






Improving Sleep Quality with Botulinum Toxin Treatment
PROSPECTIVE STUDY ON IMPROVING NIGHT’S REST AND QUALITY OF LIFE BY USING BOTULINUM TOXIN
Sistac Palacín, JM Md1. Viñas Salas J, Md.Ph.2, Sistac Ballarin, JM. Md.Ph.1
OPEN ACCESS
PUBLISHED: 28 Febuary 2025
CITATION: PALACÍN, Sistac; SALAS J, Viñas; BALLARIN, Sistac. PROSPECTIVE STUDY ON IMPROVING NIGHT’S REST AND QUALITY OF LIFE BY USING BOTULINUM TOXIN AT A DOSE OF 25 IU IN HEAD AND FACE PATHOLOGIES REFRACTORY TO ORAL TREATMENT. ON 283 CASES. Medical Research Archives, [S.l.], v. 13, n.Available at: <https://esmed.org/MRA/mra/article/view/6228>.
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i2.6228
ISSN 2375-1924
ABSTRACT
The use of Botulinum Toxin is increasingly being extended in different conditions refractory to other treatments.
Thus, it is being used in dystonias, trigeminal neuralgia, migraines, headaches and alterations of the temporomandibular joint.
OBJECTIVES
Primary: To assess the improvement of night rest in the treatment with botulinum toxin type A in chronic Migraine. Trigeminal neuralgia (regardless of the affected branch) and involvement of the temporomandibular joint and/or Bruxism, after therapeutic failure maintained over time. Over more than two years of previous oral or topical drug therapies.
Secondary: To assess the effectiveness of the dose used and its average duration over time.
METHODS: 283 patients of both sexes, aged between 85 and 43 years, were included. The patients studied were separated by sex. Group A: over 80 years old. Group B: between 65 and 79 years old and Group C: under 64 years old.
25 IU of botulinum toxin type A were administered for trigeminal neuralgia, severe temporomandibular joint (TMJ) pain, migraines and headaches. , refractory for two years or more to medical treatments
RESULTS: In all groups, with doses of 25 IU in a single dose, there was a significant improvement in the rest, from the injection, until the six months of control, especially in the group C, in trigeminal neuralgia. It was not significant in the other conditions and/or age groups
CONCLUSIONS: In all groups the effectiveness was greater in trigeminal neuralgia at the established doses P<0.5 and more in the lower group age (C) with more than 6 months of improvement in the condition. In the rest of the pathologies treated, the results at the established doses are very similar to those of the referenced studies. Its use can be effective at doses of 25 IU.
Introduction
In 1949, the first paper was published indicating how botulinum toxin inhibited the release of acetylcholine in the neuromuscular junctions of skeletal muscles, and its possible application in spasticity. This discovery was carried out by Burgen, Dickens and Zatman, and its first medical application was to treat ocular deviation in strabismus.
The use of Botulinum Toxin (BTX-A) was first approved in 1989 by the Food and Drugs Administration (FDA) in the USA, for the treatment of strabismus and blepharospasm in patients over 12 years of age. Nowadays, when we hear about the use of Botulinum toxin or Botox, we almost always associate it with rejuvenation therapies in cosmetic medicine, mainly in the correction of wrinkles on the face, such as those on the forehead, periorbital, nasal and perioral areas, or platysmal bands on the neck.
Medicine discovered its application in many areas of treatment, such as ophthalmology, maxillofacial dentistry, physiotherapy, traumatology, neurology, vascular and in the treatment of chronic pain, among others.
It was in the 80s when it began to be applied in strabismus, blepharospasm, facial hemispasm, dystonia and in cosmetics itself. In the 90s it was already consolidated as a recognized therapeutic alternative in spasticity and dystonia. Later its application was extended to the treatment of autonomic disorders (sialorrhea, hyperhidrosis), facial asymmetry, tension headache, migraine, myofascial pain, chronic lower back pain, musculoskeletal disorders.
Objectives
PRIMARY OBJECTIVE:
To assess the improvement in nighttime rest in treatment with botulinum toxin type A in chronic migraine, trigeminal neuralgia (regardless of the affected branch) and involvement of the temporomandibular joint and/or bruxism, after therapeutic failure maintained for more than two years of previous oral or topical pharmacological therapies.
SECONDARY:
To assess the effectiveness of the dose used.
To confirm this response after six months of treatment.
Methods
Following approval by the Clinical Research Committee CEIC 2894, the study was conducted from January 2020 to November 2024.
A total of 283 patients of both sexes, aged between 43 and 85 years, were included. The patients studied were separated by sex.
-
Group A: over 80 years of age.
-
Group B: age between 65 and 79 years.
-
Group C: under 64 years.
The pathologies studied, and also grouped into groups A, B and C, were:
-
Trigeminal neuralgia
-
Severe temporomandibular joint (TMJ) pain
-
Migraines and headaches refractory for two years or more to medical treatments.
The exclusion criteria were:
-
Age under 18 years
-
Patient refusal to participate in the study
-
Previous infiltrations with corticosteroids or local anesthetics
-
Associated psychiatric disorders
The dose of botulinum toxin type A administered in all cases was 25 IU.
Prior to the infiltration, the patient was asked about the assessment of their night’s rest, using the scale that was approved, and then was asked again 6 months later.
This was subsequently processed by the statistical package for processing means and comparing the study groups SPSS 29.0 — a value of P<0.05 being significant in the different variables studied.
Introduction
It was in the 1980s when it began to be used in strabismus, blepharospasm, facial hemispasm, dystonia and in cosmetics itself. In the 1990s it was already consolidated as a recognized therapeutic alternative in spasticity and dystonia.
Later its application was extended to the treatment of autonomic disorders (salivation, hyperhidrosis), facial asymmetry, tension headache, migraine, myofascial pain, chronic low back pain, musculoskeletal disorders. In recent years, its clear analgesic effect on neuropathic pain has been recognized.
Botulinum toxin was a true revolution in the treatment of focal dystonias and has therefore been a routine treatment for decades in the practice of many specialists, including neurologists, pain treatment specialists and rehabilitation specialists.
The chemical formula is: C6760H10447N1743O20 and is made up of two chains: a heavy chain (H) and a light chain (L).
The H chain binds to the ganglia and to a protein receptor located in the presynaptic nerve endings, while the light chain blocks the release of acetylcholine, which generates paralysis. We found 7 different types, classified from A to G, although clinically only types A and B are useful.
One of its characteristics is the longevity of the action of the toxin, with the protease being the most relevant in avoiding the mechanisms of cellular degradation and surviving in the cytoplasm for a long period of time.
The use of Botulinum Toxin is increasingly expanding in dystonias, hemifacial spasms, masseteric hypertrophy, temporomandibular joint pathologies, masticatory myalgia, recurrent dislocation of the jaw, bruxism or mandibular or oral pain. As well as in chronic migraine (CM) refractory to other treatments.
The first publication about the analgesic benefit of BTX-A in the treatment of trigeminal neuralgia is due to Micheli et al. in 2002.
Results
See tables III, IV and V
TABLE 1 — Demographic Data
| Gender | Total Patients | >80 years | 79–65 years | <65 years |
|---|---|---|---|---|
| Male | 102 — 36.05% | 11 — 10.7% | 72 — 70.82% | 19 — 18.62% |
| Female | 181 — 63.95% | 19 — 10.49% | 98 — 54.14% | 64 — 35.35% |
TABLE 2 — Sleep Scale
| Degree | Description |
|---|---|
| 1 | He wakes up more than twice during the night and has trouble falling asleep. |
| 2 | He wakes up more than twice during the night. It is not difficult for him to fall asleep. |
| 3 | He wakes up less than twice a night but has no trouble falling asleep. |
| 4 | Manages to sleep at least 6 hours straight. |
| 5 | It has no influence on sleep at all. |
TABLE 3. RESULTS 1
| CONDITION (< 64 years) | Mide Ages | NV NM | Pretreatment oral | Previous sleep scale | Average dose of botulinum toxin (IU) | Sleep post interventionism |
|---|---|---|---|---|---|---|
| Trigeminal neuralgia | 54 ± 3 | 7 M / 21 F | yes | 2 ± 1 | 25 | 5 ± 1 |
| TMJ | 32 ± 2 | 5 M / 19 F | yes | 2 ± 1 | 25 | 4 ± 1 |
| Bruxism | 28 ± 4 | 3 M / 5 F | yes | 4 ± 1 | 5 | 4 ± 1 |
| Migraine | 36 ± 4 | 2 M / 14 F | yes | 1 ± 1 | 25 | 3 ± 2 |
| Headaches | 30 ± 5 | 2 M / 5 F | yes | 1 ± 1 | 25 | 3 ± 2 |
Notes:
-
VAE: Visual Analógic Scale
-
N: Number of patients
-
M: Male
-
F: Female
-
IU: International units
-
TMJ: Temporomandibular joint
TABLE 4. RESULTS 2
| CONDITION (79–65 years) | Mide Ages | NV NM | Pretreatment oral | Previous sleep scale | Average dose of botulinum toxin (IU) | Sleep post interventionism |
|---|---|---|---|---|---|---|
| Trigeminal neuralgia | 68 ± 3 | 21 M / 37 F | yes | 2 ± 1 | 25 | 3 ± 1 |
| TMJ | 70 ± 2 | 20 M / 26 F | yes | 2 ± 1 | 25 | 3 ± 1 |
| Bruxism | 67 ± 2 | 9 M / 7 F | yes | 4 ± 1 | 5 | 4 ± 1 |
| Migraine | 66 ± 1 | 21 M / 25 F | yes | 1 ± 1 | 25 | 3 ± 2 |
| Headaches | 70 ± 3 | – M / 3 F | yes | 1 ± 1 | 25 | 3 ± 2 |
Notes:
-
VAE: Visual Analógic Scale
-
N: Number of patients
-
M: Male
-
F: Female
-
IU: International units
-
TMJ: Temporomandibular joint
TABLE 5. RESULTS 3
| CONDITION (> 80 years) | Mide Ages | NV NM | Pretreatment oral | Previous sleep scale | Average dose of botulinum toxin (IU) | Sleep post interventionism |
|---|---|---|---|---|---|---|
| Trigeminal neuralgia | 88.3 | 4 M / 10 F | yes | 2 ± 1 | 25 | 4 ± 1 |
| TMJ | 86.4 | 3 M / 6 F | yes | 2 ± 1 | 25 | 4 ± 1 |
| Bruxism | 88.7 | 2 M / 1 F | yes | 4 ± 1 | 5 | 3 ± 1 |
| Migraine | 85.2 | 1 M / 1 F | yes | 2 ± 1 | 25 | 3 ± 2 |
| Headaches | 87.7 | 1 M / 1 F | yes | 2 ± 1 | 25 | 3 ± 2 |
Notes:
-
VAE: Visual Analógic Scale
-
N: Number of patients
-
M: Male
-
F: Female
-
IU: International units
-
TMJ: Temporomandibular joint
Discussion
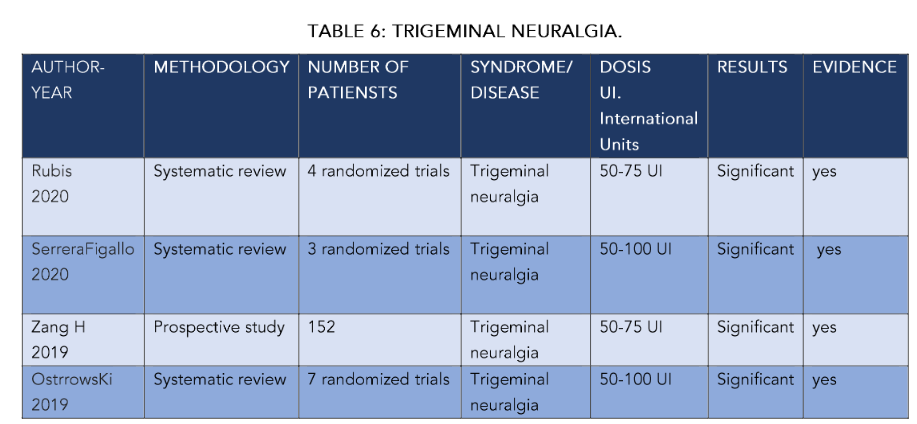
Regarding the treatment of trigeminal neuralgia (TN) with botulinum toxin type A, the work of Rubis included a bibliographic search in PubMed and the Cochrane Library in English from January 2010 to February 2020.
In all groups, with a single dose of 25 IU, there was a significant improvement in sleep quality at 6 months, with averages on the VAS scale of ± 3 points.
This was more significant in cases of trigeminal neuralgia in all groups (P < 0.05), with a longer duration in the younger age groups (around 7 months).
In cases of migraines and headaches, we did not obtain significant values, with average durations of the effect of around 8 months in groups B and C, but less in group A of older patients.
In general, positive responses to the treatments exceeded 5 months on average with the dose of 25 IU, especially in trigeminal neuralgia and bruxism and/or temporomandibular joint disorders, always in the younger age groups.
The review included 4 randomized, double-blind, placebo-controlled trials with a follow-up of 8 to 12 weeks to observe changes in the Visual Analogue Scale (VAS) and in the frequency of TN attacks. The average frequency of TN attacks in 3 studies in the BT-A group decreased by 85%, while in the placebo group only by 15.9%. Maximum efficacy was observed between 6 weeks and 3 months after the procedure, with clear improvement in nighttime rest. They did not differentiate by age, as in our case. Although in all of them, at higher doses (50 IU), they suggest a notable improvement in night rest.
Serrera-Figallo performed systematic searches in the MedLine database looking for research articles published between 2014 and 2019. They found three relevant works on trigeminal neuralgia. This treatment reduced symptoms efficiently enough to satisfy patients, including a notable improvement in rest. These results agree with our study.
As we pointed out, our doses are much lower (25 IU), although these authors do not discriminate by age. We obtain better results (SEE TABLE) in the younger patient group (P < 0.05).
In this same line, we can include the work of Wu on 104 patients, where the authors indicated that their study suggests that the success of the treatment was greater in patients aged 50 years or older (OR = 3.66, 95% CI: 1.231–10.885); in our case, they are under 64 years old.
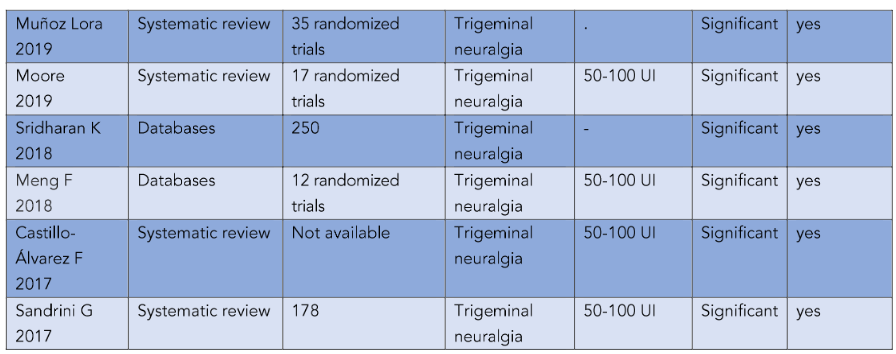
Muñoz Lora carried out a review using the criteria of the American Academy of Neurology on controlled clinical trials in bruxism, temporomandibular disorders, and trigeminal neuropathic pain.
The use of BTX-A is indicated as effective for the treatment of trigeminal neuralgia (category A), being more appropriate than in other pathologies. In our case, the improvement in the quality of rest improved in all groups, although it was evidently higher in trigeminal neuralgia compared to headaches, for example.
Moore, Sridharan, and Meng indicate that in their work, there were significant differences in the hours of sleep. This is also reflected in the work of Castillo. Although, as we can see in Table 6, our results are obtained based on lower doses than those of all these authors, which are between 50 and 100 IU.
Türk conducted a clinical trial in which a total of 27 patients were injected with 100 units of BTX-A at the maxillary and mandibular level—doses 50 IU higher than our study. In these patients, the intensity of pain and the frequency of pain attacks were significantly reduced in the first week, second, and sixth month after treatment, as well as in the quality of sleep and life. This is also reflected in the work of Morra, who searched 10 databases and search engines to access relevant publications, as well as Oh HM et al., who searched the PubMed and OvidSP databases from 1966 to May 2012, and the Hu group, who searched PubMed, EMBASE, Cochrane Library Clinical Trials and Web of Science from January 1966 to March 2013.
Five prospective studies and one double-blind, randomized, placebo-controlled study were identified. Response was achieved in approximately 70–100% of patients, and mean pain intensity and frequency were reduced by approximately 60–100% at 4 weeks after treatment in most studies. No major adverse events were reported. Their quality of life and rest were improved, but we insist on higher doses than those we used (see Table 6).
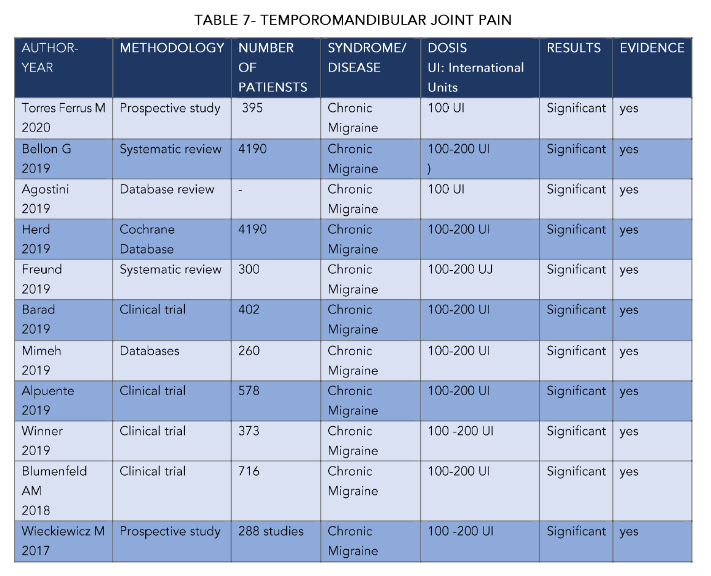
In Table 7, some studies on the treatment of temporomandibular joint pain and bruxism can be observed. These studies did not show, in any age group, a result that improved those obtained in trigeminal neuralgia. And with the exception of the youngest age group, no significant results were obtained.

In this sense, and among these studies, we will comment on the work that Kaya carried out in 2021 with 40 patients with bruxism who were divided into two groups. One group (N: 20) was treated with an occlusive splint and the other group (N: 20) received botulinum toxin injection of the masseter muscle. The maximum bite force decreased in the second and sixth weeks and increased in the third and sixth months in patients who received botulinum toxin. In patients who used splints, there were no changes until the third month and an increase was observed in the sixth month. Although we do not have data on sleep, it is possible to think that this functional improvement also influenced their quality of life.
The Canadian clinical guidelines reviewed by La Fleur indicate that more evidence is required to support decisions on the use of botulinum toxin in these conditions. This can also be seen if we compare our data, particularly in relation to trigeminal pathology.
Shandilya conducted a study on 20 patients with ankylosis of the temporomandibular joint. The patients were subdivided into control and intervention groups. The intervention group received intramuscular injections of BTX-A in the masticatory muscles and showed better results with respect to pain during mouth opening exercises and improvements in mouth opening, with evident improvement in rest and quality of life, although the doses that achieved these results were higher than ours (see Table 7).
Thambar conducted a review in 2020 to critically evaluate the existing evidence on the use of BTX-A in the treatment of temporomandibular joint disorders and masticatory myofascial pain. Three studies showed a significant reduction in pain between the BTX-A and placebo groups and one showed a clinical but non-significant difference. They were unable to perform a meta-analysis due to considerable variation in study designs, heterogeneity between groups, and different assessment tools used.
Machado also conducted a systematic review investigating the effectiveness and safety of botulinum toxin type A (BTX-A) for painful temporomandibular disorders. BTX-A was slightly more effective than placebo for pain reduction at 1 month: mean difference −1.74 points (0–10 scale), 95% confidence interval −2.94 to −0.54, 3 RCTs, 60 participants, I² = 0%. However, there were no significant differences at 3 and 6 months. BTX-A was not associated with a significant increase in the risk of adverse events and was well tolerated. For pain reduction, BTX-A, although effective, decreases in efficacy at 6 and 12 months. In our study, we did not exceed 7 months. Also in this study (Table 7), the mean doses were higher than those we used, although the conclusions are consistent, and the evident improvement in rest was not catalogued on a numerical scale.
Awans searched the PubMed, EMBASE, Scopus, and Web of Science databases in search of randomized clinical trials up to February 2018. In total, there were seven studies that met the eligibility criteria. Two studies showed a significant improvement in temporomandibular myofascial pain and the quality of life of patients, although there is heterogeneity in the ages of the samples.
Ghavimi studied 61 patients who received an injection of 50 units of botulinum toxin in the masseter muscles using an extra-oral injection technique. Doses were similar to ours, obtaining similar results in the different scales studied. This may be the work that best agrees with our results, including the different age range.
De la Torre and his group reviewed the PubMed, Scopus, Web of Science, Embase, Cochrane, Scielo and Lilacs databases from 1980 to March 2016. Randomized controlled trials (RCTs), prospective and before-and-after studies that applied BoNT-A to the masseter and/or temporal muscles were included.
Three RCTs and two studies with 904 identified citations were included in this review. All five articles dealt with sleep bruxism and had a small sample size. None of them dealt with awake bruxism. Two randomized clinical trials were double-blind, with a control group using saline solution. Two studies used polysomnography/electromyography for the diagnosis of sleep bruxism, while others were based on history and examination.
Where the worst results are obtained — and we believe that it is not very effective — is in the treatment of migraines and/or chronic headaches. These are of short duration in time and with many complications associated with their treatment.
In Table 8, we reflect some of the most significant works in the study of these entities. Among these, we highlight those of Torres, who carried out a prospective observational study on 395 patients. After 6 months, 49.1% of the patients responded with improvement in headache pain, associating better quality of sleep and rest — figures similar to our study. Although, we would like to highlight that their doses were double ours.
Bellón in 2019 carried out a review of 90 articles that included 28 trials (N = 4190) treated with botulinum toxin. The longest duration of treatment was three rounds of injections over three months. We administered only one dose (which was effective for an average of 5–6 months). The authors indicated that botulinum toxin could reduce the number of days with migraine per month in the population with chronic migraine by 3.1 days (95% confidence interval (CI): −4.7 to −1.4), with a clear improvement in sleep quality.
In one trial with 1384 participants (high evidence), botulinum toxin reduced the number of days with headache per month by 1.9 days (95% CI: −2.7 to −1.0) and improved nighttime rest, although with higher doses than ours, as can be seen in Table 8. These figures are close to what is described in the rest of the literature, and as we see, improve the sleep scale by several points, although our scale has been adapted and modified to our reality.

Agostini points out that the treatment should be repeated every 3 months to ensure its effectiveness. This review was published in the Cochrane Library systematic reviews before publication of the full review that replaced it in these guidelines. They found 90 articles describing 28 trials (4190 participants). The longest duration of treatment was three rounds of injections with three months between treatments. Migraine severity measured on a visual analogue scale improved by 3 points for chronic migraine and 5 points for episodic migraine on a 10-point scale, with improvement in nighttime rest evident.
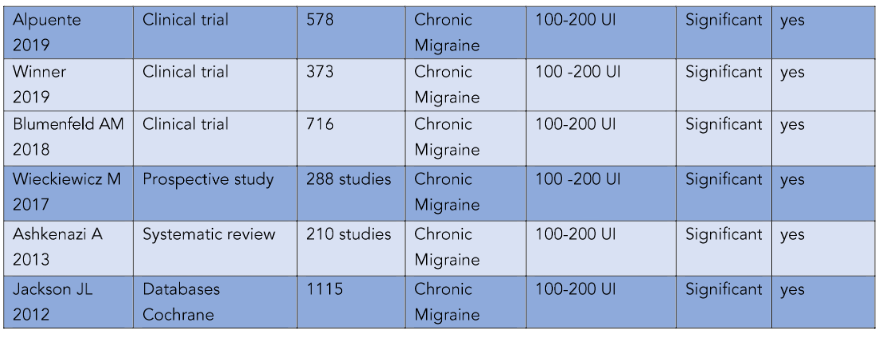
Kelli (2001) conducted three trials with 178 participants. Two trials compared a fixed dose of 100 U plus an optional dose of up to 100 U of botulinum toxin with the maximum dose of topiramate 200 mg/day. The third trial compared treatment with up to 100 U of botulinum toxin with 250 mg of sodium valproate twice a day. Although this improvement was achieved at doses higher than ours, it also showed a higher overall quality of life.
Herd CP consulted the Cochrane database and, in 4190 patients, reached conclusions similar to ours, although, we repeat, with an average dose that doubled ours (200 U vs. 50 U).
Freud analyzed 22 studies that included 300 patients, with a duration typically less than 6 months and with a single treatment period. There was moderate quality evidence that botulinum toxin improved sleep scale scores at doses of 100 U.
The Barad group assessed response in 402 patients with chronic migraine. The mean age was 47 (38–56) years and 83% were women, equivalent to our group C. After 120 days of treatment, 62% of patients reported a reduction in headache frequency, and much improvement in nighttime rest.
In the work of Mimeh et al., the authors performed an evidence-based literature review on the safety and efficacy of botulinum toxin type A in the prophylactic treatment of adult patients suffering from chronic migraine (CM) compared to placebo. They identified a total of 260 articles. They concluded that there was high quality level 1A evidence supporting treatment with BTX-A in adults with CM. This is well tolerated and considered safe, with notable improvement in quality of life and night rest.
Alpuente studied the response in 578 patients and, after 24 months, collected results. The frequency of headache was significantly reduced in 10.5 days from the beginning; 64.0% reported a ≥50% reduction in pain intensity and 70.0% of patients had a ≥50% reduction in the use of analgesics and an improvement in their night rest. For the authors, the efficacy of the use of BTX-A is significant at 6 months, as in our study, and remains stable during follow-up, while pain intensity decreases in a stepwise manner at each time point of the analysis, improving night sleep.
The COMPEL study, in which the Winner490 group participated (NCT01516892), was an open, multicenter, 108-week study.
Conclusions
The improvement in the quality of night rest was more significant in the groups of patients of younger age, although there were no significant differences between them.
In all groups, the effectiveness was greater in trigeminal neuralgia (P < 0.5), increasing its effectiveness in the younger group (C) with more than 7 months of improvement in rest.
There are no differences in the temporomandibular joint in relation to studies with higher doses. It was also slightly effective in cases of headaches and migraines, but there was no significance in this regard (P > 0.05).
References
1. Burgen, A.S.V.; Dickens, F.; Zatman, L.J. The action of botulinum toxin on the neuro-muscular junction. J. Physiol. (Lond.) 1949, 109, 10–24
2. Small RBotulinum toxin injection for facial wrinkles.Am Fam Physicia. 2014. 1;90(3):168-75.
3. DresslerD.Botulinum toxin drugs: brief history and outlook J Neural Transm. 2016;123(3): 277-9.doi: 10.1007/s00702-015-1478-1. Epub 2015 Nov 11.
4. Matak I, Bölcskei K, Bach-Rojecky L, Helyes Z. Mechanisms of Botulinum Toxin Type A Action on Pain. Toxins (Basel). 2019 Aug 5;11(8):459. doi: 10.3390/toxins11080459. PMID: 31387301; PMCID: PMC6723487.
5. Yasaman Safarpour 1, Bahman Jabbari 2 Botulinum toxin treatment of pain syndromes -an evidence based review. 2018;147:120-128. doi:10.1016/j.toxicon.2018.01.017.Epub 2018 Feb 1.
6. Jihye Park 1, Myung Eun Chung 2 Botulinum Toxin for Central Neuropathic Pain. Toxins. 2018; 10(6):224.-30 doi: 10.3390/toxins10060224.
7. Soza S. Cortés Monroy C. Usos prácticos de la toxina botulínica en adultos en medicina física y Rehabilitación REV. MED. CLIN. CONDES – 2014; 25(2) 225-236.
8. Ledermann W. D. Historia del Clostridium botulin Rev Chil Infect Edición aniversario 2003; 39-41
9. Benecke R. Relevancia clínica de la inmunogenicidad de la toxina botulínica. BioDrugs. 2012 Abr 1;26(2):e1-9. doi: 10.2165/11599840-000 000000-00000. PMID: 22385408; PMCID: PMC368 3397.
10. Matak I, Bölcskei K, Bach-Rojecky L, Helyes Z. Mechanisms of Botulinum Toxin Type A Action on Pain. Toxins (Basel). 2019 Aug 5;11(8):459. doi: 10.3390/toxins11080459. PMID: 31387301; PMCID: PMC6723487
11. Nixdorf DR, Heo GB, Major PW. Nixdorf DR, Heo GB, Major PW. Randomized controlled trial of botulinum toxin A for chronic myogenous orofacial pain. Pain. 2002;99:465–73.
12. Song PC, Schwartz J, Blitzer A. The emerging role of botulinum toxin in the treatment of temporomandibular disorders. Oral Dis. 2007;13: 253–60.
13. Nixdorf DR, Heo GB, Major PW. Randomized controlled trial of botulinum toxin A for chronic myogenous orofacial pain. Pain. 2002;99:465–73.
14. Ernberg M, Hedenberg-Magnusson B, List T, Svensson P. Efficacy of botulinum toxin type A for treatment of persistent myofascial TMD pain: A randomized, controlled, double-blind multicenter study. Pain. 2011;152:1988–96.
15. Guarda-Nardini L, Manfredini D, Salamone M, Salmaso L, Tonello S, Ferronato G. Efficacy of botulinum toxin in treating myofascial pain in bruxers: A controlled placebo pilot study. Cranio. 2008;26: 126–35
16. Micheli F, Scorticati MC, Raina G. Beneficial effects of botulinum toxin type a for patients with painful tic convulsif. Clin Neuropharmacol 2002; 25(5):260-2.
17. Rubis A, Juodzbalys G. The Use of Botulinum Toxin A in the Management of Trigeminal Neuralgia: a Systematic Literature Review. J Oral Maxillofac Res. 2020 Jun 30;11(2):e2. doi: 10.5037/jomr.2020.1 1202. PMID: 32760475; PMCID: PMC7393930.
18. Serrera-Figallo MA, Ruiz-de-León-Hernández G, Torres-Lagares D, Castro-Araya A, Torres-Ferrerosa O, Hernández-Pacheco E, Gutierrez-Perez JL. Use of Botulinum Toxin in Orofacial Clinical Practice. Toxins (Basel). 2020 Feb 11;12(2):112. doi: 10.339 0/toxins12020112. PMID: 32053883; PMCID: PMC7076767
19. WU Wu S, Lian Y, Zhang H, Chen Y, Wu C, Li S, Zheng Y, Wang Y, Cheng W, Huang Z. Botulinum Toxin Type A for refractory trigeminal neuralgia in older patients: a better therapeutic effect. J Pain Res. 2019;12:2177-2186. doi: 10.2147/JPR.S205467. PMID: 31410051; PMCID: MC6643497
20. Muñoz Lora VRM, Del Bel Cury AA, Jabbari B, Lacković Z. Botulinum Toxin Type A in Dental Medicine. J Dent Res. 2019;98(13):1450-1457. doi: 10.1177/0022034519875053. Epub 2019 Sep 18. PMID: 31533008
21. Moore D, Chong MS, Shetty A, Zakrzewska JM. A systematic review of rescue analgesic strategies in acute exacerbations of primary trigeminal neuralgia. Br J Anaesth. 2019 Aug;123(2):e385-e396. doi: 10.1016/j.bja.2019.05.026. Epub 2019 Jun 15. PMID: 31208761; PMCID: PMC6676170.
22. Sridharan K, Sivaramakrishnan G. Botulinum Toxin for Refractory Trigeminal Neuralgia: A Trial Sequential Analysis of Randomized Clinical Trials. J Neurosci Rural Pract.;9(1):3-4. doi: 10.4103/jnrp.jnr p_447_17. PMID: 29456335; PMCID: PMC5812155
23. Meng F, Peng K, Yang JP, Ji FH, Xia F, Meng XW. Botulinum toxin-A for the treatment of neuralgia: a systematic review and meta-analysis. J Pain Res. 2018 Oct 12;11:2343-2351. doi: 10.2147/ JPR.S168650. PMID: 30349359; PMCID: PMC6190 814
24. Castillo-Álvarez F, Hernando de la Bárcena I, Marzo-Sola ME. Botulinum toxin in trigeminal neuralgia. Med Clin. 2017;148(1):28-32. English, Spanish. doi: 10.1016/j.medcli.2016.07.032. Epub 2016 Oct 12. PMID: 27743594.
25. TURK Türk Börü Ü, Duman A, Bölük C, Coşkun Duman S, Taşdemir M. Botulinum toxin in the treatment of trigeminal neuralgia: 6-Month follow-up. Medicine (Baltimore). 2017;96(39):e8133. doi: 10.1097/MD.0000000000008133. PMID: 2895 3646; PMCID: PMC5626289.
26. Morra ME, Elgebaly A, Elmaraezy A, Khalil AM, Altibi AM, Vu TL, Mostafa MR, Huy NT, Hirayama K. Therapeutic efficacy and safety of Botulinum Toxin A Therapy in Trigeminal Neuralgia: a systematic review and meta-analysis of randomized controlled trials. J Headache Pain. 2016;17(1):63. doi: 10.118 6/s10194-016-0651-8. Epub 2016 Jul 5. PMID: 273 77706; PMCID: PMC4932020.
27. Oh HM, Chung ME. Botulinum Toxin for Neuropathic Pain: A Review of the Literature. Toxins (Basel). 2015;7(8):3127-54. doi: 10.3390/tox ins7083127. PMID: 26287242; PMCID: PMC4549742.
28. Hu Y, Guan X, Fan L, Li M, Liao Y, Nie Z, Jin L. Therapeutic efficacy and safety of botulinum toxin type A in trigeminal neuralgia: a systematic review. J Headache Pain. 2013;14(1):72. doi: 10.11 86/1129-2377-14-72. PMID: 23964790; PMCID: PMC3765392
29. Kaya DI, Ataoglu H. Botulinum toxin treatment of temporomandibular joint pain in patients with bruxism: A prospective and randomized clinical study. Niger J Clin Pract. 2021;24(3):412-417.
doi: 10.4103/njcp.njcp_251_20. PMID: 33723117.
30. La Fleur P, Adams A. Botulinum Toxin for Temporomandibular Disorders: A Review of Clinical Effectiveness, Cost-Effectiveness, and Guidelines [Internet]. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2020 Feb 25. PMID: 33074614
31. Shandilya S, Mohanty S, Sharma P, Chaudhary Z, Kohli S, Kumar RD. Effect of Preoperative Intramuscular Injection of Botulinum Toxin A on Pain and Mouth Opening After Surgical Intervention in Temporomandibular Joint Ankylosis Cases: A Controlled Clinical Trial. J Oral Maxillofac Surg;78 (6):916-926. doi: 10.1016/j.joms.2020.02.011. Epub 2020 Feb 19. PMID: 32171600.
32. Thambar S, Kulkarni S, Armstrong S, Nikolarakos D. Botulinum toxin in the management of temporomandibular disorders: a systematic review. Br J Oral Maxillofac Surg. 2020;58(5):508-519. doi: 10.1016/j.bjoms.2020.02.007. Epub 2020 Mar 3. PMID: 32143934.
33. Machado D, Martimbianco ALC, Bussadori SK, Pacheco RL, Riera R, Santos EM. Botulinum Toxin Type A for Painful Temporomandibular Disorders: Systematic Review and Meta-Analysis. J Pain. 2020;21(3-4):281-293. doi: 10.1016/j.jpain.2 019.08.011. Epub 2019 Sep 9. PMID: 31513934.
34. Awan KH, Patil S, Alamir AWH, Maddur N, Arakeri G, Carrozzo M, Brennan PA. Botulinum toxin in the management of myofascial pain associated with temporomandibular dysfunction. J Oral Pathol Med.2019;48(3):192-200. doi: 10.1111/jop.12822. Epub 2019 Jan 25. PMID: 30604895.
35. Ghavimi MA, Yazdani J, Afzalimehr A, Ghoreyshizadeh A, Dehnad SV. Effect of injection of botulinum toxin on decreasing the symptoms and signs of masticatory muscles in patients with temporomandibular dysfunction. J Dent Res Dent Clin Dent Prospects. 2019 Spring;13(2):128-132. doi: 10.15171/joddd.2019.020. Epub 2019 Aug 14. PMID: 31592308; PMCID: PMC6773914
36. De la Torre Canales G, Câmara-Souza MB, do Amaral CF, Garcia RC, Manfredini D. Is there enough evidence to use botulinum toxin injections for bruxism management? A systematic literature review. Clin Oral Investig. 2017;21(3):727-734. doi: 10.1007/s00784-017-2092-4. Epub 2017 Mar 2. PMID: 28255752.
37. Thomas NJ, Aronovich S. Does Adjunctive Botulinum Toxin A Reduce Pain Scores When Combined With Temporomandibular Joint Arthroscopy for the Treatment of Concomitant Temporomandibular Joint Arthralgia and Myofascial Pain? J Oral Maxillofac Surg. 2017;75(12):2521-2528. doi: 10.1016/j.joms.2017.04.011. Epub 2017 Apr 19. PMID: 28500876.
38. Torres-Ferrus M, Gallardo VJ, Alpuente A, Pozo-Rosich P. Influence of headache pain intensity and frequency on migraine-related disability in chronic migraine patients treated with OnabotulinumtoxinA. J Headache Pain. 2020;21(1):88. doi: 10.1186/s101 94-020-01157-8. PMID: 32652924; PMCID: PMC7353810.
39. Bellon G, Venturin A, Masiero S, Del Felice A. Intra-articular botulinum toxin injection in complex regional pain syndrome: Case report and review of the literature. Toxicon. 2019;159:41-44. doi: 10.10 16/j.toxicon.2019.01.002. Epub 2019 Jan 17. PMID: 30660558.
40. Agostoni EC,Barbanti P, Calabresi P, Colombo B, Cortelli P, Frediani F, Geppetti P, Grazzi L, Leone M, Martelletti P, Pini LA, Prudenzano MP, Sarchielli P, Tedeschi G, Russo A; Italian chronic migraine group. Current and emerging evidence-based treatment options in chronic migraine: a narrative review. J Headache Pain. 2019;20(1):92. doi: 10.1186/s10194-019-1038-4. PMID: 31470791; PMCID: PMC6734211.
41. Kelli. AM. The minimum clinically significant difference in visual analogue scale pain score does not differ with severity of pain. Emerg Med J 2001; 18:205–7. 10.1136/emj.18.3.205.
42. Luvisetto S. Botulinum Toxin and Neuronal Regeneration after Traumatic Injury of Central and Peripheral Nervous System. Toxins (Basel). 2020;12 (7):434. doi: 10.3390/toxins12070434. PMID: 3263 0737; PMCID: PMC7404966
43. Herd CP, Tomlinson CL, Rick C, Scotton WJ, Edwards J, Ives NJ, Clarke CE, Sinclair AJ. Cochrane systematic review and meta-analysis of botulinum toxin for the prevention of migraine. BMJ Open. 2019;9(7):e027953. doi: 10.1136/bmjopen-2018-027953. PMID: 31315864; PMCID: PMC6661 560.
44. Herd CP, Tomlinson CL, Rick C, Scotton WJ, Edwards J, Ives NJ, Clarke CE, Sinclair AJ. Cochrane systematic review and meta-analysis of botulinum toxin for the prevention of migraine. BMJ Open. 2019;9(7):e027953. doi: 10.1136/bmjopen-2018-027953. PMID: 31315864; PMCID: PMC6661 560.
45. Freund B, Rao A. Efficacy of Botulinum Toxin in Tension-Type Headaches: A Systematic Review of the Literature. Pain Pract. 2019;19(5):541-551. doi: 10.1111/papr.12773. Epub 2019 Apr 22. PMID: 30742360.
46. Barad M, Sturgeon JA, Fish S, Dexter F, Mackey S, Flood PD. Response to BotulinumtoxinA in a migraine cohort with multiple comorbidities and widespread pain. Reg Anesth Pain Med. 2019; 44(6):660-668. doi: 10.1136/rapm-2018-100196. PMID: 31101743.
47. Mimeh H, Fenech Magrin AM, Myers S, Ghanem AM. A Critical Review of Botulinum Toxin Type A in the Prophylactic Treatment of Chronic Migraine in Adults. Aesthet Surg J. 2019;39(8):898-907. doi: 10.1093/asj/sjy224. PMID: 30184084.
48. Alpuente A, Gallardo VJ, Torres-Ferrus M, Alvarez-Sabin J, Pozo-Rosich P. Early efficacy and late gain in chronic and high-frequency episodic migraine with onabotulinumtoxinA. Eur J Neurol. 2019;26(12):1464-1470. doi: 10.1111/ene.14028. Epub 2019 Jul 18. PMID: 31220392.
49. Winner PK, Blumenfeld AM, Eross EJ, Orejudos AC, Mirjah DL, Adams AM, Brin MF. Long-Term Safety and Tolerability of OnabotulinumtoxinA Treatment in Patients with Chronic Migraine: Results of the COMPEL Study. Drug Saf. 2019;42(8):1013-1024. doi: 10.1007/s40264-019-00824-3. PMID: 31102144
50. Castrillo Sanz A, Morollón Sánchez-Mateos N, Simonet Hernández C, Fernández Rodríguez B, Cerdán Santacruz D, Mendoza Rodríguez A, Rodríguez Sanz MF, Tabernero García C, Guerrero Becerra P, Ferrero Ros M, Duate García-Luis J. Experience with botulinum toxin in chronic migraine. Neurologia. 2018;33(8):499-504. English.
51. Blumenfeld AM, Stark RJ, Freeman MC, Orejudos A, Manack Adams A. Long-term study of the efficacy and safety of OnabotulinumtoxinA for the prevention of chronic migraine: COMPEL study. J Headache Pain. 2018;19(1):13. doi: 10.1186/s10194-018-0840-8. PMID: 29404713; PMCID: PMC5799088
52. Erdemoglu AK, Varlibas A. The long-term efficacy and safety of botulinum toxin in refractory chronic tension-type headache. J Headache Pain. 2007 Oct;8(5):294-300. doi: 10.1007/s10194-007-0414-7. Epub 2007 Oct 23. PMID: 17955170; PMCID: PMC3476152.
53. Mathew NT, Jaffri SF. A double-blind comparison of onabotulinumtoxina (BOTOX) and topiramate (TOPAMAX) for the prophylactic treatment of chronic migraine: a pilot study. Headache 2009;49:1466–78. 10.1111/j.1526-4610.2009.01566.x
54. Venancio Rde A, Alencar FG Jr, Zamperini C. Botulinum toxin, lidocaine, and dry-needling injections in patients with myofascial pain and headaches. Cranio. 2009 Jan;27(1):46-53. doi: 10.1179/crn.2009.008. PMID: 19241799.
55. Jackson JL, Kuriyama A, Hayashino Y. Botulinum toxin A for prophylactic treatment of migraine and tension headaches in adults: a meta-analysis. JAMA. 2012; 307(16):1736-45. doi: 10.1001/jama.2012.505. PMID: 22535858.