





Improving Dementia Diagnosis with the Florida Cognitive Assessment
In Quest of Better Clinicopathologic Correlation in the Diagnosis of Dementia: The Florida Cognitive Assessment
Stephen E. Nadeau, MD1
- Neurology Service and the Brain Rehabilitation Research Center, Malcom Randall VA Medical Center and the Department of Neurology, University of Florida College of Medicine.
OPEN ACCESS
PUBLISHED 30 September 2024
CITATION Nadeau, SE., 2024. In Quest of Better Clinicopathologic Correlation in the Diagnosis of Dementia: The Florida Cognitive Assessment. Medical Research Archives, [online] 12(9). https://doi.org/10.18103/mra.v12i9.5794
COPYRIGHT © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i9.5794
ISSN 2375-1924
ABSTRACT
Introduction: Clinical evaluation of dementia, even by experts, is neither systematic nor optimal and provides a demonstrably inadequate basis for diagnosis of specific underlying pathologies. Post-mortem pathologic evaluation also has serious limitations. As a result, clinicopathologic correlation, even with Alzheimer’s disease and even in a 2024 study, was only 71%. Thus, there is a pressing need for a bedside cognitive evaluation instrument that can potentially improve the accuracy of clinical evaluation. This paper introduces such an instrument, the Florida Cognitive Assessment.
Methods: The Florida Cognitive Assessment was designed by a group of experts in behavioral neurology with the aim of providing a profile of cognitive impairment rather than just a score. Over the years, it has been refined on the basis of clinical experience to take maximal advantage of all observed patient behaviors that could signal impairment in particular cognitive domains. Tests specific to all of the most common dementias are included.
Results and Discussion: In clinical practice, the Florida Cognitive Assessment, a test that requires 10-15 minutes to administer, has proven to be an invaluable tool in fully characterizing the nature of the cognitive profile and in quickly arriving at a diagnosis of a specific type of dementia that is fully congruent with established criteria. Results have also been congruent with those of neuropsychological testing carried out in particular individuals. The Florida Cognitive Assessment has not been empirically validated. The only truly adequate validation would be in terms of post-mortem neuropathology. Psychometric properties could be quantified and correlation of some test results with those of neuropsychological assessment is feasible.
Conclusions: The Florida Cognitive Assessment has already proven to be a very useful tool in providing a means for rapid assessment of the specific domains of impairment in particular individuals with dementia. It has the theoretical potential for substantially improving clinicopathologic correlation.
Keywords: Florida Cognitive Assessment, dementia, Alzheimer’s disease, frontotemporal dementia, Lewy body disease, vascular cognitive impairment, alcoholic dementia
Introduction
The rational for development and application of the Florida Cognitive Assessment (FLACA) lies in the limitations of current clinical assessment of dementia and the shortcomings of clinicopathologic studies. Therefore, this introduction will devote considerable space to detailing these problems, which are at the heart of how we currently go about diagnosing dementia.
The Challenges to be Met
In all neurodegenerative diseases affecting cognition and behavior, the pathology is localized to specific regions of the brain and neuronal subtypes, something first clearly shown by Brun and Gustafson in a pathologic study of Alzheimer’s disease (AD) in 1976
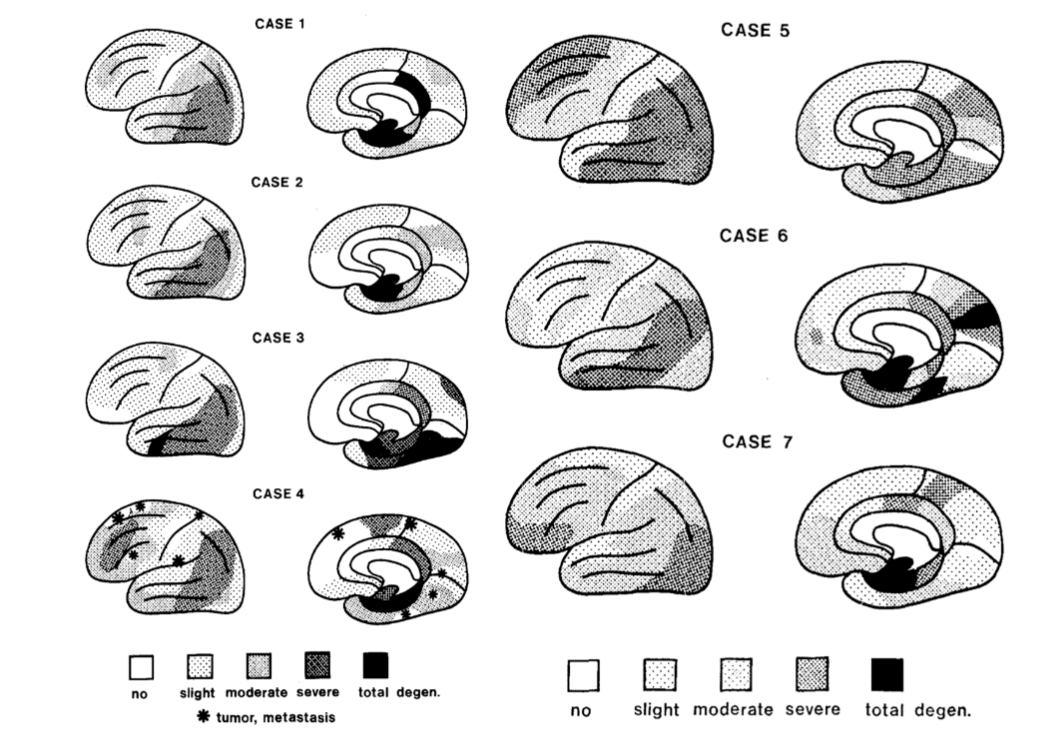
. This study was distinctive in that the entire brain was sampled at 2 cm intervals, sometime supplemented by further intermediate sections. This contrasts markedly with modern studies, which tend to sample a handful of strategically chosen regions. Innumerable imaging studies have since replicated the results of Brun and Gustafson.
Clinical features are generally determined by the anatomic distribution of the neuropathology, which in turn defines the domains of loss of knowledge encoded in neural connectivity in involved areas; this is true in both stroke and dementia. Thus, clinicopathologic correlation has long been key to clinical diagnosis of dementia type. It was a foundational principle in the development of the classification system for the primary progressive aphasias.
Recently, however, the concept of clinicopathologic correlation as a means for diagnosis of dementia has given way to a view that favors reliance on biomarkers, such as phosphorylated tau, Aβ amyloid, and transactive response DNA binding protein 43kDa (TDP-43). In 2018, a committee convened by the National Institute on Aging and the Alzheimer’s Association even concluded that AD should be defined only on its biological basis (i.e., the presence of Aβ amyloid and phosphorylated tau (pTau), irrespective of the clinical presentation). In a 2023, a report by a committee charged by the Advisory Council on Alzheimer’s Research, Care and Services, in accord with the National Alzheimer’s Project Act signed by President Obama in 2011, proffered a set of diagnostic guidelines that included clinical features of no localizing significance.
These rather nihilistic conclusions reflect serious problems in both the clinical and the pathologic components of clinicopathologic correlation. Clinically, a schism has slowly evolved over the last 20 years between behavioral neurologists, who are extensively trained in the nuances of higher cortical function and the specific functional deficits that occur with lesions in particular locations, and dementia neurologists, whose training has come to consist to a greater extent in the diagnosis and management of dementia but may lack depth of training in higher neural function. The development of this schism reflects the fact that behavioral neurologists, who are fundamentally cognitive neuroscientists, have found themselves without a reimbursable role in the clinical world, whereas dementia neurologists are vitally needed to handle the diagnosis and management of the burgeoning population of people with dementing disorders. The result is that, in practice, the diagnosis of dementia has come to rely substantially on rather nonspecific indices, such as the Montreal Cognitive Assessment (MoCA, to be further discussed).
Even in clinicopathologic correlation studies, batteries of well-chosen neuropsychological tests may be used but the Z-scores are averaged to yield a measure of global cognitive function, thereby abolishing all basis for precise correlation. In others, the final diagnosis depends upon the expertise of a neurologist. The basis for their diagnosis is generally opaque. Often terms like “executive dysfunction” and “behavioral disturbances” are used without further definition, even as both include a substantial spectrum of different disorders. In one study, the most common behavioral disturbances were irritability and apathy. In my experience, irritability is almost always a manifestation of depression and thus, is treatable. Apathy (actually abulia or loss of will) may be a manifestation of depression or a consequence of frontal neuropathology. Inappropriate social behavior, the sine qua non of classic behavioral variant frontotemporal dementia (bvFTD), associated with particularly severe disease in right orbitofrontal cortex (see reviews), is not mentioned in many series. However, the very fact that such disorders as corticobasal syndrome and progressive supranuclear palsy are now included within the spectrum of frontotemporal degenerations tells one that there is still considerable variation in the diagnostic criteria applied at the bedside, even by the world’s acknowledged experts.
Confusion about clinicopathologic correlation is compounded by the effects of severe depression, which is recognized only 50% of the time, effects of drugs, particularly neuroleptics, to treat it, and the fact that treatment of depression tends to be fairly conservative, with the result that perhaps as high as 30% of depression is considered refractory. In my own extensive clinical experience, this figure is closer to 2%. Among cognitive neurologists, there seems to be no recognition of disorders of concentration (impairment in working memory, volitional intention, volitional attention, and volitional vigilance), which, in my own clinical experience, make up roughly 30% of patients referred to me for evaluation of cognitive decline. Disorders of concentration usually stem from obstructive sleep apnea or restless leg syndrome/periodic limb movements of sleep, which are usually treatable but commonly not treated. Loss of initiative and akinesia in dementia may be interpreted as evidence of a Parkinsonian disorder or a consequence of neuropathology when actually they may be manifestations of depression. Hallucinations and delusions may be observed in almost any dementia and have no known localizing significance but often bias toward a diagnosis of Lewy body disease.
There have also been major difficulties on the neuropathology end. It has long been recognized that clinicopathologic correlation in dementia can be characterized, at best, as approximate. In a recent clinicopathologic study of 210 patients evaluated by cognitive neurologists in Lund, Sweden, overall clinical-pathological concordance was 61%. In a study of 180 participants in the Brains for Dementia Research cohort at King’s College, London, overall clinicopathologic concordance was 64%.
There are a number of reasons for these clinicopathologic discrepancies. More than one type of pathology can affect a given brain region. Thus, what might appear to be AD, given the cognitive profile, could turn out to reflect classical neurofibrillary tangle pathology (polymerized hyper-phosphorylated tau) ± amyloid plaques in various forms plus TDP-43 pathology, hippocampal sclerosis, Lewy body pathology, and/or limbic-predominant age-related TDP-43 encephalopathy (LATE) neuropathologic changes (particularly in the old old), as well as a host of variously subtle microvascular changes that could be key to pathogenesis. Many studies have demonstrated a high prevalence of mixed pathology but seldom detail the severity or geographic extent of additional pathologies (a notable exception), much less the amount of variance in cognitive impairment they additionally account for. The simple finding of a particular neuropathology does not tell one whether it has any explanatory power for the alteration of cognition and behavior. The neuropathological series published by Selvackadunco et al. suggested that 93% of Lewy body pathology occurred in the context of AD pathology
| Clinical Diagnosis | N | AD | CVD | DLB | AD + CVD | AD + DLB | FTD |
|---|---|---|---|---|---|---|---|
| AD | 75 | 37 | 2 | 1 | 14 | 12 | 7 |
| CVD | 10 | 2 | 1 | 1 | 3 | 2 | |
| DLB | 1 | 3 | |||||
| AD + CVD | 19 | 6 | 1 | 5 | 5 | 2 | |
| AD + DLB | 4 | 1 | 3 | ||||
| FTD | 6 | 1 | 1 | 4 |
. As Beach and Malek-Ahmadi have noted, the great majority of Lewy body pathology in patients with AD does not meet neuropathological diagnostic criteria for Lewy body disease because of insufficient density of pathology and brain regional distribution. In their series of 1,839 cases with extensive AD pathology, micro-infarcts were present in 35% of cases but it was not stated whether their prevalence was sufficient to account for cognitive impairment, a threshold that has been well-established by radiologic criteria. Non-AD tauopathies were found in less than 10%. TDP-43 pathology was found in 35%. James and colleagues found that, in a population of 398 patients with a clinical diagnosis of AD, 64% had TDP-43 pathology in the amygdala (a finding of uncertain if any clinical importance in humans); 50% in the hippocampus and entorhinal cortex (something that could certainly implicate TDP-43 pathology in episodic memory impairment); and 24% in the cerebral cortex. This publication exemplifies the type of work that needs to be done to understand the potential contribution of various pathologies to a given type of dementia. No study seems to have considered a deeper question: the potency of any given pathology in its effect on neuronal structure, function, and longevity.
To conclude
The widely held concept that mixed neuropathologies are the most common cause of dementia at the population level is not well supported primarily because of the failure to take into account the geographic extent, density, and potency of certain types of neuropathology, but also because of frequent reliance of these studies on either the most generic of clinical diagnostic evaluations or the opaque judgement of neurologists of unknown and undoubtedly highly variable expertise.
Two important questions may ride on optimally accurate clinical diagnosis: 1) is it possible to identify certain diagnostic features that might signal the existence of pathology other than that of classic AD? and 2) are we incorrectly using drugs such as donepezil and its congeners and memantine to treat a significant number of people who in whom AD pathology is not the main driver of their dementia? One large study suggests that the phenotype of AD (memory impairment alone, memory impairment + cognitive impairment, and cognitive impairment only is dependent only on the distribution of neurofibrillary tangle pathology and not importantly affected by distribution of TDP pathology.
Three factors are have put us on the threshold of a major crisis in our health care system: 1) inadequacies of clinical diagnosis and assessment of pathology; 2) the ready acceptance of the results of the lecanemab and donanemab trials for translation, despite a major gap between the trial results and adequate scientific justification for drug administration to patients; and 3) the high sensitivity and specificity of serum tests of the Aβ 42/40 ratio and p-tau217 in diagnosing Alzheimer’s disease. Notably, dementia specialists in this study achieved a clinical diagnostic accuracy of 73%. Primary care physicians (PCPs) are going to find themselves beset with large numbers of patients with a positive test who are desperate for treatment and are aware of the availability of lecanemab and donanemab. PCPs are ill-prepared to clinically evaluate these patients or to provide them the advice they need. If normal but worried people constitute a substantial portion of all those tested, then positive results will include a large number of false-positives.
The Rationale for Use of the FLACA
The fundamental premise underlying the use of the Florida Cognitive Assessment (FLACA) is that a substantial contributor to poor clinicopathologic correlation in dementia is the often rather generic evaluation of cognitive function in dementia patients. The goal of the FLACA is to address this deficit, dealing head-on with whatever contribution fragmentary evaluation of cognitive profile makes to less than optimal clinicopathologic correlation. The goal is also to render the judgment of the neurologist evaluating the patient transparent and to assure that it is based on one standard clinical assessment. To what extent the FLACA succeeds in addressing this challenge is a matter of empirical validation.
The FLACA also represents a significant departure from what have become standard approaches. In the spirit of Alexander Luria, a Russian neuropsychologist who made enormous contributions, the FLACA focuses not just on the degree of impairment of cognitive function but on the nature of errors made by patients. Luria found the features of errors to be much more revealing of the nature of the cognitive dysfunction than simply whether or not the patient made an error. Luria’s approach has been the predominant approach of cognitive neuropsychologists over the past 50 years; they have accounted for what I estimate to be 90% of our knowledge of how the cerebrum works. In contrast, neuropsychologists have gravitated to quantitative approaches that are solidly normed and their tests, for the most part, do not take into account the nature of errors. These tests have been highly refined and validated over the years. Neuropsychology programs tend to be highly competitive. Thus, they tend to recruit very smart people who become exacting testers. The problem rises with their interpretation of test results, which all too often does not reflect the knowledge of anatomy and dementias potentially possessed by well-trained neurologists.
The FLACA was designed to be usable by medical generalists, even non-physicians. Simply scoring the major items would be worth a great deal in guiding clinical diagnosis and management. Neurologists and cognitive neurologists, in particular, may at times, on the basis of clues provided by the FLACA performance, together with aberrations in cognition that become evident in the history or the elemental neurologic exam, carry out more highly focused inquiries into either cognitive performance and behavior or the elemental neurological examination, e.g., looking for incipient ophthalmoplegia in a case of suspected corticobasal syndrome; optic apraxia, optic ataxia, and simultaneagnosia — Bálint’s syndrome in suspected posterior cortical atrophy or corticobasal syndrome; or further inquiry into the history when behavioral variant frontotemporal dementia is suspected.
The Potential Role of the FLACA in Future Research
The FLACA could be considered a blueprint for a prospective study assessing the value of this highly refined, localization-specific instrument in more precisely pre-morbidly determining actual neuropathology and even the clinical significance of such superimposed pathologies as TDP-43.
THE FLORIDA COGNITIVE ASSESSMENT
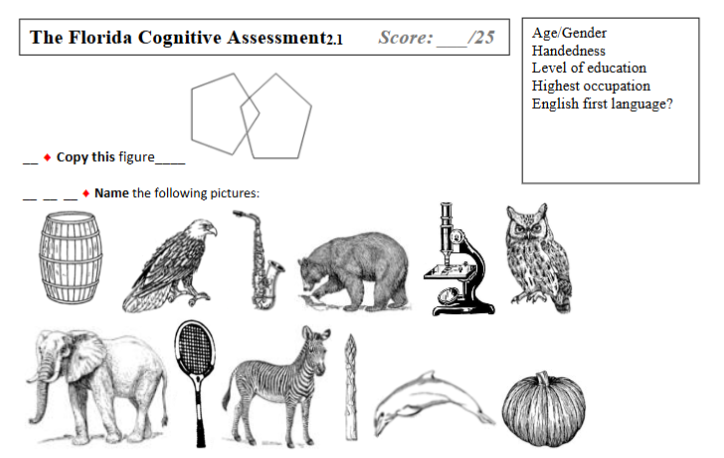
The FLACA is a MoCA-like instrument that was originally developed in 2011 by behavioral neurologists at the University of Florida to correct what were perceived as some important inadequacies of the MoCA in the assessment of patients with dementia. These included insufficient number of objects to be named to adequately ascertain the potential contributions to naming deficits of anomia (caused variously by phonological-semantic disconnection, semantic impairment, and visual/agnosic deficits); the absence of a category fluency test (which is particularly sensitive to the temporal lobe pathology characteristic of AD); the paucity of tests of executive function; and the absence of tests of irregular word reading and praxis. Thus, the FLACA has a 12-item naming test with a frequency distribution spanning the frequencies of the Frances-Kucera inventory; a test of crossed response inhibition (capturing to some degree the set shifting required for the Trailmaking B test); a test of category fluency (animals); a test of irregular word reading; and a test of ideomotor praxis. MoCA items were eliminated that either had questionable face validity or did not probe the deficits that most clearly characterize the various dementias: the Trails B practice test; cube drawing (replaced by the Folstein intersecting pentagons); the continuous performance test; serial sevens (replaced with a simple subtraction); a test of repetition; and a test of similarity identification. Two items were added to probe for features of behavioral variant frontotemporal dementia — one historical because history is most often revealing of the characteristic progressive degradation of personality observed with degeneration of the orbitofrontal cortex.
Errors (#): Anomic_____ Coordinate_____ Superordinate_____ Visual/Agnosic_____ Optic apraxia_____
♦ Spontaneous language:
___Reduced production ___Reduced content/major lexical items ___Semantic/phonemic paraphasias;
___Agrammatic; _Highly detailed history with good recollection of times and places
♦ Crossed response inhibition
Persistent reactive errors___ Errors on set change only___ Couldn’t get into set___
♦ Dorsolateral frontal dysfxn: visual grasp ___ utilization behavior ___ difficulty establishing/maintaining set ___
Poor narrative control_
♦ Language comprehension (esp. during elemental exam): normal/impaired
Subsequent revisions have eliminated some items that were found to have inadequate discriminatory value. Some items primarily assessing severity of cognitive impairment were replaced by items that had more localizing specificity. Items marked with a red diamond () have localizing value. Most particularly, a number of “sub-items” were added. These provide additional qualitative data on the nature of the errors made by patients (in the Luria spirit). They do not require additional examiner time — only documentation of observations made in the course of conducting the FLACA and the elemental neurological exam. They reflect the fact that, in our evaluations of patients, we actually bear witness to a host of different signs but simply fail to attend to them, much less document them. However, although there is great richness of detail latent in addressing the subitems, there is considerable value in just assessing the major items.
Performance on the FLACA yields a total score. However, the most important feature of the FLACA is that it yields a profile of cognitive impairment, rather than just a score, a profile that can, in turn, enable an informed diagnosis of a particular type of dementia. It is possible to achieve a relatively high score on the FLACA even as the particular profile raises concern. For example, a patient with severe impairment in episodic memory but otherwise preserved cognitive function would achieve a score of 21/25. Nevertheless, this profile would indicate serious mesial temporal lobe dysfunction and raise particular concerns about amnestic-variant AD. A patient with bvFTD might score 23/25 — missing only the two items probing social behavior. Given the profile, one can make reasonable inferences about the locus of the pathology, hence the cause of the dementia.
Scoring Guidelines
Copying Pentagons
To be correct, the figure must have two pentagons that intersect to form a diamond.
Naming pictures
Scoring: 11-12 = 3 points 8-10 = 2 points 5-7 = 1 point 0-4 = 0 points. Any type of error: anomic, coordinate, superordinate, or visual/agnosic, is to be counted. An anomic error is characterized by inability of the patient to name the object, even as she clearly knows what it is (e.g., “you play tennis with it”). A semantic error is defined by a near miss, e.g., donkey in lieu of zebra (a coordinate error) or hawk in lieu of bald eagle (a superordinate error). A visual/agnosic error is one in which the patient has no idea what the object is, e.g., calling a microscope a drill-press or asparagus a pencil. A patient with optic apraxia will have difficulty foveating the object to be named. She may name a different object or even start reading text lower on the page. Optic apraxia has nothing to do with language function. It is a parietal sign, first observed by Balint in 1909. Optic apraxia suggests the AD variant, posterior cortical atrophy, but may sometimes be seen with corticobasal syndrome.
Spontaneous language:
This should be scored as impaired if a patient exhibits anyone of a variety of language disorders. A patient may exhibit vagueness, a paucity of content (and of major lexical items such as nouns and verbs), excessive use of nonspecific determiners (“this”, “that”, “these,” “those”, “the usual”, “factory work”), and cannot be pinned down to provide specific information — a sign of degradation of semantic knowledge associated with temporal cortex pathology. It suggests either AD or, much less commonly, semantic dementia. Such patients may also produce semantic near miss errors (semantic paraphasias). Patients may produce a paucity of spontaneous language — a sign of frontal systems disease and most commonly encountered with vascular cognitive impairment. A patient may exhibit phonological paraphasic errors. This may develop in the course of two uncommon dementias. In logopenic primary progressive aphasia, it emerges as a mid to late stage of language impairment characterized throughout its course by word-finding difficulty. In primary progressive nonfluent aphasia, it typically reflects a mid to late phase of a dementia initially characterized by morphologic grammatical errors: omission (in English) or incorrect substitution (in richly inflected languages — everything but English and Chinese) of grammatical morphemes. Grammatical morphemes are the affixes and some little filler words like “is,” “was,” and “by” that signal gender, number, person (he eats, they eat), case (he/him), and tense.
On the other hand, if the patient provides a well-organized and detailed narrative with abundant references to specific times and places, this may be a clue that her impairment is not as severe as the FLACA suggests and that there is another, treatable cause for impairments, e.g., very severe depression.
Crossed response inhibition:
To test crossed response inhibition, the patient is instructed to place both hands palm down on her lap. The examiner then says “when I touch your right hand, you lift your left hand briefly and when I touch your left hand, you lift your right hand briefly.” It may help to lead the patient manually through the motions. The test is best conducted in a way that establishes an alternating set (L/R/L/R). This order is then interrupted without warning by 2-3 taps of one hand. Patients frequently have difficulty after set changes but may soon catch on. Others may never catch on and some may persist in reactive errors (raising the hand touched) throughout the test (both scored as errors) or never even manage to get into the crossed response inhibition set.
Dorsolateral frontal dysfunction:
Utilization behavior, as classically described by L’hermitte, involves appropriate use of items according to their purpose but in defiance of social convention (a failure of constraint by orbitofrontal cortex). However, it may also be exhibited when patients do “what comes naturally” instead of what they are instructed to do (dominance of behavior by automatic plans/responses driven by frontal-postcentral connectivity with inadequate customization of behavior by frontal systems). Utilization behavior always signals frontal systems dysfunction but is not specific to a particular etiology. The cases L’hermitte described had malignant left frontopolar gliomas. Various forms of utilization behavior may occasionally be seen in advanced AD and in alcoholic dementia, vascular dementia, some frontotemporal dementias (FTD) (e.g., certain variants of behavioral variant FTD), and with corticobasal syndrome.
Utilization behavior is most often exhibited during the conduct of the elemental neurologic exam. Inability to suppress saccades to the stimulus during confrontation testing of visual fields constitutes a visual grasp. Instantaneous give-way during muscle strength testing (the response to the counterforce trumps the examiner’s command) also may be a form of utilization behavior (although this may also reflect pain in the joint or motor impersistence — inability to sustain an activity: a frontal sign). Repeated tapping of either nose or the examiner’s finger, or even grabbing the examiners finger during Finger-to-Nose Maneuver is also interpretable as utilization behavior. Occasional patients may repeatedly reach for the examiner’s pen or papers or even into his coat pockets.
It may also be difficult to entrain patients with executive dysfunction in a particular set, e.g., the finger to nose to finger set or the crossed response inhibition set. A patient may exhibit a wandering and often tangential narrative (poor narrative control) — an executive dysfunction that often emerges in later stages of dementias, particularly AD, but may to some extent be apparent in the elderly as a reflection of normal cognitive changes of aging.
Language comprehension:
This can be detected as difficulty performing the commands required for conduct of the elemental neurological exam, in which case it signals disease of temporal cortex and its connections to auditory cortex, as seen with AD, semantic dementia, and sometimes logopenic primary progressive aphasia. In rare cases, it may signal difficulty getting into the set the examiner is trying to establish: a disorder of executive function.
Reading irregular words:
The ability to read irregular words is sensitive to degradation of posterior temporal networks — the hallmark of AD and semantic dementia. Ability to read regular words may be relatively preserved because regularities are deeply encoded in neural connectivity in a different pathway.
Test of visuospatial episodic memory:
The patient’s construction must meet the standards of the copy: two pentagons overlapping to form a diamond. The production need not be pretty.
Clock drawing test:
To be correct, all numbers must be reasonably well arranged in the correct quadrants and the hands must point to 11 and 2 (ten past eleven). Patients routinely produce a host of variations, some incorrect, some possibly idiosyncratic. There is a well validated scoring system that takes all of these into account but this system does not lend itself to the intentionally quickly administered FLACA.
Clock drawing performance is classically impaired in the context of executive dysfunction but it may also reflect right temporal lobe disease, as Luria reported decades ago, in which case performance correlates highly with performance on the Rey-Osterrieth complex picture, a standard assessment tool in comprehensive neuropsychological evaluation.
Test of verbal episodic memory:
Occasional patients have deficits in executive function such that they can never sufficiently get into the set of this test and succeed in immediate repetition of the three items. If this is the case, this should be counted as an error but the subsequent test for recall after distraction should not be scored (i.e., maximum possible score on their FLACA 22/25). It is free recall that we are interested in. Because of the fundamental neuroscience of the hippocampus, which provides the neural substrate for encoding new episodic memories (new facts or experiences), there is no diagnostic value in the results of queued recall.
Ideomotor praxis:
The patient must pantomime the use of the tools. The most common error is a body part as tool error, e.g., emulating the blades of scissors with the fingers rather than pantomiming the correct movement of the hand despite vigorous encouragement to visualize the scissors in their hand. The key criterion for correct use of a screwdriver is rotation on axis. The key criterion for slicing bread is maintaining a smooth back and forth motion that exhibits a constant spatial relationship to the imaginary loaf. Thus, ideomotor apraxia often has two components: an error in the nature of the movement and an error in the spatial relationship of the movement to the target. Slicing an imaginary loaf of bread using the hand as a blade forcefully brought down on the imaginary loaf itself provides a dramatic example.
For this item, we now have two subitems, magnetic apraxia and perseveration of limb position, that are associated with corticobasal degeneration. With magnetic apraxia, the patients hand shows an “inclination” to follow the examiner’s hand. With perseveration of limb position (often termed “alien limb syndrome”), a patient may, for example, leave one arm abducted at the shoulder after deltoid strength testing. One patient had this to say: “don’t worry doc, it will come down when it wants to.” These are not true apraxias. They are best observed during conduct of the elemental neurological exam. Patients with corticobasal syndrome classically exhibit severe ideomotor apraxia, worse in one hand than the other, and may not even be able to imitate arbitrary hand positions created by the examiner or even standard hand gestures, e.g., the thumbs-up sign or the OK sign.
Repeating numbers in reverse order:
Any incorrect sequence is scored as an error. Errors are commonly viewed as a reflection of breakdown in working memory, an executive function, but the fundamental substrate for the neural processes underlying the computation is thought to lie in the post-central cortices, degeneration of which classically defines AD.
Simple subtraction:
The question may be rephrased, e.g., you go to the store and you get something worth 35 cents. You give the clerk a dollar. How much change do you receive? Only an absolutely correct response will suffice. The localizing value of errors is similar to that of impairment in reverse digit span.
Orientation:
Up to a 3-day error in the date can be forgiven. Impaired orientation is most likely a measure of global cognitive impairment and has little localizing value.
Current President:
Only one name will suffice. This test is a very quick assessment of fund of knowledge.
Letter Fluency:
Only common words are allowed: not proper nouns, numbers, days of the week, or inflections/derivatives (fracture, fractured; fat/fatter/fattest). Letter fluency is definitely affected by dementias that affect temporal cortex, e.g., AD, but performance on this test to a substantial degree reflects executive function.
Category Fluency:
Broad groups (e.g., birds), subgroups (e.g., raptors), specific living things, e.g., fire-ants, and breeds (e.g., types of dogs) are allowed. This, much more than letter fluency, is a test of semantic knowledge stores, primarily in temporal lobe cortices. It is therefore far more sensitive than letter fluency to the pathology that characterizes AD and semantic dementia. A typical performance by a patient with mild/moderate AD would be a letter fluency of 8 (normal > 11) and a category fluency of 9 (normal greater than 19).
History of inappropriate social behavior and inappropriate social graces in clinic:
Examples include excessive familiarity, unwanted touching, discussion of intimate matters with strangers, cruelty founded in lack of empathy, and petty crime: in short, the features of bvFTD. This history is often accompanied by inappropriate social behavior in clinic, e.g., inappropriate personal comments, excessive flirting with females in the room, off-color language, inappropriate humor and threatening behavior toward physicians. In many cases, clinic behavior parallels behavior at home, e.g., laughing about the effects of cruelty or grossly inappropriate sexual behavior, even in the presence of the victims.
Discussion
This discussion includes a number of subtopics. It includes a section on localization of cognitive function in the brain to make clear the theoretical potential for the FLACA to tap function in particular regions of the cerebrum. It includes a section on the theoretical potential of the FLACA to identify the key properties of the major causes of dementia. It includes a section entitled Diagnostic Tool Analysis in which shortcomings of the major bedside test now used in the assessment of dementia, the MoCA, relative to the FLACA, are considered, most particularly the limited localizing value of the MoCA. Finally, it includes a section on limitations, which focuses on the opportunities that exist, most critically in prospective neuropathologic studies, for assessing the validity of the FLACA as a bedside diagnostic tool of sufficient accuracy.
Localization
Brain Region
Left Temporal: naming, spontaneous language, language comprehension, reading, ideomotor praxis (temporo-parietal), letter fluency, category fluency, calculation.
Right temporal: construction (copying the intersecting pentagons and clock drawing), although impairment is often a marker of executive dysfunction.
Mesial temporal and hippocampal: episodic memory: recall of intersecting pentagons and 3-word recall.
Parietal: ideomotor apraxia (left inferior parietal); optic apraxia (bilateral superior parietal).
Frontal: copying pentagons, clock drawing, crossed response inhibition, utilization behavior, letter fluency, paucity of spontaneous language, poor narrative control, difficulty getting into or maintaining set, and inappropriate social behavior in clinic or by history (predominantly right orbitofrontal).
Global: reversed digit span, subtraction, orientation, name of president.
Dementia Type:
Alzheimer’s disease:
Impairment in verbal and visuospatial episodic memory; worse category fluency than letter fluency, empty spontaneous language, excessive use of nonspecific determiners in spontaneous language (this, that, these, those, “the usual,” “factory work”); anomic, superordinate, coordinate and occasional visual/agnosic errors on naming to confrontation; and ideomotor apraxia. Dorsolateral frontal deficits often appear as the disease advances.
Posterior cortical atrophy variant of AD:
General picture of AD. The more dorsal variant may be associated with optic apraxia (difficulty accurately saccading to foveate a target) and/or optic ataxia (difficulty placing a finger on the target, e.g., during the finger to nose test), and simultaneagnosia (Balint’s triad). Simultaneagnosia is not included in the FLACA but should be undertaken in patients with suspected parietal lobe disease. Simultaneagnosia can be readily tested using the cookie theft picture from the Boston Diagnostic Aphasia exam (or any other complex picture). Affected patients will tend to zero in on particular items and have enormous difficulty describing the overall meaning of the picture. The ventral variant is associated with visual agnosia (agnosic/visual errors in naming) and particularly severe impairment of reading and writing. Both regions may be affected.
Logopenic primary progressive aphasia:
Another AD variant (though there are some exceptions), this one characterized by presentation with particularly severe word finding difficulties (but not semantic paraphasias, as with semantic dementia) and the relatively early appearance of phonologic paraphasias. Errors in sentence repetition are characteristic. Impairment in episodic memory typically occurs later than in typical AD. Unlike semantic dementia, word comprehension is relatively preserved. The FLACA profile will generally resemble that of AD but the word-finding difficulty during history-taking will be striking.
Behavioral variant frontotemporal dementia (bvFTD):
There exist a number of forms of this disease but the classic form is characterized by prominent changes in personality, loss of empathy, a history of inappropriate social behavior, and social behavior in clinic that tends to make everyone uncomfortable.
Primary progressive nonfluent aphasia:
This is marked by insidiously progressive deterioration of grammatic morphology. In English, this will be manifested as drop out of grammatical morphemes (which convey such things as case, gender, number, person, and mood) but in richly inflected languages will more often appear as incorrect choices of such morphemes (paragrammatisms). Later there will be deterioration of syntax (simplification of sentence structure) and phonology and the development of apraxia of speech (distortion of speech sounds). Language fluency declines, often dramatically. A detailed history of language deterioration and the patient’s spontaneous language in clinic will be most revealing.
Semantic dementia:
Progressive word finding difficulty, empty language, and proclivity for production of semantic paraphasias; loss of knowledge of the world and the objects within it (e.g., “What is a zebra?”), hence impairment in single word comprehension; reading difficulty characterized by substitution with words of similar meaning but different sound (e.g., “sea” in lieu of ocean); and by particular difficulty with reading irregular words (e.g, ocean, thought, yacht). Eventually, impairment in episodic memory and features of bvFTD may appear. The profile on the FLACA will be marked by empty language, semantic paraphasias, abundant coordinate and superordinate errors in naming, marked impairment in irregular word reading, and particularly severe impairment in category fluency and to a lesser extent, letter fluency.
Corticobasal degeneration:
Is now usually referred to as corticobasal syndrome because the various underlying pathologies that have been found, including that of corticobasal degeneration, progressive supranuclear palsy, AD, frontotemporal dementia with TDP-43 inclusions, and Lewy body disease. However, it is worth noting that the study of Shir et al. was a retrospective study in which clinical diagnosis was based on clinicians who, however expert, used largely unknown diagnostic criteria. Corticobasal syndrome, the most protean of dementias, may be difficult or impossible to diagnose on initial evaluation and may become evident only on follow-up evaluation. Important clues are the presence of ideomotor apraxia, often severe, often substantially worse in one hand than the other; perseveration of limb position (arm remains elevated after testing of deltoid strength), magnetic apraxia (patient tends to follow the examiner’s hand with her own); difficulty imitating gestures (e.g., thumbs up sign or “OK” sign and meaningless hand gestures produced by examiner); incipient evidence of hypometric saccades; at least incipient problems with gait and balance reflecting impairment in postural reflexes (detectable on a pull test); and hints of a Parkinsonian syndrome. Other features may include limb rigidity, myoclonus, features of the dorsal variant of posterior cortical atrophy, acalculia, evidence of dorsolateral frontal dysfunction on the FLACA, and apraxia of speech), and even aphasia of various types.
Lewy body disease:
A diagnostic challenge even for neuropathologists (just how much and how widely distributed do the Lewy bodies need to be?). Classically, at least some features of Parkinson’s disease, however subtle, are present within the first year, classically accompanied by rapid eye movement sleep behavior disorder (RBD), and a history of hallucinations and/or delusions. The oft noted fluctuations in level of consciousness seem more likely to be due to an associated sleep disorder, such as restless leg syndrome/periodic limb movements of sleep or obstructive sleep apnea. Patients are hypersensitive to neuroleptics. There is impairment of function on the FLACA with both deficits characteristic of AD (pathologically present in 80-90% of cases) and evidence of frontal systems impairment (reduced language fluency, diminution of both letter and category fluency, faulty reproduction of the intersecting pentagons and clock drawing, defective crossed response inhibition, utilization behavior, and difficulty getting into and maintaining set). Diagnostic challenges are posed by patients with apparent AD who, relatively early in the course, develop hallucinations or delusions. Management is particularly challenging.
Alcoholic dementia:
The concept of alcoholic dementia, its relationship to Korsakoff’s syndrome, and the role of ongoing alcohol consumption remain surprisingly controversial. The current consensus among scientists is that the role of alcohol is negligible or non-existent and that this disorder is entirely related to thiamine deficiency. This conceptualization is considerably at odds with clinical experience. Almost never is a history of Wernicke’s encephalopathy elicitable, even as at least intermittent thiamine deficiency probably played a role. A typical history is that of cognitive deficits that have remained stable since the year that alcohol consumption stopped and of alcohol consumption, sustained over many years, that was very high (e.g., a liter of distilled spirits a day). In moderate cases, the FLACA profile is of dense episodic memory impairment combined with evidence of frontal dysfunction. Often there is some evidence of orbitofrontal disease manifested as a tendency to use humor that is a little risqué and to be over-casual in relationships to professional personnel (including excessive flirtation with women present). The MRI typically reveals dramatic enlargement of the ventricular system. In more advanced cases, the clinical picture is characterized by severe episodic memory impairment, abulia (loss of will — almost universally termed apathy these days), and akinesia. The MRI in such cases typically demonstrates severe atrophy of all intracranial structures.
Vascular dementia:
For many years, the diagnosis of vascular dementia has been applied to both patients with cognitive impairment due to large vessel distribution infarctions and patients with extensive ischemic demyelination due to microvascular hypertensive/atheromatous disease. The consensus view has slowly moved toward applying the term only to patients with diffuse ischemic demyelination. In most cases, the cognitive profile is dominated by concurrent AD and ischemic demyelination is only contributory. Often the diagnosis of pure vascular dementia is made erroneously solely on the basis of the imaging findings. Vascular dementia is characterized predominantly by deficits in frontal lobe functions and reduced language production/simplified syntax, classically accompanied by some degree of akinesia/bradykinesia and increased resting muscle tone on elemental exam. The burden of ischemic demyelination sufficient to have cognitive consequences has been definitively determined by Price and her colleagues. In their 2012 paper, they demonstrated that executive function shows statistically significant decline with involvement of the white matter of as little as 4%. However, my estimate is that it is likely that bedside detectability of this dorsolateral dysfunction, even with use of the FLACA, will be feasible only with demyelination involving 9-17% of the white matter. See Price et al., figure 1, row 1, column3.
The results of the SPRINT MIND study suggest that very aggressive treatment of blood pressure (<120/80) achieved a long-term reduction in cognitive decline and occurrence of dementia. It seems likely that this was due to slowing of the progression of cerebral microvascular disease. This suggests that MRI might be warranted in the routine diagnostic evaluation of people with mild cognitive impairment, particularly if there are features of dorsolateral frontal dysfunction.
Diagnostic Tool Analysis
The MoCA has become the standard bedside instrument for assessment of dementia. The item-by-item inventory of what we view as deficiencies of the MoCA is detailed in the introduction to the section on the Florida Cognitive Assessment. The most useful and most localizing measure in the MoCA is the test of verbal episodic memory (delayed verbal recall). Most crucially, the MoCA does not provide the basis for a systematic evaluation of the function of each of the various regions of the brain involved by the different dementias.
The ascendance of the MoCA also reflects a confusion that has recurred in medicine for decades. The MoCA, by providing a score, serves well to define inclusionary and exclusionary criteria for research studies. However, what is useful for research is not necessarily useful to the clinician. The FLACA is a clinician’s instrument and it is ill-suited as an entry criterion for research studies.
Limitations
The most serious shortcoming of the FLACA is that it has not been adequately validated. The most direct route to at least partial validation is comprehensive neuropsychological testing. However, many of the items assessed on the FLACA do not have neuropsychological counterparts and, as I have noted, much neuropsychological testing tends to assess normed scores rather than the nature of errors. My experience is that, on the occasions that my patients have undergone neuropsychological testing, there has seldom been an important disparity between test results and FLACA performance.
However, the validation that is most needed is against neuropathological examination — for both neuropsychological testing and the FLACA. In the introduction, I reviewed the major gaps in the scientific literature bearing on both the clinical and the neuropathologic anchors that could support such validation. On the clinical end, investigators will need to leave behind global measures of cognitive function and turn to a portfolio of specific neuropsychological measures that are well-established as sensitive and specific indicators of pathology in a specific region of the brain. Neuropathological studies will need to adopt the systematic approach to sampling the entire brain pioneered by Brun and Gustafson, but assessing both the geographic distribution and the density of the various types of neuropathology.
The FLACA, despite its complexity, is certainly a candidate for psychometric assessment, particularly establishment of intra-rater and inter-rater agreement. The FLACA has some fundamental methodologic limitations. Major compromises had to be made to achieve a valid assessment of the entire profile of cognitive function in a 10-15 minute test. The FLACA also lacks any probes of two major right hemisphere functions: comprehension and production of emotional faces and gestures, and comprehension and production of the emotional content of spoken language. These functions are particularly important to relationships between family members. Methods exist to reliably probe these functions but they are far too cumbersome to fit into a brief bedside test.
The FLACA should be readily translatable to other languages — with some significant changes. Some items in the naming to confrontation test, e.g., barrel, bald eagle, and asparagus, might be of excessively low frequency in other languages. The number of irregularly spelled words in English is likely to be almost unique to the language and this item may need to be completely eliminated in the translation. Obviously, letter fluency would need to be tested for a different letter — one associated with a similarly large number words. Norms exist for many languages. Clocks are rapidly becoming a thing of the past. One also has to take into account the effects of bilingualism and poor education and occupation defined mainly by manual labor. Patients are almost always going to do better being able using their first language and when the FLACA is used, every effort should be made to allow them to respond in this language. Patients with low education/lowest level jobs are going to perform less well across the board and allowances need to be made.
Conclusion
Both the clinical assessment of patients with cognitive impairment and neuropathologic examination of the brains of patients with cognitive impairment have serious shortcomings, hence the generally mediocre clinicopathologic correlation that persists to the present. The FLACA, a convenient bedside instrument, seeks to define the full profile of cognitive impairment, thereby offering the theoretical potential for substantially improved clinicopathologic correlation.
Acknowledgements
The original version of the FLACA was developed by a team of cognitive neuroscientists including Adam D. Falchook, Kenneth M. Heilman, Glenn R. Finney, John B. Williamson, and the author.
Conflicts of Interest
The author has no conflicts of interest bearing on this manuscript.
Author Contributions
SEN was entirely responsible for the conceptualization of this paper, the literature review, and writing the paper.
Funding
This work was supported by resources provided by the North Florida/South Georgia Veterans Health System, Gainesville, FL. It was not supported by a specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The contents of this manuscript do not represent the views of the U.S. Department of Veterans Affairs, the United States Government, or the University of Florida.
Data Availability
This paper consists solely of an analytic review and no data were independently collected.
References
- Cullinane PW, Wrigley S, Parmera JB, et al. Pathology of neurodegernerative disease for the general neurologist. Prac Neurology. 2023. Doi: 10.1136/pn-2-23-003988
- Brun A, Gustafson L. Distribution of cerebral degeneration in Alzheimer’s disease. A clinicopathologic study. Arch Psychiat Nervenkr. 1976;223:15-33.
- Nadeau SE. Neural population dynamics and cognitive function. Front Hum Neurosci. 2020;14:50. Doi: 10.3389/fnhum.2020.00050
- Nadeau SE. Language and aphasias. Continuum. 2021;27(6):1549-1561. Doi: 10.1212/CON.0000000000001058
- Gorno-Tempini ML, Hillis AE, Weintraub S, et al. Classification of primary progressive aphasia and its variants. Neurology. 2011;76:1006-1015. Doi:10.1212/WNL.0b013e31821103e6
- Jack CR, Bennett DA, Blennow K, et al. NIA-AA research framework: toward a biological definition of Alzheimer’s disease. Alzheimers Dementia. 2018;14(4):535-562. Doi: 10.1016/j.jalz.2018.02.018
- Petersen RC, Weintraub S, Sabbagh M, et al. A new framework for dementia nomenclature. JAMA Neurology. 2023. Doi: 10.1001/jamaneurol.2023.3664
- Nasreddine Z. Montreal Cognitive Assessment. 2010. https://www.dochub.com/jsfiller-desk13/?flat_pdf_quality=low&mode=cors&requestHash=adb7f1df17c0a2df8183135d0f501601678bf4cd51c43bf59dcf29a847395bde&lang=en&projectId=1534743711&PAGE_REARRANGE_V2_MVP=true&richTextFormatting=true&isPageRearrangeV2MVP=true&jsf-page-rearrange-v2=true&jsf-dss-v2=false&LATEST_PDFJS=true&jsf-redesign-full=true&act-notary-pro-integration=true&jsf-pdfjs-fourth=false&jsf-fake-edit-embedded=false&isSkipEditorLoadFrequency=true&routeId=6a49abfc670ea77b4c86e7788c817034#90ac1b990d6f4720bb5d66f17972116a
- Kapasi A, Yu L, Stewart CS, Schneider JA, Bennett DA, Boyle PA. Association of TDP-43 pathology with domain specific literacy in older persons. Alzheimer Dis Assoc Disord. 2019;33(4):315-320. Doi:10.1097/WAD.0000000000000334
- Gil MJ, Manzano MS, Cuadrado ML, et al. Frontotemporal lobar degeneration: Study of a clinicopathological cohort. J Clinical Neurosc. 2018;58:172-180. Doi: 10.1016/j.jocn.2018.10.024
- Nadeau SE. Neural mechanisms of emotions, alexithymia, and depression. Handb Clin Neurol. 2021;183:299-314. Doi: 10.1016/B978-0-12-822290-4.00014-1
- Boeve BF. Behavioral variant frontotemporal dementia. Continuum. 2022;28:702-725. Doi:10.1212/CON.0000000000001105
- Grossman M, Seeley WW, Boxer AL, et al. Frontotemporal lobar degeneration. Nat Rev Dis Primers. 2023;9:40. Doi:10.1038/s41572-023-00447-0
- Mitchell AJ, Vaze A, Rao S. Clinical diagnosis of depression in primary care: a meta-analysis. Lancet. 2009;374:609-619. Doi: 10.1016/S0140-6736(09)60879-5
- Steffens DC. Treatment-resistent depression in older results. N Engl J Med. 2024;390:630-639. Doi:10.1056/NEJMcp2305428
- Andersson EM, Hoff EJ, Waldö ML, Englund E. Clinicopathological concordance in cognitive disease diagnostics. Clin Neuropathol. 2020;39(3):99-104. Doi: 10.5414/NP301204
- Selvackadunco S, Langford K, Shah Z, et al. Comparison of clinical and neuropathological diagnoses of neurodegenerative diseases in two centers from the Brains for Dementia Research (BDR) cohort. J Neural Transm. 2019;126:327-337. Doi:10.1007/s00702-018-01967-w
- Mehta RI, Schneider JA. What is ‘Alzheimer’s disease’? The neuropathological heterogeneity of clinically defined Alzheimer’s disease. Curr Opin Neurol. 2021;35:237-245. Doi:10.1097/WCO.0000000000000912
- Adler CH, Beach TG, Zhang N, et al. Unified staging system for Lewy body disorders: clinicopathologic correlations and comparison to Braak staging. J Neuropath Exp Neurol. 2019;78(10):891-899. Doi:10.1093/jnen/nlz080
- Bolsewig K, Annemartijn AJMvU, Blujdea ER, et al. Association of plasma amyloid, p-tau, GFAP, and Nfl with CSF, clinical, and cognitive features in patients with dementia with Lewy bodies. Neurology. 2024;102:e209418. Doi:10.1212/WNL.0000000000209418
- Beach TG, Malek-Ahmadi M. Alzheimer’s disease neuropathologic comorbidities are common in the young old. J Alzheimer Dis. 2021;79:389-400. Doi:10.3233/JAD-201213
- Boyle PA, Yu L, Wilson RS, Leurgans SE, Schneider JA, Bennett DA. Person-specific contribution of neuropathologies to cognitive loss in old age. Ann Neurol. 2018;83(1):74-83. Doi:10.1002/ana.25123
- Price CC, Jefferson AL, Merino JG, Heilman KM, Libon DJ. Subcortical vascular dementia: integrating neuropsychological and neuroradiologic data. Arch Neurol. 2005;65(3):376-382. Doi:10.1212/01.wnl.0000168877.06011.15
- Price CC, Mitchell SM, Brumback B, et al. MRI-leukoaraiosis thresholds and the phenotypic expression of dementia. Neurology. 2012;79:734-740. Doi:10.1212/WNL.0b013e3182661ef6
- James BD, Wilson BA, Boyle PA, Trojanowski JQ, Bennett DA, Schneider JA. TDP-43 stage, mixed pathologies, and clinical Alzheimer’s-type dementia. Brain 2016;139(11):2983-2993. Doi:doi:10.1093/brain/aww224
- Josephs KA, Whitwell JL, Tosakulwong N, Weigand SD, Murray ME, Lisesinger AM. TAR DNA-binding protein 43 and pathological subtype of Alzheimer’s disease impact clinical features. Ann Neurol. 2015;78:697-708. Doi:10.1002/ana.24493
- Chin NA, Erickson CM. Alzheimer’s disease, biomarkers, and mAbs — what does primary care need? N Engl J Med. 2024;390(24):2229-2231. Doi:10.1056/NEJMp2401854