

Improving Kidney Biopsy Outcomes: COVID-19 Lessons Learned
Improving patient outcomes: lessons learned from a new kidney biopsy program, a covid-19 era initiative
Karene Corvillo1, Jonathan Cerdán2, Norman Bustamante3
- Hospital Dr. Gustavo Nelson Collado, Section of Nephrology, Department of Medicine, Chitré, Herrera, Panama; Instituto de Ciencias Médicas, Las Tablas, Los Santos, Panamá
 http://orcid.org/0000-0002-4182-6736
http://orcid.org/0000-0002-4182-6736 - Departamento de Patología Humana, Facultad de Medicina, Universidad de Panamá, Panamá City, Panamá http://orcid.org/0000-0003-1245-3579
- Hospital Dr. Gustavo Nelson Collado, Section of Nephrology, Department of Medicine, Chitré, Herrera, Panama http://orcid.org/0000-0002-8896-5194
OPEN ACCESS
PUBLISHED: 31 December 2024
CITATION: Corvillo K, Cerdán J, Bustamante N, et al., 2024. Improving patient outcomes: lessons learned from a new kidney biopsy program, a covid-19 era initiative. Medical Research Archives, Volume 12 Issue 12
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v12i12.6092
ISSN 2375-1924
Abstract
The COVID-19 pandemic exposed vulnerabilities in global healthcare systems, particularly in nephrology. This crisis underscored the importance of innovative solutions to maintain essential services, including timely access to specialized diagnostic procedures.
Kidney biopsy is a crucial diagnostic tool in nephrology, providing essential information for the accurate diagnosis and management of various kidney diseases. In Panama, the pandemic exacerbated existing challenges in providing timely kidney biopsy services. Before the pandemic, patients’ access to kidney biopsies was already limited due to logistical barriers and delays in accessing these procedures, particularly in tertiary care centers, which were heavily impacted by COVID-19.
To address this critical need, our secondary-level healthcare institution established a new kidney biopsy program. This initiative aimed to streamline the process of obtaining kidney biopsies, ensuring that patients received timely diagnoses.
Keywords
- Kidney biopsy
- COVID-19
- Nephrology
- Patient outcomes
- Healthcare innovation
Introduction
The COVID-19 pandemic exposed vulnerabilities in global healthcare systems, particularly in regions with limited resources. This crisis underscored the importance of innovative solutions to maintain essential services, including timely access to specialized diagnostic procedures.
Kidney biopsy is a crucial diagnostic tool in nephrology, providing essential information for the accurate diagnosis and management of various kidney diseases. In Panama, the pandemic exacerbated existing challenges in providing timely kidney biopsy services. Before the pandemic, patients often faced significant delays and limitations in accessing these procedures, particularly in rural areas. This was due to the concentration of specialized services in tertiary care centers, which were frequently overburdened.
To address this critical need, our second-level hospital implemented an in-house kidney biopsy program. This initiative aimed to improve patient access to timely diagnosis, enhance clinical outcomes, and optimize resource utilization. By establishing a dedicated team of skilled professionals and acquiring the necessary equipment, we sought to provide high-quality kidney biopsy services within our institution. This paper delves into the implementation and impact of our program, providing valuable insights for other healthcare institutions considering similar initiatives.
BACKGROUND
Our hospital, a second-level referral center in a rural area of Panama, serves a population of approximately 200,000 individuals. Prior to the COVID-19 pandemic, kidney biopsies were not performed at our institution due to the lack of necessary expertise and infrastructure. Patients requiring these procedures were referred to a tertiary care hospital in the capital city, which became overwhelmed with COVID-19 cases and suspended outpatient services, including kidney biopsies.
IMPLEMENTATION OF THE KIDNEY BIOPSY PROGRAM
To address the unmet need for kidney biopsy services in our region, we developed and implemented an in-house program. We obtained approval from the hospital’s medical management board to initiate the kidney biopsy program. A detailed protocol was developed based on international guidelines and recommendations, outlining the indications, contraindications, procedural steps, and post-procedure care. Healthcare professionals, including interventional radiologists, nephrologists, and nursing staff, were prepared in the technical aspects of kidney biopsy procedures. Essential equipment, such as biopsy needles, ultrasound machines, and sterile supplies, was procured to ensure safe and effective procedures.
Methodology
This is a retrospective cohort study to evaluate the impact of our in-house kidney biopsy program implemented in 2021. We compared patient outcomes and resource utilization before and after the program’s initiation. Data collection was performed from electronic medical records, including patient demographics, clinical characteristics, biopsy indications, procedural outcomes, and histopathological findings. A dedicated database was established to collect all that information. Descriptive statistics were used to summarize patient characteristics and outcomes. We compared the number of kidney biopsies performed, evaluated kidney biopsy indication, monthly ratio, and histopathology results.
ETHICAL CONSIDERATIONS:
The study adhered to ethical principles and was conducted in accordance with the Declaration of Helsinki. All patient data were handled confidentially, and privacy was maintained throughout the study period. Informed consent was obtained from all participants or their legal guardians and detailed information about the procedure, potential risks, and benefits was provided.
Kidney biopsies were performed by an experienced interventional radiologist using ultrasound guidance. Two to three core needle biopsies were obtained from each patient. Cores were immediately stored in 10% buffered formalin for light microscopy and one in Michel’s transport media for immunofluorescence, labeled with patient name and identification number in a transport cooler, to maintain an adequate temperature, and for transportation to the pathology laboratory center the next morning, to the Referral Hospital where the nephropathologist analyzes the samples and sends the reports via web through the platform of the National Pathology System, from where the reports are downloaded only through the user code of the treating physician.
Results
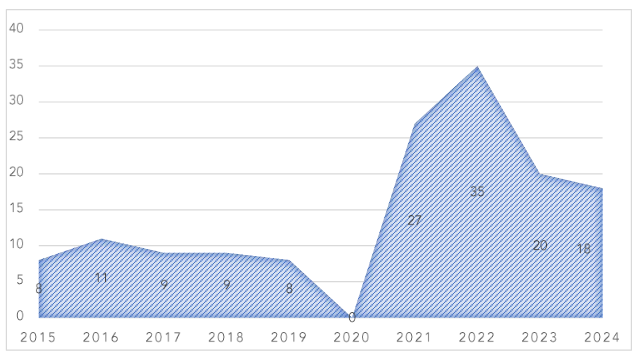
A total of 45 kidney biopsies were performed at the referral center during pre-pandemic period from 2015 to 2019. Since the implementation of our in-house kidney biopsy program in March 2021, a total of 100 biopsies have been successfully performed until October 2024, as seen in Figure 1.
Figure 1. Number of biopsies performed before and after the COVID pandemic.
In patient demographics description, 51% of the patients were female. The minimum age was 17 years (in this center, patients over 16 years of age are considered non-pediatric patients, as established by the institution’s standard) and the maximum age was 79 years, with an average age of 44 years.
Table 1. Kidney biopsy indication.
The indications for biopsy were nephrotic syndrome in 37% of cases, chronic kidney disease (CKD) of unknown cause in 22%, nephritic syndrome in 13%, proteinuria in 12%. Other indications are shown in Table 1.
| Biopsy indication | N |
|---|---|
| Nephrotic syndrome | 37 |
| Chronic kidney disease (CKD) of unknown cause | 22 |
| Nephritic syndrome | 13 |
| Proteinuria | 12 |
| Acute kidney failure | 9 |
| Acute transplant rejection | 6 |
| Microscopic hematuria | 1 |
| Total | 100 |
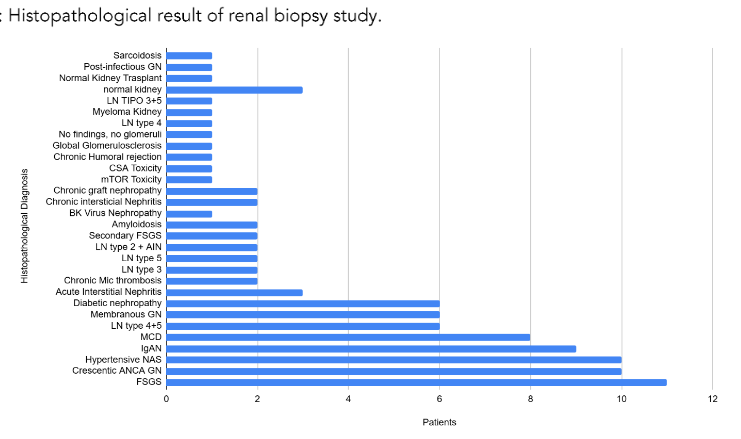
The histopathological results of the biopsies are detailed in Figure 2, the most common being Focal Segmental Glomerulosclerosis, hypertensive nephropathy, ANCA-positive crescentic vasculitis, IgA nephropathy, and minimal change disease. In the case of crescentic vasculitis, thrombotic microangiopathies, and transplanted kidney biopsies, or in any other case that the renal pathologist considered to be an important finding, the report was obtained by telephone 48 hours after the biopsy was performed.
Figure 2: Histopathological result of renal biopsy study.
A total of six patients diagnosed with kidney disease with significant deterioration of kidney function were referred for kidney transplantation after 5 kidney biopsies were performed (up to December 2023). There were also patients who rejected kidney transplantation after being diagnosed with IgA nephropathy.
GN: Glomerulonephritis; LN: Lupus Nephritis; CSA: Ciclosporine associated; mTOR: mammalian target of rapamycin; FSGS: Focal segmental glomerulosclerosis; IAN: interstitial acute nephritis; Mic: microangiopathic; MCD: minimal change disease; IgAN: IgA nephropathy; NAS: Nephroangiosclerosis; ANCA: Anti-neutrophilic cytoplasmic antibodies.
A total of sixteen patients with glomerular kidney disease with significant damage as reported in the histopathology report or acute rejection of kidney transplantation progressed to stage 5 kidney disease after the first 12 months of follow up (from 2021 to October 2023). Before the implementation of the in-house program, an average of 0.75 kidney biopsies were performed per month. After the program’s initiation, this number increased to an average of 2.52 biopsies per month.
Discussion
The pandemic caused significant disruptions in health care services, including diagnostic, prevention, and treatment services for various conditions such as HIV, tuberculosis, sexual and reproductive health, vaccination of children and adults, to mention a few among many that were affected.
These disruptions were largely due to the repurposing of health services to focus on COVID-19, as well as travel limitations and the closure of non-essential businesses. A comparative analysis across 32 countries found substantial disruptions in hospitalizations and ambulatory care, with millions of missed hospitalizations and surgical procedures.
Prior to the COVID-19 pandemic, our second-level hospital encountered significant hurdles in providing timely and accessible kidney biopsy services. Due to a lack of specialized expertise and necessary infrastructure, we were unable to perform these crucial procedures in-house. Patients requiring kidney biopsies were forced to rely on a tertiary care hospital located 115 kilometers away.
However, this referral system proved to be inadequate. The tertiary hospital, serving as a national referral center, was often overwhelmed with patients from across the country.
Overwhelming demand resulted in limited bed availability and extended waiting times for kidney biopsies. Consequently, many patients experienced delays in receiving essential diagnostic services, potentially compromising their health outcomes. A stark reflection of these limitations is evident in the number of kidney biopsies performed during the pre-pandemic period (2015–2019). A mere 45 biopsies were conducted at the referral center during this time.
The COVID-19 pandemic, while a global health crisis, inadvertently catalyzed a significant transformation in our approach to kidney biopsy services. The pandemic exposed the vulnerabilities of centralized healthcare systems and highlighted the need for decentralized solutions. As the tertiary care hospital became overburdened with COVID-19 cases, it was forced to prioritize emergency and critical care, further limiting its capacity to provide elective procedures like kidney biopsies.
Recognizing the urgent need to address this gap in care, our hospital embarked on a mission to establish an in-house kidney biopsy program. This initiative was driven by several key factors, such as improving access to timely diagnosis. By performing biopsies locally, we were able to significantly reduce waiting times and speed up the diagnostic process. This results in a reduction in healthcare costs by eliminating the need for patient transfers and associated costs, such as transportation, ambulance fuel, and accommodation, which substantially reduces costs for both the hospital administration and those of the patient and their families. In addition, this resulted in a strengthening of the healthcare infrastructure, as the establishment of this program improved the capabilities of our hospital and positioned it as a regional center of excellence for the management of kidney disease. More importantly, it improves patient care, as getting an early and accurate diagnosis is crucial for effective treatment and better patient outcomes.
In Latin America and the Caribbean, the pandemic disrupted routine health services. A systematic review highlighted that the pandemic led to interruptions and reduced adherence to chronic therapies. Factors contributing to this included fear of infection, difficulty accessing healthcare facilities, and medication unavailability. In Panamá City, the tertiary referral hospital, overwhelmed by COVID-19 cases, prioritized emergency and critical care, limiting its capacity to perform elective procedures like kidney biopsies. Delays in obtaining biopsy results led to suboptimal patient outcomes. In addition, some treatments were put on hold, either because of lack of access to therapy, lack of medication, lack of diagnosis, or due to the lack of appointments, caused by the closure of day hospital consultations.
However, telemedicine and community pharmacists played a role in maintaining continuity of care for some patients and also led to innovative strategies such as telemedicine and public-private coordination to sustain and recover services. These adaptations highlight the potential for strengthening healthcare systems through innovation and reform.
In response to the challenges posed by the pandemic, our hospital seized the opportunity to establish an in-house kidney biopsy program. Since the implementation of our in-house kidney biopsy program in 2021, we have successfully performed 100 biopsies up until October 2024. This increase in the number of procedures underscores the significant impact of this initiative.
By implementing our in-house kidney biopsy program, we have achieved several significant benefits. We can now provide timely kidney biopsy services to our patients, eliminating the need for long-distance referrals and reducing wait times. Early diagnosis and targeted treatment based on histopathological findings have led to improved patient outcomes and reduced complications. By minimizing the need for patient transfers, we have significantly reduced transportation costs, accommodation expenses, and other associated costs. The cost of a bed day in our second-level hospital is less than in a third-level hospital, even though it is the same public system.
References
1 Bustamante Izquierdo JP, Puertas EB, Hernández Hernández D, Sepúlveda H. COVID-19 and human resources for health: analysis of planning, policy responses and actions in Latin American and Caribbean countries. Hum Resour Health. 2023;21 (1):21. doi:10.1186/s12960-023-00795-8
2 Bharati B, Sahu KS. Effect of COVID-19 pandemic on home delivery of contraceptives by community health workers in India: Time to (re) evaluate and innovate. J Family Med Prim Care. 2022;11(5):1598 -1601. doi: 10.4103/jfmpc.jfmpc_1930_21.
3 Luciano RL, Moeckel GW. Update on the Native Kidney Biopsy: Core Curriculum 2019. Am J Kidney Dis. 2019;73(3):404-415. doi:10.1053/j.ajkd.2018.10.011
4 Courville K, Milord R, Cerrud J, Bustamante N. Overcoming obstacles in Panama to starting a renal biopsy program in a rural area during the COVID-19 pandemic. J Nephrol. 2022;35(9):2387-2389. doi:10.1007/s40620-022-01403-z
5 Fogo AB (2003) Approach to renal biopsy. Am J Kidney Dis; 42(4):826-836. https://pubmed.ncbi.nlm.nih.gov/14520635/
6 Šimunov B, Gunjača M, Čingel B, Škegro D, Knotek M (2018) Safety of Outpatient Kidney Biopsies. Nephron; 138(4):275-279. doi:10.1159/000484991
7 Causey K, Fullman N, Sorensen RJD, et al. Estimating global and regional disruptions to routine childhood vaccine coverage during the COVID-19 pandemic in 2020: a modelling study. Lancet. 2021;398(10299):522-534. doi:10.1016/S0 140-6736(21)01337-4
8 Pennisi F, Odelli S, Borlini S, Morani F, Signorelli C, Renzi C. Impact of the Covid pandemic on timely cancer diagnosis across European healthcare settings: a scoping review. Ann Ig. 2024;36(2):194-214. doi: 10.7416/ai.2024.2596.
9 Baral S, Rao A, Rwema JOT, et al. Competing health risks associated with the COVID-19 pandemic and early response: A scoping review. PLoS One. 2022;17(8):e0273389. doi:10.1371/ journal.pone.0273389
10 Ledesma JR, Chrysanthopoulou SA, Lurie MN, Nuzzo JB, Papanicolas I. Health system resilience during the COVID-19 pandemic: A comparative analysis of disruptions in care from 32 countries. Health Serv Res. Published online September 18, 2024. doi:10.1111/1475-6773.14382
11 Jakovljevic M, Timofeyev Y, Zhuravleva T. The Impact of Pandemic-Driven Care Redesign on Hospital Efficiency. Risk Manag Healthc Policy. 2024(4);17: 1477-1491. doi: 10.2147/RMHP.S465167.
12 Hakroush S, Tampe D, Korsten P, Tampe B. Impact of the COVID-19 Pandemic on Kidney Diseases Requiring Renal Biopsy: A Single Center Observational Study. Front Physiol. 2021 (8);12: 649336. doi: 10.3389/fphys.2021.649336.
13 Hallan SI, Øvrehus MA, Bjørneklett R, Aasarød KI, Fogo AB, Ix JH. Hypertensive nephrosclerosis: wider kidney biopsy indications may be needed to improve diagnostics. J Intern Med. 2021;289(1):69-83. doi: 10.1111/joim.13146.
14 Herrera CA, Juárez-Ramírez C, Reyes-Morales H, et al. COVID-19 Disruption To Routine Health Care Services: How 8 Latin American And Caribbean Countries Responded. Health Aff (Millwood). 2023;42(12):1667-1674. doi:10.1377/ hlthaff.2023.00694
15 Olmastroni E, Galimberti F, Tragni E, Catapano AL, Casula M. Impact of COVID-19 Pandemic on Adherence to Chronic Therapies: A Systematic Review. Int J Environ Res Public Health. 2023;20 (5):3825. doi:10.3390/ijerph20053825
16 Clement J, Jacobi M, Greenwood BN. Patient access to chronic medications during the Covid-19 pandemic: Evidence from a comprehensive dataset of US insurance claims. PLoS One. 2021;16 (4):e0249453. Published 2021 Apr 1. doi:10.1371/ journal.pone.0249453
17 Courville K, McCarthy F, Valdes R. Efectos de la infección por COVID-19 en pacientes renales. Encuesta Latinoamericana ACECANH 2020. Nefrologia Latinoamericana. 2020;17:81-85. doi: http://dx.doi.org/10.24875/nefro.200000461
18 De Foo C, Verma M, Tan SY, et al. Health financing policies during the COVID-19 pandemic and implications for universal health care: a case study of 15 countries. Lancet Glob Health. 2023;11 (12):e1964-e1977. doi:10.1016/S2214-109X(23)00448-5
19 World Health Organization. Accessed November 26, 2024. https://apps.who.int/nha/database#:~:text=The%20Global%20Health%20Expenditure%20Database,2000%20with%20open%20access%20to .
20 Amodu A, Porteny T, Schmidt IM, Ladin K, Waikar SS. Nephrologists’ Attitudes Toward Native Kidney Biopsy: A Qualitative Study. Kidney Med. 2021;3(6):1022-1031. doi: 10.1016/j.xkme.2021.06.014.
21 Kodner C. Diagnosis and Management of Nephrotic Syndrome in Adults. Am Fam Physician. 2016;93(6):479-85. PMID: 26977832.
22 Pana N, Chiotan L, Ciurea O, Petre N, Dumitru D, Capusa C. Is the Prevalence of Biopsy-Proven Glomerulopathies in Adults Changing Over Time? Maedica (Bucur). 2024;19(3):519-525. doi: 10.2657 4/maedica.2024.19.3.519.
23 Hull KL, Adenwalla SF, Topham P, Graham-Brown MP. Indications and considerations for kidney biopsy: an overview of clinical considerations for the non-specialist. Clin Med (Lond). 2022;22(1):34-40. doi:10.7861/clinmed.2021-0472