






Influenza Vaccination in Immunocompromised Pediatric Patients
Influenza in Immunocompromised Pediatric Patients: Presentation, Risk Factors, Vaccine Strategies, and Areas of Future Study
Markus Buchfellner¹, Rawan Budair¹˒³, Hana Hakim¹˒⁴, Diego R. Hijano¹˒², Ramia Zakhour⁵*, Lisa Hiskey¹*
Affiliations: Department of Infectious Diseases, St. Jude Children’s Research Hospital, Memphis, TN, United States; Department of Pediatrics, University of Tennessee Health Science Center, Memphis, TN, United States; Department of Pediatrics, King Hussein Cancer Center, Amman, Jordan; Department of Pediatrics, Memphis, TN, United States.
Abstract
Influenza viruses are single-stranded, negative-sense RNA viruses classified within the family Orthomyxoviridae. There are three antigenically distinct species of influenza that infect humans: influenza A, B, and C. Influenza A and B cause most human infections and may cause clinically significant disease, whereas influenza C viruses are less common and typically cause mild respiratory illness. In the Northern hemisphere, influenza typically circulates between October and May, with peak activity in December and January.
Globally, the World Health Organization (WHO) estimates that influenza viruses cause up to 650,000 deaths per year due to respiratory disease alone. This number does not account for the additional morbidity associated with influenza in immunocompromised patients.
In this review, we discuss the presentation and risk factors for influenza in immunocompromised pediatric patients, the current vaccination strategies, and areas for future research.
Keywords
Influenza, immunocompromised, pediatric patients, vaccination, risk factors.
Introduction
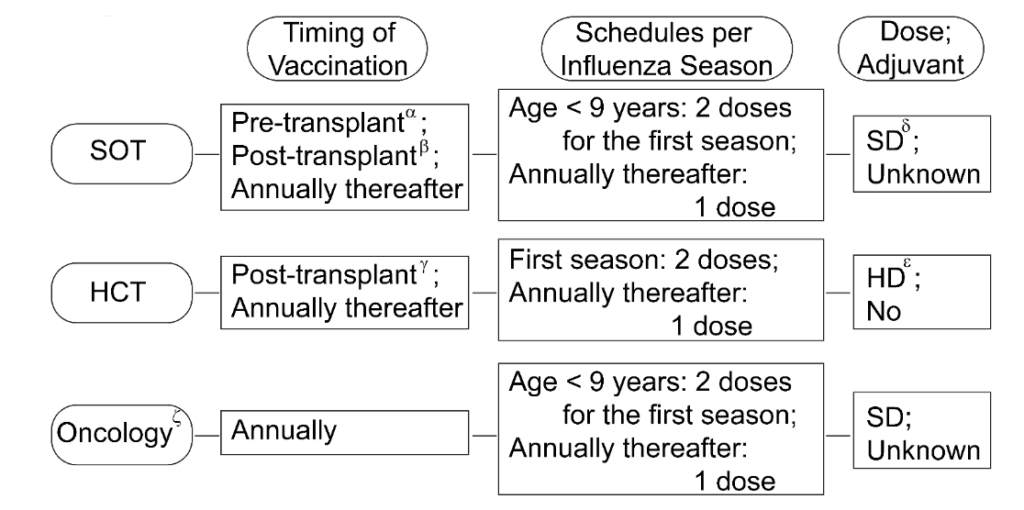
Figure 1. Summary of approaches to improve the response to influenza vaccine in pediatric oncology patients, solid-organ transplant recipients, and hematopoietic cell transplant recipients.
-
Pediatric recipients of solid organ transplants (SOT) are suggested to receive the inactivated influenza vaccine as soon as possible prior to the transplant.
‡ Pediatric recipients who already underwent SOT are recommended to administer the inactivated influenza vaccine 3 to 6 months after the transplant, with earlier administration at 1 month during peak season.
† Pediatric recipients who already underwent hematopoietic cell transplant (HCT) are recommended to administer the inactivated influenza vaccine 6 months after the transplant, with earlier administration at 3 months during the influenza outbreak.
§ Ongoing research is comparing high-dose (HD) and standard-dose (SD) formulations of the inactivated vaccine. Preliminary data suggest that HD vaccine may elicit a stronger immune response; however, it has not been adopted as standard practice.
⁑ Evidence supports the benefit of a two-dose HD vaccine in the first influenza season post-transplant. Subsequently, a single-dose SD vaccine may be given annually thereafter.
ζ The vaccination strategy recommendations and corresponding humoral responses vary depending on the chemotherapy. Patients who receive rituximab within 6 months prior to vaccination have significantly impaired humoral responses to influenza vaccines. Safety in patients receiving immune checkpoint inhibitors is unclear.
Acknowledgements:
Author Contributions:
All listed co-authors made substantial and direct contribution to this manuscript, including conception, design, analysis, writing, and proofreading. We also thank Winston Gu for the overall proofreading and reformatting.
Conflicts of Interest Statement:
The authors report no conflicts of interest pertaining to this work.
Funding Statement:
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
2. Organization WH. Influenza (seasonal). 2025. https://www.who.int/news-room/fact-sheets/detail/influenza-(seasonal) (accessed 24 Mar 2025).
3. Grohskopf LA, Ferdinands JM, Blanton LH, Broder KR, Loehr J. Prevention and Control of Seasonal Influenza with Vaccines: Recommendations of the Advisory Committee on Immunization Practices – United States, 2024-25 Influenza Season. MMWR Recomm Rep 2024; 73(5): 1-25.
4. Organization WH. Burden of Disease. 2025. https://www.who.int/teams/global-influenza-programme/surveillance-and-monitoring/burden-of-disease (accessed 24 Mar 2025).
5. United States Centers for Disease Control and Prevention. Preliminary Estimated Flu Disease Burden 2023-2024 Flu Season. 2024.
https://www.cdc.gov/flu-burden/php/data-vis/2023-2024.html (accessed April 16 2025).
6. Organization WH. Vaccines against influenza: WHO position paper – May 2022. 19, 2022.
7. Caldera F, Mercer M, Samson SI, Pitt JM, Hayney MS. Influenza vaccination in immunocompromised populations: Strategies to improve immunogenicity. Vaccine 2021; 39 Suppl 1: A15-A23.
8. Prevention TCfDCa. People at Increased Risk for Flu Complications. 11 September 2024 2024. https://www.cdc.gov/flu/highrisk/index.htm.
9. European Centre for Disease Prevention and Control. Seasonal influenza vaccines. 2023.
https://www.ecdc.europa.eu/en/seasonal-influenza/prevention-and-control/seasonal-influenza-vaccines (accessed April 15 2025).
10. Dulek DE, de St Maurice A, Halasa NB. Vaccines in pediatric transplant recipients-Past, present, and future. Pediatr Transplant 2018; 22(7): e13282.
11. GiaQuinta S, Michaels MG, McCullers JA, et al. Randomized, double-blind comparison of standard-dose vs. high-dose trivalent inactivated influenza vaccine in pediatric solid organ transplant patients. Pediatr Transplant 2015; 19(2): 219-28.
12. Hakim H, Allison KJ, Van De Velde LA, Li Y, Flynn PM, McCullers JA. Immunogenicity and safety of inactivated monovalent 2009 H1N1 influenza A vaccine in immunocompromised children and young adults. Vaccine 2012; 30(5): 879-85.
13. Long CB, Ramos I, Rastogi D, et al. Humoral and cell-mediated immune responses to monovalent 2009 influenza A/H1N1 and seasonal trivalent influenza vaccines in high-risk children. J Pediatr 2012; 160(1): 74-81.
14. Ryan AL, Wadia UD, Jacoby P, et al. Immunogenicity of the inactivated influenza vaccine in children who have undergone allogeneic haematopoietic stem cell transplant. Bone Marrow Transplant 2020; 55(4): 773-9.
15. Haddadin Z, Spieker AJ, Amarin JZ, et al. Incidence of and risk factors for influenza-associated hospital encounters in pediatric solid organ transplant recipients. Am J Transplant 2023; 23(5): 659-65.
16. Kumar D, Ferreira VH, Blumberg E, et al. A 5-Year Prospective Multicenter Evaluation of Influenza Infection in Transplant Recipients. Clin Infect Dis 2018; 67(9): 1322-9.
17. Danziger-Isakov L, Kumar D, Practice AICo. Vaccination of solid organ transplant candidates and recipients: Guidelines from the American society of transplantation infectious diseases community of practice. Clin Transplant 2019; 33(9): e13563.
18. Rubin LG, Levin MJ, Ljungman P, et al. 2013 IDSA clinical practice guideline for vaccination of the immunocompromised host. Clin Infect Dis 2014; 58(3): e44-100.
19. Santibanez TA, Black CL, Zhou T, Srivastav A, Singleton JA. Parental hesitancy about COVID-19, influenza, HPV, and other childhood vaccines. Vaccine 2024; 42(25): 126139.
20. Camerino M, Jackson S, Chinnakotla S, Verghese P. Effects of the influenza vaccine on pediatric kidney transplant outcomes. Pediatr Transplant 2019; 23(2): e13354.
21. Harboe ZB, Modin D, Gustafsson F, et al. Effect of influenza vaccination in solid organ transplant recipients: A nationwide population-based cohort study. Am J Transplant 2022; 22(10): 2409-17.
22. Perez-Romero P, Bulnes-Ramos A, Torre-Cisneros J, et al. Influenza vaccination during the first 6 months after solid organ transplantation is efficacious and safe. Clin Microbiol Infect 2015; 21(11): 1040 e11-8.
23. Suresh S, Upton J, Green M, et al. Live vaccines after pediatric solid organ transplant: Proceedings of a consensus meeting, 2018. Pediatr Transplant 2019; 23(7): e13571.
24. Haddadin Z, Krueger K, Thomas LD, Overton ET, Ison M, Halasa N. Alternative strategies of posttransplant influenza vaccination in adult solid organ transplant recipients. Am J Transplant 2021; 21(3): 938-49.
25. Cordero E, Roca-Oporto C, Bulnes-Ramos A, et al. Two Doses of Inactivated Influenza Vaccine Improve Immune Response in Solid Organ Transplant Recipients: Results of TRANSGRIPE 1-2, a Randomized Controlled Clinical Trial. Clin Infect Dis 2017; 64(7): 829-38.
26. Mombelli M, Neofytos D, Huynh-Do U, et al. Immunogenicity of High-Dose Versus MF59-Adjuvanted Versus Standard Influenza Vaccine in Solid Organ Transplant Recipients: The Swiss/Spanish Trial in Solid Organ Transplantation on Prevention of Influenza (STOP-FLU Trial). Clin Infect Dis 2024; 78(1): 48-56.
27. Carr SB, Adderson EE, Hakim H, Xiong X, Yan X, Caniza M. Clinical and demographic characteristics of seasonal influenza in pediatric patients with cancer. Pediatr Infect Dis J 2012; 31(11): e202-7.
28. Furlong E, Kotecha RS. Lessons learnt from influenza vaccination in immunocompromised children undergoing treatment for cancer. Lancet Child Adolesc Health 2023; 7(3): 199-213.
29. Yarnall JN, Mertens A, Yee M, Orenstein E, Lai KW, Wasilewski-Masker K. Influenza Vaccination Receipt in Pediatric Patients With Cancer or Sickle Cell Disease. J Pediatr Hematol Oncol 2023; 45(2): e228-e35.
30. Tasian SK, Park JR, Martin ET, Englund JA. Influenza-associated morbidity in children with cancer. Pediatr Blood Cancer 2008; 50(5): 983-7.
31. Choi DK, Fuleihan RL, Walterhouse DO. Serologic response and clinical efficacy of influenza vaccination in children and young adults on chemotherapy for cancer. Pediatr Blood Cancer 2016; 63(11): 2011-8.
32. Mavinkurve-Groothuis AM, van der Flier M, Stelma F, van Leer-Buter C, Preijers FW, Hoogerbrugge PM. Absolute lymphocyte count predicts the response to new influenza virus H1N1 vaccination in pediatric cancer patients. Clin Vaccine Immunol 2013; 20(1): 118-21.
33. Kersun LS, Reilly A, Coffin SE, et al. A prospective study of chemotherapy immunologic effects and predictors of humoral influenza vaccine responses in a pediatric oncology cohort. Influenza Other Respir Viruses 2013; 7(6): 1158-67.
34. Kotecha RS, Wadia UD, Jacoby P, et al. Immunogenicity and clinical effectiveness of the trivalent inactivated influenza vaccine in immunocompromised children undergoing treatment for cancer. Cancer Med 2016; 5(2): 285-93.
35. Mikulska M, Cesaro S, de Lavallade H, et al. Vaccination of patients with haematological malignancies who did not have transplantations: guidelines from the 2017 European Conference on Infections in Leukaemia (ECIL 7). Lancet Infect Dis 2019; 19(6): e188-e99.
36. Sykes A, Gerhardt E, Tang L, Adderson EE. The Effectiveness of Trivalent Inactivated Influenza Vaccine in Children with Acute Leukemia. J Pediatr 2017; 191: 218-24 e1.
37. Hakim H, Allison KJ, Van de Velde LA, et al. Immunogenicity and safety of high-dose trivalent inactivated influenza vaccine compared to standard-dose vaccine in children and young adults with cancer or HIV infection. Vaccine 2016; 34(27): 3141-8.
38. Walti CS, Loes AN, Shuey K, et al. Humoral immunogenicity of the seasonal influenza vaccine before and after CAR-T-cell therapy: a prospective observational study. J Immunother Cancer 2021; 9(10).
39. Chong CR, Park VJ, Cohen B, Postow MA, Wolchok JD, Kamboj M. Safety of Inactivated Influenza Vaccine in Cancer Patients Receiving Immune Checkpoint Inhibitors. Clin Infect Dis 2020; 70(2): 193-9.
40. Engelhard D, Mohty B, de la Camara R, Cordonnier C, Ljungman P. European guidelines for prevention and management of influenza in hematopoietic stem cell transplantation and leukemia patients: summary of ECIL-4 (2011), on behalf of ECIL, a joint venture of EBMT, EORTC, ICHS, and ELN. Transpl Infect Dis 2013; 15(3): 219-32.
41. Renaud C, Campbell AP. Changing epidemiology of respiratory viral infections in hematopoietic cell transplant recipients and solid organ transplant recipients. Curr Opin Infect Dis 2011; 24(4): 333-43.
42. Cordonnier C, Einarsdottir S, Cesaro S, et al. Vaccination of haemopoietic stem cell transplant recipients: guidelines of the 2017 European Conference on Infections in Leukaemia (ECIL 7). Lancet Infect Dis 2019; 19(6): e200-e12.
43. Pinana JL, Perez A, Chorao P, et al. Respiratory virus infections after allogeneic stem cell transplantation: Current understanding, knowledge gaps, and recent advances. Transpl Infect Dis 2023; 25 Suppl 1: e14117.
44. Ogimi C, Xie H, Waghmare A, et al. Novel factors to predict respiratory viral disease progression in allogeneic hematopoietic cell transplant recipients. Bone Marrow Transplant 2022; 57(4): 649-57.
45. Kmeid J, Vanichanan J, Shah DP, et al. Outcomes of Influenza Infections in Hematopoietic Cell Transplant Recipients: Application of an Immunodeficiency Scoring Index. Biol Blood Marrow Transplant 2016; 22(3): 542-8.
46. Kim YJ, Waghmare A, Xie H, et al. Respiratory viruses in hematopoietic cell transplant candidates: impact of preexisting lower tract disease on outcomes. Blood Adv 2022; 6(18): 5307-16.
47. Zhang W, Rowntree LC, Muttucumaru R, et al. Robust immunity to influenza vaccination in haematopoietic stem cell transplant recipients following reconstitution of humoral and adaptive immunity. Clin Transl Immunology 2023; 12(6): e1456.
48. Halasa NB, Savani BN, Asokan I, et al. Randomized Double-Blind Study of the Safety and Immunogenicity of Standard-Dose Trivalent Inactivated Influenza Vaccine versus High-Dose Trivalent Inactivated Influenza Vaccine in Adult Hematopoietic Stem Cell Transplantation Patients. Biol Blood Marrow Transplant 2016; 22(3): 528-35.
49. Natori Y, Humar A, Lipton J, et al. A pilot randomized trial of adjuvanted influenza vaccine in adult allogeneic hematopoietic stem cell transplant recipients. Bone Marrow Transplant 2017; 52(7): 1016-21.
50. Schuster JE, Hamdan L, Dulek DE, et al. The Durability of Antibody Responses of Two Doses of High-Dose Relative to Two Doses of Standard-Dose Inactivated Influenza Vaccine in Pediatric Hematopoietic Cell Transplant Recipients: A Multi-Center Randomized Controlled Trial. Clin Infect Dis 2024; 78(1): 217-26.
51. Amarin JZ, Dulek DE, Simmons J, et al. Immunophenotypic predictors of influenza vaccine immunogenicity in pediatric hematopoietic cell transplant recipients. Blood Adv 2024; 8(8): 1880-92.
52. Bahakel H, Spieker AJ, Hayek H, et al. Immunogenicity and Reactogenicity of High- or Standard-Dose Influenza Vaccine in a Second Consecutive Influenza Season. J Infect Dis 2025; 231(1): e123-e31.
53. Sung L, Heurter H, Zokvic KM, et al. Practical vaccination guidelines for children with cancer. Paediatr Child Health 2001; 6(6): 379-83.