





Innovative Training Solutions in Obstetrics and Gynecology
Innovating to overcome challenges:A descriptive retrospective review of novel elements of a new Obstetrics and Gynaecology specialty training programme in Botswana
Sarah Jean Hanson¹²³⁴⁵, Rebecca Luckett¹²³⁴⁵, Mercy-Nkuba Nassali¹², G Justus Hofmeyr¹²⁶, Leatile Sedabadi¹², Thabo Moloi², Francoise D Rubgega¹², Modimowame Jamieson², Kyungu M Kime², Lisa Bazzett-Matabele¹²
- Department of Obstetrics and Gynaecology, Faculty of Medicine, University of Botswana, Gaborone, Botswana
- Department of Obstetrics and Gynaecology, Princess Marina Hospital, Gaborone, Botswana
- Botswana Harvard Health Partnership, Gaborone, Botswana
- Department of Obstetrics and Gynecology, Division of Global and Community Health, Beth Israel Deaconess Medical Center, Boston, USA
- Harvard Medical School, Boston, USA
- Effective Care Research Unit, University of the Witwatersrand and Walter Sisulu University, East London, South Africa
OPEN ACCESS
PUBLISHED: 31 May 2025
CITATION: Hanson, S. J., et al., 2025. Innovating to overcome challenges: A descriptive retrospective review of novel elements of a new Obstetrics and Gynaecology specialty training programme in Botswana. Medical Research Archives, [online] 13(5).
https://doi.org/10.18103/mra.v13i5.6533
COPYRIGHT: © 2025 European Society of Medicine.This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i5.6533
ISSN 2375-1924
ABSTRACT
Introduction
In 2020 the University of Botswana launched a novel in-country Obstetrics and Gynaecology specialty training programme. Low and middle-income country programmes face inherent challenges due to resource limitations including unpredictability in access to services, system inefficiencies, and human resource shortages for training, especially subspecialists.
Methods
In order to meet training needs in the face of these challenges, we have utilized creative teaching methods, including novel technologies and maximizing sustainable international partnerships. We have encouraged the use of technology including online resources, simulations, and artificial intelligence to enhance training for ultrasound and minimally invasive surgery. Remote lectures and imaging review engage subspecialists in sustained academic partnerships to build skills and knowledge. Finally, we conceived a departmental wellness program to address provider burnout.
Results
Our trainees have gained needed skills in laparoscopy and ultrasound using technology. We are achieving subspecialty training through collaboration with our international academic partners. A new wellness program has started and been well-received.
Discussion
Using these methods we have not only met trainee needs, but improved patient care and service access. Challenges still remain to encourage programme sustainability. Implementation of laparoscopy and ultrasound will require adequate continued training and system support for quality assurance. Subspecialty training needs on-going bolstering and requires building in-country sub-specialization pathways. Wellness programs need to be broadened.
Conclusion
By utilizing creative solutions involving collaboration and technology, our trainees gain skills needed despite context limitations. We believe our programme has been successful in part because it has been dynamic during its initial rollout, and will continue to be as the programme continues to evolve.
INTRODUCTION
The greatest unmet need for medical care remains in LMIC (low- and middle-income countries), especially in SSA (sub-Saharan Africa). A shortage of trained doctors contributes to this gap as substandard threshold densities of doctors to population are directly related to poor health outcomes. Women are particularly impacted by inadequate access to maternal health care, gynaecologic surgery, and reproductive health services. Botswana is an upper middle-income country in the heart of SSA and despite its economic standing, maternal deaths in Botswana are 185 per 100,000 deliveries, more than double the target outlined in the World Health Organization (WHO) Sustainable Development Goals for Maternal Mortality (MM).
Lack of trained providers, especially Obstetrician-Gynaecologist (OB/GYN) specialists, is one well-established cause of these access limitations in Botswana. Increasing the number of skilled specialist providers has been identified as one critical initiative to improve reproductive health care and contribute to MM reduction. The establishment of in-country medical training programmes has been shown to ameliorate this health care disparity, as those wishing to seek training may not be willing nor able to relocate to another country to seek educational opportunities. Those training elsewhere are at risk of not returning and emigrating away from their home healthcare system.
However, resource limitations pose significant challenges to implementing successful OB/GYN residency training programmes in LMIC settings. Hospitals may lack advanced diagnostics and human resources, especially in subspecialties. Training sites often face unpredictability in access to essential services like imaging modalities, operating theaters, and critical care. To overcome these barriers, innovative solutions being explored include exchange programs, simulation-based learning, remote coaching and didactics, and open-access learning through virtual grand rounds and online resources.
Background
In 2020 the University of Botswana (UB) launched a novel in-country OB/GYN Masters of Medicine (MMED) residency training programme. By training OB/GYNs in-country, the programme seeks to elevate the quality of women’s health care at a national level, including improving maternal and neonatal outcomes, increasing access to care, developing regional leaders, and driving innovation in women’s health. The UB OB/GYN MMED training programme curriculum was designed to specifically meet the health needs of Botswana.
The teaching hospital, Princess Marina (PMH), is a 592-bed tertiary care government referral hospital in Botswana’s capital, performing 6500 deliveries per year. While PMH serves as the UB educational site, it faces challenges common to public and government hospitals, including high patient volumes, inadequate facilities, logistic issues, and limited access to intensive care beds and diagnostic capabilities. Limited experience with novel technologies like minimally invasive surgery hinders its adoption. Subspecialties are scarce, with only one gynaecologic oncologist in the public sector. These limitations pose challenges to training programmes, but also impact retention of providers within the system.
Aim
We will present a descriptive retrospective review of some novel solutions implemented to address select training challenges in our setting. We will discuss the outcomes of these interventions and next steps based on our experiences. The scope of this review is not a comprehensive evaluation, but a reflective assessment of some aspects of the UB MMED OB/GYN programme educational innovations that addressed training gaps and optimized trainee exposure for success in our setting. We hope our experiences can be applied to programmes in other countries facing similar problems.
IDENTIFIED TRAINING CHALLENGES
Minimally Invasive Surgical Training Exposure
Minimally invasive surgery (MIS) approaches, such as laparoscopy, have become the standard of surgical care for many gynaecologic conditions. Nevertheless, in resource-limited regions including Botswana, laparoscopy is vastly under-utilized with little to no training occurring in our hospital. Simulation training has been shown to be a valuable tool for surgical training, including MIS; however, utilization of simulation-based surgical training is limited in LMICs. We realized the need to develop a simulation-based training program for our residents in order to gain the important skillset of laparoscopic gynaecologic surgery.
Diagnostic and Emergency Assessment Limitations
With a large patient volume and limited access to timely radiologic services, bedside ultrasound assessment allows for expedited real-time decision making for both gynaecologic and fetal assessments. In addition, we have many critical care obstetric patients, also needing rapid diagnosis without easy access to imaging. Point of care ultrasound (POCUS) has been shown to facilitate response to care in studies in emergency care settings outside of Africa. Our trainees need high-quality ultrasound skills, yet have limited education access, calling upon us to devise methods of self-study and remote support for training. Online and hybrid modules address challenges like travel bans faced during the COVID pandemic.
Lack of OB/GYN Subspecialists
With a void of subspecialists, general OB/GYNs provide many of the services that would be within subspecialty purview in settings with more resources. While the generalist faculty are quite experienced in providing advanced care, some skills lie outside of their scope of practice, yet trainee exposure to subspecialty clinical skills and education is essential to provide comprehensive OB/GYN training on par with international standards. Our programme recognized the need to leverage international academic partnerships for subspecialty support.
Provider Burnout
Burnout prevalence estimates for OB/GYNs approach 75%. Trainees are particularly at-risk due to a myriad of factors including demanding on-call schedules coupled with erratic work hours. Providers experiencing burnout are more likely to contribute to adverse patient safety events, exhibit unprofessional behavior, lose empathy, and at worst, leave medical practice. In addition to the triggers and drivers of burnout experienced in high-income countries, providers in our setting also contend with moral distress, related to the inability to provide appropriate medical care due to structural constraints or limited resources. Confronting and mitigating OB/GYN burnout through the use of wellness curricula has been demonstrated to be effective and beneficial to providers in well-resourced countries. However, the impact of wellness curricula on burnout mitigation is not well-studied in SSA. To proactively address burnout, we conceived a novel departmental wellness program for our trainees.
Methodology
SIMULATION TRAINING AND SELF-ADMINISTERED ARTIFICIAL INTELLIGENCE ASSESSMENT FOR MIS
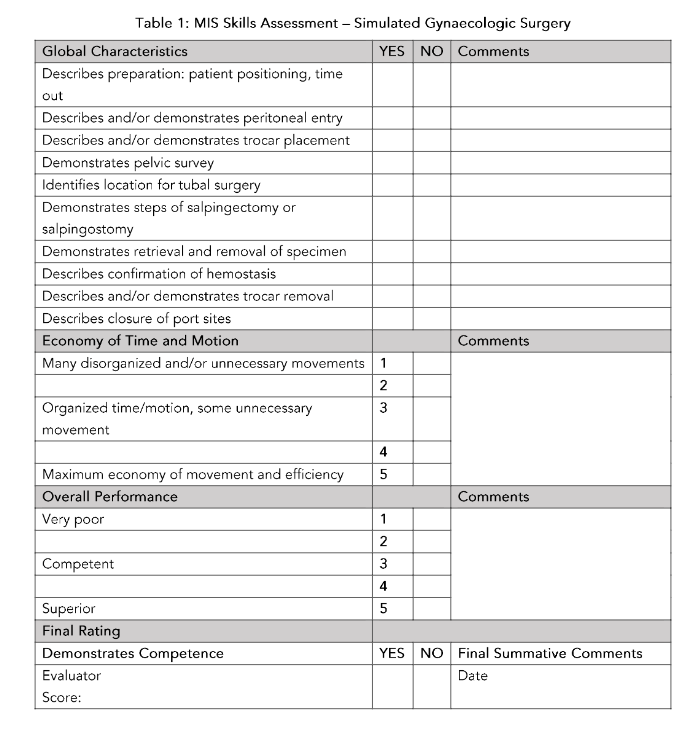
We planned implementation of a requisite MIS simulation training with the aim of increasing baseline knowledge and skills among trainees such that they could fully capitalize on the limited opportunity to participate in laparoscopy in our clinical setting resulting from limited equipment and faculty experience. Our trainees enrolled in open-access online MIS skills education modules through a program called ALL-SAFE. These modules were developed for settings where opportunities for clinical experience with MIS cases are limited and have been shown to be effective in building laparoscopic skills. The training included case-based modules and educational videos demonstrating laparoscopic skills, as well as instructions for simulation, and self-administered assessments. The modules had directions for building a MIS box trainer and simulated pelvic structures from simple items. After building and practicing with these homemade box trainers, participants uploaded videos of their practice sessions to the training website. There the videos were reviewed by artificial intelligence (AI) technology. The AI assessment provided feedback on the fluidity of skills performed in the video. The de-identified video was also sent to peers also enrolled in the online training for review and feedback. Learners then reflectively completed a self-administered assessment of their skills after concluding the training. We then anonymously surveyed residents including a self-reflective confidence assessment of their MIS skills, the number of actual MIS cases they had participated in before and after training, and any other feedback about the learning. After completing this training, we assessed their skills while performing a simulated task, observed by an OB/GYN faculty expert in MIS (Table 1).
ON-LINE, IN-PERSON AND POINT-OF-CARE OB/GYN ULTRASOUND TRAINING DIAGNOSTICS
To address the need for high-quality ultrasonography skills, we partnered with the Foundation for the Society for Maternal Fetal Medicine (MFM) Queenan Global Health program and The International Society of Ultrasound in Obstetrics and Gynecology (ISUOG) for longitudinal ultrasound training. University-based LMIC training programmes have free access to online ISUOG courses. Residents self-paced home study of nine hours of the ISUOG Basic Training course (Table 2). This was augmented with planned annual visits from senior MFM fellows for hands-on practice to reinforce the skills learned from the modules. We assessed the residents pre-and post-course with a written knowledge exam, a survey of self-reported competence, and an objective image review assessment from their scans. Finally, residents had competency-based assessments completed based on skills observed during a hands-on scan. To augment the training, UB secured an ultrasound simulator for ongoing training, providing feedback even when expert subspecialists are unavailable. Residents were each assigned the simulator for a week to practice modules aligning with ISUOG course topics. Additionally, we developed an ultrasound intervention to fill a gap in rapid emergency assessment of obstetrics and gynaecology patients. We pioneered using POCUS curriculum as a component of the critical care training received in our residency programme. This included elements such as FAST (Focused Assessment with Sonography in Trauma) and cardiopulmonary assessments of critical care obstetric patients. Lectures were one to two hours in length, delivered either virtually or in-person by a critical care trained MFM subspecialist (Table 3). Trainees practiced POCUS skills hands-on during daily clinical care, with MFM supervision when available. Trainees were surveyed after course completion to guide course effectiveness and future planning.
Table 2: Ultrasound Self-Study Course Topics
| Ultrasound Topic | Time |
|---|---|
| Introductory Principles: Physics of Ultrasound, Knobology | 1 hour |
| OB Ultrasound Basics: “6 Step” Approach | ½ hour |
| First Trimester Ultrasound: Dating, Viability, Pregnancy of Unknown Location, Ectopic Pregnancy, Multiple Gestation | 1 hour |
| Gyn Ultrasound – Uterus: Abdominal vs TVUS, IUD Localization, Intra-cavitary Lesions, Fibroids, Adenomyosis, Retained products | 1 hour |
| Gyn Ultrasound – Ovaries/Adnexae: IOTA terminology, Adnexal Lesions | 1 hour |
| Introduction to Doppler Ultrasound: Basics, Umbilical Artery Dopplers | 1 hour |
| Anatomy: “20 + 2 Planes” | 2 hours |
| Cervical Length Assessment | ½ hour |
| Placenta Assessment: Accreta Spectrum | 1 hour |
Table 3: POCUS Topics for OB/GYN
| POCUS Topic | Time |
|---|---|
| Cardiac | 2 hours |
| Lung | 1 hour |
| FAST | 1 hour |
| Duplex Doppler | 1 hour |
| Procedural Guidance (Including amniocentesis simulation) | 2 hours |
ENGAGING SUSTAINABLE INTERNATIONAL ACADEMIC SUBSPECIALIST COLLABORATIONS
Cultivating long-term international partnerships to meet our programme needs related to subspecialty training was identified as a potentially impactful way improve our training experience. Along with the MFM collaborations described, we devised solutions for other subspecialty support utilizing academic partnerships. In urogynecology, a core team of collaborating international urogynecologists convened with our UB team to plan surgical and educational initiatives. Surgical visits are supported through a non-profit organization, Global Surgical Expeditions (GSE), that seeks to improve surgical access to LMIC. We planned two-week long urogynecology operating campaigns, two to three times per year. We also had quarterly virtual meetings between UB and GSE for patient preparation and logistic discussions. Beyond clinical education and patient care, these visits provided the opportunity for intensive in-person didactic sessions and simulation-based technical skill building. After each visit, we formulated a summary report of the total surgical cases, consults, and educational sessions completed. Finally, we engaged our regional collaboration with academic partners in South Africa to help to bolster our subspecialty exposure for residents. This was targeted especially for exposure to Reproductive Endocrinology and Infertility (REI), amongst the other OB/GYN subspecialties. We planned to have our chief residents rotate with subspecialty teams at the University of Stellenbosch during elective time in their final year. We also organized educational support from University of Pretoria and University of Cape Town for visiting lectures.
WELLNESS PROGRAMME FOR SUSTAINABILITY AND RETENTION
To prevent, recognize, and address burnout proactively, we developed a trainee-focused OB/GYN departmental wellness program. Drawing on research and recommendations from around the world, our wellness curriculum incorporated themes and tools centered around mindfulness, resiliency, gratitude, time management, dealing with adverse outcomes, and self-awareness. This curriculum was tailored to meet the unique needs and challenges of the OB/GYN profession in Botswana. Drawing on the guidance set forth by the Council on Resident Education in Obstetrics and Gynecology (CREOG), we additionally sought input from context- and culturally specific advisors. Local experts in coaching, counseling, and spiritual services were consulted in program planning, and participated in the sessions. The curriculum intended to bring awareness to mental health and burnout, provide better access to mental health services, and equip our OB/GYN trainees with tools that promote overall health and well-being, such as developing and strengthening resiliency. The sessions were integrated in the educational schedule monthly. Sessions lasted two hours each, and were delivered by faculty and some content experts, such as psychologists and wellness coaches (Table 4). In order to assess program efficacy, we anonymously surveyed attendees about factors related to wellness both before the start of the program, and after completion of all sessions.
Table 4: Wellness Session Topics
-
Introduction to Wellness
-
Empathy and Gratitude
-
Increasing Resilience
-
Managing Time and Priorities
-
Mission, Values, and Culture
-
Resident Retreat
-
Coping with Difficult Events and Debriefing
-
Psychological Safety and Team Communication
-
Wellness Feedback
CREOG Adapted
Results
MIS SIMULATION TRAINING
The MIS training was implemented in 2024. Of 18 enrolled residents, a total of 13 completed the training. Some residents built the homemade box trainer and practiced independently, while the others chose to work in teams of two to four resident groups. Of the participants, eight individuals completed all of the assigned tasks, self-administered assessments, and faculty observed skills. Survey data was available from 13 resident trainees. On self-administered assessments, the majority (92%, n=12) reported increased confidence in MIS skills after the training. Of the 13 enrolled residents, 11 completed faculty-observed skills assessments. All assessed trainees achieved competence in the observation (100% n=11). This included the eight trainees who completed the entire program, as well as the additional three residents who completed a portion of the online training. Surveys also reported that clinical case exposure increased after the training, effectively upscaling our MIS services (average case exposure before training 0–1 cases, average >5 cases per resident after).
ULTRASOUND TRAINING
Since the formal ultrasound training curriculum began, 25 trainees completed ISUOG modules, pre- and post-assessments, and image reviews. Trainees showed improvement of knowledge based on a pre- and post-assessment examination (52% vs 89%). All reported improvement with self-reported competence. This was substantiated by objective image acquisition assessment with scores improving in image capture after the educational intervention (64% to 94%). All trainees were found to have competency in basic OB/GYN ultrasound at the completion of the training through hands-on assessment from trainers, as well as through remote image review, with 100% achieving passing scores after training. Supporting in-person ultrasound training, five MFM fellows and two attendings have provided educational visits between 2022–2025. For sustained teaching, fellows visited for at least two months, and attendings for at least two weeks. Collaboration with the Queenan Global Health Program also led to an in-person ISUOG course in 2024, inviting nationally, and attended by 89 providers from across Botswana. Participants included UB faculty and residents from radiology, family and emergency medicine, as well as OB/GYN specialists, general medical officers, and midwives from the community. All attendees received certification. Education using the ultrasound simulator is on-going, and its impact on training still under investigation. To date, it has been used by twenty residents and three faculty. The POCUS training sessions were attended by 22 residents with trainings annually since 2023. Of those who attended, 11 completed post-course surveys. The majority of trainees reported increased confidence in their POCUS skills after the training (73% n=8), and reported increased use of POCUS in clinical care after training (81% n=9).
COLLABORATIONS
Since 2022, four US-based subspecialty faculty and two of their fellows have supported educationally intensive urogynecology surgical campaigns twice yearly. The number of urogynecology cases has increased with each visit. The teams have completed 144 surgeries and 216 clinic consults, with 40 trainees participating in lectures and simulations. GSE members have also provided remote lectures and coordinated surgical equipment donations. Four UB residents visited the University of Stellenbosch in South Africa for chief year electives, and the university invited our department to attend subspecialty lectures and grand rounds. University of Pretoria hosted an outreach conference in Botswana on MFM and other subspecialty topics in 2023. Since 2022, adjunct University of Cape Town faculty visited annually for lectures and laparoscopy training, enhancing REI and MIS education.
WELLNESS PROGRAM
Since the onset of the program in 2023, 35 participants attended ten wellness sessions over two years. Along with all residents and all faculty attending at least one session, some department interns, medical officers,
and specialists from the MOHW staff at PMH also attended. Anonymous surveys and direct feedback from trainees were positive. Residents and specialists enjoyed the sessions, and reported they used learned tools like mindfulness and breathing for stress management. Quantitative improvements were shown in pre/post-session feedback. Participants reported more skills for wellness (60% to 88%), a positive attitude (50% to 88%), and a sense of purpose at work (70% to 100%). They also felt improved focus on wellness at home (60% to 100%) and increased gratitude (40% to 77% at work, 60% to 100% at home). Resiliency also improved (40% to 88% at work, 60% to 88% at home).
Discussion
MIS SIMULATION TRAINING
While MIS case numbers are still rising, our AI-augmented simulation training program offers more skills practice than the small volume of in vivo cases allow. These simulations have excited trainees about MIS, and the department has gained consultants with MIS skills. International collaborations secured a gynaecology-specific laparoscopy tower. Faculty led simulated equipment setups with the theatre team, sensitizing them to these cases. Interested department MIS champions have also built additional simple MIS simulation models. We plan to share these with the SELF developers for open-access on their platform. Routine laparoscopy cases led by MIS-competent faculty are now weekly, and hysteroscopy was introduced. Twice yearly laparoscopy surgical campaigns accelerated momentum. Training in laparoscopy and hysteroscopy expand patient access and provide residents with MIS opportunities.
While the self-administered online MIS learning program encouraged skill-building, not all of our residents enrolled, and only about half of our residents ultimately finished the program in its entirety. They reported technology challenges and lack of time for practice. All except one of those who completed even portions of the training reported improved confidence, but all of them felt they needed more practice beyond the modules alone. All assessed residents were found to have achieved competence in their observed assessments; nevertheless, some still requested more training to feel confident enough to begin cases independently. Additional faculty support and hands-on training are needed to encourage these skills. In similar settings, incorporating didactics and simulation-based short courses in laparoscopy enhanced training benefits. As more surgeons become skilled in MIS, the rate-limiting step will shift from training to the system. Continued upscaling of the operating theater, including ongoing staff training and stocking of necessary items, is essential to support MIS. Efforts to limit consumables will reduce costs and logistic challenges. These operating theater practices, necessary due to limited resources in LMIC, can also be applied to more resourced settings to reduce surgical waste for environmental and financial sustainability. Finally, more efforts toward enhanced recovery and ambulatory surgery are needed for the benefit of the system and patients.
ULTRASOUND TRAINING
Ultrasound training, once confined to residents, has significantly improved diagnostic quality and patient access to clinical care, resulting in shorter waiting times. Senior residents, recent graduates, and experienced specialists now lead ultrasound training instruction at the bedside. After four years, the department became self-sustaining for sonography. In-person support has also allowed residents to learn ultrasound-guided procedures like amniocentesis. One of our trainees has created an amniocentesis simulation in collaboration with our visiting fellow and shared a video version of this online for ongoing training. International collaborations procured additional portable ultrasound machines, enabling daily and on-call use by residents, enhancing obstetric and POCUS skill practice; however, more high-quality ultrasound machines are needed due to the increasing demand for OB/GYN sonography. Improvements in handheld POCUS technology may address this issue. Ongoing quality assurance is also crucial.
engaged MFM specialists can facilitate virtual didactics, remote image review, and recruitment of additional subspecialty support. We plan to continue engaging with ISUOG as their AI-based online course technology enhances learning without on-site subspecialists. The ultrasound simulator is still under investigation as a training modality. Feedback from the first learners has been subjectively positive; however, formal assessment is ongoing. Research is needed to determine if ultrasound simulation can be used for ongoing performance assessments. Limited POCUS feedback has been positive, but on-going training and assessment is needed.
Expanded OB/GYN ultrasound and POCUS skills have excited faculty and residents, strengthened international partnerships, and encouraged interest in high-risk obstetrics. We are now conceiving the first steps of an MFM fellowship in Botswana using a hybrid model. Developing in-country subspecialty training tailored to context and resources will improve care beyond the scope of generalists. Leveraging partnerships and increasing resident and faculty skills will enable novel hybrid subspecialty training. Subspecialty care is also important for trainee retention and professional development in-country.
COLLABORATIONS
Our urogynecology training has thrived through our longitudinal international academic collaborations. The logistical operations surrounding these visits has been streamlined with residents coordinating evaluation of complex cases and preoperative consultation clinics with the urogynecologists. Trainee and faculty confidence has led to a monthly dedicated urogynecology clinic managed by senior residents under mentored faculty. This improves care and efficiency by quickly triaging patients, performing simpler urogynecologic surgeries, and collecting complex cases for subspecialist management. Continued remote dialogue on emerging cases has strengthened our collaborative effort. Faculty mentorship has improved, with specialists gaining novel or improved skills through daily attendance.
We now have faculty champions in vaginal surgery and perform increasing numbers of urogynecology cases without subspecialists present. Faculty and senior residents attend educational sessions to learn how to make and teach simulations for repeated use. Our quarterly calls have been optimized to improve trip planning, such as identifying benefits of multidisciplinary trips with anesthesia to boost operating theatre specialist staff and prevent disruptions to operating theatre workflow.
Despite funding limitations, elective placements with our regional partners provided valuable insights into other systems and quality improvement areas. Continued leveraging international partnerships to bridge training deficits in subspecialties like REI is crucial. REI training challenges include reliance on complex technologies like embryology labs for advanced reproductive technology. International academic partnerships and engagement with the private sector can bridge this gap. Our current public-private partnership provides students with exposure to more efficient and resourced systems, which could be expanded for future training needs.
Continued international elective opportunities depend on adequate funding for registration and travel. This training faces financial challenges and requires ongoing support from partners. A sustainable, equitable, and meaningful training exchange model is desirable. However, international bidirectional exchanges are limited by travel visa restrictions and licensing requirements restrict practice to basic observership. Advocacy to minimize these barriers and ongoing critical review of collaborative relationships are vital.
Infrastructure improvements and financial resource allocation are needed to ensure adequate staffing, equipment, and faculty positions for quality training and patient care. This model has proven successful in other parts of SSA and can retain and develop trainees into leaders within programmes. We must innovate to grow and expand sustainably. As educators, we recommend prioritizing targeted
OB/GYN subspecialty training. The MOH should collaborate with UB faculty to recruit subspecialists for service provision and training advancement.
WELLNESS PROGRAM
Our wellness program pilot successfully fostered a wellness culture among residents, who now lead sessions and suggest future objectives like financial wellness and creative expression. However, balancing these sessions with clinical, educational, and research responsibilities poses a challenge. While many attended some sessions, only a few attended all. Survey data was limited to half of attendees, and other departments and faculty were underrepresented. Collaboration is essential for broader culture change. Other UB residency departments have invited us to share wellness sessions. Plans include expanding wellness program elements to undergraduate medical students and UB faculty. Continued commitment to a wellness culture is crucial for preventing burnout and retaining excellent providers.
CONTINUOUS ASSESSMENT, EVOLVING NEEDS AND CHALLENGES
We integrated unique methodologies to fill training gaps for our OB/GYN programme in a LMIC setting. By collaborating and using technology, our trainees gain essential skills despite limitations. These novel methods aim to meet trainee needs, improve patient care, and enhance service access. Ongoing programme review continues to assess curriculum effectiveness. These innovative approaches are a start, offering many opportunities for expansion.
Other SSA programmes include long-term posts at rural hospital posts as part of training. We have begun limited rural outreach with the MOHW to reduce patient wait times and travel, expose residents to remote areas, and allow them to teach and lead. As specialists, they may serve these communities full-time after graduation, so outreach helps them understand rural patient and provider needs and appreciate the healthcare system more holistically. Outreach improves care locally by capacitating the local healthcare team to keep women at their facilities, allowing women delivery closer to their homes and support structures. For women who still need to transfer, familiarity and engagement between the transferring and accepting providers improve with a prior relationship of trust and support. Active inclusion in outreach posts as part of training will decentralize and disseminate academic knowledge and encourage engagement throughout the healthcare system. However, planning is needed to engage beyond monthly visits due to conflicting clinical and educational responsibilities. Optimizing visits by adding targeted education elements is necessary. Longer outreaches with surgical training and engagement with host facility healthcare providers are most desirable and impactful as resources permit. With improved staffing and partnerships, we hope to maximize resident educational benefit, faculty engagement, and local health system impact.
Balancing the MMED curriculum resident research requirement with clinical training is challenging. Residents are encouraged to choose topics with simple, novel approaches directly impacting patient care. Tangible research engages staff and encourages completion. Some resident theses include novel labor induction and magnesium sulfate administration techniques, and technology-based approaches for immediate postpartum intrauterine device retention. Faculty-led hospital quality improvement projects include innovative ideas, such as postpartum hemorrhage management prevention using the WHO E-MOTIVE approach, such as investigation of the use of a reusable, inexpensive uterine tamponade device, and tray for quantifying blood loss. Other department research includes implementation of the new WHO Labor Care Guide, especially respectful maternity care, addressing perinatal outcomes from a health equity approach. This uses the Checklist COPE: Companions, Oral fluids, Pain relief, and Eliminate the supine position. This reduced the proportion of patients who reported labor experience as “very bad” from 60% to 6%. Uptake of immediate post-pregnancy long-acting contraception was substantially increased through our ‘BACKUP’ quality improvement project.
projects include starting an outpatient sterilization surgical service, thereby training residents in MIS and reducing unplanned pregnancies to impact MM. Addressing practical hospital needs engages the healthcare team in research for success.
Conclusion
Thoughtful planning to address anticipated challenges has been vital from programme onset. New obstacles will always arise as the programme matures and trainee progress. Continued flexibility is needed, with programmatic additions and adjustments to meet dynamic training needs. We have found success in meeting challenges creatively. We remain open to finding dynamic and innovative solutions to meet ongoing training gaps. By sharing our experiences, we hope these innovations can benefit other training programmes regionally and globally. As our training needs shift, OB/GYN education that integrates diverse populations, technologies, and rapid knowledge expansion models is valuable as we reimagine how to train high-quality residents to meet the needs of our patients.
Conflicts of Interest:
The authors have no conflicts of interest to declare.
Funding Statement:
Intuitive Foundation funded the purchase of minimally invasive equipment. St Luke’s University Health Network and ISUOG provided access to a Volutracer OPUS ultrasound simulator. The SMFM Queenan Global Health program has funded visits for our MFM fellows. GSE funds travel for our visiting urogynecologists. We are grateful for your support.
Acknowledgements:
If you want to go fast, go alone; if you want to go far, go together. – African Proverb
Collaboration is the key to success and sustainability of our programme. The development, launch, and growth of the programme today could not have been possible without the continuing unwavering dedication of the University of Botswana Faculty of Medicine, the Ministry of Health and Wellness of Botswana, the Botswana Harvard Health Partnership, and the Department of OB/GYN, Division of Global and Community Health, at Beth Israel Deaconess Medical Center and Harvard Medical School for funding adjunct faculty support. Additional vital partners are Oregon Health Sciences University, Albert Einstein College of Medicine and Montefiore Einstein, St Luke’s University Health Network, Nuvance Health, the University of Stellenbosch Department of OB/GYN and Tygerberg Hospital, and University of Pretoria, all of whom have provided subspecialty training support. A special thanks to our MFM Queenan fellows Odessa Hamidi, Dr Lilly Liu, Dr Anar Gojayev, and Dr Laura Mroue. Additional appreciation to our GSE urogynecology collaborators, Dr Rahel Nardos, Dr Quinn Lippman, Dr Ian Fields, Dr Kimberly Kenne, and Dr Charles Nager. Additional thanks to Dr Femi Olarogun for providing REI and MIS education, and Professor Jorge Tolosa and Dr Daniela Febres-Cordero for ultrasound education. Finally, gratitude to Dr Kagiso Tlhabanela-David and Mme Chibengwe Pilane for supporting our wellness program through the UB Counseling Center
References
1. World Health Organization. Health workforce. Published 2025. Accessed April 2025.
https://www.who.int/health-topics/health-workforce#tab=tab_1
2. Ahmat A, Okoroafor SC, Kazanga I, et al. The health workforce status in the WHO African region: Findings of a cross-sectional study. BMJ Glob Health. 2022;7:e008317. doi:10.1136/bmjgh-2021-008317
3. Crisp N, Chen L. Global supply of health professionals. N Engl J Med. 2014;370:950-957. doi:10.1056/NEJMra1111610
4. Meara JG, Leather AJM, Hagander L, et al. Global Surgery 2030: evidence and solutions for achieving health, welfare, and economic development. Lancet. 2015;386(9993):569-624. doi:10.1016/S0140-6736(15)60160-X
5. Graham WJ. Diversity and divergence: the dynamic burden of poor maternal health. Lancet. 2016;388(10056):2164-2175. doi:10.1016/S0140-6736(16)31533-1
6. Powell BL, Luckett R, Bekele A, Chao TE. Sex disparities in the global burden of surgical disease. World J Surg. 2020;44:1231-1239.
7. Holmer H, Oyerinde K, Meara JG, et al. The global met need for emergency obstetric care: a systematic review. BJOG. 2014;122(2):183-192. doi:10.1111/1471-0528.13230
8. Martey JO, Hudson CN. Training specialists in the developing world: ten years on, a success story for West Africa. BJOG. 2005;112(2):177-179. doi:10.1111/j.1471-0528.1999.tb08206.x
9. Rager TL, et al. Growth model for international academic medicine partnerships: Qualitative analysis of Ghana postgraduate Ob/Gyn training program. PLOS Glob Public Health. 2023;3(1):e0000546. doi:10.1371/journal.pgph.0000546
10. Small M, et al. Increased Rwandan access to obstetrician-gynecologists through a U.S.-Rwanda academic training partnership. Obstet Gynecol. 2019;134(1):149-156. doi:10.1097/AOG.00000000 00003317
11. Bachan V, et al. The financial cost of physician emigration from sub-Saharan Africa. BMJ. 2011; 343:d6817. doi:10.1136/bmj.d6817
12. Clinton Y, Anderson FW, Kwawukume EY. Factors related to retention of postgraduate trainees in obstetrics-gynecology at the Korle-Bu Teaching Hospital in Ghana. J Acad Med. 2009; 84(10 Suppl):S93-S96. doi:10.1097/ACM.0b013e3 181f09112
13. Luckett R, Nassali M, et al. Development and launch of the first obstetrics and gynaecology master of medicine residency training programme in Botswana. BMC Med Educ. 2021;21:42. doi:10.11 86/s12909-020-02446-1
14. Gokcen E. Sustainable orthopaedic surgery residency training in East Africa: A 10-year experience in Kenya. J Am Acad Orthop Surg Glob Res Rev. 2019;3(7):e035. doi:10.5435/JAAOSGlobal-D-19-00035
15. Kendig C, Tyson A, Young S, et al. The impact of a new surgery residency program on case volume and case complexity in a sub-Saharan African hospital. J Surg Educ. 2015;72(1):94-99.
16. Baqain L. Post-graduate urology training in low- and middle-income countries. Uro. 2021;5(5):53.
17. McCullough MC. Google Glass for remote surgical tele-proctoring in low- and middle-income countries: A feasibility study from Mozambique. Plast Reconstr Surg Glob Open. 2018;6(12):e1999. doi:10.1097/GOX.0000000000001999
18. Chinyepi N, et al. Four-year overall surgical mortality rate at Princess Marina Hospital, a tertiary hospital in Botswana. J Public Health Afr. 2023; 14(3):2262. doi:10.4081/jphia.2023.2262
19. Wilkinson E, et al. Barriers to training in laparoscopic surgery in low- and middle-income countries: A systematic review. Trop Doct. 2021;51 (1):8-15. doi:10.1177/004947552199
20. Campain NJ, et al. An evaluation of the role of simulation training for teaching surgical skills in Sub-Saharan Africa. World J Surg. 2018;42(5):1272-1281. doi:10.1007/s00268-017-4261-7
21. Beard JH, Akoko L, Mwanga A, et al. Manual laparoscopic skills development using a low-cost trainer box in Tanzania. J Surg Educ. 2014 Jan-Feb;71(1):85-90. doi: 10.1016/j.jsurg.2013.06.005.
22. Lee W, Hodges AN, Williams S, et al. Fetal ultrasound training for obstetrics and gynecology residents. Obstet Gynecol. 2004;103(2):333-338. doi:10.1097/01.aog.0000109522.51314.5c
23. Alrahmani L, Codsi E, Borowski KS. The current state of ultrasound training in obstetrics and gynecology residency programs. J Ultrasound Med. 2018;37:2201-2207. doi:10.1002/jum.14570
24. Abuhamad A, Minton KK, Benson CB, et al. Obstetric and gynecologic ultrasound curriculum and competency assessment in residency training programs: Consensus report. J Ultrasound Med. 2018;37:19-50. doi:10.1002/jum.14519
25. Wheatley RG. Maternal critical care: What’s in a name? Int J Obstet Anesth. 2010;19(4):391-392. doi:10.1016/j.ijoa.2010.07.008
26. Edwards M. Is training in obstetric critical care adequate? An international comparison. Int J Obstet Anesth. 2018;36:71-72.
27. Algodi M, Wolfe DS, Taub CC. The Utility of Maternal Point of Care Ultrasound on Labor and Delivery Wards. J Cardiovasc Dev Dis. 2022;9(1): 29. doi: 10.3390/jcdd9010029.
28. Moore CL, Copel JA. Point-of-Care Ultrasonography. N Engl J Med. 2011;364:749–757. doi: 10.1056/NEJMra0909487.
29. Nding’ori D, et al. Improving health equity through sustained academic partnership: development of a maternal-fetal medicine fellowship training program in Western Kenya. AJOG Glob Rep. 2024;4(3):100362. doi:10.1016/j.xagr.2024.100362.
30. Kirubarajan A, Got T, Park B, et al. Interventions to prevent and treat burnout in obstetrics/ gynaecology: A scoping review. J Obstet Gynaecol Can. 2021;43(4):490–496. doi: 10.1016/j.jogc.202 0.12.011.
31. Iorga M, Socolov V, Muraru D, et al. Factors influencing burnout syndrome in obstetrics and gynecology physicians. Biomed Res Int. 2017; 2017:9318534. doi: 10.1155/2017/9318534.
32. Sinskey JL, Margolis RD, Vinson AE. The wicked problem of physician well-being. Anesthesiol Clin. 2022;40(2):213–223. doi: 10.1016/j.anclin.2022.0 1.001.
33. Patel RS, Bachu R, Adikey A,et al. Factors related to physician burnout and its consequences: A review. Behav Sci. 2018;8(11):98. doi: 10.3390/b s8110098.
34. Agyeman-Manu K. Prioritising the health and care workforce shortage: protect, invest, together. Lancet Glob Health. 2023;S2214-109X(23):00224-3. doi: 10.1016/S2214-109X(23)00224-3.
35. Workneh RS, Tuyishime E, Mumbwe M, et al. Not a “first world problem”—Care of the anesthetist in east and southern Africa. Pediatr Anesth. 2021; 31(1):39–43. doi: 10.1111/pan.14054.
36. Dzeng E, Curtis JR. Understanding ethical climate, moral distress, and burnout: A novel tool and a conceptual framework. BMJ Qual Saf. 2018; 27(10):766–770. doi: 10.1136/bmjqs-2018-007905.
37. Stabnick A. “Once you get one maternal death, it’s like the whole world is dropping on you”: experiences of managing maternal mortality amongst obstetric care providers in Ghana. BMC Pregnancy Childbirth. 2022;22:206. doi: 10.1186/s1 2884-022-04535-z.
38. Dubale BW, Friedman LE, Chemali Z, et al. Systematic review of burnout among healthcare providers in sub-Saharan Africa. BMC Public Health. 2019;19(1):1247. doi: 10.1186/s12889-019-7566-7.
39. West CP, Dyrbye LN, Sinsky C, et al. Resilience and burnout among physicians and the general US working population. JAMA Netw Open. 2020;3(7): e209385. doi: 10.1001/jamanetworkopen.2020.9385.
40. Ahart ER, Gilmer L, Tenpenny K, et al. Improving resident well-being: A narrative review of wellness curricula. Postgrad Med J. 2023;99(1173):679–686. doi: 10.1136/postgradmedj-2022-141541.
41. ALL-SAFE. African Laparoscopic Learners – Surgical Advancement for Ectopic Pregnancy. Training courses in laparoscopic surgery. 2025. Available at: www.allsafe.education
42. Obayemi JE, Ekeh AP, et al. The efficacy of a low-cost laparoscopic training curriculum for Nigerian surgeons. Glob Surg Educ. 2025;4:25. doi:10.100 7/s44186-024-00333-7
43. Hsu K, et al. Evidence for a case-based module in the low-resource setting to teach ectopic pregnancy management. Syst Implement Pract. 2023;2(1):10 0209. doi:10.1016/j.sipas.2023.100209
44. Queenan Global Health Awards. Society for Maternal-Fetal Medicine Foundation. Available at: foundationforsmfm.org/programs/queenan-global-health-awards
45. International Society of Ultrasound in Obstetrics and Gynecology (ISUOG). Basic training. Available at: www.isuog.org/education/basic-training1.html
46. Volutracer Opus. Available from: https://www.volutraceropus.com
47. Chawla L, Kumar R, Rajaram E, et al. Capacity building in obstetric ultrasound: Impact of simulation based clinical teaching on resident training at a health facility in India. Int J Obstet and Gynecol. 2025;169:267-273. doi.org/10.1002/ijgo.16076
48. American Institute of Ultrasound in Medicine. Point-of-care ultrasound. Available from:
https://www.aium.org/practice-topics/point-of-care-ultrasound.
49. Grimes CE, Maraka J, Kingsnorth AN, et al. Guidelines for surgeons on establishing projects in low-income countries. World J Surg. 2013;37:1203-1207.
50. Riviello R, Ozgediz D, Hsia RY, et al. Role of collaborative academic partnerships in surgical training, education, and provision. World J Surg. 2010;34:459-465.
51. Global Surgical Expedition. Available from: www.globalsurgicalexpedition.org.
52. Council on Resident Education in Obstetrics and Gynecology. Available from:
www.acog.org/education-and-events/creog/curriculum-resources/wellness-curriculum.
53. Boughizane S, et al. (2023, September 9) AAGL23 Pre-Congress Webinar: Necessity is the Mother of Invention – How Cost and Environmental Mindfulness May Help Improve the Future of MIGS. AAGL. Available from:
surgeryu.aagl.org/view?m=otnQvrSrO
54. Riad AM, Barry A, Knight SR, et al. Perioperative optimisation in low- and middle-income countries (LMICs): A systematic review and meta-analysis of enhanced recovery after surgery (ERAS). J Glob Health. 2023 Oct 3;13:04114. doi: 10.7189/jogh.1 3.04114.
55. Kulesa J, Brantuo NA. Barriers to decolonising educational partnerships in global health. BMJ Global Health. 2021;6:e006964.
56. Oti SO, Ncayiyana J. Decolonising global health: where are the Southern voices? BMJ Glob Health. 2021;6(7):e006576. doi: 10.1136/bmjgh-2021-006576.
57. Airborne Lifeline. Available from: airbornelifeline.org.
58. Miller J. No. 282-Rural Maternity Care. SOGC Reaffirmed Guidelines. 2017;39(12):E558-E565.
59. Committee on Health Care for Underserved Women. ACOG Committee Opinion No. 586: Health disparities in rural women. Obstet Gynecol. 2014;123(2 Pt 1):384-388. doi:10.1097/01.AOG.00 00443278.06393.d6
60. Matshitsa L, Nassali MN, Hofmeyr J. Extended balloon labour induction: A single arm proof of concept trial. Eur J Obstet Gynecol Reprod Biol X. 2023 Aug 13:19:100226. doi: 10.1016/j.eurox.202 3.100226.
61. Jamieson M, Luckett R, Hofmeyr GJ. Novel use of local analgesia prior to intramuscular magnesium sulphate injection compared to mixed local analgesia with magnesium sulfate to reduce pain: a randomized crossover study in patients being managed for eclampsia and preeclampsia. Frontiers in Pain Res. 2024 July 10. doi:10.3389/fpain.2024.1376608
62. Hofmeyr J, Kime K. Novel Concepts for Intrauterine Device Placement at Caesarean Delivery: Description of Technique and Video Recording. Obstet Gynecol Int. 2023 May 5;2023:4410984. doi:10.1155/2023/4410984
63. Singata-Madliki M, et al. Suction tube uterine tamponade versus uterine balloon tamponade for treatment of refractory postpartum hemorrhage: A randomized clinical feasibility trial. Int J Gynaecol Obstet. 2025 Jan 24. doi: 10.1002/ijgo.16164
64. Gallos I, et al. Randomized Trial of Early Detection and Treatment of Postpartum Hemorrhage. N Engl J Med. 2023 July 6;389(1):11-21. Doi: 10.1056/NEJMoa2303966.
65. World Health Organization. Labour care guide. Published 2021. Accessed April 2025. Available at: www.who.int/publications/i/item/9789240017566
66. Nassali MN, Russell JC, Tsuaneng M, et al. Promoting respectful maternity care with the WHO Labor Care Guide and the checklist mnemonic ‘COPE’: a quality improvement project. IJGO, accepted. DOI: 10.1002/ijgo.70238
67. Hofmeyr GJ, et al. Improving postpregnancy contraceptive method choice and long-acting reversible contraception provision in Botswana: a quality improvement pilot. BMJ Sex Reprod Health. 2023 Oct;49(4):293-297. doi: 10.1136/bmjsrh-2022-201748