

Innominate Artery Dissection: Acute Stroke Case Study
Isolated Dissection of the Innominate Artery Presenting as Acute Stroke: A Case Report and Review of the Literature
Ilson Sepúlveda. 1; Aristides Capizzano 2 & Sergio Castillo 3
- Radiology Department, Otorhinolaryngology and Maxillofacial Services, General Hospital of Concepción
- Radiology Department, Division of Neuroradiology, University of Michigan Health System, Ann Arbor, MI, USA
- Otorhinolaryngology, General Hospital of Concepcion, University of Concepción School of Medicine, Concepcion, Chile
OPEN ACCESS
PUBLISHED: 31 January 2026
CITATION: Sepúlveda, I., Capizzano, A., et al., 2026. Isolated Dissection of the Innominate Artery Presenting as Acute Stroke: A case report and review of the literature. Medical Research Archives, [online] 14(1).
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v14i1.7232
ISSN 2375-1924
ABSTRACT
Isolated innominate artery dissection is a rare vascular disorder, and its symptoms may vary. We present the case of an elderly patient who was admitted to the emergency department at an external hospital. A clinical examination revealed symptoms of acute stroke. No other neurological symptoms were observed. A computed tomography angiography (CTA) revealed dissection of the innominate artery.
Keywords: Isolated; Innominate Artery dissection; Stroke; CT; Angiogram
Introduction
Isolated dissection of the innominate artery is a rare vascular condition, but it can carry a high risk of mortality. Due to the limited number of cases described, the existing literature is scarce. This clinical entity is characterized by traumatic or spontaneous separation of the layers that form the arterial wall. Patients with isolated dissection of the innominate artery may present with a wide spectrum of symptoms depending on the extent of the dissection and ischemic involvement. Common symptoms include sudden, localized pain in the right cervical or thoracic region, often characterized as stabbing or pulsating, and often accompanied by radiation to the head, neck, or upper chest. Diagnostic imaging tests are essential for diagnosis and planning optimal treatment. Contrast-enhanced computed tomography (CT) angiography and magnetic resonance (MR) angiography are the preferred diagnostic modalities.
Treatment of isolated innominate artery dissection should be comprehensive and personalized, taking into account the severity of the injury, associated complications, and the patient’s comorbidities. The prognosis varies depending on the timely diagnosis and appropriate treatment.
Case Report
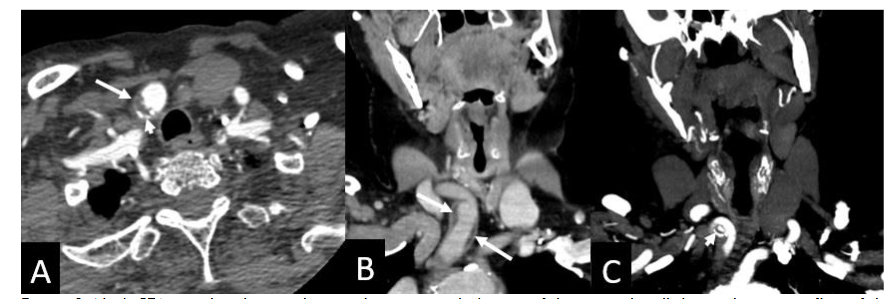
An 89-year-old patient was admitted to the emergency department at an external hospital, having presented with symptoms of an acute cerebrovascular accident. These symptoms included headache, ataxia, slurred speech, and facial weakness on the left side. No history of head or neck trauma or other neurological deficits was detected. A neck computed tomography angiogram (CTA) was performed. The imaging revealed a segmental wall thickening of the innominate artery (IA) with luminal narrowing and an expansion of its diameter. These findings are consistent with innominate artery dissection.
Discussion
Isolated dissection of the innominate artery (also known as the brachiocephalic artery) is a rare vascular condition, but one that can carry a high risk of mortality. Given that it is an uncommon condition and its presentation is heterogeneous, it can pose a significant diagnostic and therapeutic challenge. The innominate artery is a large-caliber artery that emerges from the aortic arch and bifurcates into the right common carotid artery and the right subclavian artery, supplying blood to the right side of the head, neck and right upper limb. This clinical entity is characterized by a separation of the layers that make up the arterial wall, affecting only the innominate artery, without affecting other nearby structures such as the aortic arch or other supra-aortic arteries, a situation that distinguishes it from extended aortic dissections. Dissection in this vessel can lead to severe complications, such as pseudoaneurysm formation, vascular occlusion, cerebral embolisms, and even arterial rupture with potentially lethal hemorrhage. Due to the low number of reported cases, the existing literature is scarce.
Arterial dissection involves the appearance of a tear in the intima that allows blood to enter the space between the layers of the arterial wall, creating a false lumen. In the specific case of isolated innominate artery dissection, this separation occurs only in the artery itself, without extension to the aortic arch or adjacent branches. This condition can occur spontaneously or secondary to trauma, with the former being a rarer cause. Some reports have described it in association with high-energy trauma, including vehicle accidents or gunshot wounds, with a potential risk of arterial rupture, distal thromboembolism, and cerebral ischemia.
The incidence of isolated innominate artery dissection is low, and precise epidemiological data are lacking due to the scarcity of reported cases. The incidence of aneurysms involving the innominate artery has been estimated at 3-5% of traumatic thoracic vessel dissections and 0.003% of all arterial aneurysms, making isolated dissections even less common. Fewer than ten documented cases of spontaneous innominate artery dissection have been reported in the literature, usually in older adults with cardiovascular risk factors such as high blood pressure and atherosclerosis. On the other hand, when the dissection is traumatic in origin, it is only occasionally reported in young people following accidents or penetrating injuries. The paucity of cases limits the generation of robust epidemiological data.
Isolated innominate artery dissection involves a tear in the arterial intima, allowing blood to enter and spread into the media, forming a false lumen. In patients with atherosclerosis, the presence of calcified plaque in the proximal area of the artery may contribute to the limited location and extent of the dissection, acting as a barrier to progression toward the aorta or aortic arch. Furthermore, hemodynamic stress on this artery, resulting from high blood pressure or trauma, may favor the development of the lesion. In traumatic cases, the force of mechanical impact can cause an immediate tear of the intimal layer.
The compromised blood flow due to the dissection can lead to cerebral or distal ischemia due to malperfusion or embolization of thrombotic material from the false lumen, increasing the risk of stroke. When the dissection progresses to a pseudoaneurysm, there is a high risk of rupture and severe mediastinal hemorrhage.
Patients with isolated dissection of the innominate artery may present with a wide spectrum of symptoms depending on the extent of the dissection and ischemic involvement. Common symptoms include sudden onset of localized pain, partially in the right cervical or thoracic region, which may be stabbing or pulsating in character, often accompanied by radiation to the head, neck, or upper chest. Neurological deficits, suggestive of cerebrovascular accidents or transient ischemic attacks, may be secondary to embolic events resulting from the dissection, affecting cerebral or vertebral arteries, and may include symptoms such as dizziness, weakness, aphasia, or visual changes. In addition, ischemia of the ipsilateral extremities may be observed, manifested by weakness, coldness, or pallor, due to compromise of the arteries supplying these regions. Syncope may also be a symptom if the dissection causes a rapid reduction in cerebral or cardiovascular blood flow. Other clinical signs described include hypoesthesia of the ipsilateral arm, neck pain, a sensation of pulsation or mass in the cervical or supraclavicular region, and signs of proximal or distal vascular insufficiency. The variability in clinical presentation can lead to the condition being confused with other vascular or neurological pathologies, such as aneurysms, arterial thrombosis, cervical diseases, or cerebrovascular events, thus hampering timely diagnosis.
Diagnostic imaging is essential for confirming innominate artery dissection and planning optimal treatment. Contrast-enhanced computed tomography (CT) angiography and magnetic resonance (MR) angiography are the modalities of choice due to their high sensitivity and specificity, allowing detailed visualization of arterial anatomy. These techniques allow detection of double lumen, intraluminal thrombi, dissection maps, arterial stenosis or occlusions, and assess the proximal and distal extent of the lesion. Chest CT is commonly used in the initial evaluation to rule out other thoracic pathologies and delineate the extent of the dissection. It also detects associated complications, such as mediastinal bleeding or involvement of adjacent structures. MR angiography provides visualization without radiation exposure and is better able to assess changes in the arterial wall and blood flow in real time. It is useful in patients with a contraindication to iodinated contrast therapy. In cases where examinations are inconclusive, conventional angiography using vascular catheterization can provide detailed visualization of the arterial anatomy, also allowing for dynamic flow assessment and facilitating interventional therapeutic decisions. Characteristic findings in these examinations include a double lumen with separation of the intima and media, the presence of parietal hematomas, intraluminal thrombi, and blood flow abnormalities, such as reduced or altered perfusion to the cerebral arteries.
In addition, carotid ultrasound and Doppler ultrasound play an important role in the evaluation of extracranial arteries in accessible areas, allowing for the detection of changes in flow, the presence of thrombi, and alterations in the arterial wall. However, their usefulness in direct visualization of dissection in the innominate artery is limited due to the depth and anatomical position of this artery. They are more useful for assessing the status of the cervicocranial arteries in their extracranial course.
The treatment of isolated innominate artery dissection requires a comprehensive and personalized approach, considering the severity of the injury, associated complications, and the patient’s comorbidities. In stable cases without acute neurological symptoms, with a vascular diameter less than 3 cm, and no signs of poor perfusion or distal embolization, conservative medical management is initially recommended. This approach includes strict blood pressure control with antihypertensives, pain management, and close clinical and radiological monitoring to detect possible changes in the extent of the dissection or complications.
Endovascular repair is presented as a less invasive and potentially effective alternative in certain cases, especially in localized lesions with adequate proximal landing zones and without significant calcification that would compromise stenting. However, its applicability may be limited by vascular anatomy, the extent of the dissection, and the presence of calcified plaques or arteriovenous abnormalities.
Open surgical repair remains the definitive option in cases of unstable dissection, rupture, aneurysm, or severe hemodynamic compromise. The procedure generally involves resection of the dissection and reconstruction with prosthetic grafts, performed through a median sternotomy. The use of cardiopulmonary bypass and hypothermic circulatory arrest may be necessary in cases where the aortic arch is involved or when an extended repair is required. The choice between open surgical treatment and endovascular treatment requires a multidisciplinary evaluation, considering the risks of cerebral ischemia, the experience of the team, vascular anatomy, and potential toxicity of the contrast agent. It is recommended that medical management be performed in cases involving vessels with a diameter less than 3 centimeters and the absence of any evidence of distal emboli or malperfusion. The literature includes only a few reports on isolated dissections of the brachiocephalic artery presenting with stroke and treated with anticoagulants. One case improved with thrombolysis, but worsened after. This could be from an intramural hematoma causing flow disturbance. The decision should be based on a careful assessment of the benefits and risks, seeking the safest and most effective option for each patient.
The prognosis for isolated innominate artery dissection varies depending on timely diagnosis and appropriate management. Patients who receive early surgical intervention for ruptured or complicated dissections have favorable outcomes with low rates of cerebral complications and mortality. In contrast, patients treated medically require careful long-term monitoring, as dissections may remain stable or rarely progress, justifying intervention if they enlarge or develop symptoms. Overall, the rarity of the condition limits large-scale cohort analyses, but available case reports suggest that strict blood pressure control and close monitoring contribute significantly to reducing adverse events.
Conclusion
Isolated innominate artery dissection is a rare vascular disorder with a varied clinical presentation, posing diagnostic and therapeutic challenges. Timely imaging is essential to guide management, which can range from conservative therapy to complex surgical repair. Given the potential for serious complications, including fractures and strokes, increased awareness and individualized treatment protocols are crucial to optimize patient outcomes.
Conflict of interest: None.
References
- Karmy-Jones R, DuBose R, King S. Traumatic rupture of the innominate artery. Eur J Cardiothorac Surg. 2003;23(5):782-787. doi:10.1016/s1010-7940(03)00032-0
- Hirose H, Gill IS. Blunt injury of the innominate artery: a case report and review of literature. Ann Thorac Cardiovasc Surg. 2004;10(4):218-223.
- Yaghi S, Maalouf N, Keyrouz SG. Cervical artery dissection: risk factors, treatment, and outcome; a 5-year experience from a tertiary care center. J Neurosci. 2012;122(1):40-44. doi:10.3109/00207454.2011.622453
- Kasashima F, Urayama H, Ohtake H, Watanabe Y. Intrathoracic aneurysm of the innominate and right subclavian arteries: report of a case. Surg Today. 2001;31(1):51-54. doi:10.1007/s005950170220.
- Kieffer E, Chiche L, Koskas F, Bahnini A. Aneurysms of the innominate artery: surgical treatment of 27 patients. J Vasc Surg. 2001;34(2):222-228. doi:10.1067/mva.2001.115807
- Kotoulas C, Georgiou C, Chouliaras E, et al. Diagnostic dilemma in spontaneous innominate artery pathology: a case report. Gen Thorac Cardiovasc Surg. 2021;69(2):367-370. doi:10.1007/s11748-020-01472-6
- Hirose H, Moore E. Delayed presentation and rupture of a posttraumatic innominate artery aneurysm: case report and review of the literature. J Trauma. 1997;42(6):1187-1195. doi:10.1097/00005373-199706000-00038
- Mani H, Ahluwalia S. Isolated brachiocephalic artery dissection presenting as acute stroke. BMJ Case Rep. 2015;2015:bcr2014208815. Published 2015 Aug 27. doi:10.1136/bcr-2014-208815
- Deshpande AA, Agasty S, Kumar S, Ramakrishnan P. Isolated traumatic innominate artery dissection: an exceedingly rare entity!. BMJ Case Rep. 2021;14(3):e241710. Published 2021 Mar 1. doi:10.1136/bcr-2021-241710
- Munakata H, Okada K, Tanaka H, Yamashita T, Nakagiri K, Okita Y. Acute dissection of the innominate artery: a case of report. Gen Thorac Cardiovasc Surg. 2008;56(3):131-133. doi:10.1007/s11748-007-0205-8
- Seese L, Kilic A, Navid F, Gleason TG, Sultan I. Nonoperative Management of Brachiocephalic Artery Dissection. Ann Thorac Surg. 2019;107(2):e97-e99. doi:10.1016/j.athoracsur.2018.06.047
- Murray LW. Spontaneous brachiocephalic artery dissection: a case report. J Surg Case Rep. 2025;2025(2):rjaf040. Published 2025 Feb 5. doi:10.1093/jscr/rjaf040
- Francillard I, Grangeon L, Triquenot-Bagan A, Ozkul-Wermester O. Innominate artery dissection and stroke after rifle recoil. Acta Neurol Belg. 2018;118(4):557-559. doi:10.1007/s13760-018-0945-5
- Bush RL, Hurt JE, Bianco CC. Endovascular management of a ruptured mycotic aneurysm of the innominate artery. Ann Thorac Surg. 2002;74(6):2184-2186. doi:10.1016/s0003-4975(02)03976-0
- Hirose T, Tabayashi N, Yoshikawa Y, et al. Isolated dissecting aneurysm of the brachiocephalic artery associated with contained rupture. Gen Thorac Cardiovasc Surg. 2012;60(4):225-227. doi:10.1007/s11748-011-0809-x
- Sharaf OM, Martin TD, Jeng EI. Management of a spontaneous supra-aortic arterial dissection: a case report. J Med Case Rep. 2021;15(1):283. Published 2021 Jun 2. doi:10.1186/s13256-021-02886-3
- Ohki S, Obayashi T, Koyano T, Yasuhara K, Hirai H, Hatori K. Spontaneous innominate and left common carotid artery dissection with bovine aortic arch. Gen Thorac Cardiovasc Surg. 2014;62(4):238-240. doi:10.1007/s11748-013-0253-1
- Nagata T, Johno H, Wang Y, Asanuma M. Isolated innominate artery dissection. J Card Surg. 2017;32(11):710-711. doi:10.1111/jocs.13229
- Takagi H. Spontaneous isolated brachiocephalic artery dissection with subsequent type-A acute aortic dissection. Eur Heart J Case Rep. 2025;9(4):ytaf142. Published 2025 Mar 25. doi:10.1093/ehjcr/ytaf142
- Williams DM, Masuno K, Kanchuger MS, Hisamoto K. Innominate artery dissection due to selective cerebral antegrade perfusion. J Card Surg. 2021;36(2):761-763. doi:10.1111/jocs.15290