

Incidence of Secondary Overtriage in Trauma Patients
Incidence of Secondary Overtriage in Trauma Patients During the COVID-19 Pandemic
Joshua Hill1, Bhairav Shah1, Emily Rady1, Norwood Yost2, Samuel Schonfeld2
- OhioHealth Grant Medical Center Department of Trauma Columbus, Ohio, United States.
- Ohio University Heritage College of Osteopathic Medicine Dublin, Ohio, United States.
OPEN ACCESS
PUBLISHED: November 2024
CITATION: Hill, J., Shah, B., Rady, E., Yost, N., & Schonfeld, S. (2024). Incidence of Secondary Overtriage in Trauma Patients During the COVID-19 Pandemic. Medical Research Archives, 12(11). https://doi.org/10.18103/mra.v12i11.4673
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v12i11.6073
ISSN 2375-1924
Abstract
Introduction: Secondary Overtriage (SO) has been defined as transfer to a higher level of care without intervention or ICU admission, and is determined from the accepting facility within 48 hours. The COVID-19 pandemic placed additional stressors on healthcare delivery. This study aimed to explore the effect of the COVID-19 pandemic on SO rates.
Methods: We identified the beginning of the COVID-19 pandemic as March 20, 2020. This retrospective cohort study analyzed trauma patients transferred to our center from January 1, 2019, to December 31, 2021. The primary outcome was the incidence of SO before and during the COVID-19 pandemic.
Results: A total of 6774 patients were transferred to our level 1 trauma center. Overall, 27.9% (n=1914) of transferred patients did not require intervention. The overall rate of SO before the pandemic was 29.1% while during the pandemic it was 26.6% (p=0.37). There was no significant difference in the incidence of SO between patient groups. The most commonly consulted specialties were Speech and Language Pathology, Neurosurgery, Orthopedic Surgery, and others.
Discussion: To our knowledge, this is the first study examining the rate of SO before and during the COVID-19 Pandemic. The overall rate of SO was similar between groups, suggesting that the pandemic did not significantly alter the incidence of SO.
Keywords
Secondary Overtriage, Trauma Patients, COVID-19 Pandemic, Healthcare Delivery
Introduction
Level 1 trauma centers provide a full spectrum of care to the injured patient¹. They play a vital role in local and regional healthcare systems by acting as a safety net for surrounding, less equipped facilities¹. Rural areas of the United States often have an incidence of traumatic injury that is not matched with facilities that are verified trauma centers²²⁻²⁴. Our institution in particular admits patients transferred in from a large rural swath of our state where traumatic injury is prevalent, but no verified trauma centers exist. These patients are often transferred to a higher level for specialized care. Common reasons for transfer include subspecialty consultation, specifically Neurosurgery, Orthopedic Surgery, and Plastic Surgery⁵.
However, there is accumulating evidence to suggest that patients are being transferred for non-life-threatening injuries and even non-medical reasons²³. This phenomenon is known as secondary overtriage (SO). Definitions of SO in trauma vary, however, most definitions include: a length of stay <24–48 hours, low injury severity score, no need for major surgical interventions, and no need for critical care⁴⁻⁶. The rate of SO in existing literature ranges from 12.2 – 39%¹,⁴,⁵,⁷⁻⁹. Overtriage can negatively affect patients, providers, and the healthcare system. It displaces patients from their homes and leaves loved ones to travel to farther tertiary care centers⁵, as well as increased cost to the patient with estimates ranging from $2859 – $47,233⁵,¹⁰,¹¹.
Hospitals may have a financial incentive to accept or reject these patients due to net profit for each patient ranging from -$2673 to +$25694¹². Aside from financial gain or loss, however, hospitals must consider resource allocation. SO may lead to overcrowding and may take away resources from severely injured patients to be used for patients with minor injuries¹³. SO can lead to excessive workload for providers which has been shown to cause burnout¹⁴.
The Coronavirus Disease 2019 (COVID-19) pandemic stressed hospital systems nationwide. COVID-19 altered patterns of trauma admission volume, mechanism of injury, and mortality¹⁵,¹⁶. How COVID-19 impacted SO, however, is unclear. The purpose of our study was to evaluate the effects of the COVID-19 pandemic on rate and reasons for SO. Secondarily, we hope to quantify SO and describe patterns of SO to minimize its negative impact to patients and the hospital system in the future. We hypothesized that the incidence of SO at our institution increased over the course of the COVID-19 pandemic. We also hypothesize that patients who are overtriaged are likely to be discharged from the ED after transfer.
Methods
An Institutional Review Board approved retrospective study was conducted at our American College of Surgeons nationally verified Level 1 Trauma Center located in Columbus, Ohio in the United States. We admit patients from both our local urban location, as well as rural areas from as far as 125 miles away. Data was collected from January 1st, 2019 to June 18th, 2021. Inclusion criteria were patients ≥18 years old who were transferred to our institution for trauma evaluation and met our definition of secondary overtriage. We defined secondary overtriage as patients who were discharged alive within 48 hours and did not require operative intervention or ICU admission.
We defined the beginning of the COVID-19 pandemic as March 18th, 2020, when our state’s (Ohio) governor began closing businesses, declaring a health emergency. The 15 months of data collected before this date was classified as pre-pandemic (PP) while 15 months of data collected after this date was classified as intra-pandemic (IP).
Clinical data collected via a chart review included demographics (age, sex), admission vitals, Glasgow Coma Score (GCS), mechanism of injury (MOI), injury severity score (ISS), insurance status, transfer day and distance, number of CT scans, treatments received, and specialists consulted. Our primary outcome was rate of SO in PP and IP.
Our secondary outcome was disposition from the ED.
Descriptive statistics were reported as means and standard deviations for continuous or semi-continuous variables and as frequencies with percentages for categorical data. Mann-Whitney U-tests (continuous variables) or chi-squared tests (categorical variables) were used to determine whether select variables differed significantly between patient groups. The usual p < 0.05 was required for statistical significance.
Results
During the study period, 6774 patients were transferred to our level 1 trauma center. Overall, 29.1% (1974) of transferred patients met our definition of SO. 29.7% (948/3196) of patients were overtriaged PP while 28.7% (1026/3578) were overtriaged IP. There was no significant difference in the rate of SO between the two groups (p > 0.37).
The average age overall was 47.6 ± 19.8 years. Most of the overtriaged patients were males (61.1%). The most common mechanism of injury (MOI) was found to be falls (37.7%), followed by MVCs (35.2%). More patients were assaulted PP than IP (12.9% PP, 8.6% IP, p = 0.002). Overall, average GCS was 14.7 ± 1.4 and average ISS was 6.2 ± 4.6.
Age, sex, average transfer distance, and insurance status were not significantly different between PP and IP. Additionally, GCS and ISS were both found to be significantly lower PP (p = 0.002 and p = 0.022, respectively).
The overall average transfer distance was 46.3 ± 30 miles. Most overtriaged patients had Medicare or commercial insurance (60.8%). A summary of demographics can be found in Table 1.
Table 1: Demographics of the PP and IP Groups
| PRE-PANDEMIC (N=948 unless otherwise indicated) | INTRA-PANDEMIC (N=1026 unless otherwise indicated) | P-value | |
|---|---|---|---|
| AGE | 47.4 (19.3) | 47.7 (20.3) | 0.93 |
| SEX | 558 M (58.9%) 390 F (41.1%) |
648 M (63.2%) 378 F (36.8%) |
0.05 |
| AVERAGE TRANSFER DISTANCE (miles) | N=947 46.1 (28.4) |
N=1026 46.5 (31.5) |
0.97 |
| INSURANCE | N=941 COMMERCIAL/MEDICARE: 585 (62.2%) MEDICAID: 296 (31.5%) UNINSURED: 60 (6.4%) |
N=1021 COMMERCIAL/MEDICARE: 607 (59.5%) MEDICAID: 345 (33.8%) UNINSURED: 69 (6.8%) |
0.47 |
| MOI | N=944 MVC: 316 (33.5%) FALL: 349 (37.0%) STAB: 8 (0.8%) ASSAULT: 122 (12.9%) GSW: 20 (2.1%) OTHER*: 129 (13.7%) |
N=1020 MVC: 375 (36.8%) FALL: 391 (38.3%) STAB: 14 (1.4%) ASSAULT: 88 (8.6%) GSW: 27 (2.6%) OTHER*: 125 (12.3%) |
0.026 |
| GCS | N=921 14.8 (1.2) |
N=1002 14.7 (1.5) |
0.002 |
| ISS | N=928 6.0 (4.5) |
N=980 6.5 (4.8) |
0.022 |
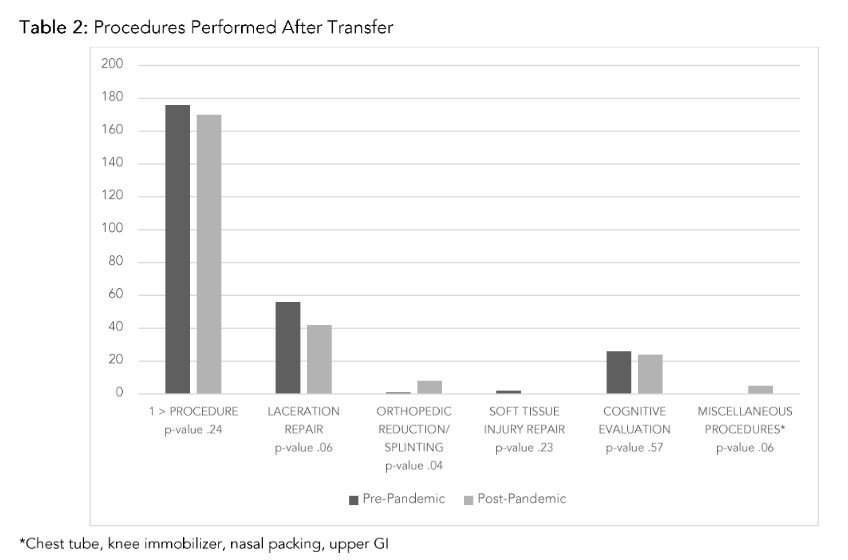
Table 2 summarizes the procedures performed after patients were transferred. Overall, 17.5% of overtriaged patients had at least 1 procedure after transfer (18.6% PP, 16.6% IP, p=0.24). The most common procedure after transfer was laceration repair (5.0%). More patients transferred IP required orthopedic reduction/splinting (0.1% PP, 0.8% IP, p=0.04).
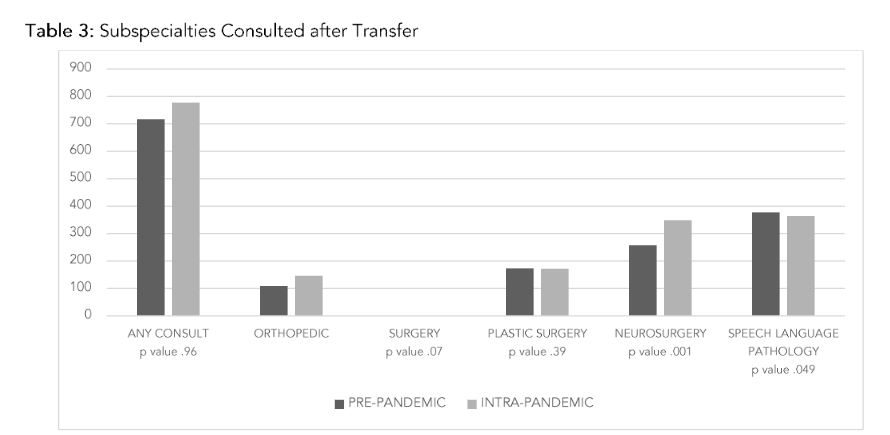
Overall, 75.7% of patients had at least one subspecialty service consulted after being transferred (Table 3). Speech Language Pathology (SLP) was the most commonly consulted service after transfer (39.8% PP, 35.5% IP, p=0.049). Neurosurgery was the second most common (27.2% PP, 34.0% IP, p=0.001).
We examined the disposition of the patients who met the definition for significant overtriage. Results are found in Table 4. Of the patients transferred to our center, only 2 patients were discharged home from the ED, one each from both the PP and IP cohorts. More patients were transferred from the Emergency Department to Observation and Intermediate levels of care IP, while fewer patients were transferred to the Floor.
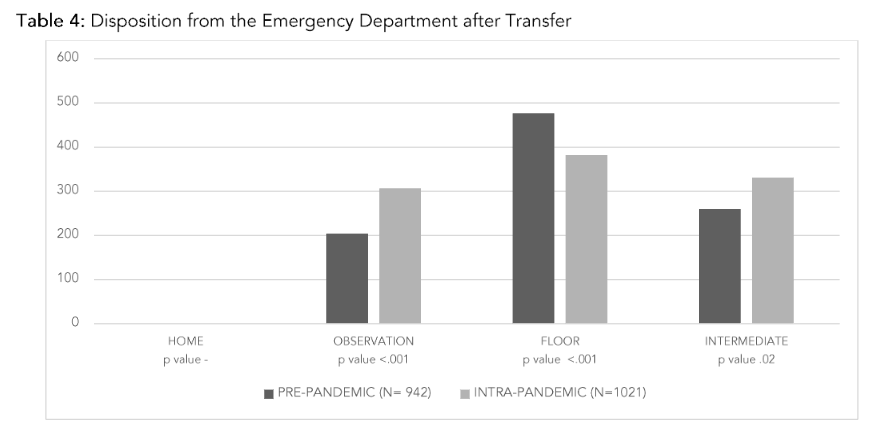
Table 4: Disposition from the Emergency Department after Transfer
We examined the disposition of the patients who met the definition for significant overtriage. Results are found in Table 4. Of the patients transferred to our center, only 2 patients were discharged home from the ED, one each from both the PP and IP cohorts. More patients were transferred from the Emergency Department to Observation and Intermediate levels of care IP, while fewer patients were transferred to the Floor.
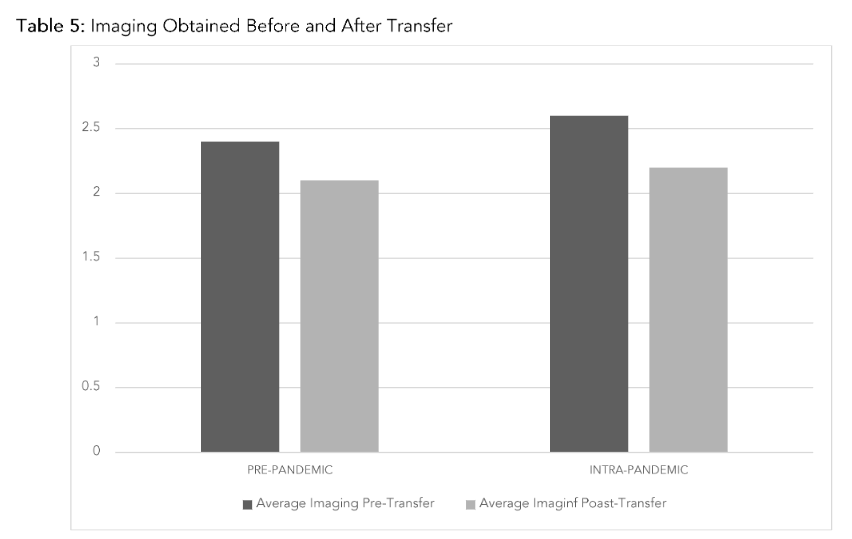
Table 5: Imaging Obtained Before and After Transfer
A summary of the number of images obtained before and after transfer is found in Table 5. Pre-Pandemic, the average number of pre-transfer images was 2.4 (SD 1.9) and Post-Transfer was 2.6 (SD 1.9). The IP group had a significantly lower average number of pre-transfer CT scans with 2.1 (SD 1.9) and Post-Transfer 2.2 (SD 1.9) (p=0.004).
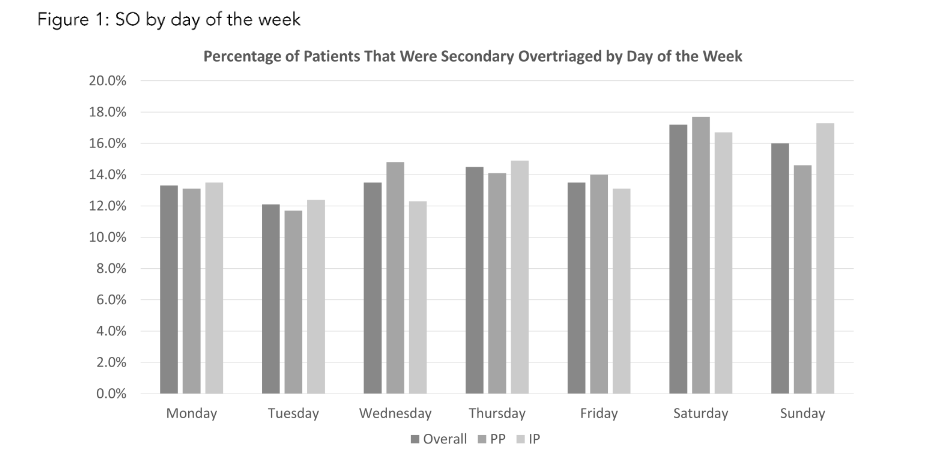
Figure 1: SO by Day of the Week
Finally, we analyzed the incidence of SO by day of the week of transfer. A summary of which is represented in Figure 1. Of note, Saturday (17.2%) and Sunday (16.0%) were the most common days of transfer. A significant difference was found between transfer days of the week between PP and IP (p=0.47).
Discussion
To our knowledge, this is the first study examining rate of SO before and during the COVID-19 Pandemic. The overall rate of SO found in our study (29.1%) falls within the observed rate in previously reported literature (12.2–39%)¹,⁴,⁵,⁷⁻⁹. Despite the shortage of resources and the burden of the COVID-19 pandemic, we found no significant difference in SO rates between the PP (29.7%) and IP (28.7%) groups (p>0.37).
When compared, the PP and IP groups were similar in age, sex, insurance status, and mean distance of transfer. More males than females were transferred overall as well as IP compared to PP. This is consistent with prior studies on SO¹⁷,¹⁸. Unsurprisingly, secondary overtriage was most likely to occur on the weekend, regardless of whether the transfer occurred PP or IP. This is most likely related to decreased resources at the transferring centers on the weekend compared to tertiary centers.
In our population, the most common mechanism of injury remained falls and motor vehicle accidents. The only significant difference in MOI was a decrease in the incident of assault during the pandemic. This is incongruent with recent estimates of domestic violence¹⁹, however, our data collection stopped in 2021 after which the incidence of assault including domestic violence may have increased as the mental toll of the pandemic continued.
While the difference in GCS and ISS were statistically significant, we feel that the clinical difference in these numbers (GCS 14.9 PP and 15 IP and an ISS of 6.0 PP and 6.5 IP) is so small as not to be clinically significant.
Previous studies have found that insurance status affects the likelihood of transfer. Koval et al. found that patients with Medicaid are twice as likely to be transferred to a higher level of care than those with other types of insurance¹⁷. Similarly, another retrospective review by Nathans, et al. found that patients without commercial insurance were 2.4 times more likely to be transferred to a Level I facility than patients with commercial insurance¹⁸. In our population, however, this was not the case.
The majority of our SO patients either had commercial insurance or Medicare while uninsured patients made up the fewest number of transferred patients. This calls into question the idea that there is a financial incentive for referring facilities to unburden themselves of uninsured patients.
In our institution, the most commonly consulted specialties were Speech and Language Pathology, Neurosurgery, Plastic Surgery, and Orthopedic Surgery. The most commonly provided services were, unsurprisingly: laceration repair, cognitive evaluation for concussion, orthopedic splinting, and soft tissue repair, with a statistically significant increase only in orthopedic splinting after the onset of the COVID pandemic. In fact, most other procedures saw a decline after the onset of the pandemic.
These procedures are consistent with previous literature documenting secondary overtriage. This tells us that, in our transfer population, 25% of patients receive no subspecialty consultation and the most commonly performed special procedures was orthopedic splinting—a procedure commonly performed by Emergency Medicine physicians—and cognitive evaluation, which is often safely performed in an outpatient setting. While these procedures and consultations may seem necessary or beyond the scope of practice in a referring facility, it is reasonable to wonder if their necessity requires physical transfer from a patient’s home to accomplish.
During our study, more patients were admitted to our intermediate, or “step down” floors. It is reasonable to ask why more ICU stepdown beds were occupied with patients if they met criteria for overtriage. However, this change in admission location is coupled with a nearly 8% increase in the use of our observation unit and a decrease in floor bed use by over 13%. A likely explanation is not an increase in severity of injury, as all patients met criteria for overtriage, but a redistribution of admission location given the strains of the pandemic over the whole hospital.
We believe this study is an important evaluation of our transfer patterns with regards to and independent of the COVID-19 pandemic. Overall, an average of 2.1 post-transfer CT scans were obtained. The out-of-pocket cost of a CT scan of the abdomen and pelvis with contrast at our institution is $1445, meaning that post-transfer CTs cost about $3,034.50 per every patient in this study²⁰. Based on data from CMS.gov, the average cost for ambulance transportation to our facility, per overtriaged patient, is $661²¹. This estimate is for Medicare patients and likely would be higher for patients with private insurance. In addition to financial cost, patients and their family incur emotional stress that comes with being displaced an average of 46 miles away from their home and community.
Our study is not without limitations. Due to its retrospective nature, this study utilizes data collected during routine clinical care and not original intentional study observations. Thus, the data may have been recorded inconsistently across providers or be incomplete. Also, this was a single institution study only, and thus the results may not be broadly applicable to other regions. Another important limitation of this study is that it cannot take into account the variable experience between providers at referring facilities that influence tests ordered, diagnoses made, and decisions to transfer, independent of the pandemic. We also do not have information about the availability of the subspecialties at the referring institution which also influences the need to transfer. Additionally, we focused our data on procedures and specialty consultations previously described in other literature, thus, while we made our best, most complete attempt to collect all procedures and consultations, there may be other consultations such as Ophthalmology or Hand surgery that were missed.
Conclusion
The COVID-19 Pandemic and insurance status did not affect SO rates at our institution. The results of this study may serve as a basis for development of new guidelines to aid in decision-making to transfer trauma patients to our institution. This in conjunction with potential incorporation of telemedicine and educational outreach to the referring centers may reduce the burden of unnecessary transfers in the future.referring facilities may reduce our SO rates. This paper, however, should also be seen as a tribute to our referring facilities that during a time of significant stress to the entire health care system during a global pandemic, these hospitals did their best to retain the care they normally provide for their communities.
Conflict of Interest
None.
Funding Statement
None.
References
1. Ciesla DJ, Sava JA, Street JH 3rd, Jordan MH. Secondary overtriage: a consequence of an immature trauma system. J Am Coll Surg. 2008;206(1):131-137. Doi:10.1016/j.jamcollsurg.2007.06.285
2. Nathens AB, Maier RV, Copass MK, Jurkovich GJ. Payer status: the unspoken triage criterion. J Trauma. 2001; 50 (5): 776–783.
3. Koval KJ, Tingey CW, Spratt KF. Are patients being transferred to level-I trauma centers for reasons other than medical necessity? J Bone Joint Surg Am. 2006; 88 (10): 2124–213
4. Kappy, N. S., Hazelton, J. P., Capano-Wehrle, L., Gibbs, R., Dalton, M. K., & Ross, S. E. (2019). Financial Impact of Minor Injury Transfers on a Level 1 Trauma Center. The Journal of surgical research, 233, 403–407. https://doi.org/10.1016/j.jss.2018.08.036
5. Tang, A., Hashmi, A., Pandit, V., Joseph, B., Kulvatunyou, N., Vercruysse, G., Zangbar, B., Gries, L., O’Keeffe, T., Green, D., Friese, R., & Rhee, P. (2014). A critical analysis of secondary overtriage to a Level I trauma center. The journal of trauma and acute care surgery, 77(6), 969–973.
6. Sorensen, M. J., von Recklinghausen, F. M., Fulton, G., & Burchard, K. W. (2013). Secondary overtriage: the burden of unnecessary interfacility transfers in a rural trauma system. JAMA surgery, 148(8), 763–768.
7. Lindsey, L. J., Rasmussen, L. S., Hendrickson, L. S., Frech, E. S., Bozell, S. P., Stewart, K. E., Kennedy, R. O., Cross, A., Albrecht, R. M., & Celii, A. M. (2021). Trauma Transfers Discharged from the Emergency Department – Is There a Role for Telemedicine?. The journal of trauma and acute care surgery, 10.1097/TA.0000000000003505. Advance online publication.
8. Moslehi S, Haghdoust Z, Masoumi G, et al. Secondary overtriage of trauma patients in a trauma center: frequency and associated factors. J Inj Violence Res. 2023;15(1):45-54. doi:10.5249/ jivr.v15i1.1701
9. Parikh PP, Parikh P, Mamer L, McCarthy MC, Sakran JV. Association of System-Level Factors With Secondary Overtriage in Trauma Patients. JAMA Surg. 2019;154(1):19-25. doi:10.1001/jama surg.2018.3209
10. Medford-Davis, L. N., Holena, D. N., Karp, D., Kallan, M. J., & Delgado, M. K. (2018). Which transfers can we avoid: Multi-state analysis of factors associated with discharge home without procedure after ED to ED transfer for traumatic injury. The American journal of emergency medicine, 36(5), 797–803.
11. Tripod, M., Tait, M., Bracey, J., Sexton, K., Beck, W., & Wyrick, T. O. (2020). The Use of Telemedicine Decreases Unnecessary Hand Trauma Transfers. Hand (New York, N.Y.), 15(3), 422–427.
12. Ward, M. M., Carter, K. D., Ullrich, F., Merchant, K., Natafgi, N., Zhu, X., Weigel, P., Heppner, S., & Mohr, N. M. (2021). Averted Transfers in Rural Emergency Departments Using Telemedicine: Rates and Costs Across Six Networks. Telemedicine journal and e-health : the official journal of the American Telemedicine Association, 27(5), 481–487.
13. Crowley BM, Griffin RL, Andrew Smedley W, et al. Secondary Overtriage of Trauma Patients: Analysis of Clinical and Geographic Patterns. J Surg Res. 2020;254:286-293. doi:10.1016/j.jss.2020.04.009
14. West CP, Dyrbye LN, Shanafelt TD. Physician burnout: contributors, consequences and solutions. J Intern Med. 2018;283(6):516-529. doi:10.1111/ joim.12752
15. French G, Hulse M, Nguyen D, et al. Impact of Hospital Strain on Excess Deaths During the COVID-19 Pandemic – United States, July 2020-July 2021. MMWR Morb Mortal Wkly Rep. 2021;70(46):1613-1616. Published 2021 Nov 19. doi:10.15585/mmwr.mm7046a5
16. Sheets NW, Fawibe OS, Mahmoud A, Chawla-Kondal B, Ayutyanont N, Plurad DS. Impact of the COVID-19 Pandemic on Trauma Encounters. Am Surg. 2023;89(3):434-439. doi:10.1177/000313482 11029858
17. Koval KJ, Tingey CW, Spratt KF. Are patients being transferred to level-I trauma centers for reasons other than medical necessity?. J Bone Joint Surg Am. 2006;88(10):2124-2132. doi:10.210 6/JBJS.F.0024517
18. Nathens AB, Maier RV, Copass MK, Jurkovich GJ. Payer status: the unspoken triage criterion. J Trauma. 2001;50(5):776-783. doi:10.1097/000053 73-200105000-00002
19. Kourti A, Stavridou A, Panagouli E, et al. Domestic Violence During the COVID-19 Pandemic: A Systematic Review. Trauma Violence Abuse. 2023;24(2):719-745. doi:10.1177/1524838 0211038690
20. Out-of-pocket estimates and pricing | ohiohealth. OhioHealth.com.
21. Ambulance Fee Schedule Public Use Files | CMS. https://www.cms.gov/medicare/payment/fee-schedules/ambulance/ambulance-fee-schedule-public-use-files
22. Bardes, J. M., Grabo, D. J., LaRiccia, A., Spalding, M. C., Warriner, Z. D., Bernard, A. C., Dougherty, M. B. L., Armen, S. B., Hudnall, A., Stout, C., & Wilson, A. (2023). A multicenter evaluation on the impact of non-therapeutic transfer in rural trauma. Injury, 54(1), 238–242. https://doi.org/10.1016/j.injury.2022.07.045
23. Hill, A. D., Fowler, R. A., & Nathens, A. B. (2011). Impact of interhospital transfer on outcomes for trauma patients: a systematic review. The Journal of trauma, 71(6), 1885–1901. https://doi.org/10.1097/TA.0b013e31823ac642
24. Viel, I. L., Moura, B. R. S., Martuchi, S. D., & de Souza Nogueira, L. (2019). Factors Associated With Interhospital Transfer of Trauma Victims. Journal of trauma nursing : the official journal of the Society of Trauma Nurses, 26(5), 257–262. https://doi.org/10.1097/JTN.0000000000000452