






Inclusive Mental Health Services for Key Populations in Thailand
Towards Inclusive Mental Health and Psychosocial Support Services for Key Populations with Higher Risk of HIV Exposure in Thailand
Ravipa Vannakit¹,²,³,⁴; David Clarke¹; Phubet Panphet⁵; Terence Beney⁶; Surang Janyam⁷; Jennifer Ho⁷; Yves Miel Zuniga⁸; Ryan Joseph Figueiredo⁹; Jean-Luc El-Kaim¹⁰; Michael Cassell¹¹; R. Cameron Wolf¹²; Jintanat Ananworanich²,³,⁴
- Bangkok Interdisciplinary Research and Development, Bangkok, Thailand
- Amsterdam Public Health, Amsterdam University Medical Center, University of Amsterdam, Amsterdam, The Netherlands
- Amsterdam Institute for Global Health and Development, Amsterdam, The Netherlands
- Amsterdam Institute for Immunology and Infectious Diseases, Amsterdam, The Netherlands
- Plus Foundation, Chiang Mai, Thailand
- Independent consultant, Pretoria, South Africa
- SWING Foundation, Bangkok, Thailand
- United for Global Mental Health, London, United Kingdom
- Equal Asia Foundation, Bangkok, Thailand
- Expertise France, Paris, France
- FHI 360, North Carolina, United States
- AIDS Action Baltimore, Maryland, United States
OPEN ACCESS
PUBLISHED 30 November 2025
CITATION Vannakit, R., Clarke, D., et al., 2025. Towards Inclusive Mental Health and Psychosocial Support Services for Key Populations with Higher Risk of HIV Exposure in Thailand. Medical Research Archives, [online] 13(11). https://doi.org/10.18103/mra.v13i11.7102
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i11.7102
ISSN 2375-1924
Abstract
Thailand is facing major mental health challenges due to a constellation of factors including rapid socio-economic changes and pressures on vulnerable populations. These cause many Thais to experience stress, anxiety, depression, isolation and suicidal ideation. Mental health is a public health priority; yet, mental health and psycho-social support services (MHPSS) are failing to meet some specific basic needs in mental health promotion, prevention and responsive care. MHPSS efficacy is limited by significant gaps in addressing the mental health needs of four overlapping key populations: LGBTQI+, sex workers, migrant workers and drug users. Adolescents and youth from these are a particular concern. Currently, these key populations are effectively excluded from the National Plan for Mental Health (2018-2037). Because they are at higher risk of HIV exposure, the deficit in MHPSS is detrimental to epidemic control and ending AIDS by 2030.
To better understand the mental health needs of the four abovementioned key populations, we conducted a rapid situation analysis of mental health issues that they experience. We used an analytical framework to investigate the salient factors shaping their mental health in terms of four social domains. These are as follows: i) the family and home; ii) the school; iii) the workplace; and iv) the community. We also conducted a rapid assessment of MHPSS in relation to access and uptake of services by the four key populations. Data were obtained through qualitative research involving key informant interviews enhanced by a literature review of mental health among key populations in Thailand.
The four key populations experience a range of common stressors such as stigma, discrimination, social exclusion, gender-based violence and increased vulnerability to HIV infection. Each population faces a specific combination of stressors across social domains and the life course, with varying mental health outcomes as well as specific barriers to accessing responsive care. Our findings reinforce the need for developing differentiated mental health promotion, prevention and care services for these excluded populations within the national policy framework for mental health. Improving mental health literacy more broadly and countering discrimination against marginalised groups will continue to be indispensable prerequisites for a successful public mental health response.
Keywords
Mental health, psychosocial support, LGBTQI+, sex workers, migrant workers, drug users, HIV, Thailand
Introduction
Mental health is a fundamental human right and increasingly recognised as “a universal human asset, indivisible from other public health priorities”. Mental disorders are the leading cause of sickness, absence and long-term work incapacity in most developed countries. They also co-occur significantly with leading causes of morbidity, such as heart disease, hypertension, diabetes, eating disorders, cancer and HIV, in a pernicious, mutually reinforcing relationship that complicates and further raises the costs of management, treatment and recovery. Mental health programming is clearly indispensable to an effective public health response.
In Thailand, public, private and non-governmental providers deliver MHPSS. In the public sector, institutional responsibility for mental health is distributed across several ministries; however, the Department of Mental Health in the Ministry of Public Health assumes the most prominent operational role, including issuing guidelines for service provision. Although national mental health policy, strategy and planning guarantee services to all in need and provide for promotion, prevention and care, in practice, treatment services predominate. Over 80% of the 2020 mental health budget was spent on psychiatric hospitals and psychotropic medication supply. In contrast, mental health promotion and prevention efforts are severely underfunded and there is no meaningful differentiation of publicly funded mental health promotion, prevention and care for specific populations. This pattern of investments is radically different from the approach prescribed by WHO (See
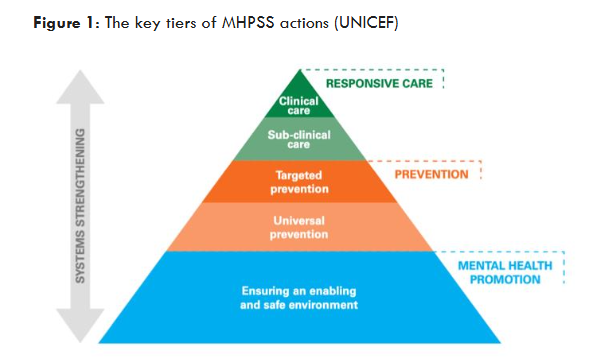
). It is essentially an inversion of the WHO model in which the base of the MHPSS reflecting scale of activity is allotted to mental health promotion followed by prevention with responsive care at the apex of the pyramid. A key challenge for Thailand is to allocate increased resources for effective mental health promotion and prevention interventions for the general population as well as key populations to complement investment in responsive care.
The national HIV epidemic is characterised by concentrated incidence among younger key populations of LGBTQI+, people who use drugs, migrants and sex workers and migrant sex workers who are most vulnerable to HIV, sexually transmitted infections (STIs) and workplace discrimination. These key populations face heightened mental health risks due to a complex interplay of identity-based stigma, discrimination, systemic marginalization and otherization. Individuals, situated at the intersection of overlapping stigmatised identities by belonging to two or more of these key populations, would be subjected to amplified systemic discrimination. Minority stress theory anticipates their chronic psychological duress as they struggle to conceal or own identities defined by discrediting attributes that discount their personhood. Exacerbating their struggle are intersectional social determinants of health such as poverty, unemployment, displacement, gender-based violence and limited access to health and social services, of which they are disproportionately affected.
In 2024, a process was initiated to develop the case for tailored MHPSS for the four key populations at heightened risk of HIV exposure and infection – LGBTQI+, drug users, migrants and sex workers – as well as those who are further marginalised by identities that overlap across these. The evidence informing the case from primary research activity and a synthesis of material from secondary sources is presented in this article. While presented with specific reference to Thailand, we contend that it is relevant wherever distinct minority key populations are at heightened risk of exposure to HIV infection and poor health outcomes.
Methods
Data were collected to assess the mental health needs and demand for MHPSS among four key populations, as well as the availability, accessibility and affordability of services. The study consisted of two components, distinguished by the focus on primary or secondary data, as outlined below.
Qualitative methods
Primary data were obtained through 30 stakeholder key informant interviews in March-June 2024 with systematically identified stakeholders, including mental health service providers and representatives of the key populations of interest. These involved in-depth conversations with individuals selected for their specialized knowledge of mental health and key populations. A set of open-ended questions were developed covering MHPSS implementation investigating current challenges, access and quality of services. Discussion was focused on what needs to happen for key populations to be included in MHPSS policy and service delivery responding to the mental health needs identified in the desk research. The findings from these interviews inform the discussion on MHPSS reform.
This method was used to gain expert insights, understand perspectives and gather descriptive information that was not be available through other means, such as understanding sensitive issues. The interviews were semi-structured, to allow for a more comprehensive and detailed conversation. Field visits were made to community and public health facilities delivering MHPSS in Bangkok, Chiang Mai (northern Thailand), Nakorn Ratchasima (north eastern Thailand), Pattaya (eastern Thailand) and Ranong (southern Thailand).
Participant sampling
Purposive sampling was used. Selection was based on intentional selection of participants with specific characteristics to meet the study objectives i.e their specialized knowledge of mental health and key populations. This method relies on researcher judgment to choose “information-rich” stakeholders that can provide valuable, in-depth data, rather than using random selection. This approach is useful for focusing on a specific group with particular knowledge or experiences.
Data collection and analysis
The key informant interviews were recorded and transcribed verbatim. The data analysis process included organizing and transcribing the data, identifying common themes and summarizing the findings to answer the research questions, using a matrix analysis to ensure consistency. Thematic analysis was used to identify recurring themes, categories and patterns that emerged from the interviews.
Literature review
The secondary data component consisted of a literature review covering published research on key population mental health disorders and their causes. This explored published research on the mental health situation and MHPSS needs of the four key populations. Documents with international, regional and Thai-specific content were all included but prioritised for relevance to the Thai context. Rather than being delimited by a list of prescribed terms, searches were broad but favoured PubMed-, SCOPUS- and Google-referenced academic literature in health, sociology and psychology.
Analytical framework
Data analysis was guided by an ecological interpretive framework that arranged factors shaping mental health into the social contexts in which their influence is exerted, based on the literature review. These are: i) the family and home; ii) the school and education; iii) the workplace; and iv) the community (See
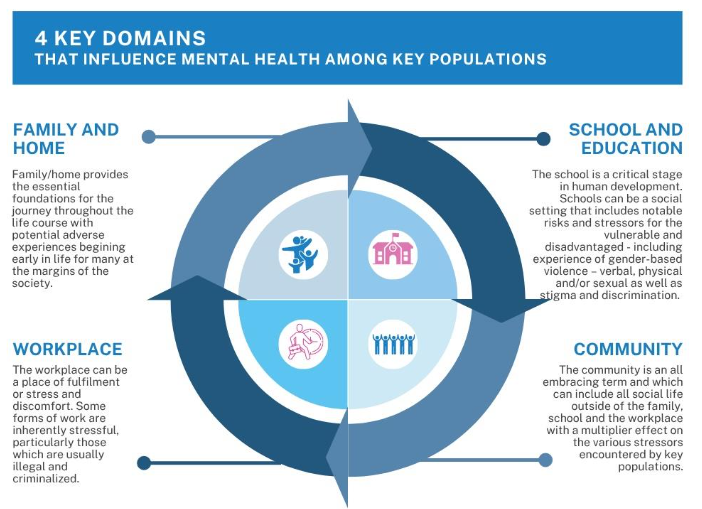
). Our rationale was that this approach better differentiated the mental health profiles of the four sub-populations and increase the value of the study for designing interventions tailored to the realities each key population experiences within each social context.
Results
MHPSS Needs
The four key populations in this study have abundant MHPSS needs. Research consistently demonstrates that the mental well-being of sexual minorities is affected across all social contexts. Drug use is a recurring intersectional feature of migrant, sex worker and LGBTQI+ mental health conditions, complicating the mental health profiles of these key populations. The relationship between physical and mental well-being is mediated by social determinants that favour or hinder positive health outcomes. In the context of HIV, studies consistently demonstrate the significant negative impact of mental health comorbidities on health-seeking behaviours and HIV outcomes, while also revealing intersectional correlations between the severity of mental health conditions and factors such as income, housing stability and social support. Importantly, such mediating factors differ across key populations of people living with HIV. For example, access to treatment and retention in care for HIV positive youth are compromised by forms of discrimination and internalised stigma that differ from those confronting adults and which are exacerbated by LGBTQI+ identities and sexual orientations that diverge from dominant cultural expectations. The lesson from HIV programming is clear: a prerequisite for equitable care and improved mental well-being is responsiveness to the specific needs, experiences and social contexts of the populations being served. When services fail to acknowledge and address the unique constellation of challenges and vulnerabilities experienced by populations of people living with HIV, the care offered is less likely to be appropriate, accessible, or effective.
The interconnectedness of physical health, mental well-being and social determinants is reinforced in the context of substance use disorders (SUDs). According to the National Household Survey on Drug and Alcohol Use in Thailand (2016), an estimated 5.8% of the total population aged 12–65 years have used at least one addictive substance in their lives and 2.8% reported using one or more substances “within the past 12 months”. Individuals abusing substances have an elevated risk of mental illness and often present with co-occurring mental health conditions, necessitating integrated approaches to mental health service delivery. The relationship between substance abuse and mental health is also reciprocal, with substance use exacerbating mental health conditions and vice versa. LGBTQI+ experience mental health conditions at higher rates than their non-minority peers, including higher rates of anxiety, depression, suicidal ideation and attempted suicide. The mental health of young LGBTQI+ (15-24 years) is a concern, with available survey results indicating very high rates of at least mild anxiety and depression and higher rates of severe depression, suicidal ideation and non-suicidal self-harm, when compared to non-minority peers. In a 2018 survey, transgender women reported particularly high rates of attempted suicide (over 20%), followed by non-binary individuals (19.6%) and those identifying as ‘other’ (18.9%).
Mental health stressors can be found in experiences of discrimination and exclusion which are widespread across the family, school, work, healthcare, housing and financial services. Experiences of discrimination and exclusion are mediated by factors such as socio-economic status, with low income linked to higher vulnerability and an increased likelihood of suicidal ideation; and severely exacerbated by traumatic experiences including bullying at school, physical violence, forced sex and sexual assault.
Sex workers suffer from depression, anxiety and post-traumatic stress disorder at rates higher than the general Thai population. Being female, older, unemployed, HIV positive, a survivor of trauma, a habitual drug user and lacking meaningful social support are all characteristics that exacerbate poor sex worker mental health. The threat of incarceration due to criminalisation of sex work is a significant stressor with almost 10% (n=1,511) of a survey of sex workers in 7 provinces reported having been incarcerated in their sex work career. High rates of gender-based violence were also reported (35% of respondents). These experiences contribute to a climate of fear (Vannakit R, Clarke D, et al. unpublished data, 2025).
Increased sexual health risks both exacerbate and are exacerbated by mental health vulnerabilities, particularly for sex workers living with HIV. Depression and anxiety are the most prevalent mental health conditions among people living with HIV. In one study, approximately half of the sampled people living with HIV met diagnostic criteria for one or more mental health disorders because of adapting to life with a chronic condition, experiencing or anticipating stigma and managing life stressors. HIV is also associated with neurocognitive conditions, including dementia and motor disorders. These mental health issues affect not only the well-being and quality of life of individuals, but aggregated, have implications for HIV management and transmission prevention. Over half of sex workers surveyed in a MHPSS needs assessment indicated that mental health (58%) and counselling services (64%) are desperately needed. However, the ubiquitous stigma sex workers encounter in the community and the discrimination they experience in health care settings make them reluctant to seek care. Mental health conditions reinforce the aversion to mainstream health services and further reduce treatment adherence, contributing to higher morbidity and, ultimately, mortality rates.
Migrant workers. Several studies document anxiety, depression and other mental disorders among migrant workers, noting higher prevalence rates compared to the general Thai population. Their compromised mental well-being is linked to several stressors unique to the migrant experience. The acculturative stress of adapting to a new culture, language and social environment aggravates the trauma of their initial displacement and the alienating living conditions they are often forced to endure. This is amplified by the continuous, casual discrimination that widespread stigmatised stereotypes tend to trigger.
People who use drugs have an elevated risk of mental illness and often present with co-occurring mental health conditions. The relationship between substance abuse and mental health is also reciprocal, with substance use exacerbating mental health conditions and vice versa. There is a need to better understand the constellation of mental health stressors that particularly affect the abovementioned key populations through the life course in the family, the school, the workplace and the community. Mental health stressors are encountered differently by each key population.
The Family
For adolescent LGBTQI+, family relationships can produce significant mental health stressors. In the family, these include a lack of parental and sibling understanding and acceptance, pressure for filial duty and traditional gender norms, lack of opportunity for disclosure, discrimination and violence and experience of tolerance accompanied by exclusion. People who use drugs face multiple mental health stressors involving the family, including weak family and social support, severe social stigma and economic vulnerability. These factors create a cycle of mental distress that can both lead to and be worsened by substance use. Poor family relationships are a consistent finding in studies on the mental health of substance users in Thai rehabilitation centres. Lack of communication and visits from family members is significantly associated with mental distress. Family relationships and school participation do not appear as significant mental health stressor environments for sex workers or migrant workers. Research is, however, very limited in this regard. Family conflict, parental attitudes towards drugs, drug use by family members and easy access to illicit drugs in the family context are all predictors of drug use. Adverse childhood experiences, including those that are family-situated, have also been linked to the initiation of substance use. During adolescence, when substance misuse typically presents, susceptibility to addiction increases to the extent that substance abuse is common within peer groups in educational settings or workplaces. Low drug literacy is also considered a contributing factor to this vulnerability.
For migrant workers, a notable stressor is the financial demand of providing for their accompanying family, including paying for social services, to which access may be restricted due to their migrant status. Migrants may also be responsible for supporting family members still residing in their home country, who depend on remittances. In a study of undocumented migrant workers from Myanmar, mental health conditions were found to be worse among single children supporting elderly parents through remittances. Family back home is not just a source of stress, however. Social support is a crucial buffer ameliorating migrants’ mental burdens and family in the home country is often a source of comfort. While communicating with family back home is an important coping mechanism, fellow migrants are typically the primary source of tangible and emotional social support.
The School
In school, LGBTQI+ experience mental health stressors that include bullying, discrimination, verbal harassment and stigma as a result of their identity being recognized by their peers. These are compounded by factors such as low self-esteem and a lack of family or sibling support. Some students also experience a fear of rejection and feel the need to conceal their identity. Transgender females face unique challenges related to school dress codes.
The Workplace
In the workplace, mental health stressors are experienced by all four key populations. Minority stress is the main mental health stressor for LGBTQI+ individuals in the workplace, encompassing stigma, direct discrimination and the fear of prejudice. LGBTQI+ individuals are frequently confronted with discriminatory practices that exclude their participation, limit their opportunities, victimise or endanger them. Key workplace stressors for LGBTQI+ employees include harassment, refusal to promote and restrictive dress codes. Acts like unfair firing, harassment, or denial of opportunities are still experienced by many LGBTQI+ workers despite legal protections. There is subtle discrimination and microaggressions which can include offensive jokes, exclusionary “banter,” or invalidating comments. Transgender and gender-diverse individuals face exceptionally high levels of discrimination, including misgendering (using the wrong pronouns or former name), harassment and exclusion. Many LGBTQI+ employees lack confidence that harassment or bullying claims will be handled effectively by management. Discrimination can come from clients, customers and contractors not just colleagues. Many LGBTQI+ employees, particularly those in less accepting environments, conceal their identity to avoid prejudice, which can be immensely mentally draining. Expending energy to hide a core part of one’s identity can lead to social isolation, loneliness and psychological distress. Employees risk having their sexual orientation or gender identity disclosed without their consent, which can damage their psychological safety. Sex work is hazardous, marked by heightened risk of sexually transmitted diseases, violence, abuse and harassment from clients and others in the workplace. The illegal and stigmatized nature of sex work in Thailand creates numerous mental health stressors for workers, which also increase their vulnerability to violence, economic instability and social exclusion. Sex workers face high rates of violence from clients, police and even intimate partners. Many workers experience exploitative conditions, including low autonomy, pressure to perform unsafe sexual acts and long hours without paid leave. The fear of being criminally charged for their work prevents many sex workers from reporting violence to the police, leaving them with little to no legal recourse or protection. The fears of exposure, public shaming and arrest are compounded for those with intersecting LGBTQI+ or migrant identities. Migrant sex workers, already subject to the additional stressors of acculturation, report fearing deportation due to the criminalisation of sex work and their insecure legal status.
Key mental health stressors for migrant workers include exploitation, low wages and poor conditions, job insecurity, discrimination, cultural and language barriers, limited access to social support and healthcare and fears related to legal status. These factors can lead to a higher prevalence of mental health problems such as depression, anxiety and psychological distress compared to the general population. Migrant women in domestic or service jobs are vulnerable to abuse, harassment and discrimination from supervisors and employers. Migrant workers often face prejudice and xenophobia. Acculturative friction is amplified by the continuous, casual discrimination that widespread stigmatised stereotypes tend to trigger. Due to discriminatory treatment, many migrants adopt a “separation” strategy, isolating themselves from the host community. Many migrants have limited Thai language proficiency, which creates challenges in communicating with healthcare providers, accessing important information and navigating daily life. The stress of adapting to a new culture can be a major mental health risk. This is often compounded by homesickness, cultural differences in the workplace and perceived discrimination. A lack of understanding of Thai laws and policies can prevent migrants from accessing health benefits and other entitlements, especially under the Social Security Scheme.
The Community
There appears to be limited research into the community dimensions of mental health. The effects seem to be particularly strong in relation to people who use drugs. In rural and remote communities, drug abuse can lead to community distress, fighting and theft, which further isolates people who use drugs and weakens community bonds. Studies in northern Thailand have noted a lack of leadership and community skills to manage substance abuse issues, leaving families without adequate support. Thailand’s history of punitive drug policies, which have included compulsory treatment in rehabilitation centres, creates significant mental health challenges. Research indicates that the strict, controlled nature of this treatment is associated with a higher rate of abnormal mental health among participants.
Discussion
The need
All stakeholders including community-based organisations, UN Agencies and bi-lateral agencies consulted recognise that mental health issues are rising in prevalence and are increasingly prominent in key population programming. The various mental health stressors and conditions are reasonably well researched and mapped for the four key populations in this study. However, there is a greater quantity of research involving LGBTQI+ than sex workers, for example and there remains a need for further research with these and people who use drugs. The prime focus needs to be on research that can inform delivery of MHPSS. Better understandings are needed of key populations.
Lack of policy and strategy
Stakeholders identified the lack of a clearly defined MHPSS policy and strategy for key populations as constituting a significant barrier to the delivery of appropriate services provision. MHPSS is currently designed for the general population. Specific entitlements and mechanisms for key populations are missing in Thailand’s National Strategy (2018–2037) which includes a mental health component focused on enhancing the well-being of the Thai population by promoting mental health knowledge, preventing mental health risk factors, creating supportive environments and developing public health systems. This puts at risk, not only the wellbeing of these vulnerable and marginalized populations, but also the reputation of national mental health services. A direct consequence of the policy gap is the lack of specific systems and programming to meet the special mental health needs of the range of key populations including where they need support. These have not yet been adequately assessed and therefore interventions to address needs have not yet been designed or appropriately resourced. As a result, key populations are excluded and do not have meaningful access to MHPSS. There is a need to develop policy and programming that covers mental health promotion, prevention as well as responsive care.
Need for key population-tailored MHPSS
There was stakeholder consensus that key population-tailored MHPSS should be developed across various settings, including general hospitals, primary health care facilities and community-based organisations. Key population stakeholders from diverse backgrounds and experiences should be involved in the design, implementation and evaluation of MHPSS interventions. These include those with lived experience of mental ill-health, or experience of supporting peers with mental ill-health. Medical staff should receive training on the specific needs of key populations, including sensitivity training. Expanding inclusive clinics and addressing rural infrastructure challenges is essential, alongside exploring task-shifting approaches and improving coordination with community service providers. A strategic approach will be needed to respond to the MHPSS needs and mental health stressors experienced by the four key populations as identified in the results section.
MHPSS mental health promotion needs investment to promote a safer society for better mental wellbeing of key populations. Key population-focused strategic frameworks should be developed to enhance safe environments in families, schools, workplaces and communities. This includes programmes to promote mental health literacy, increase awareness of stigma and discrimination and develop specific mental health education packages tailored to the need of each key population. Advocacy programmes are needed to improve workplace safety, addressing gender diversity, equality, inclusion, gender-based violence, stigma and discrimination.
Prevention programming for key populations
Prevention programming for key populations needs to focus on gender-based violence, stigmatization and discrimination in relation to all four key populations in this study. Mental health conditions are stigmatized. Social stigma can limit the provision and uptake of HIV services for prevention, treatment and care. It typically supports discrimination and can interact with other forms of stigmatization of social identities such as gender and sexual orientation. Consideration should be given to decriminalizing sex work. The criminalization of sex work and drug use has an additional stigmatizing effect that creates significant barriers to HIV prevention and care service delivery.
HIV and MHPSS
HIV should be integrated as a cross-cutting issue in MHPSS. Exposure to HIV infection among key populations is increasingly understood to be linked with mental health issues. This is particularly relevant to sex workers and people who use drugs, populations with recognized HIV needs across the cascade. Mental health programming is now being introduced into HIV programming. The challenge now is to include HIV in MHPSS policy and planning.
Critical role of community-based organisations
The community-based organisations consulted reported that they are not adequately equipped to provide comprehensive MHPSS and are just beginning to initiate mental health capacity building in their organisations. Some public health infrastructure is in place to provide MHPSS in urban settings. Rural settings, however, face significant challenges in delivering MHPSS for everyone in need. The only LGBTQI+ specific services currently provided in hospital facilities are mental health screening for transgender women with certification for good mental health to be used for military conscription purposes. Investments are needed to build the role and capacity of community-based organisations to assist MHPSS delivery for key populations. Although community-based organisations working with and for key populations have an abundance of expertise, this needs further strengthening in relation to scaling up mental health promotion, prevention and responsive care. Efforts need to be made to enhance the active participation of concerned key population communities for better mental health. Community-based organisations can be tasked with disseminating information on mental health and facilitating access to services. Increasing mental health awareness is important as well as interventions aimed at reducing stigma and discrimination in general and specifically regarding MHPSS. Stigma reduction in the community is also urgently needed, working with families, community leaders and developing linkages/referral support.
The mental health care providers consulted greatly recognised the need to work with community-based organisations that are currently providing services to key populations. A critical role will be to provide information to key populations for mental health promotion, screening and linking those in need to the health facilities for clinical care. More resources are urgently needed. The state of mental health financing in Thailand is currently at a low level. The most recent figure available is 2.3% of government health spending, reported for the year 2020. This needs to be increased to meet the needs of currently excluded key populations.
Capacity building
Capacity needs to be built to enable MHPSS programming for the four key populations. There is a scarcity of professional staff for MHPSS in general. In the South, the shortage of trained staff is particularly acute. The professional staff that are available are not adequately trained to address the specific needs of the four key populations in this paper and their emerging mental health needs. Key informant interviews revealed a demand among mental health professionals for improved knowledge of key population mental health issues, better data, guidance and specific training on how to provide services to key populations, particularly LGBTQI+. There is some professional infrastructure in place to provide services to people who use drugs, which can be expanded.
Monitoring and evaluation (M&E)
Stakeholders raised the issue of M&E and the lack of data with regard to MHPSS for key populations. Problems of misreporting, underreporting and a lack of understanding of the need for data and data quality at the community level are reported by community-based organisations and health care providers. There is a lack of understanding of LGBTQI+ population level data and a lack of ability to disaggregate data. It is, therefore, critically important to enhance strategic information systems to improve the national MHPSS programme M&E framework to include key populations. This will need to include selection of indicators, appropriate data capture methods and data disaggregation specific to key populations.
Stigma and discrimination
Stakeholders commented on the pervasive negative effects of stigma and discrimination that affect each of the four key populations. It will be important to identify effective interventions that can reduce stigma against key populations and people with mental health disorders. This should include support for the family, schools, workplaces and communities to enhance their knowledge and skills for identifying risks and providing support. Workplace policies and programmes should integrate mental health into occupational safety and health, with training for employers and peers to detect mental health issues and provide peer support.
Awareness raising
The issue of lack of awareness of mental health and service provision among the general population was raised in several key informant interviews. This also applies to each of the key populations in this study. There is a need to improve mental health literacy within the key populations, focusing on risk factors, stressors and access to MHPSS. The participation of key populations and community-based organisations needs to be enhanced in mental health promotion and stigma reduction, along with strengthening access to counselling services, including peer support systems and helplines.
Conclusions
Ensuring meaningful access to MHPSS of the 4 key population groups will require a strategic approach involving both demand and supply side interventions. Increasing demand for services will require the development of key-population friendly services, demand generation activities and the active participation of key population representatives at all stages. On the supply side, further reform of MHPSS is needed to accelerate the transition of service delivery to community health facilities, invest in capacity building of staff and improved monitoring of service delivery. A better balance of investments is needed for key populations to support mental health promotion, mental health disorder prevention strategies as well as responsive care provision.
There is considerable enthusiasm among the mental health facilities to develop MHPSS for key populations. All stakeholders are keen to advance MHPSS for populations that are not currently catered for. While MHPSS have long been established in Thailand and largely available in formal health settings, there is an urgent need to bring in reforms that address the exclusion of key populations and move more towards effective delivery of community-based services. There is existing capacity, skills and systems in place that can be expanded and oriented to better meet key population needs. Increased investment is needed in mental health promotion and prevention with the general population and key populations in particular. There is a need to develop participatory situation-response analyses for MHPSS with each key population in this study. This study has identified a set of common mental health issues, but these need to be validated with key population representatives for each group. On the basis of validated findings, differentiated MHPSS strategies should be developed with and for each key population within the policy framework set by the National Mental Health Plan 2018-2037. These strategies should include i) mental health promotion, ii) prevention and iii) affordable, quality, responsive care, implemented within the appropriate social contexts.
Authors’ contributions
Conceptualization, methodology and project administration, R.S.F., J.L.K., D.C. and R.V.; data collection and analysis, R.V., P.P., D.C. and S.R.; writing of the manuscript R.V., D.C. and T.B.; review & editing; S.J., J.H., Y.M.Z., R.S.F., J.L.K., M.C., C.W. and J.A.; All authors have read and agreed to the published version of the manuscript.
Acknowledgements
The funding support from L’Initiative, through Expertise France, together with technical assistance from Equal Asia Foundation and Mplus Foundation made it possible to interview key stakeholders in Thailand and across Asia. Their guidance was critically important for this publication, which aims to support the development of a roadmap for more inclusive mental health and psychosocial support services for underserved populations with a higher risk of HIV exposure in Thailand.
The data analysis was complemented by the GILEAD-funded survey designed to investigate the factors influencing decision-making on Pre-Exposure Prophylaxis (PrEP) use among sex workers in Thailand. This included data on factors affecting mental health of sex workers.
We are deeply indebted to key stakeholders in Thailand and the Asia region who participated in key informant interviews from the Department of Mental Health, Ministry of Public Health; Thanyarak Chiangmai hospital; Suan Prung Psychiatric Hospital; and Nakhon Ratchasima Rajanagarindra Psychiatric Hospital.
We also thank participating non-governmental organisations and community-based organisations for their invaluable contributions. These included Caremat, HON, Sisters, Tangerine Clinic/Institute of HIV Research and Innovation, Thai Drug Users Network, World Vision; regional organisations including APCOM, the Asia Pacific Network of People Living with HIV (APN+), the Centre for Supporting Community Development Initiatives, International Drug Policy Consortium and development partners: UNAIDS Thailand, UNDP Thailand and the Regional Hub.
Funding
The MHPSS study was funded by L’Initiative, through Expertise France while the PrEP study was funded by Gilead Sciences, Inc. The findings and conclusions in this report are those of the authors and do not necessarily represent the views of L’Initiative or Gilead Sciences, Inc. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing interests
The authors declare no conflict of interest.
References
- Remien RH, Patel V, Chibanda D, Abas MA. Integrating mental health into HIV prevention and care: a call to action. J Int AIDS Soc. 2021 Jun;24(S2):e25748.
- Harvey SB, Modini M, Joyce S, Milligan-Saville JS, Tan L, Mykletun A, et al. Can work make you mentally ill? A systematic meta-review of work-related risk factors for common mental health problems. Occup Environ Med. 2017 Apr;74(4):301–10.
- Collins PY, Velloza J, Concepcion T, Oseso L, Chwastiak L, Kemp CG, et al. Intervening for HIV prevention and mental health: a review of global literature. J Int AIDS Soc. 2021 Jun;24(S2):e25710.
- O’Grady T, Inman N, Younger A, Huang B, Bouton TO, Kim H, et al. The Characteristics and HIV-Related Outcomes of People Living with Co-occurring HIV and Mental Health Conditions in the United States: A Systematic Review of Literature from 2016 to 2021. AIDS Behav. 2024 Jan;28(1):201–24.
- World Mental Health Report: Transforming Mental Health for All. 1st ed. Geneva: World Health Organization; 2022. 1 p.
- Ojanen T, Freeman C, Sopitarchasak S, Suparak P. Mental Health and Well-being of Children and Youth with Diverse SOGIESC in Thailand. Save the Children; 2023.
- Mental Health Atlas 2020. 1st ed. Geneva: World Health Organization; 2021. 1 p.
- Thai National AIDS Program Review 2022. Thai Ministry of Public Health; 2022.
- Pamoso AHG, Rasmussen ML, Sutarsa IN, Scholz B. The whole is greater than the sum of its parts: Integrating syndemics and intersectionality in tackling the HIV and mental health epidemics among Filipino gay and bisexual men. Montague-Cardoso K, editor. PLOS Ment Health. 2025 Feb 7;2(2):e0000252.
- Goffman E. Stigma notes on the management of spoiled identity. London: Penguin Books; 1990. (Penguin psychology).
- Sherman ADF, Higgins MK, Balthazar MS, Hill M, Klepper M, Schneider JS, et al. Stigma, social and structural vulnerability, and mental health among transgender women: A partial least square path modeling analysis. J of Nursing Scholarship. 2024 Jan;56(1):42–59.
- Adelson SL, Stroeh OM, Ng YKW. Development and Mental Health of Lesbian, Gay, Bisexual, or Transgender Youth in Pediatric Practice. Pediatric Clinics of North America. 2016 Dec;63(6):971–83.
- Meyer IH, Frost DM. Minority stress and the health of sexual minorities. In: Handbook of psychology and sexual orientation. Oxford University Press; 2013. p. 252–66.
- Shuper PA, Joharchi N, Bogoch II, Loutfy M, Crouzat F, El-Helou P, et al. Alcohol consumption, substance use, and depression in relation to HIV Pre-Exposure Prophylaxis (PrEP) nonadherence among gay, bisexual, and other men-who-have-sex-with-men. BMC Public Health. 2020 Dec;20(1):1782.
- Jaichuang S, Ratanasiri A, Kanato M. Substance abuse among migrant workers of Thai-Laos border, Thailand. J Med Assoc Thai. 2012 Sep;95(9):1219–24.
- Kirmayer LJ, Narasiah L, Munoz M, Rashid M, Ryder AG, Guzder J, et al. Common mental health problems in immigrants and refugees: general approach in primary care. Canadian Medical Association Journal. 2011 Sep 6;183(12):E959–67.
- Bhana A, Kreniske P, Pather A, Abas MA, Mellins CA. Interventions to address the mental health of adolescents and young adults living with or affected by HIV: state of the evidence. J Int AIDS Soc. 2021 Jun;24(S2):e25713.
- Newman PA, Prabhu SM, Akkakanjanasupar P, Tepjan S. HIV and mental health among young people in low-resource contexts in Southeast Asia: A qualitative investigation. Global Public Health. 2022 Jul 3;17(7):1200–14.
- Poteat TC, Keatley J, Wilcher R, Schwenke C. HIV epidemics among transgender populations: the importance of a trans-inclusive response. Journal of the International AIDS Society. 2016 Jul;19:21259.
- Fukunaga R, Pierre P, Williams JK, Briceno-Robaugh R, Kalibala S, Peterson M, et al. Prioritizing Mental Health within HIV and Tuberculosis Services in PEPFAR. Emerg Infect Dis [Internet]. 2024 Apr [cited 2025 Apr 11];30(4). Available from: https://wwwnc.cdc.gov/eid/article/30/4/23-1726_article
- Saingam D. Substance Abuse Policy in Thailand: Current Challenges and Future Strategies. J Drug Alcohol Res. 2018;7:1–10.
- Vannakit R. Mental Health and Psychological Support Services (MPHSS) for LGBTQI+, sex workers, people who use drugs, and migrant workers in Thailand. Expertise France, Equal Asia Foundation, Bangkok Interdisciplinary Research and Development; 2024.
- Desai R, Karim S, Freeborn J, Trivedi C, Husain K, Jain S. Contextualizing the Relationship Between Social Isolation and Substance Abuse. Prim Care Companion CNS Disord. 2024 Sep 24;26(5):23m03679.
- Shuper PA, Joharchi N, Bogoch II, Loutfy M, Crouzat F, El-Helou P, et al. Alcohol consumption, substance use, and depression in relation to HIV Pre-Exposure Prophylaxis (PrEP) nonadherence among gay, bisexual, and other men-who-have-sex-with-men. BMC Public Health. 2020 Dec;20(1):1782.
- Spencer L, Alderson H, Scott S, Kaner E, Ling J. ‘The Addiction Was Making Things Harder for My Mental Health’: A Qualitative Exploration of the Views of Adults and Adolescents Accessing a Substance Misuse Treatment Service. IJERPH. 2023 May 26;20(11):5967.
- Ojanen TT. Sexual/gender minorities in Thailand: Identities, challenges, and voluntary-sector counseling. Sexuality Research & Social Policy. 2009 Jun 1;6(2):4–34.
- Sopitarchasak S, Kihara M, Min Soe K, Ono-Kihara M. Disparities in Mental Well-being between Non-Minority and Sexual Minority Male Youth in Bangkok, Thailand: Quantitative Findings from a Mixed Method Study. JPSS. 2017 Apr 1;25(2):83–98.
- Hatzenbuehler ML, Lattanner MR, McKetta S, Pachankis JE. Structural stigma and LGBTQ+ health: a narrative review of quantitative studies. The Lancet Public Health. 2024 Feb;9(2):e109–27.
- Meyer IH. Prejudice, Social Stress, and Mental Health in Lesbian, Gay, and Bisexual Populations: Conceptual Issues and Research Evidence. 2007;
- Van Griensven F, Kilmarx PH, Jeeyapant S, Manopaiboon C, Korattana S, Jenkins RA, et al. The Prevalence of Bisexual and Homosexual Orientation and Related Health Risks Among Adolescents in Northern Thailand. Arch Sex Behav. 2004 Apr;33(2):137–47.
- UNDP. Tolerance But Not Inclusion: A national survey on experiences of discrimination and social attitudes towards LGBT people in Thailand. UNDP; 2019.
- Suriyasarn B. Gender identity and sexual orientation in Thailand. Bangkok: ILO; 2014.
- Parent MC, DeBlaere C, Moradi B. Approaches to Research on Intersectionality: Perspectives on Gender, LGBT, and Racial/Ethnic Identities. Sex Roles. 2013 Jun;68(11–12):639–45.
- Boonmongkon P, Ojanen T, Ratchadapunnathikul C, Samoh N, Damri T, Mudjalin C, et al. Bullying targeting secondary school students who are or are perceived to be transgender or same-sex attracted: types, prevalence, impact, motivation and preventive measures in 5 provinces of Thailand; 2014. Mahidol University, Plan International, UNESCO; 2014.
- Kaltiala-Heino R, Rimpelä M, Rantanen P, Rimpelä A. Bullying at school—an indicator of adolescents at risk for mental disorders. Journal of Adolescence. 2000 Dec;23(6):661–74.
- Beattie TS, Smilenova B, Krishnaratne S, Mazzuca A. Mental health problems among female sex workers in low-and middle-income countries: A systematic review and meta-analysis. PLoS Med. 2020 Sep;17(9):e1003297.
- Martín-Romo L, Sanmartín FJ, Velasco J. Invisible and stigmatized: A systematic review of mental health and risk factors among sex workers. Acta Psychiatr Scand. 2023 Sep;148(3):255–64.
- Somwaeng A, Pramualratana K, Sumalu S. Need assessment for mental health services among sex workers in Bangkok and Pattaya. SWING Foundation; 2024.
- Kinyanda E, Hoskins S, Nakku J, Nawaz S, Patel V. Prevalence and risk factors of major depressive disorder in HIV/AIDS as seen in semi-urban Entebbe district, Uganda. BMC Psychiatry. 2011 Dec 30;11:205.
- Waldron EM, Burnett-Zeigler I, Wee V, Ng YW, Koenig LJ, Pederson AB, et al. Mental Health in Women Living With HIV: The Unique and Unmet Needs. J Int Assoc Provid AIDS Care. 2021;20:2325958220985665.
- Chibanda D, Benjamin L, Weiss HA, Abas M. Mental, neurological, and substance use disorders in people living with HIV/AIDS in low- and middle-income countries. J Acquir Immune Defic Syndr. 2014 Sep 1;67 Suppl 1:S54-67.
- Todd JV, Cole SR, Pence BW, Lesko CR, Bacchetti P, Cohen MH, et al. Effects of Antiretroviral Therapy and Depressive Symptoms on All-Cause Mortality Among HIV-Infected Women. Am J Epidemiol. 2017 May 15;185(10):869–78.
- Kesornsri S, Sitthimongkol Y, Hegadoren KM. Mental Health Problems among Migrant Workers: Challenges for Nurses in Thailand. 2014;32(3).
- Aung TNN, Shirayama Y, Moolphate S, Lorga T, Angkurawaranon C, Yuasa M, et al. Prevalence and social determinants of depression: A cross-sectional survey of Myanmar migrant workers in Chiang Mai, Northern Thailand. Global Public Health. 2024 Dec 31;19(1):2334316.
- Hasan SI, Yee A, Rinaldi A, Azham AA, Mohd Hairi F, Amer Nordin AS. Prevalence of common mental health issues among migrant workers: A systematic review and meta-analysis. PLoS One. 2021;16(12):e0260221.
- Desai R, Karim S, Freeborn J, Trivedi C, Husain K, Jain S. Contextualizing the Relationship Between Social Isolation and Substance Abuse. Prim Care Companion CNS Disord. 2024 Sep 24;26(5):23m03679.
- Spencer L, Alderson H, Scott S, Kaner E, Ling J. ‘The Addiction Was Making Things Harder for My Mental Health’: A Qualitative Exploration of the Views of Adults and Adolescents Accessing a Substance Misuse Treatment Service. IJERPH. 2023 May 26;20(11):5967.
- Ojanen TT. Sexual/gender minorities in Thailand: Identities, challenges, and voluntary-sector counseling. Sexuality Research & Social Policy. 2009 Jun 1;6(2):4–34.
- Sopitarchasak S, Kihara M, Min Soe K, Ono-Kihara M. Disparities in Mental Well-being between Non-Minority and Sexual Minority Male Youth in Bangkok, Thailand: Quantitative Findings from a Mixed Method Study. JPSS. 2017 Apr 1;25(2):83–98.
- Hatzenbuehler ML, Lattanner MR, McKetta S, Pachankis JE. Structural stigma and LGBTQ+ health: a narrative review of quantitative studies. The Lancet Public Health. 2024 Feb;9(2):e109–27.
- Meyer IH. Prejudice, Social Stress, and Mental Health in Lesbian, Gay, and Bisexual Populations: Conceptual Issues and Research Evidence. 2007;
- Van Griensven F, Kilmarx PH, Jeeyapant S, Manopaiboon C, Korattana S, Jenkins RA, et al. The Prevalence of Bisexual and Homosexual Orientation and Related Health Risks Among Adolescents in Northern Thailand. Arch Sex Behav. 2004 Apr;33(2):137–47.
- UNDP. Tolerance But Not Inclusion: A national survey on experiences of discrimination and social attitudes towards LGBT people in Thailand. UNDP; 2019.
- Suriyasarn B. Gender identity and sexual orientation in Thailand. Bangkok: ILO; 2014.
- Parent MC, DeBlaere C, Moradi B. Approaches to Research on Intersectionality: Perspectives on Gender, LGBT, and Racial/Ethnic Identities. Sex Roles. 2013 Jun;68(11–12):639–45.
- Boonmongkon P, Ojanen T, Ratchadapunnathikul C, Samoh N, Damri T, Mudjalin C, et al. Bullying targeting secondary school students who are or are perceived to be transgender or same-sex attracted: types, prevalence, impact, motivation and preventive measures in 5 provinces of Thailand; 2014. Mahidol University, Plan International, UNESCO; 2014.
- Kaltiala-Heino R, Rimpelä M, Rantanen P, Rimpelä A. Bullying at school—an indicator of adolescents at risk for mental disorders. Journal of Adolescence. 2000 Dec;23(6):661–74.
- Beattie TS, Smilenova B, Krishnaratne S, Mazzuca A. Mental health problems among female sex workers in low-and middle-income countries: A systematic review and meta-analysis. PLoS Med. 2020 Sep;17(9):e1003297.
- Martín-Romo L, Sanmartín FJ, Velasco J. Invisible and stigmatized: A systematic review of mental health and risk factors among sex workers. Acta Psychiatr Scand. 2023 Sep;148(3):255–64.
- Somwaeng A, Pramualratana K, Sumalu S. Need assessment for mental health services among sex workers in Bangkok and Pattaya. SWING Foundation; 2024.
- Kinyanda E, Hoskins S, Nakku J, Nawaz S, Patel V. Prevalence and risk factors of major depressive disorder in HIV/AIDS as seen in semi-urban Entebbe district, Uganda. BMC Psychiatry. 2011 Dec 30;11:205.
- Waldron EM, Burnett-Zeigler I, Wee V, Ng YW, Koenig LJ, Pederson AB, et al. Mental Health in Women Living With HIV: The Unique and Unmet Needs. J Int Assoc Provid AIDS Care. 2021;20:2325958220985665.
- Chibanda D, Benjamin L, Weiss HA, Abas M. Mental, neurological, and substance use disorders in people living with HIV/AIDS in low- and middle-income countries. J Acquir Immune Defic Syndr. 2014 Sep 1;67 Suppl 1:S54-67.
- Todd JV, Cole SR, Pence BW, Lesko CR, Bacchetti P, Cohen MH, et al. Effects of Antiretroviral Therapy and Depressive Symptoms on All-Cause Mortality Among HIV-Infected Women. Am J Epidemiol. 2017 May 15;185(10):869–78.
- Kesornsri S, Sitthimongkol Y, Hegadoren KM. Mental Health Problems among Migrant Workers: Challenges for Nurses in Thailand. 2014;32(3).
- Aung TNN, Shirayama Y, Moolphate S, Lorga T, Angkurawaranon C, Yuasa M, et al. Prevalence and social determinants of depression: A cross-sectional survey of Myanmar migrant workers in Chiang Mai, Northern Thailand. Global Public Health. 2024 Dec 31;19(1):2334316.
- Hasan SI, Yee A, Rinaldi A, Azham AA, Mohd Hairi F, Amer Nordin AS. Prevalence of common mental health issues among migrant workers: A systematic review and meta-analysis. PLoS One. 2021;16(12):e0260221.