsive and/or hyperkinetic behaviors and are not addressed, such as poverty and socio-economic difficulties, childhood trauma, child abuse, death in the family, poor family cohesion, parental psychiatric disorders, separation from parents (or blended family), parental criminality, household dysfunction, family incarceration, and long-term parental unemployment. However, all risk factors are part of the different forms of ACE, because they are potentially the cause of complex trauma. Shouldn’t we make sure that the child’s or adolescent’s living environment meets his or her needs clearly, even if it does not have to be perfect, before concluding that he or she has ADHD?
Fifth, it is necessary to assess visual abilities. Indeed, vision problems are increasing in children, adolescents and young adults. Optometrists often cite that screens have a deleterious effect on visual acuity. While three-dimensional vision and increasingly dry eyes are frequently cited, other problems emerge because of the short distance between the eye and the screen, especially in very young children whose visual system is immature. A meta-analysis of 77 studies found links between emerging vision problems and symptoms associated with ADHD. There appear to be increased risks of astigmatism, farsightedness, and strabismus, which are much higher in young people suspected of having ADHD than in other children, teens, or young adults. In addition, it appears that patients in the ADHD group had more vision problems at the near point of convergence, as well as the shift and variability of the accommodative response. Still, there does not seem to be any evidence of an anatomical malformation of the retinal nerve fiber layer. In addition, dry eyes are sometimes the result of a lack of vitamin-A. If not treated properly, sensory deficits contribute to functional impairment. In addition, impaired vision can lead to problems recognizing other people’s emotions, which impairs social functioning. Finally, visual acuity problems can also disrupt concentration, as the efforts to compensate for the deficit are imposing for some students.
Sixth, lifestyle habits impact the nature and intensity of certain behaviors associated with ADHD symptoms. We should therefore better measure the manifestations of mental fatigue, but also physical fatigue, as well as the duration and quality of sleep. This is even more important in teens and college students, as the circadian rhythm differs from that of their childhood or adult world. In addition, many teens and young adults may work 20 hours a week, while maintaining a social life.
Seventh, virtual leisure activities modulate attentional capacities, triggering frequent distractions or motor activities. However, students spend nearly 4 hours a day in front of screens at home. Researchers have shown that high levels of screen time of more than 2 hours are correlated with increased symptoms of inattention and hyperactivity in children and adolescents. Social media and video games is now well known that fast-paced, interactive digital content stimulates the brain in an intense and repetitive way, leading to a constant search for instant gratification. This can reduce boredom tolerance and the ability to concentrate on less challenging school tasks. Prolonged exposure to screens activates the brain’s reward circuitry, artificially increasing dopamine levels. In the long run, this can make it more difficult to regulate attention and control motor drives, especially in the classroom. Finally, prolonged periods of screen exposure can interfere with the development of brain regions responsible for attention, planning, and emotional control, resulting in symptoms that fit well with ADHD.
In addition, students using electronic devices have disordered eating behaviours. These behaviors contribute to poor nutritional quality and increased calorie intake, exacerbating ADHD-like symptoms through metabolic dysfunction. In addition, exposure to screens, especially in the evening, disrupts melatonin production resulting in poor quality sleep while disruption of the circadian rhythm and lack of sleep affect the regulation of attention, emotion, and the inhibition conducting inappropriate behaviours at certain times of the day.
Finally, there is the entire nutritional and digestive sphere. The clinician should therefore look at the extent to which the microbiota may influence the patient’s academic or social skills before concluding neurological disorders.
Optimize therapeutic treatment
As mentioned at the beginning of the article, it is possible that the pharmacological treatment plan is the only option to help the child, adolescent or young adult succeed in his or her school year. This treatment option will be more necessary if the family or the school institution resists transforming certain educational practices and lifestyle habits or if the ACE-score is high. However, the prescription of a psychostimulant or Intuniv® should not hide the family and school problems for which it is adults who need help. Thus, will they be humble enough to recognize this, or will the psychiatrization of the young patient not allow them to dodge a questioning by parents or school workers? Moreover, economic restructuring in the health and social services sector, as well as in the school environment, does not necessarily allow workers to act as effectively as they could, the use of medication will compensate for the lack of social support, whether family, school or medical, but also leads to a misorientation of treatment to meet the needs of the young patient.
Even if medication is preferred, the health professional must ensure that the young patient is psychosocially equipped to support the development of his or her emotional, cognitive and social resources. This is more important if the student is not yet biologically ready to meet academic expectations or is not mentally available to meet pedagogical and disciplinary standards. ADHD-like behaviors are therefore not a psychiatric disorder at all. In addition, psychometric tests are standardized, while behaviors can reflect the heterogeneity of the normal and natural process of brain maturation within the population without, again, there being a child psychiatric disorder. Finally, it is also necessary to consider an intervention targeting healthy lifestyle habits, or even the learning of concentration or emotion regulation techniques. Sometimes, pupils and students are constantly in action or change their living spaces too often, which increases the mental load and reduces their attention span in class or during study time. In other words, it requires good conditions to support the overall development of the pupil or student and reduce the risk of ADHD-like symptom manifestation. These are educational, not psychiatric issues.
Of course, the distress of the child or adolescent can be tempered momentarily by taking a psychotropic drug, but this often leads adults to hide his or her real psychological suffering. However, clinical experience makes us aware of the fact that the distress of the population has greatly increased since 2020, which disrupts the determinants of health and increases the vulnerability factors for educating children and adolescents. As a result, it is likely that the number of ADHD-like patients will increase further in the coming years. However, the various avenues of evaluation can also become proposals for preventive intervention to avoid the deterioration of the clinical situation.
Finally, most interventions, both psychosocial and pharmacological, tend to be strictly oriented towards the symptoms and not the causes of the difficulties. The risk is that, over time, real mental health problems will crystallize, when we could have intervened from a developmental perspective and promoted the development of the young person, despite temporary or chronic adversity. From an intervention perspective that promotes the overall development of the student, it is important to consider the development of mentalization skills, strategies to improve lifestyle habits and explore resources to optimize the determinants of health.
Conclusion
Professionals, both in the medical and school sectors, are trying to screen those who have a neurological condition to reduce the risk of dropping out of school. However, scientific knowledge is sometimes overly popularized and there is a lack of psychosocial resources. In this context, it is therefore easy to shorten the diagnostic process and minimize the real needs of children and adolescents, whereas a process of differential diagnostic evaluation is necessary to reduce the chances of confusion between child psychiatric disorders. The problem is similar in adults, where the speed of the assessment process is seen to ignore real health difficulties in adults. Of course, health authorities, but also pharmaceutical companies, inform professionals of certain risks of misuse of psychostimulants, but it appears that many adults minimize the effects of chronic drug use and hide family, school and social issues. In such a context, the medicalization of the behavioural difficulties of children and adolescents simplifies the intervention by offering rapid results, without calling into question the environment in which young patients are welcomed, whereas other medical problems could explain these same behaviours. However, is it ethical? In fact, we invite clinicians to refer to a fundamental clinical principle: when a patient questions a theory, let us humbly put the theory aside and deal with the patient. It is the one that counts, not the theory. To improve clinicians’ reflective approach, we explored the current consensus on ADHD, but also its multifactorial aspects, both biochemically and psychosocially, to propose more rigorous assessment strategies to differentiate ADHD from ADHD-like. In the second article, we will discuss metabolic factors that can also induce ADHD-like clinical profiles.
Disclosure Statement
The authors or immediate family members have no potential conflicts of interest for the findings presented, nor has any funding source influenced the content of this article.
References
- Swanson JM, Sergeant J, Taylor E, et al. Attention-deficit hyperactivity disorder and hyperkinetic disorder. Lancet. 1998;351:429–433.
- Sergeant J. The cognitive-energetic model: an empirical approach to ADHD. Neurosci Biobehav Rev. 2000;24(1):7–12.
- Monzée J. La médicalisation des humeurs des enfants. Revue internationale d’éthique sociétale et gouvernementale. 2006;8(2):76–88.
- Maumaha Noune R, Monzée J. Problématiques éthiques quant au bris de la confidentialité du dossier médical des enfants. Revue internationale d’éthique sociétale et gouvernementale. 2011;12(2):261–295.
- Monzée J. Évolution des connaissances biotechnologiques et pratiques psychothérapeutiques. Revue québécoise de psychologie. 2012;33(2):97–122.
- Vaillancourt JP. L’origine neurologique du trouble déficitaire de l’attention avec ou sans hyperactivité: fait ou hypothèse? Revue québécoise de psychologie. 2012;33(1):253–270.
- Monzée J. L’usage immodéré des psychotropes chez les jeunes de 0 à 26 ans au Québec: quel avenir pour les jeunes générations? IDEF; 2024.
- Monzée J. Evolution of psychotropic medication prescription in young people: reflection from the Quebec experience. Psychotherapy and Psychosomatics. 2025;94(1):8–14.
- Barkley RA, Behavioral inhibition, sustained attention, and executive functions: constructing a unifying theory of ADHD. Psychol Bul. 1997;121:65–94.
- Charney DS, Nestler EJ. Neurobiology of mental illness, Oxford PU; 2004.
- Diagnostic and Statistical Manual of Mental Disorders-DSM-5, American Psychiatric Publishing; 2013.
- Diagnostic and Statistical Manual of Mental Disorders-DSM-5-TR, American Psychiatric Publishing; 2022.
- AI Dionne, J. Monzée. Improving the medical assessment of young people with ADHD: II. Genetic, psychosocial or metabolic issues? ESMED (Submitted).
- Monzée J. Dopage sportif: de la responsabilité des chercheurs et des entreprises pharmaceutiques. Revue internationale d’éthique sociétale et gouvernementale, 2005;7(2):53–70.
- MSSS-MEES, Protocole: trouble de déficit de l’attention avec ou sans hyperactivité, 2019.
- Currie J, Stabile M, Jones LE. Do stimulant medications improve educational and behavioral outcomes for children with ADHD? NBER, 2013:19105.
- J. Currie J, Stabile M, Jones LE, Do stimulant medications improve educational and behavioral outcomes for children with ADHD? J Health Econ. 2014;37:58–69.
- Diagnostic and Statistical Manual of Mental Disorders-DSM-IV, American Psychiatric Publishing; 1996.
- Diagnostic and Statistical Manual of Mental Disorders-DSM-IV-TR, American Psychiatric Publishing; 2000.
- INSPQ. Surveillance du trouble du déficit de l’attention avec ou sans hyperactivité chez les enfants et jeunes adultes au Québec, 2022.
- HCFEA. Quand les enfants vont mal, comment les aider? Conseil de l’enfance et de l’adolescence; 2023.
- Wolraich ML, Hagan JF Jr, Allan C, et al. Clinical Practice Guideline for the Diagnosis, Evaluation, and Treatment of ADHD in Children and Adolescents. Pediatrics. 2019;144(4):e20192528.
- Psychodynamic diagnostic manual. World Psychiatry; 2006.
- Jeannerod M. Psychothérapie et cerveau. In Monzée J.(dir). Neurosciences et psychothérapie. Liber;2009:33–49.
- Monzée J. Développement de l’enfant et représentations symboliques. In J. Monzée, Ce que le cerveau a dans la tête. Liber;2011:107–144
- Monzée J. Rendez-vous pour la réussite éducative. IDEF;2021.
- Labbé V, Falardeau G, Monzée J, Poulin PC. Le TDAH et la consommation de psychostimulants et autres médicaments. Mémoire déposé à l’Assemblée nationale du Québec; 2019.
- CSSS. Mandat d’initiative sur l’augmentation préoccupante de la consommation de psychostimulants chez les enfants et les jeunes en lien avec le trouble déficitaire de l’attention avec hyperactivité. Assemblée nationale du Québec; 2019.
- INESSS. Portrait des services psychosociaux utilisés dans le traitement du trouble de TDAH chez les Québécois de moins de 25 ans. 2017.
- Haeck J, Lefebvre G, Lefebvre P, Merrigan Ph. Surdiagnostic du TDAH au Québec: impact de l’âge d’entrée à l’école, différences régionales et coûts sociaux et économiques, rapport de projet, CIRANO;2023.
- Gonon F. L’hypothèse dopaminergique du TDAH. In Le Collectif pas de 0 de conduite, Enfants turbulents. Eres. 2008:131–155.
- Faraone S, Asherson P, Banaschewski T et al. Attention-deficit/hyperactivity disorder. Nat Rev Dis Primers. 2015;1:15020.
- Ponnou S, Thomé B. ADHD diagnosis and methylphenidate consumption in children and adolescents: A systematic analysis of health databases in France over the period 2010-2019. Frontiers in Psychiatry. 2022;13:957242.
- Polanczyk G, de Lima ML, Horta BL et al. The worldwide prevalence of ADHD: a systematic review and metaregression analysis. American Journal of Psychiatry. 2007;164(6):942–48.
- INSPQ, Analyse des recommandations en matière de réduction des risques sur la santé associés à l’utilisation des écrans en contexte scolaire. MSSS;2023.
- Monzée J. Impacts socioaffectifs et psychiatriques de l’usage des écrans de loisir chez les jeunes. IDEF;2024.
- Monzée J. Les comportements dérangeants chez l’enfant. In Monzée J.(dir.). Neurosciences, psychothérapie et développement affectif de l’enfant, Liber;2014:199–236.
- Mackes NK, Golm D, Sarkar S et al. Early childhood deprivation is associated with alterations in adult brain structure despite subsequent environmental enrichment. PNAS. 2020;117(1):641–649.
- Shore AN. Affect Regulation And The Repair Of The Self. Norton Professional Books; 2003.
- Porges SW. The polyvagal theory: New insights into adaptive reactions of the autonomic nervous system. Cleve Clin J Med. 2009;76(Suppl 2):S86–S90.
- Psychodynamic diagnostic manual (2nd edition), World Psychiatry, 2015.
- Krueger M. Description of self: An exploratory study of adolescentes with ADHD. JCAPN. 2001;14(2):61–72.
- Koutsoklenis A, Honkasilta J. ADHD in the DSM-5-TR: What has changed and what has not. Front Psychiatry. 2023;13:1064141.
- Monzée J. Neuropsychologie et généticisation: limites scientifiques et éthiques. In Ch. Hervé et al.(dir.). Généticisation et responsabilités. Dalloz;2008:53–78.
- Faraone S, Sergeant J, Gillberg C, Biederman J. The worldwide prevalence of ADHD: is it an American condition? World Psychiatry. 2003;2(2):104–13.
- Rubia K, Overmeyer S, Taylor E et al. Hypofrontality in ADHD During Higher Order Motor Control: a Study with fMRI. INABIS’98;1998.
- Malaspina D, Corcoran C, Kleinhaus KR et al. Acute maternal stress in pregnancy and schizophrenia in offspring. BioMed Central Psychiatry. 2008;8(1):71–80.
- Laplante DP, Brunet A, Schmitz N et al. Project Ice Storm. American Academy of Child and Adolescent Psychiatry. 2008;47(9):1063–1072.
- Valdimarsdóttir M, Hrafnsdóttir AH, Magnússon P, Gudmundsson OO. [The frequency of some factors in pregnancy and delivery for Icelandic children with ADHD]. Laeknabladid. 2006;92(9):609–14.
- Tian XB, Zhao YR, Ma J, Liu F. [Attentiveness in school children: effect of cesarean section birth]. Zhongguo Dang Dai Er Ke Za Zhi. 2009;11(11):913–6.
- Amiri S, Malek A, Sadegfard M, Abdi S. Pregnancy-related maternal risk factors of attention-deficit hyperactivity disorder: a case-control study. ISRN Pediatr. 2012:458064.
- Monzée J. Les sensations cutanées contribuent à la réassurance affective tant du poupon que de sa mère. Spirale. 2019;89:49–59.
- Allen JG. Traumatic relationships, and serious mental disorders. Wiley & Sons Ltd; 2001.
- McGowan PO, Sasaki A, D’Alessio AC et al. Epigenetic regulation of the glucocorticoid receptor in human brain associates with childhood abuse. Nature Neuroscience. 2009;12:342–348.
- CDC, About Adverse Childhood Experiences. Published online October 8, 2024. Accessed April 15, 2025. https://www.cdc.gov/aces/about/index.html.
- Bellato A, Perna J, Ganapathy PS et al. Association between ADHD and vision problems. A systematic review and meta-analysis. Mol Psychiatry. 2023;28(1):410–422.
- Seng KBH, Tan PY, Lim CC et al. High prevalence of xerophthalmia linked to socio-demographic and nutritional factors among vitamin A-deficient rural primary schoolchildren in Malaysia. Nutr Res. 2024;131:14–26.
- Sommer A. Vitamin a deficiency and clinical disease: an historical overview. J Nutr. 2008;138(10):1835–9.
- Généreux M. Enquête en santé psychologique chez les jeunes de 12 à 25 ans. CISSS-Estrie/R3ussir;2023.
- Nagata JM, Ganson KT, Iyer P et al. Sociodemographic Correlates of Contemporary Screen Time Use among 9- and 10-Year-Old Children. J Pediatr. 2022;240:213–220.
- Tamana SK, Ezeugwu V, Chikuma J et al. Screen-time is associated with inattention problems in preschoolers: Results from the CHILD birth cohort study. PLoSOne. 2019;14(4):e0213995.
- Wallace J, Boers E, Ouellet J et al. Screen time, impulsivity, neuropsychological functions and their relationship to growth in adolescent attention-deficit/hyperactivity disorder symptoms. Sci Rep. 2023;13(1):18108.
- Chen YY, Yim H, Lee TH. Negative impact of daily screen use on inhibitory control network in preadolescence: A two-year follow-up study. Dev Cogn Neurosci. 2023;60:101218.
- Likhitweerawong N, Boonchooduang N, Khorana J et al. Executive dysfunction as a possible mediator for the association between excessive screen time and problematic behaviors in preschoolers. PLoSOne. 2024;19(4):e0298189.
- Meri R, Hutton J, Farah R et al. Higher access to screens is related to decreased functional connectivity between neural networks associated with basic attention skills and cognitive control in children. Child Neuropsychol. 2023;29(4):666–685.
- Tong L, Xiong X, Tan H. Attention-Deficit/Hyperactivity Disorder and Lifestyle-Related Behaviors in Children. PLoSOne. 2016;11(9):e0163434.
- van Egmond-Fröhlich AW, Weghuber D, de Zwaan M. Association of symptoms of attention-deficit/hyperactivity disorder with physical activity, media time, and food intake in children and adolescents. PLoSOne. 2012;7(11):e49781.
- Green A, Cohen-Zion M, Haim A, Dagan Y. Evening light exposure to computer screens disrupts human sleep, biological rhythms, and attention abilities. Chronobiol Int. 2017;34(7):855-865.
- Cavalli E, Anders R, Chaussoy L et al. Screen exposure exacerbates ADHD symptoms indirectly through increased sleep disturbance. Sleep Med. 2021;83:241–247.
- Thoma VK, Schulz-Zhecheva Y, Oser C et al. Media Use, Sleep Quality, and ADHD Symptoms in a Community Sample and a Sample of ADHD Patients Aged 8 to 18 Years. J Atten Disord. 2020;24(4):576–589.