

Interdisciplinary Approach to Radicular Cyst Management
Interdisciplinary Management of an Extensive Radicular Cyst in the Anterior Mandible Using Cone Beam Computed Tomography, Biopsy, and Guided Bone Regeneration: A Case Report
Ahmad Soolari1, DMD, MS, Adjunct Professor
- West Virginia University, Department of Periodontics, School of Dentistry
OPEN ACCESS
PUBLISHED 28 February 2026
CITATION Soolari, A., 2026. Interdisciplinary Management of an Extensive Radicular Cyst in the Anterior Mandible Using Cone Beam Computed Tomography, Biopsy, and Guided Bone Regeneration: A Case Report. Medical Research Archives, [online] 14(2).
COPYRIGHT © 2026 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
ISSN 2375-1924
ABSTRACT
Large periapical lesions in the anterior mandible present significant diagnostic and therapeutic challenges due to their proximity to vital structures and the potential for extensive alveolar bone loss. This case report describes the management of a 58-year-old African American female with a large radicular cyst associated with tooth #26. Utilizing Cone Beam Computed Tomography and histopathological biopsy, a definitive diagnosis was established while ruling out more aggressive neoplastic entities. The treatment involved the extraction of the non-vital tooth #26 and tooth #30, while successfully preserving the vitality of the adjacent tooth #27 through periodontal regenerative therapy and Guided Bone Regeneration. A 6-month follow-up revealed significant bone fill and stabilization of the anterior segment. This case underscores the “team approach” between referring and treating clinicians in prioritizing biological preservation over aggressive extraction and dental implant placement.
Keywords: Radicular Cyst, Cone Beam Computed Tomography, Biopsy, Guided Bone Regeneration, Tooth Preservation, Interdisciplinary Dentistry.
1. Introduction
The management of large radiolucent lesions in the jaw requires a meticulous diagnostic protocol to differentiate between inflammatory, developmental, and neoplastic entities. Radicular cysts are the most common inflammatory odontogenic cysts, typically arising from the epithelial rests of Malassez as a result of pulp necrosis. In the anterior mandible—a region critical for both esthetics and function—large lesions pose a specific risk to the biological and mechanical stability of the alveolar ridge. Traditional two-dimensional periapical radiography often fails to capture the true volumetric extent of such defects, particularly regarding the involvement of the lingual cortical plate or the proximity to the mental foramen. Furthermore, clinicians must navigate a complex differential diagnosis in middle-aged African American females, where periapical cemento-osseous dysplasia frequently mimics the appearance of inflammatory periapical pathology. While dental implants are often presented as the primary solution for tooth loss, the rising incidence of implant-related complications has sparked a renewed interest in tooth preservation and the “interdisciplinary approach” to disease arrest.
2. Case Presentation
2.1 CLINICAL AND RADIOGRAPHIC EVALUATION
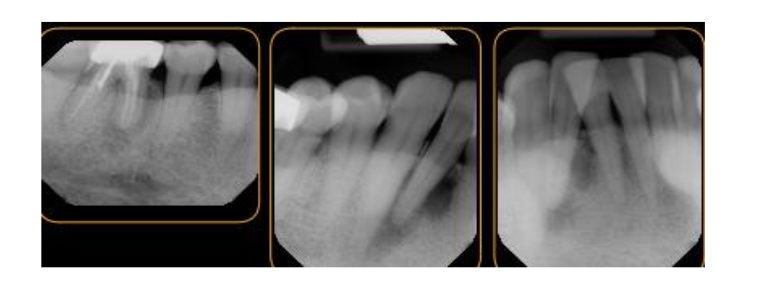
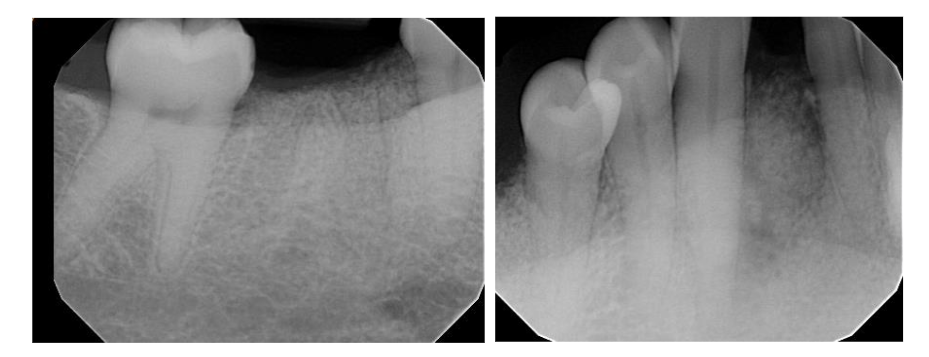
A 58-year-old African American female was referred for the evaluation of localized pain and swelling associated with the mandibular anterior segment. Clinical examination revealed a slight buccal expansion and localized distress at tooth #26. Initial two-dimensional radiographic examination disclosed a large, well-circumscribed radiolucency extending from the alveolar ridge to the apices of teeth #26 and #27. Vitality testing was performed:
- Tooth #27: Responded positively to cold and electric pulp testing (vital).
- Tooth #26: Responded negatively (non-vital).
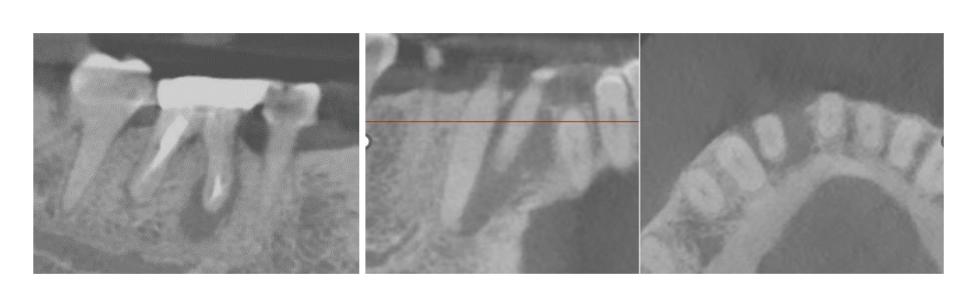
2.2 ADVANCED DIAGNOSTICS: CONE BEAM COMPUTED TOMOGRAPHY AND BIOPSY
An in-office Cone Beam Computed Tomography (CBCT) scan was performed to assess the three-dimensional dimensions of the defect. The scan disclosed a periapical low-density area originating from #26 and extending from the apex to the level of the alveolar crest. It further involved the apical foramen of the adjacent vital tooth #27. Based on the CBCT findings, the prognosis for #26 was determined to be poor. Additionally, an incidental endodontic failure was identified on tooth #30, requiring extraction. Given the lesion’s size and the patient’s demographic, a biopsy was deemed mandatory to rule out tumor formation or malignancy.
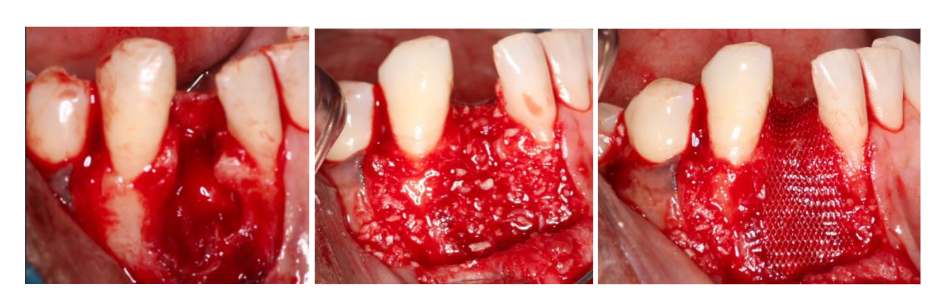
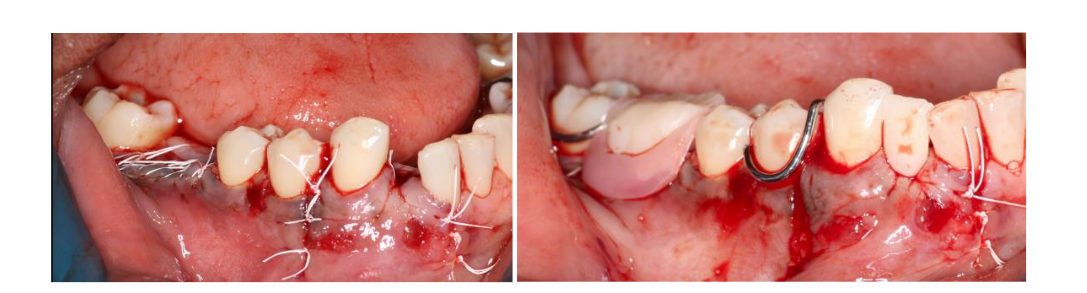
2.3 SURGICAL EXECUTION AND RECONSTRUCTION
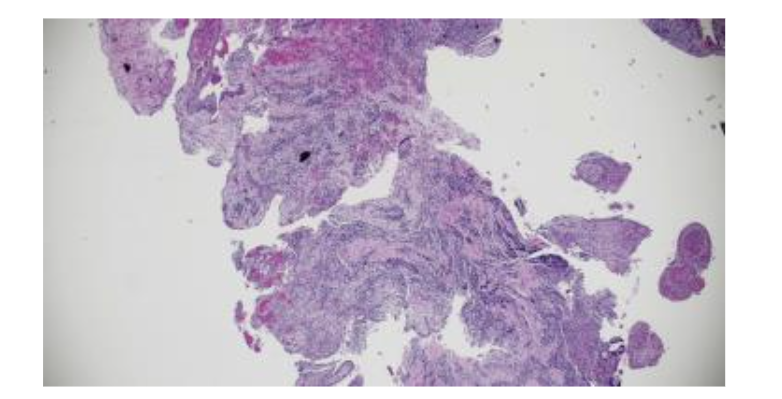
The patient accepted a plan prioritizing the preservation of tooth #27. Following flap elevation, the entire lesion was enucleated and submitted for histopathological analysis. To manage the extensive bony defect and prevent soft tissue collapse, Guided Bone Regeneration (GBR) and Periodontal Regenerative Therapy (PRT) were performed. The defect was filled with a bone allograft scaffold and covered with a barrier membrane to facilitate osteoconduction prior to tension-free primary closure.
3. Discussion
3.1 DIAGNOSTIC COMPLEXITY AND THE UTILITY OF THREE-DIMENSIONAL IMAGING
The use of CBCT in this case provided a definitive advantage over conventional imaging. As noted by Elhakim et al., preserving the vitality of adjacent teeth during the management of large cysts is dependent on understanding the precise spatial relationship between the lesion and the neighboring roots. CBCT allows the surgeon to visualize the “safety zone” around vital teeth, ensuring the blood supply to tooth #27 was not compromised during enucleation. The differential diagnosis was a critical component of this case. In African American females, Periapical Cemento-Osseous Dysplasia (PCOD) must be ruled out; in PCOD, the teeth remain vital and surgical intervention is contraindicated. The non-vital response of #26 and the subsequent biopsy confirmed the diagnosis of a Radicular Cyst (K04.8), characterized by a stratified squamous epithelial lining and chronic inflammatory infiltrate. Distinguishing this from a Lateral Periodontal Cyst (LPC) or Odontogenic Keratocyst (OKC) is vital, as the latter carries a higher recurrence rate and requires different surgical management.
3.2 REGENERATIVE BIOLOGY: GUIDED BONE REGENERATION VS. IMPLANT REPLACEMENT
The clinical success of this case, evidenced by complete bone fill at the 6-month follow-up, validates the use of GBR in large cystic cavities. Ramalingam et al. have demonstrated that bioactive scaffolds can successfully fill large mandibular voids, facilitating the body’s natural healing capacity. Choosing to regenerate the bone and save tooth #27 rather than performing multiple extractions for implants aligns with the evidence-based findings of Chaush, G and Kim K regarding the superior long-term success of tooth preservation. Afrashtehfar K further supports this by highlighting the cost-effectiveness of preservation over the rising costs of managing implant complications.
4. Conclusion
This case demonstrates that the “team approach” between the referring doctor and the specialist creates a pathway for comfortable, predictable outcomes. By utilizing CBCT and biopsy, clinicians can provide personalized care that arrests disease without the premature loss of healthy adjacent teeth. The patient remains happy and healthy, with the natural dentition preserved and the bone architecture fully restored.

5. References:
- Kerezoudis NP, Donta-Bakoyianni C, Siskos G. The lateral periodontal cyst: aetiology, clinical significance and diagnosis. Endod Dent Traumatol. 2000;16(4):144-150.
- Mireles JCG, Siqueira JF Jr, Ricucci D. Microsurgical management of radicular cyst using guided tissue regeneration technique: A case report. World J Clin Cases. 2024;12(7):1346-1355.
- Murugesan I, Et al. Bone Trabecular Pattern Analysis in Odontogenic Cysts Using Cone Beam Computed Tomography: A Clinical Retrospective Study. Cureus 2024 Feb 19;16(2)e54452.
- MacDonald D. Cemento-osseous dysplasia: an updated review. Dentomaxillofac Radiol. 2015;44(1):20140322.
- Sartoretto SC, Calasans-Maia J, Costa MF, et al. Comparing the long-term success rates of tooth preservation and dental implants: a critical review. J Funct Biomater. 2023;14(3):142.
- Nagpal D, Garlapati D, Chhabra V, Chhabra A. The cost-effectiveness of tooth preservation vs implant placement in severe periodontal disease patients: a systematic review. Quintessence Int. 2024;55(1):76-85.
- Bornstein MM, Scarfe WC, Vaughn VM, Jacobs R. Cone beam computed tomography in endodontics: a review of the literature. Int Endod J. 2014;47(2):103-127.
- Stoor P, Apajalahti S, Kontio R. Regeneration of cystic bone cavities and bone defects with bioactive glass S53P4 in the upper and lower jaws. J Craniofac Surg. 2017;28(5):1197-1205.
- Salaria SK, Ghai AS, Gaba R, Garg S. Periodontal regenerative management of residual tunnel osseous defect results from the enucleation of lateral periodontal cyst in anterior maxilla: A rare case report. J Indian Soc Periodontol. 2016;20(6):638-642.
- Elhakim A, Kim S, Grawish ME. Preserving the vitality of teeth adjacent to a large radicular cyst in periapical microsurgery: a case report with 4-year follow-up. BMC Oral Health. 2021;21(1):382.
- Barbirato DSB, Et al. Lateral periodontal cyst: A rare clinicopathological presentation mimicking a residual cyst. J Clin Exp Dent. 2022 Jan 1;14(1):e95-e99.
- Ramalingam S, Al-Qahtani AS, Al-Hindi M, et al. Lateral periodontal cyst treated with enucleation and guided bone regeneration: a report of a case and a review of pertinent literature. Case Rep Dent. 2019;2019:4591019.
- Chaush G, Parvanov S, Chaush M. Use of a resorbable magnesium membrane for bone regeneration after large radicular cyst removal: a clinical case report. Healthcare (Basel). 2025;13(9):1068.
- Kim K, Lee CH, Li RK, et al. Guided bone regeneration using barrier membrane in dental applications. ACS Biomater Sci Eng. 2023;9(10):5457-5478.
- Afrashtehfar K, Et al. Maintaining periodontally compromised teeth seems more cost-effective than replacing them with dental implants. Evi Based Dent. 2024 Sep;25(3):129-130.