





Interprofessional Education in Brazilian Health Care
STATE OF INTERPROFESSIONALITY IN BRAZIL: practical applications and challenges for interprofessional education in health
Adélia Delfina da Motta Silva DDS¹, Roberta Rios Soares MD², Maria Auxiliadora Budib MD¹, Tatiana Serra da Cruz MD¹, Rodrigo Guimarães dos Santos Almeida RN³
- Master Professor at the Faculty of Medicine, Federal University of Mato Grosso do Sul (UFMS), Campo Grande, Mato Grosso do Sul, Brazil
- Family and Community Physician, through the Family and Community Medicine Residency Program, Federal University of Mato Grosso do Sul (UFMS), Campo Grande, Mato Grosso do Sul, Brazil
- PhD Professor at the Ribeirão Preto School Nursing, University of São Paulo (USP), Ribeirão Preto, São Paulo, Brazil
OPEN ACCESS
PUBLISHED: 30 April 2025
CITATION: da Motta Silva, A. D., et al., 2025.
STATE OF INTERPROFESSIONALITY IN BRAZIL: practical applications and challenges for interprofessional education in health. Medical Research Archives, [online] 13(4).
https://doi.org/10.18103/mra.v13i4.6503
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i4.6503
ISSN 2375-1924
ABSTRACT
Interprofessionality, defined as the collaborative practice between health professionals from different professions, is essential for health education and performance in Brazil, especially in the context of the Unified Health System (SUS). This study addresses interprofessional education (IPE) and interprofessional collaborative practices (IPC), highlighting experiences, advances, and challenges in the country. Interprofessional education promotes joint learning between professions, developing collaborative skills to improve the quality of care, and comprehensiveness of health care. This work is the result of an integrative literature review, with a qualitative approach, following the six stages of the method, using the PRISMA tool, to answer the following guiding question: “What are the practical applications and challenges for interprofessional education in health in Brazil?”.
The used descriptors were “interprofessionality” / “interprofessionality in health” in the Scientific Electronic Library Online – SciELO Brazil database, on February 18, 2025, since our focus was on Brazilian experiences. After applying the methodology, 37 references were incorporated by their proposal coherence. Since 2010, the World Health Organization (WHO) has encouraged interprofessional education as a strategy to strengthen health systems, which has become a milestone for interprofessional education in Brazil. One of the change-inducing initiatives that has stimulated IPE is the Education through Work for Health Program (PET-Health), which has played a crucial role in bringing about changes in health education, promoting collaborative practices, and teaching-service-community integration. Experiences such as that of the Federal University of São Paulo (Unifesp) on the Baixada Santista campus demonstrate the potential of interprofessional education to transform curricula and practices, aligning them with the needs of SUS.
Despite the advances, however, challenges persist, such as the predominance of uniprofessional training and the resistance to the inclusion of interprofessionality in the curricula. The effective implementation of interprofessional education requires structural changes in health courses, teacher training, and institutional support. Devices such as the Singular Therapeutic Project (PTS) and user embracement stand out as practical tools to promote interprofessionality in care in practice scenarios. It is concluded that interprofessionality is fundamental for the consolidation of SUS, requiring continuous efforts to integrate interprofessional education into health curricula and practices, with a focus on collaboration, humanization, and user-centered care.
Keywords: Unified Health System, National Health Strategies, Interprofessional Education (IPE), Health Human Resource Training, Permanent Education.
Introduction
In 2005, D’Amour and Oandasan¹ defined Interprofessionality “as the development of a cohesive practice between professionals from different disciplines. It is the process by which professionals reflect on and develop ways of practicing that provides an integrated and cohesive answer to the needs of the client/family/population”.¹(p.9)
According to Cecim², the notoriety that the term Interprofessionality has gained in recent years is still permeated by the confusion of words used in the health sector, being mistakenly thought as a synonym for “multiprofessionality”, “multidisciplinarity” and “interdisciplinarity”.
In this aspect, it is common to identify the words discipline and profession, with the juxtaposition of different prefixes, among which “uni-“, “multi-“, “pluri-“, “inter-“, “trans-“, elaborating concepts whose essential difference concerns the degree of aggregation, exchanges and articulation between disciplines or professions.³˒⁴
Thus, before starting this discussion, it was considered important to understand that, in Brazil, according to Rosa et al.⁴(p.11): “uniprofessional refers to the process in which the knowledge of an area of knowledge predominates. Multi and pluriprofessional knowledge refers to the process in which there is a certain coordination between disciplines. Interprofessionality, on the other hand, occurs when professionals learn from each other and about each other, and transprofessionality is placed at a higher stage, characterizing the fusion of certain fields of knowledge. Furthermore, the concept of teamwork is characterized as complementarity of practices while collaboration has a sense of cooperation”.
And teamwork, so important to the Brazilian Unified Health System (SUS), precisely implies this: sharing each other’s knowledge, to expand the set of competencies and the capacity to respond to health care. Thus, Interprofessionality in health enhances care by promoting “patient safety, comprehensive care, humanization of practices and the promotion of relief (comfort and well-being) for workers”.²(p.1741)
It is fundamental, therefore, to demarcate that when one speaks of profession, one speaks of “a cut of craft, of power and of the formal exercise of an occupation”, and when one addresses discipline, one is talking about a “cut or domain of technical or scientific information”.²(p.1740) Also considering the prefix “inter-” while within, within two (or more), when addressing Interprofessionality, we are talking about the encounter or intersection between professions, resulting in a set of common elements between them. It is essential to understand that for the exercise of Interprofessionality it is necessary to make use of interdisciplinary knowledge, which includes “knowledge from various sciences, popular knowledge and tacit knowledge”, as well as interprofessional competencies, “the skills systematized in professions, the actions organized in professional aptitudes”.²(p.1741)
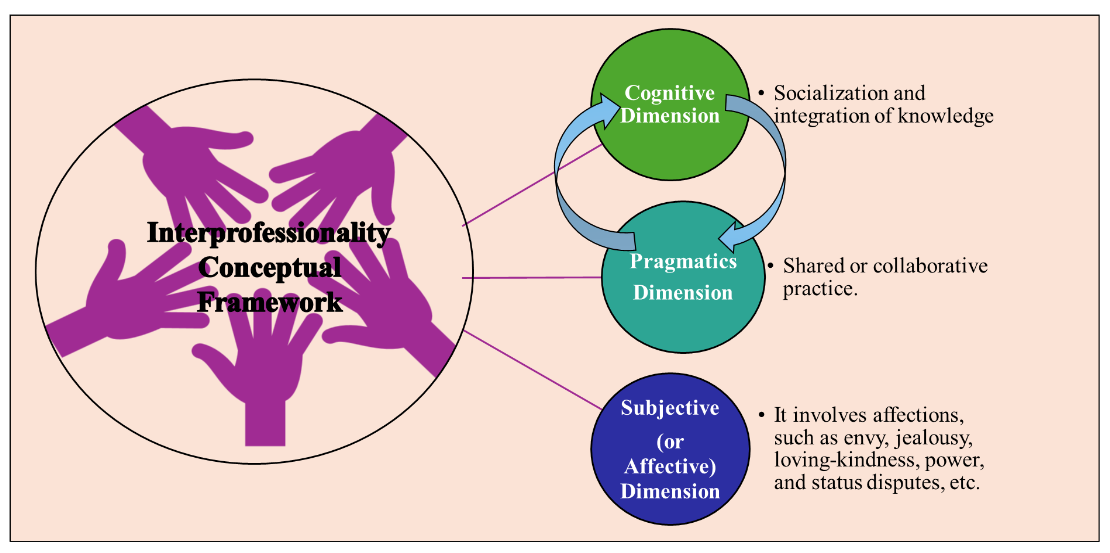
For Ellery⁵, three dimensions of Interprofessionality need to be considered for the conformation of its conceptual structure, as can be seen in Figure 1. For Ellery⁵, Interprofessionality is a work process that emerges from the combination of cognitive, pragmatic, and subjective processes, experienced and put into practice by professionals of the same category and of different professional categories, who work together.
In addition, Interprofessionality is aligned with the fundamental principles of SUS, such as integrality of care, user centricity, teamwork, and organization of health systems, focusing on people’s health needs, families and communities’ health needs, reinforcing the complementarity between training and health work. The research emphasizes interprofessional education, defined as the process in which members of diverse professions learn together in an interactive way to improve collaboration and quality of care.
In this sense, interprofessional education favors the sharing of knowledge, the understanding of values.and respect for the roles of health professionals, in addition to articulating specific competencies in collaborative practice. It articulates new training arrangements and develops a collaborative environment, promoting interactive learning to form interprofessional skills.
From Ellery’s perspective⁵˒⁷, it is necessary to understand that professionals with different academic backgrounds, working together, do not automatically transform into a team, which produces interprofessional, collaborative work that produces comprehensive care. In addition, in health work, professionals are affected by each other, which can expand the methods of seeing and interpreting the phenomena. If the practice is collaborative, the professionals’ resort both to their specific core of action and to building a common field of intervention, where the practices are shared, dependent of knowledge core. In fact, this interprofessional common field “lives in permanent agreement, as new knowledge and practices are incorporated”⁵(p.150) into health care.
Obviously, this conceptual discussion is not exhausted here, but it was considered essential to clearly bring, from the beginning of our study, which Interprofessionality we are talking about.
Thus, this article intends to address the state of Interprofessionality in Brazil, addressing interprofessional education (IPE) in health and the interprofessional collaborative practices (ICP) experienced in the country, as well as the challenges to advance in its institutionalization and consolidation.
Methodology
Our study is the result of an integrative literature review⁸, with a qualitative approach, following the six stages of the method (establishment of the hypothesis and objectives, criteria for inclusion and exclusion of articles, definition of the information to be extracted from the selected articles, analysis of the results, discussion, and presentation of the results)⁸, using the PRISMA tool⁹, to answer the following guiding question: “What are the practical applications and challenges for interprofessional education in health in Brazil?”. The used descriptors were “interprofessionality” / “interprofessionality in health” in the SciELO (Scientific Electronic Library Online) Brazil database, on February 18, 2025, since our focus was on Brazilian experiences.
The inclusion criteria considered articles, published since 2010, of open access, in Portuguese, English, or Spanish, which provided an answer to the research question. The year 2010 was chosen because it is a milestone for Interprofessionality and Interprofessional Education for Brazil, with the publication of PAHO¹⁰. The first search resulted in 78 selected references. The first check was made in the database, and the repeated references were excluded (five). It used the software Mendeley Reference Manager for the deletion steps, and for the management and proper citation of the references used, its Mendeley Cite plug-in for text applications.¹¹ The categorization was made into three major themes, as shown in the results. For this, the titles and abstracts were dynamically read, and later, the 25 selected articles were read in full and all included in the review, and some of them brought 12 new literatures – such as official documents from PAHO, the Brazilian government and other key-articles/publications for the theme – totaling 37 references incorporated by their proposal coherence.
As we seek, especially in the discussions, to confront the literature with our experience in the area, we can classify this article much more as an academic essay on Interprofessionality in Brazil.
Results and Discussion
There were used 37 references to compose the context of the state of Interprofessionality in Health in Brazil, organized into three major topics: the first which brings a general notion of the art state on interprofessional education in undergraduate health courses; the second addresses the PET-Health Program, its role in inducing changes; and the third, the challenges in training for Interprofessionality in health practice as well as Brazilian experiences.
INTERPROFESSIONALITY IN BRAZIL: THE STATE OF THE ART IN UNDERGRADUATE HEALTH
Improving collaboration and the quality of health care and services has been the focus of interprofessional education by bringing two or more professions together to learn about each other and their professions, support each other, and share resources.
It is understood, therefore, that interprofessional education is not a content or a technique to be taught, but the training for the development of competencies for interprofessional work during mutual learning, with the attitudes acquisition guided by interpersonal interactions for teamwork, respect for ethical values, definition of roles for adequate decision-making, effectiveness in interprofessional communication, so that it is possible; finally, through the encounter of co-produced knowledge, to focus attention on the patient, the family and the community, to meet their needs with greater problem-solving capacity and qualification. Interprofessional education is, therefore, a way to enhance the capacity of professionals, teams, and systems for comprehensive health care and a more problem-solving system.¹,²,¹³
In 2010, through the publication of the document **”Framework for action on interprofessional education & collaborative practice”**¹², the WHO pointed to this model, with a proposal for action for interprofessional education and collaborative practice. The framework presented by WHO is characterized by a call to action for policymakers, decision-makers, educators, health professionals, community leaders, and global health advocates to advance the incorporation of interprofessional education and collaborative practice in all the services they provide.¹²
Progressively, health systems demand services’ provision in the face of increasingly complex health issues¹², and the proposed structure by WHO in 2010 already pointed to some characteristics to be observed so that the health workforce is collaborative and ready for interprofessional practice. Without effective training in interprofessional education, we will be doomed to fail in this task. Such training, theoretical and practical, from technical training and/or graduation, contributes to “Interprofessional healthcare teams understand how to optimize the skills of their members, share case management, and provide better health services to patients and the community”.¹²
Another demarcated point by WHO¹², is the issue of joint work between health and education systems, coordinating this effort through interprofessional education, which results in interprofessionality exercise – collaborative practice – in health teams. The proposed framework is not a prescription, but a call to action for global health, so that measures are taken to incorporate interprofessional education and collaborative practice into health services.
The World Health Organization points out, since 2010, that there is **”sufficient evidence to indicate that interprofessional education provides effective collaborative practice that, in turn, optimizes health services, strengthens health systems and incites improvements in health outcomes.”**¹⁰(p.18)
Collaborative practices have a direct impact on greater user and professional satisfaction, better acceptance of offered services, and more satisfactory health outcomes.¹⁰
When addressing the training of health professionals for teamwork with a focus on users, Peduzzi et al.³ already reinforced the importance of interprofessional training, although uniprofessional training predominated at the time in Brazil.
In SUS, several experiences¹⁴–¹⁷ have been established, and reinforce the transformative power of collaborative practices, especially in the scenarios of Primary Health Care (PHC), the Family Health Strategy (FHS). Whether from the work process of the FHS teams themselves, or the induction of changes caused by programs such as PET-Health, Interprofessionality version, the results demonstrate that there needs to be an increasing mobilization of all those involved so that interprofessional education permeates all undergraduate health courses.
After all, for Brazil to achieve a collaborative health workforce prepared for practice, it is essential that the devices that promote interprofessional education in practice¹² – self-training, leadership, institutional support, managerial commitment, results (educator mechanisms) as well as logistics and schedule, syllabus, mandatory attendance, shared objectives, adult learning principles, learning methods, conceptual learning and evaluation (curricular mechanisms) – are effective in the daily life of health education for SUS.
There is a historical facts series in Brazilian reality that has contributed to the institutionalization of interprofessional education in undergraduate courses, ranging from the creation of the Secretary of Work Management and Health Education (SGTES), and programs that induce change to the induced ones and the experience of Federal University of São Paulo (Unifesp) in the Baixada Santista¹⁵˒¹⁸, that deserve to be highlighted.
Lima et al.¹⁹, when studying Interprofessionality in Brazilian national curriculum guidelines (NCG) for health courses in 2024, highlighted that the current guidelines for undergraduate health courses point to teamwork, however, with few mentions of Interprofessionality. The most recent guidelines, such as the one on Medicine, presented more references to Interprofessionality, but they are still insufficient and superficial.
Although the issue of Interprofessionality has been in discussion about changes in higher education for years, according to Ferla and Toassi²⁰, it is possible to understand that within the discussion about health care comprehensiveness, the perspective of uniprofessionality is exhausted. To produce comprehensive health care, with comprehensiveness being one of the pillars of SUS, it is necessary to transform the education and organization of health work, especially at the local/municipal level, where the system takes place in practice. Also, according to Ferla and Toassi²⁰, the movements and changes to produce comprehensive health care are linked to local experiences, still punctual, and resulting from the approximation between training and work in health, that is, from the teaching-service-community integration.
According to Costa²¹, it is known that strengthening health systems certainly involves strengthening the training of the workforce which, in face of increasingly dynamic and complex health needs, points to the need for collaborative work, teamwork, breaking with the strength of traditional and hegemonic training model, which, by establishing itself as uniprofessional, ends up determining obstacles to the collective production of knowledge and practices.
Costa²¹ also recalls that the strengthening and consolidation of Brazilian health system requires permanent reflection on the health professionals’ practices and training, which are inseparable. In other words, “The training of health professionals needs to be consistent with the project to strengthen the health system. The process of building a new logic of health practices must be accompanied by a model of health education that sustains these practices”.²¹(p.15)
That said, therefore, one of the great challenges for Brazil is the discussion around the fact that health professionals who necessarily produce health care together are still trained separately. This uniprofessional, disciplinary training, with a focus on specific competencies, ends up perpetuating fragmented care, which does not meet population health needs. Thus, interprofessional education presents itself as an important path to be followed and (re)thought in the daily life of health education, requiring its confrontation and debate, intending to strengthen the SUS and improve the quality of health care.²¹
By understanding interprofessional education (IPE) as an innovative pedagogical strategy capable of resulting in ICP and health care qualification, Araújo et al.²², when studying the multiprofessional residency in family and community health, recognized it with the potential for joint and coordinated work between different professionals, contributing to the formation of more integrated teams prepared to meet the complex needs of patients in the Brazilian public health system.
In any case, interprofessional education is one of the emerging themes in the field of health education¹², at the national and international levels, and has been widely supported by public policies, in view of the changes in the epidemiological profile of the population, especially in chronic health conditions, requiring collaborative professional practices with a comprehensive approach. Considered an education style that prioritizes teamwork, the concept of interprofessional education has been maturing and improving over time.
For Montanari²³, when reviewing the transformations in medical and health education driven by SUS and the National Curricular Guidelines (NCGs), the great challenge in force is still to train in health, not only to contemplate the disease, but also to teach how to take care of human life, what are different contents.
It is also worth noting that the principle of interprofessionality is essential for multiprofessional teams in the Family Health Strategy (FHS), but there is a conflict between the logic of professionalization and interprofessional collaboration. Interprofessionality is seen as the integration of knowledge and collaboration between professionals, mediated by affections. Three dimensions that enable interprofessionality in the FHS were identified²⁴: organizational, collective, and subjective. In the organizational dimension, devices such as the creation of a “Health Network – School” stand out, transforming health units into spaces for teaching, research and care; the collective dimension addresses the organization of professionals in a working group, or community of practice, with a focus on the development of a common project, mutual engagement, and shared repertoires; and the subjective dimension focuses on the identification of professionals with the FHS care model, in addition to the ability to deal with frustrations and affectivity.
PET-HEALTH PROGRAM – INTERPROFESSIONALITY AND ITS ROLE IN INDUCING CHANGES IN UNDERGRADUATE COURSES
From some years till now, the Brazilian Ministry of Health²⁵ has invested in policies that induce change in health education. Although there is still “training of professionals with ‘specialist’ profiles; disease-focused interventions; misunderstanding and relativization of real health problems; misalignment with the principles of the Unified Health System (SUS), etc.”²⁵(p.1), there is a national effort for change that involves universities, health departments, and health teams in this movement.
The movement around Teaching Care Integration (IDA)²⁶ began in the 1950s and unfolded, over forty years, into several proposals for teaching reform and reorganization of health services throughout Latin America. In Brazil, in 1981, the program was created with the function of inserting students in primary care units through a project distributed all around the country, forming a network with numerous experiences, however, without a significant impact on health curricula.
In the 1980s, the World Federation for Medical Education (WFME) and its regional associations held meetings to establish goals for improving the quality of medical education. And, in 1988, the Edinburgh Declaration was drafted at the world conference, pointing out the need for reforms in medical education. In Brazil, in 1985, the United Network was created, encouraged by the Kellogg Foundation, to qualify professional education in health, based on the expanded concept of health.²⁶–²⁸
It is also worth noting that in 1986 the 8th National Health Conference happened, a fundamental event in the history of Brazilian public health, which subsidized the insertion of the health chapter in the Brazilian constitution.¹⁶˒²⁶˒²⁷ From the Federal Constitution of 1988 and the Organic Health Law (Law 8080/1990), it was established that health education in Brazil should take place in SUS, with SUS and for SUS²⁵. This means that the learning scenarios need to be practical (in SUS), with teaching-learning processes exercising the teaching-service-community integration, being discussed and built with workers, managers and users of the system (with SUS), for the strengthening of Brazilian health system and its consolidation as a great democratic population achievement (for SUS).
The UNI Program²⁷ – A New Initiative in the Education of Health Sector Professionals, which emerged in the 1990s, was a fundamental initial milestone, by proposing changes in education for health professionals, revising the Flexnerian model of medical training, adding the interdisciplinary and multidisciplinary perspective, an important approximation of the theoretical-conceptual and methodological frameworks of interprofessional education.
In 2003, the Secretariat for the Management of Work and Education in Health (SGTES) was created in the Ministry of Health, which has contributed to the creation of policies that reorient professional training for SUS²⁹. In the same year, the project “Experiences and Internships in the Reality of the Unified Health System” – VER-SUS/BRAZIL was also launched³⁰, whose pilot version was the experience in the State of Rio Grande do Sul, and which created the opportunity for 1,200 students to contact 60 Municipal Health Secretariats throughout 2004.
Subsequently, the EnsinaSUS Project³¹ – teaching development, research, and documentation in comprehensive health care construction – in turn, was developed by the Research Laboratory on Practices of Integrality in Health (Lappis), of Social Medicine Institute (IMS) of Rio de Janeiro State University (UERJ), which became institutionalized in 2003. The work officially began in 2004, with the support of the Pan American Health Organization (PAHO), the Ministry of Health, the National Council for Scientific and Technological Development (CNPq), and the Research Support Foundation Rio de Janeiro State (Faperj). The EnsinaSUS program had the role of supporting experiences carried out by different education, health and law institutions, seeking to improve the professionals training in these areas in two specific fields of action: a) training and continuing education, because of the interfaces education, health, law and work; and b) the development/incorporation of new care technologies capable of articulating knowledge and practices produced in the services, to know them, evaluate them and promote their dissemination. The program mapped and systematized studies on professional curricula focused on comprehensiveness, which resulted in several subsequent publications.
In the same year, the National Policy for Permanent Education in Health (PNEPS)³¹ was instituted, which also reoriented health practices and education, by presenting in its precepts the orientation of actions and programs that promoted the meeting among students from different courses, professionals, universities, managers, and social control, inducing changes in the daily routine of health work and promoting what we currently call teaching-service-management-community integration.
Also in 2004, the National Forum for the Education of Health Professions (FNEPAS) was created²⁷, which consists of a network of professional associations in the health area, focusing on the discussion of themes that promote the development of institutional scenarios for changes in health education. With representation from all over the country, FNEPAS ended up being an important space for provocation for the debate on IPE.
Also noteworthy in this process of inducing change is the institution of the National Curriculum Guidelines (NCGs) for undergraduate courses in the health area²⁵˒²⁹, in a joint work of the Brazilian Ministries of Health (MS) and Education (MEC). This process began in 2001 and included 14 health professions, the first document being published in Resolution CNE/CES No. 1,133/2001 – of August 7, 2006, with the NCGs of Medicine, Nursing and Nutrition courses. The other 11 courses that had their NCGs published were: Biomedicine, Biology, Physical Education (bachelor’s degree), Pharmacy, Physiotherapy, Speech Therapy, Veterinary Medicine, Dentistry, Psychology, Social Work and Occupational Therapy.
In this context, the NCGs clearly contemplate the curriculum and the desired professional profile²⁹.
The changes are complex for IPE to be effective in undergraduate courses, and involve the processes of teaching-learning, evaluation, and the curricular organization itself, in addition to working for a graduate profile capable of acting collaboratively, whether in care, education, or health management.
In addition to the guidelines which alone could not account for these complex changes necessary in health education in Brazil, in 2002 the National Program for the Incentive of Curricular Changes in Medical Courses (PROMED) was created, which encouraged internships in university hospitals and public network services to train medical students in meeting the new health realities of the population and the SUS, from PHC/AB. Between 2003 and 2004, the Project Experiences and Internships in the Reality of the Unified Health System – VER-SUS – was launched²⁵˒²⁶, in partnership with the Student Movement, which had several versions over the years.
The NCGs for health courses emphasize, to different extents, the importance of training future professionals for interprofessional teamwork³², with interdisciplinary curricula aligned with the public policies of the SUS. In this context, the VER-SUS program was important because it integrated students into the health system, promoting learning in an environment of collaboration between different actors, such as managers, health professionals, and social movements. This project influenced interprofessional education, highlighting the importance of teamwork and the integration of sciences for better health outcomes.
With the Ver-SUS project, it had been demonstrated that, to improve teamwork, it is necessary to invest in affective relationships and communication between teams. It resignified the idea of a quality public health system and fostered the exchange of experiences among different areas. In addition, it contributed to the differentiated training of health professionals, bringing teaching, service, and community closer together, and providing a critical view of SUS. The project reinforced the importance
of interprofessional collaboration, offering better outcomes and promoting quality health care. The multiplication of training opportunities such as VER-SUS was essential to meet growing social demands and strengthen the SUS care model.
It is also worth mentioning the launch of AprenderSUS program, in 2004, that centered on comprehensiveness idea, understood as the transformation of professional practices, and the creation of the **National Program for the Reorientation of Professional Training in Health (Pro-Health)**³³˒³⁴, which aimed to promote and integrate teaching-service, expanding the participation of courses beyond medicine, professional training based on a comprehensive approach to the health-disease process, and insertion in primary health care.
The Education through Work for Health Program (PET-Health) was inaugurated by Interministerial Ordinance No. 1,802, of August 26, 2008, as part of the Brazilian PNEPS³⁵, whose assumption is based on the feasibility of initiatives for improvement and specialization in the service of health professionals, as well as initiation to work, internships, and experiences, aimed at students in the health area, according to the SUS needs. PET-Health is a program that provides meetings and dialogues among SUS professionals, students, professors from different areas of undergraduate health care, managers, and system users.
From this history, we dared to (re)construct a timeline of the actions that contributed to interprofessional education in Brazil (Figure 2).
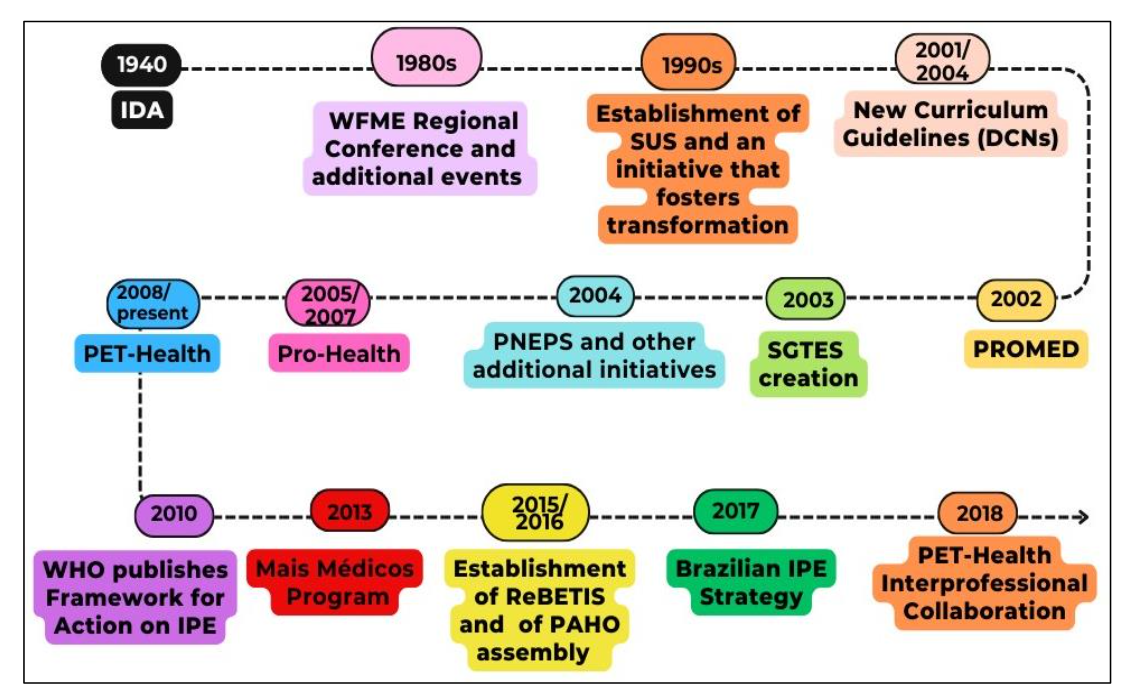
Figure 2 – Timeline of actions that contributed to IPE in Brazil
Font: Prepared by the authors, based on various sources.²⁶˒²⁷˒³⁰˒³³The Brazilian IPE Strategy was especially important for thinking about Interprofessionality in Brazil. And the Brazilian Network of Education and Interprofessional Work in Health (ReBETIS in Portuguese) was fundamental for this. The main educational initiatives underway in Brazil were raised, whose potential for applying the theoretical and methodological assumptions of IPE could contribute to the strengthening of SUS organizational framework.³⁵It is worth noting that, in twelve editions of the program, from 2008 to 2025 (CHART 1), the Ministry of Health has been making progress in inducing changes in health education³⁶, always giving directions to the program organization in practice, with the edition theme. In addition, the formation of interprofessional tutorial groups is encouraged in various editions so that the collaboration and comprehensive care that Interprofessionality can provide and be experienced in the practice scenarios.
Chart 1 – Data from the editions of the Pet-Health Program from 2008 to 2025, Ministry of Health, Brazil
| Announcement | Central theme (Name of Pet-Health) | Period | Selected projects |
|---|---|---|---|
| Public Notice No. 12, of September 3, 2008 | Family Health (PET-Health /SF) | 2009 | 84 |
| Public Notice No. 18, of September 16, 2009 | Family Health (PET-Health/SF) | 2010/2012 | 111 |
| Public Notice No. 7, of March 3, 2010 | Health Surveillance (PET-Health /VS) | 2010/2012 | 70 |
| Joint Notice No. 27, of September 17, 2010 | Mental health (PET-Health /SM) | 2011 | 69 |
| Public Notice No. 24, of December 15, 2011 | Health Care Networks (PRO-Health and PET-RAS) | 2012/2014 | 120 |
| Call Notice No. 28, of November 22, 2012 | Health Surveillance (PET-Health /VS) | 2013/2014 | 105 |
| Public Notice No. 14, of March 8, 2013 | Health Care Networks (PET-Health/RAS) | 2013/2015 | 116 |
| Public Notice No. 13, of September 28, 2015 | Bachelors in Health (PET-Health /GraduaSUS) | 2016/2017 | 105 |
| Public Notice No. 10, July 23, 2018 | Interprofessionality (PET-Health Interprofessionality) | 2018/2019 | 120 |
| Public Notice No. 1, of January 11, 2022 | Management and Assistance (PET-Health/GA) | 2022/2023 | 142 |
| SGTES/MS Notice No. 11, of September 16, 2023 | Health Equity (PET-Health /Equity) | 2023/2025 | 150 |
| Joint Notice SEIDIGI/SGTES-MS No. 1/2025, of February 26, 2025 | Information and Digital Health (PET-Health/I&SD) | 2025/2027 | In progress |
The PET-Health/Interprofessionality had 120 projects monitored by the Ministry of Health³⁵, whose coordinators all around the country contributed directly to the implementation of interprofessionality in education and work in health in Brazil. This edition had its development evaluated, considering the commitments, goals, and evaluation indicators of the program, which resulted in an important bibliographic record of the advances achieved by this program version.Since the beginning of Pet-Health Program, in 2008, a total of 1192 projects have been contemplated, not considering the ongoing edition, Equity in Health, and the new public notice in progress, whose central theme is Information and Digital Health. The promotion of Interprofessionality is undeniable, as well as the effort to induce changes in teaching or education for health professions in Brazil.Interprofessionality presents itself as an impetus for more research, experimentation, and renewal⁷, without eliminating professions, but improving their competencies and skills, making them more capable of solving problems and interacting with different knowledge in the field of health. PET-Health stands out by contributing to the implementation of the National Curriculum Guidelines (NCG) of undergraduate health courses, with Interprofessionality as one of its mottos, for the transformation of future health professionals’ training for SUS. It can be said that over the years, the program has been qualifying the teaching-service-community integration, promoting collaborative practices and interprofessional education.⁷˒³⁷And because of this, the PET-Health Interprofessionality played a prominent role in reorienting health education in SUS⁶, promoting shared learning and the qualification of care. The initiative relied on a systematized support process to ensure the sustainable adoption of interprofessional education and improve health care quality.Furthermore, health work has faced transformations due to changes in the epidemiological and demographic profile, such as the increase in chronic conditions, population aging, and urban violence, exacerbated by the COVID-19 pandemic³⁷. These changes indicate an increasing complexity in health needs. To face this challenge, it was necessary to integrate the health and education systems, and it can be said that interprofessional education is a promising strategy to learn together, interactively, to improve collaboration and quality of care.The PET-Health Interprofessionality also stood out as an important experience³⁷ to promote the debate on interprofessional education in undergraduate courses and health services, even during the pandemic. The potentialities and barriers study of this program helped to identify advances and weaknesses, highlighting the need to continue this process both in teaching and in health practices.Over the last few years, it is undeniable that the different editions of PET-Health, with emphasis on PET-Health Interprofessionality, have encouraged changes in training and work in health, providing significant experiences for the development of essential interprofessional skills, such as clarity of roles, commitment to problem solving and negotiation in decision-making. These characteristics contribute to the construction of curricula that prioritize coexistence, shared learning, and more inclusive and interactive interpersonal relationships, consolidating itself as a strategic action in Brazil to value interprofessionality in the training and health care model.
CHALLENGES IN TRAINING FOR INTERPROFESSIONALITY IN HEALTH PRACTICE: THE SINGULAR THERAPEUTIC PROJECT AND OTHER EXPERIENCES IN PHCThe Multiprofessional Residency in Family and Community Health²² has the potential to offer interprofessional education and ICP, promoting joint and coordinated work among resident professionals, contributing to a more integrated training, and preparing them to meet the complex needs of users of the Brazilian public health system.In this context, it is undeniable that interprofessional practices play a significant role through experience sharing between multiprofessional teams and between residents of different professions³⁸. However, the training of most professionals remains uniprofessional, which ends up generating difficulties in communication between professions and openness to dialogue. Thus, IPE and ICP should be seen as opportunities, seeking to improve the communication skills of residents, preceptors, and professionals in general, to improve teaching and work processes within the scope of Multiprofessional Health Residencies.³⁸For Peduzzi et al.³, in the world scenario, interprofessional education and its practices were still emerging in the field of health in the past decade, especially after the WHO milestone in 2010.³⁸Cassaro et al.³⁹, when studying Interprofessionality in the Nursing courses of public universities in the South Region of Brazil, among the eighteen courses studied, detected that only three of these institutions had Interprofessionality as a theme in the curriculum, and of these, only one offered a discipline focused on it. This is an important finding that reveals the resistance to adherence to interprofessionality since the Nursing Course is generally a pioneer in the adherence to “innovations” in the curriculum. The authors also reinforce that interprofessional education provides opportunities for collective learning, promoting skills and aptitudes necessary for collaborative work.³⁹According to Müller et al.³⁹, innovative curricular changes need to prioritize the collaborative teaching process throughout the undergraduate course. They also reaffirm that IPE and CP need to break with the teaching and practice instituted in Brazilian reality and seek new modes of health care and training. But it is not enough to transform the undergraduate program. New curricular initiatives are welcomed and should be thought of and executed from the beginning to the end of academic training. At the same time, there must be spaces for dialogue and reflection in the services that promote integration and sharing of knowledge. In Brazil, according to the same authors, multiprofessional residencies and PET-Health have proven to be a fertile space for interprofessional education and consequent collaborative practices, although limitations in the training of teachers and preceptors for such change are recognized. In other words, there is a challenge to overcome the gaps between training, health needs, and SUS demands, for the training of professionals capable of acting collaboratively in the practice of health care.A Brazilian example interprofessional training experience in undergraduate health that deserves to be highlighted is that of Unifesp, in the Baixada Santista Campus¹⁵˒¹⁸. By assuming IPE as a guide for training in health courses, the university was able to develop a proposal that seeks to break with the organization in specific disciplines and professional profiles, implementing new ways of training health professionals, connected with the health needs of the population and the professional profile necessary for the consolidation of SUS.It should be noted that, according to Batista et al.¹⁵, the pedagogical project, in addition to have been collectively constructed, in coherence with the current national curriculum guidelines and with the SUS, “is based on the training of a health professional from the perspective of interprofessional teamwork, with an emphasis on comprehensiveness in user care, articulating the ethical, political, technical-scientific and human dimensions in training and performance in the field of health.”¹⁵Thus, the Baixada Santista Campus assumed as organizing principles of this innovative training proposal¹⁵: “inseparability teaching, research and extension; professional practice as the guiding axis of the pedagogical project; problematization of teaching from practice and research; interdisciplinarity; active posture of the student in the construction of knowledge; facilitating/mediating posture of the teacher in the teaching-learning process; integration with the community; recognizing their active and interactive participation in the production of care plans; formative evaluation as feedback on the learning process, and teacher development”.Different courses in the health area – Nutrition, Psychology, Physical Therapy, Occupational Therapy and Physical Education (2006), and Social Work (2009) – had, since the first class, a curricular design directed by four training axes, three of which are common to all courses, and one is specific to each¹⁵˒²⁰. All courses belong to the Institute of Health and Society, with an emphasis on interprofessional and interdisciplinary education as well as a formative conception of qualified professionals for teamwork and comprehensive care. As for the axes, one axis, the “Approximation to a specific practice in health” is organized for students of each professional category. The others are common to the courses, working with classes that mix students from different health courses. They are: “The human being and its biological dimension”, which includes the contents of the biological area; “The human being and his social insertion”, which deals with the contents of the field of Human Sciences (anthropology, sociology, philosophy) and the axis “Work in health”, which includes themes and practices related to the field of health.Complex cases, frequent in PHC, which demand complex solutions, end up bringing to light transversal demands in the production of care¹⁴, presenting therapeutic conducts that require articulation among different professionals and the use of team meetings to reflect on the case and viable solutions. The experience with Singular Therapeutic Project (PTS in Portuguese), a device of the Brazilian National Humanization Policy (NHP), provokes this need for articulation and teamwork, collaboratively approaching interprofessional care, enabling the effective practice of interprofessionality, with the consequent improvement in the results of comprehensive health care for people.In this experience¹⁴, we were able to bring together academics from a tutorial group of the PET-Health Interprofessionality, preceptors, professionals from the Expanded Center for Family Health and Primary Care, and a tutor (that was me), a professor at a School of Medicine. The developed PTS demonstrated the potential to evaluate, assist, and execute interprofessional practices to strengthen happiness projects for the people cared for, going beyond the disease, but also for the individual cared for. The interprofessional home visits also resulted in an opportunity for qualified listening, allowing the identification of not only the needs felt by the monitored user.According to Ferreira et al.¹⁴, it can be said that interprofessionality differs from multiprofessionality by converting the production of specific care into comprehensive care, with teamwork, collaborative, integrating professional centers, focusing on the health needs of users and the population. In this experience, the potentiality of the singular therapeutic project is evidenced – the PTS, as a powerful learning and care device in PHC, which considers the historicity and needs of the user, being a care management instrument capable of producing autonomy, protagonism and social inclusion of the subject. In this scenario, therefore, the PET-Health, especially the Interprofessionality version, presented itself as a favorable experience for interprofessional education.On the other hand, it must be admitted that interprofessional work has not happened in undergraduate health daily in Brazil¹⁴˒¹⁵ – sometimes appearing superficially in the pedagogical projects of the courses, and rarely in practice, except in extension projects as Pet-Health or in institutions such as Unifesp in the Baixada Santista¹⁵˒¹⁸, whose courses were born in this logic of comprehensive health care production, with Interprofessionality as one of its structuring axes.It should be noted that in Brazil, as well as the PTS, there are other interprofessional practices that deserve to be featured⁴⁰, such as: welcoming, which corresponds to the constitutive process of health production and promotion practices that implies the responsibility of the worker/team for the user, from their arrival to their departure; reference teams and specialized matrix support, which correspondto the group that is made up of professionals from different areas and knowledge, organized according to the objectives/mission of each health service, establishing itself as a reference for the users of this service; field and core of knowledge and practices, where the “core” corresponds to the area of knowledge and practices of a given profession, while the “field” is the space of indeterminate limits where disciplines and professions seek support among themselves to fulfill their theoretical and practical tasks, taking care of people in a collaborative way; among other devices.Thus, it is worth thinking about the effective inclusion of IPE and ICP not only in the pedagogical projects of health courses, but also in practice scenarios.
Conclusions
The practice of Interprofessionality in SUS depends directly on changes in undergraduate health education in the country. However, in addition to being present in the guidelines, it needs to be more detailed and align with the connections that need to exist in the formation of different health professions in Brazil. It is necessary for the Ministries of Health and Education to reaffirm the essentiality of training with SUS, in SUS and for SUS, implementing not only curricular content, but also the routine of interprofessional actions in undergraduate health courses. On the other hand, teamwork has been a condition for the consolidation of SUS⁷, of universality, equity, and comprehensiveness. But it is also necessary to understand that teamwork does not happen by a magic wand touch.The existing Brazilian reports of theoretical and practical experiences with interprofessional education are consistent, but they are still few and punctual, and, therefore, need components that demarcate the purpose of the development of collaborative competencies in these processes. It is necessary to reorganize the modes of team training²⁷, breaking the limits of the conformation of courses based on the core of uniprofessional knowledge, moving towards training that also encompasses the field of health and its complexities and possibilities. And this, of course, requires (re)training of teachers as well. It is necessary to understand that promoting interprofessional education goes far beyond bringing together students from different courses in the same space, but it is necessary to have an environment that favors collective production, with the use of methodologies that value such production, collaboration, learning together and doing together in health care, with the center of care not one profession or another, but the person who is cared for. Therefore, there must be guaranteed meetings of students from different health courses, in theory and practice in the SUS real scenarios.The power of Interprofessionality for professionals training committed to collaborative practices in the SUS is undeniable. However, effective implementation requires constant analysis⁷ of the curricula of health courses, the adjustments in teaching practices and institutional support, and the permanent education practices in SUS service. Thusly, the challenge of Interprofessionality is posed, and without the articulation between the health system and the education of these professionals, with the support of the institutions involved, which is not simply financial, but also of time and space for these actions, delivery of a better quality of health services to the population. And for Interprofessionality to be present in the practices of training and services, we definitely need care to be centered on the reception of the user and their demands, on the ethical quality of care and on the humanized problem-solving capacity of care, leaving aside professional practices centered on the corporate interests of their respective professions. As Ceccim often says, it is necessary to **”work together and dismantle fragmentations.”**⁴⁰(p.53) If this is not the case, we will not soon have the consolidation of Interprofessionality as a premise for the professionals’ training with SUS, in SUS, and for SUS.
Conflict of Interest
None.
Funding Statement
None.
Acknowledgements
To the Secretariat for the Management of Work and Education in Health (SGTES) of the Brazilian Ministry of Health, for remaining steadfast in offering programs that contribute to inducing changes in health education in Brazil.
References
1. D’Amour D, Oandasan I. Interprofessionality as the field of interprofessional practice and interprofessional education: An emerging concept. J Interprof Care. 2005;19(SUPPL. 1):8-20. doi:10.108 0/13561820500081604
2. Ceccim RB. Connections and boundaries of interprofessionality: Form and formation. Interface: Communication, Health, Education. 2018;22:1739-1749. doi:10.1590/1807-57622018.0477
3. Peduzzi M, Norman IJ, Germani ACCG, da Silva JAM, de Souza GC. Interprofessional education: Training for healthcare professionals for teamwork focusing on users. Revista da Escola de Enfermagem. 2013;47(4):977-983. doi:10.1590/S0080-623420130 000400029
4. Rosa OM, Teo CRPA, Mattia BJ, Ribeiro KP. Educação Interprofissional em Saúde: elucidando conceitos. Research, Society and Development. 2022;11(12):e74111234216. doi:10.33448/rsd-v11i 12.34216
5. Ellery AEL. Interprofissionalidade. In: Ceccim RB, Dallegrave D, Amorim ASL, et al., eds. EnSiQlopédia das Residências em Saúde. Rede Unida; 2018. doi:10.18310/9788566659986
6. Marques JFL, Costa MV da. PET-Health Interprofessionality and the readiness of students for interprofessional learning. Saude e Sociedade. 2023;32(Supl.2):e220878pt. doi:10.1590/S0104-129 02023220878pt
7. Sousa EDP, Chagas M de S. O Programa de Educação pelo Trabalho para a Saúde/ Interprofissionalidade: experiências de uma acadêmica de Medicina. Rev Bras Educ Med. 2022;46(2). doi:10.1 590/1981-5271v46.2-20210427
8. Tavares De Souza M, Dias Da Silva M, De Carvalho R. Revisão Integrativa: O Que é e Como Fazer Integrative Review: What is it? How to do it? Vol 8.; 2010.
9. Tricco A, Lillie E, Zarin W, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med. 2018; 169(7):467-473. doi:https://doi.org/10.7326/M18
10. Organização Mundial da Saúde. Redes de Profissões de Saúde Enfermagem e Obstetrícia Recursos Humanos para a Saúde. Marco Para Ação Em Educação Interprofissional e Prática Colaborativa.; 2010. http://www.who.int/hrh/nursing_midwifery/en/
11. Elsevier. Mendeley Reference Manager Version 2.131.0. Published online 2025. Accessed March 17, 2025. https://www.mendeley.com/
12. Gilbert JH V, Yan J, Hoffman SJ. A WHO Report: Framework for Action on Interprofessional Education and Collaborative Practice. Vol 39.; 2010. http://www.who.int/hrh/resources/framework_action/en/.
13. Barr H, Low H. Introdução à Educação Interprofissional: Hugh Barr & Helena Low. 1st ed. Centro para o Avanço da Educação Interprofissional (CAIPE); 2013.
14. Ferreira MG, Ferreira KHG, Souza CRP de, et al. Projeto Terapêutico Singular no manejo de casos complexos: relato de experiência no PET-Saúde Interprofissionalidade. Rev Bras Educ Med. 2022;46(1). doi:10.1590/1981-5271v46.1-20210260
15. Batista NA, Rossit RAS, Batista SHS da S, et al. Interprofessional health education: The experience of the Federal university of Sao Paulo, Baixada Santista campus, Santos, Brazil. Interface: Communication, Health, Education. 2018;22:1705-1715. doi:10.159 0/1807-57622017.0693
16. Viana SBP, Hostins RCL, Beunza JJ. Educação interprofissional na graduação em saúde no Brasil: uma revisão qualitativa da literatura. e-Curriculum. 2021;19(2):817-839. doi:10.23925/1809-3876.202 1v19i2p817-839
17. Benevides R, Miranda ES, Abrahão AL, Pereira S. Educação Interprofissional nos cursos da área da saúde de uma universidade pública. Saúde em Debate. 2023;47(139):905-917. doi:10.1590/01 03-1104202313913
18. Capozzolo AA. Formação em comum de profissionais da saúde: experiência da Unifesp, Campus Baixada Santista. In: Toassi RFC, ed. Interprofissionalidade e formação na saúde : onde estamos? [recurso eletrônico]. Rede Unida; 2017. doi:10.18310/9788566659931
19. Lima RBD, Miranda ES, Silva ALA da, Freitas SEAP de. A interprofissionalidade nas diretrizes curriculares nacionais brasileiras dos cursos da área da saúde. Avaliação: Revista da Avaliação da Educação Superior (Campinas). 2024;29. doi:10.1590/1982-57652024v29id279379
20. Ferla AA, Toassi RFC. Formação interprofissional em saúde: um caminho a experimentar e pesquisar. In: Toassi RFC, ed. Interprofissionalidade e formação na saúde: onde estamos? Rede Unida; 2017. doi:10.18310/978856 6659931
21. Costa MV. A potência da educação interprofissional para o desenvolvimento de competências colaborativas no trabalho em saúde. In: Toassi RFC, ed. Interprofissionalidade e formação na saúde : onde estamos? [recurso eletrônico]. Rede Unida; 2017. doi:10.18310/9788566659931
22. Araújo HPA, Dos Santos LC, Da Silva Domingos T, Alencar RA. Multiprofessional family health residency as a setting for education and interprofessional practices. Rev Lat Am Enfermagem. 2021;29. doi:10.1590/1518-8345.4484.3450
23. Montanari PM. Work training in undergraduate degrees in health. Saude e Sociedade. 2018;27(4): 980-986. doi:10.1590/s0104-12902018180974
24. Ellery AEL. Interprofissionalidade na Estratégia Saúde da Família: Condições de possibilidade para a integração de saberes e a colaboração interprofissional. Interface: Communication, Health, Education. 2014;18(48):213-214. doi:10.1590/1807-57622013.0387
25. Lima ES de, Sales ML da H. Políticas Indutoras Da Formação Em Saúde No Brasil -Infográfico. Accessed February 25, 2025.
https://educapes.capes.gov.br/bitstream/capes/714706/2/%5BM3%5D%20Infogr%C3%A1fico%20-%20Pol%C3%ADticas%20Indutoras%20%281%29.pdf
26. Dias HS, Dias A, Lima LD de, Teixeira M. A Trajetória Da Política Nacional de Reorientação Da Formação Profissional Em Saúde No SUS.; 2013. doi:https://doi.org/10.1590/S1413-81232013000600013
27. Freire Filho JR, Silva CBG, Costa MV, Forster AC. Educação Interprofissional nas políticas de reorientação da formação profissional em saúde no Brasil. Saúde em Debate. 2019;43(spe1):86-96. doi:10.1590/0103-11042019s107
28. VIANA SBP, HOSTINS RCL. EDUCAÇÃO INTERPROFISSIONAL E INTEGRALIDADE DO CUIDADO: UMA LEITURA FILOSÓFICA CONTEMPORÂNEA DOS CONCEITOS. Educação em Revista. 2022;38. doi:10.1590/0102-469826460
29. Costa DAS, da Silva RF, Lima VV, Ribeiro ECO. National curriculum guidelines for health professions 2001-2004: An analysis according to curriculum development theories. Interface: Communication, Health, Education. 2018;22(67): 1183-1195. doi:10.1590/1807-57622017.0376
30. Ferla AA, Ramos A de S, Leal MB, Carvalho MS de, eds. VER-SUS Brasil: cadernos de textos. 2013;1(Coleção VER-SUS/Brasil):106. Accessed March 15, 2025.
https://www.redeunida.org.br/media/ckeditor_files/2020/06/08/caderno-de-textos-min.pdf
31. Koifman L, Henriques RLM. A experiência da pesquisa EnsinaSUS. Trabalho, Educação e Saúde. 2007;5(1):161-172. doi:10.1590/S1981-774 62007000100008
32. Do Amaral VF, Cavalcante ASP, Farias QLT, Ribeiro MA, Araújo Júnior DG, Gomes DF. Mobilizing students in the Brazilian national health system (SUS) defense: Interprofessional experiences of VER-SUS – Sobral, CE, Brasil. Interface: Communication, Health, Education. 2018;22(Supl.2):1787-1797. doi:10.1590/1807-57622017.0715
33. Universidade Federal de Santa Catarina. AprenderSUS. Accessed March 15, 2025.
https://unasus2.moodle.ufsc.br/pluginfile.php/6126/mod_resource/content/1/Conteudo_on-line_2403/un03/pdf/aprendersus.pdf
34. Brasil. Ministério da Saúde. Secretaria de Gestão do Trabalho e da Educação na Saúde. Departamento de Gestão da Educação na Saúde. AprenderSUS: O SUS e Os Cursos de Graduação Da Área Da Saúde.; 2004. Accessed March 15, 2025. https://bvsms.saude.gov.br/bvs/publicacoes/cartilha_aprender_sus.pdf
35. Brasil . Ministério da Saúde. Secretaria de Gestão do Trabalho e da Educação na Saúde. Departamento de Gestão da Educação na Saúde. As contribuições do PET-Saúde/Interprofissionalidade para a reorientação da formação e do trabalho em saúde no Brasil. Published online 2024:84. Accessed February 19, 2025.
https://bvsms.saude.gov.br/bvs/publicacoes/contribuicoes_pet_saude_interprofissionalidade.pdf
36. Brasil. Ministério da Saúde. Secretaria de Gestão da Educação na Saúde. Departamento de Gestão da Educação na Saúde. Programa de Educação Pelo Trabalho Para a Saúde: Um Panorama Da Edição PET-Saúde: GraduaSUS. Ministério da Saúde; 2018. www.saude.gov.br/sgtes
37. Morais IF de, Medeiros SM de. PET-Saúde interprofissionalidade and interprofessional education: contributions, barriers, and sustainability. Interface: Communication, Health, Education. 2023;27:e22 0319. doi:10.1590/interface.220319
38. Maffissoni AL, Martini JG, Lazzari DD, Vendruscolo C, Sanes M da S, Bresolin P. Disponibilidade de residentes e preceptores para práticas interprofissionais: estudo de métodos mistos. Rev Lat Am Enfermagem. 2024;32. doi:10.1590/15 18-8345.7374.4396
39. Cassaro BC, De F, Cipolato A, et al. Interprofessionality in Nursing Courses at Public Higher Education Institutions in the Southern Region of Brazil. Revista Saúde em Redes. 7(2):1-7. doi:10.18310/2446-48132021v7n2.3133g648
40. Ceccim RB. Interprofissionalidade e experiências de aprendizagem: inovações no cenário brasileiro In: Toassi RFC, ed. Interprofissionalidade e formação na saúde : onde estamos? [recurso eletrônico]. Vol 06.; 2017. doi:10.18310/97885666 59931