






Institutional Capacity of LTCFs in China During COVID-19
Institutional Capacity of Long-Term Care Facilities in China During the COVID-19 Pandemic
Jun Zhang 1,2, Di Xiao3, Yushan Yu2, Jiehui Ren4, Xiaomei Pei1, Wei-Hong, Zhang2,5
- Research Center for Medical Sociology, Tsinghua University, Beijing, China
- International Centre for Reproductive Health (ICRH), Department of Public Health and Primary Care, Ghent University, Gent, Belgium
- Department of Comprehensive Maternal and Child Health, Guangzhou Women and Children’s Medical Center, Guangzhou Medical University, Guangdong Provincial Clinical Research Center for Child Health, Guangzhou, China
- Hebei University, Baoding, China
- School of Public Health, Université libre de Bruxelles (ULB), 1070 Brussels, Belgium
OPEN ACCESS
PUBLISHED: 31 January 2025
CITATION: Zhang, J., Di, X., et al., 2025. Institutional Capacity of Long-Term Care Facilities in China During the COVID-19 Pandemic. Medical Research Archives, [online] 13(1). https://doi.org/10.18103/mra.v13i1.6126
COPYRIGHT © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i1.6126
ISSN 2375-1924
ABSTRACT
Background: The coronavirus disease 2019 (COVID-19) pandemic has heavily impacted long-term care facilities (LTCFs) worldwide, resulting in extremely high infection and death rates within these settings. One major factor is the limited institutional capacity of long-term care facilities to respond effectively to such public health emergencies. However, there is limited research on this topic, especially concerning China. Therefore, this study seeks to examine the institutional capacities of long-term care facilities of China to better understand these challenges and identify measures for improving long-term care provision in future public health emergencies.
Objective: To assess the institutional capacity of Chinese long-term care facilities during public health emergencies.
Methods: A cross-sectional study collected data from 104 long-term care facilities across 20 provincial capitals or prefecture-level cities in China through questionnaires. Institutional capacity was measured with the social organization development index encompassing six dimensions: activity, resources, structure, environment, value and influence.
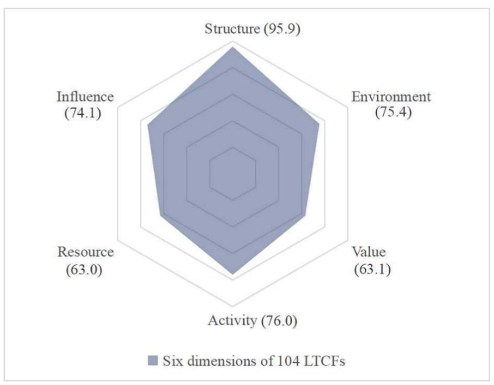
Results: Institutional capacity encompassing six dimensions showed scores of 76%, 63%, 95.9%, 75.4%, 63.1% and 74.1% in Activity, Resources, Structure, Environment, Value and Influence, respectively. These results indicate areas of strength, as well as notable gaps where improvements would be needed.
Conclusion: The social organization development index provides a comprehensive framework for assessing the institutional capacities of long-term care facilities and their roles during a public health crisis. The findings may offer insights into government policymaking related to the industry, particularly in enhancing institutional capacities to improve virus prevention and control during future public health emergencies.
Keywords: Institutional Capacity; Long-Term Care Facilities (LTCFs); Social Organization Development Index; Six dimensions; COVID-19; China
INTRODUCTION
COVID-19 pandemic has led to a significant high death rate among elderly population worldwide, especially among those in long-term care facilities (LTCFs). In the European region, the World Health Organization (WHO) reported that over 95% of COVID-19 fatalities were among individuals aged 60 and above. In North America, residents in these facilities faced a fivefold higher mortality risk than seniors living within the community. In the United States, the death rate of residents in LTCFs was over three times higher than the national average, and in Canada, deaths within LTCFs accounted for more than 80% of the country’s deaths. These facilities have thus emerged as epicenter of COVID-19, struggling to protect residents from severe outcomes associated with the virus’s morbidity and mortality.
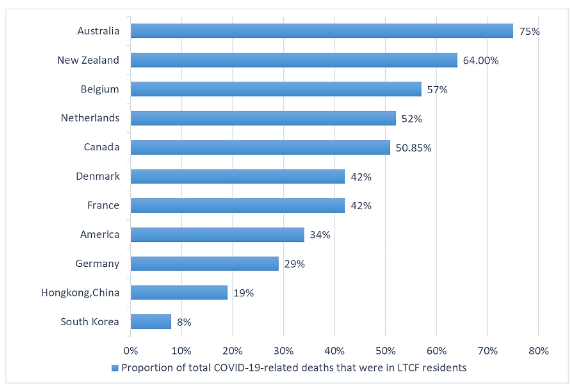
It has been globally recognized that long-term care facilities were “heavily impacted areas” of the COVID-19 pandemic, with mortality related to COVID-19 among their residents consistently exceeding that of the general population worldwide. COVID-19-related death rates in LTCFs have shown wide regional and international variation, ranging from 8% to 75% by early 2021. In Europe, COVID-19 related deaths exceeded 50% in Belgium and Netherlands, compared to less than 30% in Germany according to the European Centre for Disease Prevention and Control. In North America, LTCFs accounted for 50% of total deaths in Canada and 34% in the United States. Comparatively, Oceania reported higher death rates than Asia.
The pandemic also had a profound effect in China, particularly in Wuhan. The China Center for Disease Control and Prevention documented 82,545 COVID-19 cases in the first three months of the outbreak in 2020, with individuals aged 60 and older representing 30.2% of cases and accounting for over 80% of deaths, which indicated elderly were undoubtedly the most vulnerable group during the pandemic in China. These significant mortality differences across countries and regions highlighted that, in addition to acute medical interventions, the potential influence of preventive strategies on the outcomes in these facilities during public health emergencies. In many countries, the LTCFs residents faced higher risk due to the rapid spread of the COVID-19 virus. Infected individuals were mostly transferred to hospitals for treatment, while those remaining in the facilities, along with caregivers and staff, adhered to strict quarantine measures. Facilities with strict protocols reported lower infection rates compared to those that did not, as well as reduced rates of COVID-related hospitalizations and deaths.
The pandemic highlighted the need to examine the internal experience of these quarantined facilities and how the institutional factors, such as a strict lockdown measure, affecting the daily living of their residents and operational management. Moreover, given the responsibilities of health system governance, it became essential to examine the relationship between resource allocation and its impact on the operations of LTCFs during the COVID-19 pandemic.
Over the past three decades, China’s rapidly aging population has spurred significant growth of LTCFs, with over 34,000 facilities registered in the country by the end of 2019. This expansion bolstered institutional capacity, but the COVID-19 pandemic and subsequent quarantine requirements posed unforeseen challenges. Worse still, the prioritization of resources for hospitals and community prevention leaving LTCFs only with limited support, resulting these facilities encountered many management challenges, including shortages of critical supplies, personal protective equipment (PPE), diagnostic tests, and staffing etc. during the pandemic.
To understand how LTCFs adapted their risk management and managed the infection is also an added value for assessing the capacity of the healthcare system in aging societies. This study employs a comprehensive framework of institutional capacity to examine the resilience of Chinese LTCFs during the COVID-19 pandemic.
METHODS
DATA COLLECTION
Data were collected through questionnaire surveys using a standardized instrument designed to measure capacity building efforts of long-term care facilities during the pandemic. The questionnaire collected detailed information on resident demographic, facility characteristics, challenges encountered, the infection control measures implemented during the pandemic, as well as the current capacity-building efforts and outcomes. A convenience sampling approach was employed, collecting data from 104 LTCFs across 20 provincial capitals or prefecture-level cities in China between November 2020 to March 2021.
The questionnaire, intended for facility managers, was divided into four sections: 1) Characteristics of LTCFs (see Supplemental Table 1) 2) Characteristics of residents (see Supplemental Table 2) 3) Current status and challenges, measures implemented in LTCFs during the COVID-19 pandemic 4) Institutional capacity of nursing Measures.
Institutional capacity was evaluated using the Social Organization Development Index, encompassing six dimensions: activity, resource, structure, environment, value, and influence (United States Agency for International Development, 2021). Specifically, the availability of key services and resources at each LTCF were examined, including health assessments for residents, full-time psychological support, diagnostic and treatment facilities, exercise equipment, hospice services, hospital affiliations, collaborations with other agencies, social support funding, tax exemptions, and media support. Additionally, the survey also investigated the strategies for public image management, resource acquisition, and employee qualifications assessment at the LTCFs.
The availability of services and resources at the LTCFs were determined using binary codes, which “absent” (“no” = 0) and “present (“yes” = 1) were assigned. Specific factors evaluated included the presence of full-time psychological consultants, medical diagnostic and treatment facilities, exercise equipment, medical services, partnership agreement or with hospitals, telemedicine services, health and disease management for residents, hospice care, funding support, tax reductions or exemptions, media publicity, policy recommendations or proposals to governments or local authorities, cooperation with other agencies, and health assessment for the residents. Further areas of investigation included promotional slogan of LTCFs, resource demands, decision-making processes, conflict resolution methods, and organizational structures of the LTCFs.
Six dimensions
For each dimension different indicators were used to assess the institutional capacity, and the result of each dimension was calculated as the average of these indicators.
- Activity: Calculated by the average responses and activities undertaken by LTCFs across two phases: during the first outbreak (January 23 to April 7, 2020) and phased success in controlling (April 8 to June 30, 2020) of the COVID-19 pandemic.
- Resource: Measured based on the average score of the indicators of technical assistance, government and non-governmental organizations.
- Structure: Determined by averaging responses across organizational systems, encompassing staff employment, financial management, project management, and records management systems.
- Environment: Calculated by averaging factors such as tax exemptions, information and media support, and registration status.
- Value: Assessed through the average score of the indicators, identified as presence of corporate culture elements (e.g., mottos or slogans) and staff awareness, which encompassed the awareness levels of key leaders, internal staff, residents as well as the residents’ family and social support departments.
- Influence: Gauged by the average level of LTCFs’ promotional materials, media coverage, policy recommendations submitted to national or local government departments, and information exchange and resource-sharing initiatives with other LTCFs.
STATISTICAL ANALYSIS
Data were managed and analysed using Microsoft Excel 2017 and SPSS version 20.0 (IBM SPSS, Chicago, IL). Descriptive and univariable analyses were performed to identify LTCFs’ resident characteristics, current facility conditions, and COVID-19 pandemic related challenges.
RESULTS
Activity
Onset of 1st COVID Outbreak (January 23 to April 7, 2020)
Table 1 presents the responses and activities of LTCFs at different stages of the COVID-19 pandemic. At the onset of the outbreak (January 23 to April 7, 2020), 94.2% of the 104 LTCFs reviewed relevant policies and regulations issued by government and industries, and 96.1% established specific measures and detailed regulations. Additionally, 38.8% of LTCFs provided COVID-19 knowledge training for residents, while 44.7% offered similar training for staff. During this period, 71.8% of LTCFs organized cultural activities, and 91.4% facilitated residents to maintain interaction with families via video and phone calls. Social welfare activities, such as public education, were held by 61.2% of the facilities. Furthermore, 68.9% LTCFs carried out nucleic acid testing and 95.1% required residents to wear masks and undergo regular temperature checks. The average activity rate across these measures during the initial outbreak was calculated as follows: (94.2% + 96.1% + 38.8% + 44.7% + 71.8% + 91.4% + 61.2% + 68.9% + 95.1%) / 9 = 73.6%.
| Variables | 2020.01.23-04.07 | 2020.04.08-06.30 | P |
|---|---|---|---|
| Learn policies and regulations (issued by government and industries) | No 6 (5.8) | No 5 (4.9) | 0.757 |
| Yes 97 (94.2) | Yes 98 (95.1) | ||
| Missing data | 1 | 1 | |
| Formulate Measures and detailed rules | No 4 (3.9) | No 5 (4.9) | 0.733 |
| Yes 99 (96.1) | Yes 98 (95.1) | ||
| Missing data | 1 | 1 | |
| Carry out COVID-19 knowledge training for residents | No 63 (61.2) | No 61 (59.2) | 0.776 |
| Yes 40 (38.8) | Yes 42 (40.8) | ||
| Missing data | 1 | 1 | |
| Carry out COVID-19 knowledge training for staff | No 57 (55.3) | No 55 (53.4) | 0.780 |
| Yes 46 (44.7) | Yes 48 (46.6) | ||
| Missing data | 1 | 1 | |
| Conduct cultural activities | No 29 (28.2) | No 14 (13.6) | 0.010* |
| Yes 74 (71.8) | Yes 89 (86.4) | ||
| Missing data | 1 | 1 | |
| Allow interaction with family (via video and phone calls) | No 7 (6.8) | No 4 (3.9) | 0.353 |
| Yes 96 (91.4) | Yes 99 (96.1) | ||
| Missing data | 1 | 1 | |
| Organize social welfare (public education, etc.) | No 40 (38.8) | No 32 (31.1) | 0.242 |
| Yes 63 (61.2) | Yes 71 (68.9) | ||
| Missing data | 1 | 1 | |
| Provide COVID-19 nucleic acid testing | No 32 (31.1) | No 18 (17.5) | 0.023* |
| Yes 71 (68.9) | Yes 85 (82.5) | ||
| Missing data | 1 | 1 | |
| Require mask-wearing and temperature detection | No 5 (4.9) | No 2 (1.9) | 0.249 |
| Yes 98 (95.1) | Yes 101 (98.1) | ||
| Missing data | 1 | 1 |
The second period (April 8 to June 30, 2020) As China achieved phased success in controlling COVID-19, 95.1% of LTCFs reviewed policies and regulations issued by government and industry bodies and developed corresponding measures and detailed regulations. COVID-19 knowledge training was offered to residents by 40.8% of the facilities and to staff by 46.6%. Cultural activities were held by 86.4% of LTCFs, and 96.1% facilitated residents maintaining interactions with families through video and phone calls. Social welfare activities were held by 68.9% of the LTCFs, while 82.5% provided nucleic acid testing. Nearly all LTCFs (98.1%) enforced the practice of mask-wearing and temperature-checking. Hence, during this period the average activity rate was: (95.1% + 95.1% + 40.8% + 46.6% + 86.4% + 96.1% + 68.9% + 82.5% + 98.1%) / 9 = 78.4%.
The overall activity dimension, calculated by averaging levels across both stages, was 76%. In addition, the proportion of LTCFs conducting cultural activities and nucleic acid tests during the second period was significantly higher than that during the initial outbreak phase (P<0.05), while no statistical significance was found between the two stages in the activities carried out (P>0.05).
Resource
During the COVID-19 pandemic, LTCFs frequently encountered resource shortages, particularly in foundational support (55.9%), volunteers (48.0%), nurses (44.7%), non-governmental organization support (44.0%), information and media support (37.3%), government support (33.7%), technical support such as training (33.3%), and staffing (29.4%).
| Variables | Number | Proportion (%) |
|---|---|---|
| Foundation | Shortage 57 | 55.9 |
| Meeting needs basically 38 | 37.3 | |
| Meeting the needs 7 | 6.9 | |
| Missing data | 2 | |
| Staff | Shortage 30 | 29.4 |
| Meeting needs basically 61 | 59.8 | |
| Meeting the needs 11 | 10.8 | |
| Missing data | 2 | |
| Nurses | Shortage 46 | 44.7 |
| Meeting needs basically 48 | 46.6 | |
| Meeting the needs 9 | 8.7 | |
| Missing data | 1 | |
| Volunteers | Shortage 49 | 48.0 |
| Meeting needs basically 42 | 41.2 | |
| Meeting the needs 11 | 10.8 | |
| Missing data | 2 | |
| Technical support (e.g. training) | Shortage 34 | 33.3 |
| Meeting needs basically 59 | 57.8 | |
| Meeting the needs 9 | 8.8 | |
| Missing data | 2 | |
| Information and media | Shortage 38 | 37.3 |
| Meeting needs basically 57 | 55.9 | |
| Meeting the needs 7 | 6.9 | |
| Missing data | 2 | |
| Government support | Shortage 34 | 33.7 |
| Meeting needs basically 56 | 55.4 | |
| Meeting the needs 11 | 10.9 | |
| Missing data | 3 | |
| Non-governmental organization support | Shortage 44 | 44.0 |
| Meeting needs basically 49 | 49.0 | |
| Meeting the needs 7 | 7.0 | |
| Missing data | 4 |
Resources of LTCFs are evaluated based on the support they have received across different sectors. Results showed that 66.7% of the facilities received technical support and 66.3% received government support and 56% were supported by non-governmental organizations. Therefore, the average resources accessibility for LTCFs was: (66.7% + 66.3% + 56%) / 3 = 63%.
Structure
During the COVID-19 pandemic, LTCFs reported having clear and comprehensive systems in place for staff employment (96.2%), financial management (97.1%), project management (94.2%), and records management (96.0).
| Variables | None | Yes, but not clear | Yes, clear and complete |
|---|---|---|---|
| Staff employment system, n (%) | 2 (1.9) | 2 (1.9) | 100 (96.2) |
| Financial management system, n (%) | 1 (1.0) | 2 (1.9) | 101 (97.1) |
| Project Management system, n (%) | 2 (1.9) | 4 (3.8) | 98 (94.2) |
| Records management system, n (%) | 2 (1.9) | 2 (1.9) | 100 (96.0) |
Environment
Based on the quantitative questionnaire, 63.5% of LTCFs reported benefiting from tax exemptions, while 37.3% indicated a lack of information and media support. All LTCFs in the study were registered (100%). The calculated social environment score was: (63.5% + 62.7% + 100%) / 3 = 75.4%.
Value
In assessing the value of LTCFs, the highest awareness level regarding COVID-19 related knowledge was observed among internal staff (62.1%), followed by key leaders (61.2%), residents (57.3%), residents’ family members (35.9%), and social support departments (34.0%), resulting in an average awareness level of 50.1%. Furthermore, 76% of the LTCFs employed mottos or slogans, suggesting a focus on cultivating a corporate philosophy that highlights their values and vision. These mottos or slogans served as key elements of corporate culture and symbols of unity. Therefore, the average value of LTCFs was: (50.1% + 76%) / 2 = 63.1%.
Influence
Among the LTCFs in this study, 87.5% reported having their own promotional materials, and 88.5% reported media coverage of their activities, while 52.9% had made policy recommendations to national or local government departments, and 67.3% engaged in resources and information sharing with other LTCFs. Therefore, the average social impact of LTCFs was: (87.5% + 88.5% + 52.9% + 67.3%) / 4 = 74.1%.
The study revealed several key aspects of LTCFs’ institutional capacity in China as depicted in Figure 3.
DISCUSSION
In this study, the six dimensions – activity, resource, structure, environment, value, and influence – were measures across 104 LTCFs, with scores of 76%, 63%, 95.9%, 75.4%, 63.1% and 74.1%, respectively, highlighting both strengths and areas for improvement across the facilities.
Throughout the COVID-19 pandemic, LTCFs implemented various measures, including reviewing policies and regulations, introducing prevention and control measures, training residents and staff on COVID-19 related knowledge, organizing cultural activities, facilitating family interactions, providing public education, organizing nucleic acid testing, and enforcing mask-wearing and temperature checks. During the initial outbreak, the average LTCF activity score for LTCFs was 73.6%, which increased to 78.4% following China’s initial success in countering COVID-19. Besides, 76% of the LTCFs conducted various well-targeted activities aimed at combating the pandemic. According to the survey, these measures proved effective in preventing and controlling the virus spread as well as supporting residents’ health and well-being. This indicated that LTCFs effectively prioritized and executed their responsibilities. By comparing the figures before and after the COVID-19 pandemic, we found that LTCFs intensified their efforts in the prevention and control of the virus during the outbreak.
However, the study identified that resources received the lowest score among the six dimensions at 63%, pointing to a need for increased support in technical resources, government support, and NGO engagement. While government support was considerable significant, enhancing contribution from NGOs and volunteer involvement remained a critical area for further development.
The social impact of LTCFs has shown considerable improvement over time, reflecting an ongoing evolution in their role in society. The recent score of 74.1% in social impact indicates that LTCFs have made significant strides in policy advocacy, public relations, and industry integration, which were the keys for enhancing LTCFs’ social acceptance and public awareness of LTCFs’ role in providing care to the vulnerable population, especially the elderly and those with long-term health condition. However, additional efforts are required to further strengthen public awareness and acceptance, as well as to substantially enhance the media presence and informational support for LTCFs.
In addition, the assessment also revealed LTCFs generally had a well-defined corporate culture, as evidenced by the value score of 63.1%. This highlighted the importance of institutional values and areas for improvement. The high awareness level among leaders and staff underscored their professional knowledge and commitment to humanistic care. However, engagement with residents and their families was relatively modest, suggesting a need for enhanced communication with residents and their families, which could help LTCFs better understand residents’ backgrounds and health conditions, facilitating the provision of higher-quality care.
Moreover, staff awareness of LTCFs still needed reinforcement, especially in social support, where the LTCFs scored the lowest. To bridge this gap, the recommendation included strengthening public relations and promoting volunteer involvement in welfare activities. The prevalence of organizational mottos and slogans in LTCFs indicated a focus on cultivating a distinct philosophy aligning with their identity and service principles.
In the structure dimension, LTCFs showed strength with an average score of 95.9%, demonstrating robust system that benefited for both management and operations resilience during the COVID-19 crisis. Meanwhile, an environmental dimension score of 75.4% showed positive social support and recognition, though suggested a need of increasing volunteer participation and public awareness concerning LTCFs.
The capacity building assessment further identified significant gaps in certain areas. Specially 62.5% of the LTCFs reported a deficit in employing full-time counselling staff, highlighting the urgent need for strengthened mental health support. This was particularly critical during lockdown periods when residents were more likely to experience anxiety and other mental health challenges. Psychological counselling was essential support for ensuring residents’ compliance with the infection prevention and control measures.
Additionally, 43.3% of LTCFs lacked on-site medical diagnosis and treatment facilities, though 61.0% had established their own or affiliated age-care hospitals. Telemedicine connections facilitated prioritized (“green channel”) services with 80.8% of general hospitals. However, 78.6% of LTCFs had not set up general clinics within these partner hospitals, suggesting a gap in the integration of healthcare services.
While most LTCFs (91.3%) were equipped with physical exercise and rehabilitation equipment, showing a strong commitment to residents’ physical fitness and rehabilitation needs. Developing tailored prevention and rehabilitation programs for residents, based on their age, health conditions, and individual needs, could ensure that residents receive the most suitable and up-to-date services.
Furthermore, 81.7% of LTCFs indicated their capability in health and disease management for their residents, and 88.8% reported the capability for conducting physical health assessments for new admissions, allowing for customized care plans and appropriate fee structures. However, the study found that hospice care services were available in only 51.9% of the LTCFs. facilities. This highlights the critical need to expand and enhance hospice services, ensuring that end-of-life care is available to all residents who require it. Improved collaboration with medical institutions was recommended to provide residents with comprehensive support, including pain management and appropriate medication.
Limitations
This study acknowledged certain limitations. First, the small sample size might not fully represent the diverse landscape of LTCFs, potentially limiting the generalizability of the findings. In addition, the survey’s scope did not thoroughly address all aspects of LTCF operations, which restricted the understanding of their foundational situations. Given that this study primarily assessed the impact of closed management and the overall institutional capacity of LTCFs in China during the COVID-19 pandemic, future research should aim to expand both the detail and breadth of data collection. Furthermore, exploring the relationship between LTCFs’ capacity building and pandemic outcomes would be valuable in identifying effective and practical strategies for infectious diseases management within such settings.
CONCLUSIONS
The development of a six-dimension Social Organization Development Index has enabled a more systematic and comprehensive evaluation of the institutional capacity of LTCFs in managing public health emergencies. This framework has proven to be an invaluable tool for policymakers in designing targeted policies that address the specific needs of LTCFs effectively during public health crises.
Future research should focus on identifying strategies and methods to enhance medical services in LTCFs during pandemics, with particular emphasis on improving the integration of medical and hospice care. Strengthening these areas will be crucial in providing more holistic support to residents’ comprehensive needs.
Research Implications
Basing on the six dimensions and capacity building of the LTCFs, the government could develop a Social Organization Development Index to serve as a comprehensive framework for assessing the institutional capacity and role of LTCFs during public health crises. In addition, society should direct more attention and resource toward older adults in LTCFs, providing greater support and assistance for the growth and development of these facilities.
Finally, LTCFs should enhance collaboration with medical institutions, especially during the times of public health crisis.
Author Contributions
Study design: ZJ, ZWH; data collection: ZJ, R JH, YYS; data analysis: XD; study supervision: PXM, ZWH; manuscript writing: ZJ; critical revisions for important intellectual content: ZWH, ZJ, XD.
Funding Information
This research study was funded by the Tsinghua University Spring Breeze Foundation under Grant No: 20203080032.
Ethical Considerations
Data were collected, anonymized, and processed for analysis. The study was approved by the Institutional Review Board of Tsinghua University (No. 2020019). Participation was voluntary, with all participants fully informed about the purpose of this study.
Conflict of Interest Statement
The authors declare no conflict of interest.
Acknowledgments
The authors extend their sincere appreciation to all the participating long-term care facilities involved in this study.
Data Availability Statement
Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Table
Supplemental Table 1: Basic characteristics of participated long-term care facilities (LTCFs) (N=104).
| Variable | N (%) |
|---|---|
| Type of institutions | Government owned and operated 25(24.0) |
| Government owned but privately operated 21(20.2) | |
| Privately owned and operated 53(51.0) | |
| Privately owned but government supported 5 (4.8) | |
| Year of establishment time | 1950-1960 6(5.8) |
| 1961-1970 2(1.9) | |
| 1971-1980 1(1.0) | |
| 1981-1990 2(1.9) | |
| 1991-2000 5(4.9) | |
| 2001-2010 22(21.4) | |
| 2011-2020 65(63.1) | |
| Missing data | 1 |
| Geographical distribution | Eastern region 45(43.3) |
| Central region 40(38.5) | |
| Western region 19(18.3) | |
| Bed numbers | 32,101(100) |
| Bed occupancy rates, % (Mean±SD)a | 67.7±24.7 |
| Mode of Combination of Medical Treatment and Endowment | Hospitals run nursing homes 10(10.9) |
| Nursing homes run hospitals 19(20.7) | |
| Contract hospital services 36(39.1) | |
| Combination of medical care and health 27(29.3) | |
| Missing data | 12 |
| a Missing data =3 |
Supplemental Table 2: Characteristics of residents (N=19,914).
| Variables | Number | Proportion (%) |
|---|---|---|
| Residents | 19,914 | 100 |
| Gender | Male 8147 | 41.7 |
| Female 11,389 | 58.3 | |
| Missing data | 808 | |
| Age, year | 60 to 69 2413 | 13.7 |
| 69 to 79 4049 | 23.0 | |
| 80 to 89 8623 | 49.0 | |
| > 90 2505 | 14.2 | |
| Missing data | 2754 | |
| Physical condition | Self-reliant 6356 | 32.5 |
| Partial loss of self-care 5338 | 27.3 | |
| Unable to self-care 7887 | 40.3 | |
| Missing data | 808 |
Supplemental Table 3: The cognitive degree level for COVID-19 related knowledge of staff in long-term care facilities during the COVID-19 epidemic.
| Variables | Unclear | Not quite clear | Preliminary understanding | More familiar | Very familiar | Missing data |
|---|---|---|---|---|---|---|
| Key leaders, n (%) | 1 (1.0) | 3 (2.9) | 4 (3.9) | 32 (31.1) | 63 (61.2) | 1 |
| Internal staff, n (%) | 1 (1.0) | 3 (2.9) | 2 (1.9) | 33 (32.0) | 64 (62.1) | 1 |
| Residents, n (%) | 1 (1.0) | 3 (2.9) | 10 (9.7) | 30 (29.1) | 59 (57.3) | 1 |
| Residents’ family members, n (%) | 0 | 5 (4.9) | 19 (18.4) | 42 (40.8) | 37 (35.9) | 1 |
| Social support departments, n(%) | 2 (1.9) | 13 (12.6) | 30 (29.1) | 23 (22.3) | 35 (34.0) | 1 |
Supplemental Table 4: Characteristics of capacity of LTCFs during the COVID-19 epidemic (N=104)
| Variables | Number | Proportion (%) |
|---|---|---|
| Full-time psychological consultant | No 65 | 62.5 |
| Yes 39 | 37.5 | |
| Medical diagnostic and treatment facilities | No 45 | 43.3 |
| Yes 59 | 56.7 | |
| Physical exercise and rehabilitation equipment | No 9 | 8.7 |
| Yes 95 | 91.3 | |
| With medical qualification and establish care hospital | No 40 | 38.5 |
| Yes 64 | 61.5 | |
| Establishment of Medical Service Agreement with General Hospital (Green Channel) | No 20 | 19.2 |
| Yes 84 | 80.8 | |
| Telemedicine services | No 80 | 76.9 |
| Yes 24 | 23.1 | |
| Establish a general clinic with cooperative hospitals | No 82 | 78.8 |
| Yes 22 | 21.2 | |
| Health and disease management for residents | No 19 | 18.3 |
| Yes 85 | 81.7 | |
| Provide physical health assessment for the newly residents | No 11 | 11.2 |
| Yes 87 | 88.8 | |
| Missing data | 6 | |
| Provide palliative care (hospice care) services | No 50 | 48.1 |
| Yes 54 | 51.9 | |
| Enjoy tax relief treatment | No 19 | 18.3 |
| Yes 66 | 63.5 | |
| Unclear 19 | 18.3 |
Supplemental Table 5: The publicity status of long-term care facilities during the COVID-19 epidemic (N=104)
| Variables | Number | % |
|---|---|---|
| Information on the LTCFs’ own promotional materials | No 13 | 12.5 |
| Yes 91 | 87.5 | |
| Media coverage of activities organized by LTCFs | No 9 | 8.7 |
| Yes 92 | 88.5 | |
| Unclear 3 | 2.9 | |
| Make policy recommendations to the authorities of the state or local government | No 49 | 47.1 |
| Yes 55 | 52.9 | |
| Share resources and information with other LTCFs | No 33 | 32.7 |
| Yes 68 | 67.3 | |
| Missing data | 3 | |
| Top support for LTCFs | Media 11 | 11.3 |
| Academic community 11 | 11.3 | |
| Business authorities 71 | 73.2 | |
| Registration and annual review authorities 3 | 3.1 | |
| Other parts of government 1 | 1.0 | |
| Missing data | 7 | |
| Established motto or slogan for LTCFs | No 25 | 24.0 |
| Yes 79 | 76.0 |
References
- Kluge H. Older people are at highest risk from COVID-19, but all must act to prevent community spread. World Health Organization statement. Published April 3, 2020. https://www.who.int/europe/news/item/03-04-2020-statement-older-people-are-at-highest-risk-from-covid-19-but-all-must-act-to-prevent-community-spread.
- Fisman DN, et al. Risk factors associated with mortality among residents with coronavirus disease 2019 (COVID-19) in long-term care facilities in Ontario, Canada. JAMA Netw Open. 2020;3(7):e2015957. doi:10.1001/jamanetworkopen.2020.15957.
- Canadian Institute for Health Information. Long-term care and COVID-19: international comparisons. Published 2023. https://www.cihi.ca/en/long-term-care-and-covid-19-international-comparisons.
- Barnett ML, Grabowski DC. Nursing homes are ground zero for COVID-19 pandemic. JAMA Health Forum. 2020;1(3):e200369. doi:10.1001/jamahealthforum.2020.0369.
- Cronin CJ, Evans WN. Nursing home quality, COVID-19 deaths, and excess mortality. J Health Econ. 2022;82:102592. doi:10.1016/j.jhealeco.2022.102592.
- European Centre for Disease Prevention and Control. Surveillance data from public online national reports on COVID-19 in long-term care facilities. Published 2021. https://www.ecdc.europa.eu/en/all-topics-z/coronavirus/threats-and-outbreaks/covid-19/prevention-and-control/LTCF-data.
- Curiskis A, et al. What we know—and what we don’t know—about the impact of the pandemic on our most vulnerable community. Published 2021. https://covidtracking.com/analysis-updates/what-we-know-about-the-impact-of-the-pandemic-on-our-most-vulnerable-community.
- Comas-Herrera A, et al. Mortality associated with COVID-19 in care homes: international evidence. International Long-term Care Policy Network (ILPN); 2021.
- Lu Q, et al. Social policy responses to the Covid-19 crisis in China in 2020. Int J Environ Res Public Health. 2020;17(16):5597. doi:10.3390/ijerph17165597.
- Cazzoletti L, et al. Risk factors associated with nursing home COVID-19 outbreaks: a retrospective cohort study. Int J Environ Res Public Health. 2021;18(16):8696. doi:10.3390/ijerph18168696.
- Li Z. How can private elderly care institutions get out of the epidemic “swamp” after their income plummeted by 20%. Published April 29, 2020. https://m.gmw.cn/baijia/2020-04/29/33794113.html.
- Dykgraaf SH, et al. Protecting nursing homes and long-term care facilities from COVID-19: a rapid review of international evidence. J Am Med Dir Assoc. 2021;22(10):1969-1988. doi:10.1016/j.jamda.2021.06.027.
- Ham C. A home by any other name: building an understanding of infection prevention in small residential care facilities. Public Policy & Aging Report. 2022;32(4):140-145.
- Létourneau J, et al. Identifying performance factors of long-term care facilities in the context of the COVID-19 pandemic: a scoping review protocol. Syst Rev. 2022;11(1):203. doi:10.1186/s13643-022-01975-6.
- Fleming SP, et al. COVID-19 cases, hospitalizations, and deaths in nursing homes: factors impacting the second surge. Innov Aging. 2021;5:15-16.
- Yin C, et al. Factors associated with nursing home residents’ COVID-19 infections: a systematic review of literature. Innov Aging. 2021;5:16-16.
- Ministry of Civil Affairs of the People’s Republic of China. China Civil Affairs Statistical Yearbook. Beijing, China: China Social Press; 2020.
- Frank L, Concannon T, Patel K. Health care resource allocation decision-making during a pandemic. Santa Monica, CA: RAND Corporation; 2020.
- Abbasi J. “Abandoned” nursing homes continue to face critical supply and staff shortages as COVID-19 toll has mounted. JAMA. 2020;324(2):123-125.
- United States Agency for International Development. Organizational performance index: definitions and measurements. https://pdf.usaid.gov/pdf_docs/PA00XM82.pdf.