

Indirect Signs of Portal Hypertension in Liver Casts
Indirect Signs of Portal Hypertension in Resin Casts of Cirrhotic Human Livers
Vasconcelos-Filho JOM, MD, MS, PhD
- Prof of Vascular Surgery, and Bases of Surgical Technique Pernambuco University (UPE), Brazil
OPEN ACCESS
PUBLISHED: 30 April 2025
CITATION: Vasconcelos-Filho, JOM., 2025. Indirect Signs of Portal Hypertension in Resin Casts of Cirrhotic Human Livers. Medical Research Archives, [online] 13(4). https://doi.org/10.18103/mra.v13i4.6486
COPYRIGHT: This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i4.6486
ISSN 2375-1924
Abstract
Fourteen resin liver casts obtained from patients with advanced cirrhosis who underwent liver transplantation were evaluated. The findings were compared with a cast obtained from a case without cirrhosis and without portal hypertension. The most common alteration was dissociation between the two venous beds, existing in a variable degree in all casts, in a diffuse or focal manner, in some cases, associated with thrombosis of one or more intrahepatic branches of the portal vein. Other signs suggestive of portal hypertension were also found, such as dilated intrahepatic branches of the portal vein, corkscrew-shaped venules, close to the surface of the liver and dilated venous collaterals, which originally communicated with a systemic vein. The author considers the resin casts a good research resource, able to complement data from pathology and modern imaging studies.
Keywords: portal hypertension, resin casts, cirrhosis, liver transplantation, venous anatomy
Introduction
Vascular casts have been used in anatomical studies of various organs, including the liver. Despite this, there are not many studies on the influence of portal hypertension on intrahepatic venous anatomy, using this model. The aim of this article is to present what we consider to be indirect signs of portal hypertension, found in these models.
Material And Methods
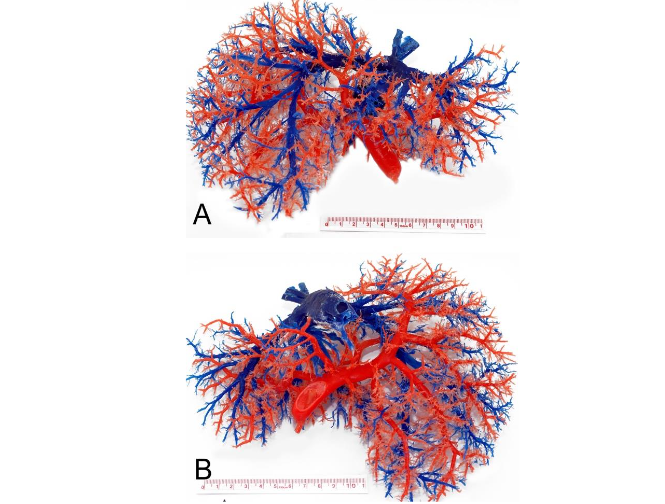
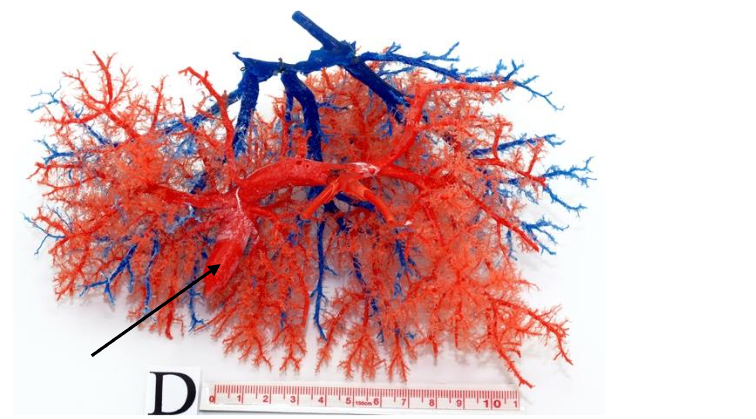
Fourteen cases of patients with liver cirrhosis and clinical or radiological signs of portal hypertension who underwent liver transplantation, during the year March/2013-March/2014, after signing an Informed Consent Form, were studied. The study was carried out at the University of Pernambuco/Brazil authorized by the Research Ethics Committee (Universidade de Pernambuco – UPE, Brazil). Cases of neoplasia (Hepatocellular Carcinoma – HCC) and history of B hepatitis (frequently associated with HCC in our country) were excluded from the study, as well as cases of biliary cirrhosis. The method of preparing the resin casts has been previously described. The findings were compared with a mold obtained from a case without cirrhosis and without portal hypertension (Fig. 1). The diameter of the intrahepatic branches of the portal vein was compared with literature data obtained from normal livers.
Results
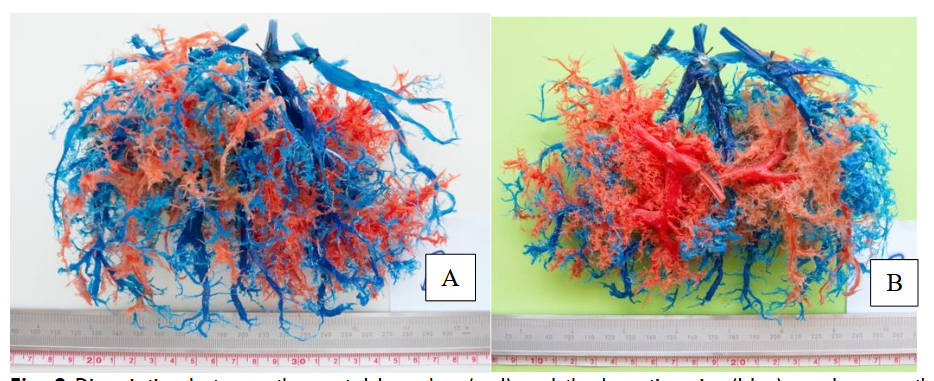
The characteristics of the patients studied are summarized in Table 1. All the casts presented some degree of “dissociation” between the portal bed and the hepatic veins, suggestive of a “blockage” between both venous systems. In some cases, it was more localized in certain segments and in others, diffusely throughout the liver.
| Characteristics | Totals |
|---|---|
| Age (mean and SD) | 54,9 ± 7,9 |
| Gender | Male 12 (85,7%) Female 2 (14,3%) |
| Clinical Diagnostic | Alcoholic Cirrhosis 5 (35,7%) CHD/HSS a 1 (7,1%) Cryptogenic Cirrhosis 4 (28,6%) Cirrhosis due to hepatitis C 4 (28,6%) |
| Histopathological Diagnosis | Cirrhosis with Mild Inflammatory Activity 4 (28,6%) Cirrhosis with Moderate Inflammatory Activity 6 (42,8%) Fibrosis with Cirrhosis 2 (14,3%) Active Cirrhosis 2 (14,3%) |
| Signs of Portal Hypertension | Digestive Hemorrhage b 6 (42,6%) Ascites 7 (50,0%) Ectasia in the Portal System c 13 (92,8%) |
a Chronic Hepatic Disease / Hepatosplenic Schistosomiasis
b Includes a case of lower gastrointestinal bleeding due to shunt from the inferior mesenteric vein
c Evidenced by digestive endoscopy, Doppler ultrasound, CT angiography, or magnetic resonance imaging
| Characteristics | Totals |
|---|---|
| Dissociation between portal branches and hepatic veins | 14 (100%) |
| Dilation of intrahepatic portal branches | 6 (42,9%) |
| Portal branch thrombosis a | 4 (28,6%) |
| Collateral Veins b | 7 (50%) |
| Corkscrew venules | 6 (42,9%) |
a Interpreted by the absence of complete filling and respective branches
b Dilated portal branches, with evidence of communication with extrahepatic veins

Discussion
Surprisingly, in this study, the mean diameter of the portal branches was found below others in the literature, for normal livers. However, in six cases, these limits were exceeded, characterizing thrombosis (Table 3). The lack of portal branches in certain sectors of the mold is evidence of the degree of obstruction in the venous microcirculation in the cirrhotic liver, which in many cases even affects the flow through the hepatic veins, due to fibrosis and regeneration nodules. The lack of filling of portal branches could also hide a possible thrombosis of this branch.
In many cases, the left lobe of the liver was enlarged in relation to the right, possibly due to compensatory hyperplasia. Although the arterial bed was not studied (it was not the object of this study), during the mold preparation procedures, an increase in arterial caliber and branches was observed, as reported in the literature.
Well-prepared casts provide a three-dimensional and durable study model that can help in understanding the anatomy and changes produced by diseases in various organs, complementing histopathological and imaging studies, such as Computerized Tomography and Nuclear Magnetic Resonance.
| Cast Num. | Diameter (mm) | R | L | Signs of Thrombosis |
|---|---|---|---|---|
| 1 | 8 | 9 | – | |
| 2 | 6 | 8 | Yes | |
| 3 | 7 | 11* | – | |
| 4 | 9 | 7 | – | |
| 5 | 6 | 6 | Yes | |
| 6 | 7 | 7 | – | |
| 7 | 14* | 9 | – | |
| 8 | 10 | 7 | – | |
| 9 | 8 | 12* | – | |
| 10 | 7 | – | Yes | |
| 11 | 15* | 7 | – | |
| 12 | 8 | 6 | Yes | |
| 13 | 10 | 14* | – | |
| 14 | 9 | 10* | – |
Mean ± SD 8,9±2,61 8,7±2,36
(minimum; maximum) (6; 15) (6; 14)
* Considered dilated
Conclusion
Several indirect signs of portal hypertension could be demonstrated in resin casts of cirrhotic human livers. The most common were dissociation between the 2 venous beds (portal branches and hepatic veins) and dilatation/thrombosis of intrahepatic portal branches.
Conflicts of Interest
The author has no conflicts of interest to declare.
References
- Domagała Z, Domański J, Smyczek N, Galk C. Maceration stage in corrosion cast specimen procedure in anatomy: a minireview. Folia Morphol (Warsz). 2022;81(4):825-833. doi:10.5603/FM.a2021.0119
- Hales MR, Allan JS, Hall EM. Injection-corrosion studies of normal and cirrhotic livers. Am J Pathol. 1959;35(5):909-941
- Haratake J, Hisaoka M, Yamamoto O, Horie A. Morphological changes of hepatic microcirculation in experimental rat cirrhosis: a scanning electron microscopic study. Hepatology. 1991;13(5):952-956
- Peeters G, Debbaut C, Cornillie P, et al. A multilevel modeling framework to study hepatic perfusion characteristics in case of liver cirrhosis. J Biomech Eng. 2015;137(5):051007. doi:10.1115/1.4029280
- Tutkuviene J, Navakauskaite A, Narutyte R, Brazaitis A, Barkus A, Tamosiunas A. Hepatic portal vein branching patterns according to different liver assessment methods and classifications of branching type. Ann Anat. 2024;252:152204. doi:10.1016/j.aanat.2023.152204
- Uflacker R, Reichert P, D’Albuquerque LC, de Oliveira e Silva A. Liver anatomy applied to the placement of transjugular intrahepatic portosystemic shunts. Radiology. 1994;191(3):705-712. doi:10.1148/radiology.191.3.8184050
- Vasconcelos-Filho JM, Pereira AH, Pitta GBB, et al. Measurements between the hepatic veins and portal venous system, in human cirrhotic liver: a cast study. Surg Radiol Anat. 2018;40(4):395-400. doi:10.1007/s00276-017-1909-9
- Vasconcelos JO Filho, Batista LL, Pitta GB, Lacerda CM. Modified technique for preparation of venous circulation resin casts in the cirrhotic liver. Rev Col Bras Cir. 2016;43(5):392-394. doi:10.1590/0100-69912016005011