






Intervertebral De-Tethering for Early Onset Scoliosis
“`html
Anterior Scoliosis Correction with Intervertebral De-Tethering Releases for the Treatment of Patients 5 to 10 Years of Age
ABSTRACT
Anterior Scoliosis Correction (ASC) with intervertebral de-tethering releases has emerged as a viable treatment option for children with early onset scoliosis (EOS) and associated thoracic deformity. This study aims to evaluate the outcomes of patients aged 5 to 10 years who underwent ASC with intervertebral de-tethering releases.
Keywords: early onset scoliosis, anterior scoliosis correction, de-tethering releases, pediatric spine surgery
1.0 Introduction
The treatment paradigm for early onset scoliosis (EOS) is inherently complex due to the wide spectrum of underlying etiologies and the potential to accommodate the growth potential of the pediatric spine. Progressive thoracic scoliosis, manifesting in early childhood, is linked to a trajectory of restrictive pulmonary disease, with a potential extension to cardiac dysfunction and increased early mortality risk. Traditional approaches, notably early posterior spinal fusion (PSF) in patients younger than 10 years of age, have been employed; nevertheless, their suitability for young patients with EOS is still a matter of debate.
Since 2014, ASC with anterior longitudinal ligament and annular disc complex (intervertebral) de-tethering releases has been employed through a modified anterior thoracic approach which provides both compression across the convexity and effective derotation. This technique of screws and pliable cords is designed to circumvent the limitations associated with VBT, such as limited curve correction, operative curve size requirements, and the reliability to achieve significant restoration or correction of the deformity.
2.0 Surgical Technique
Intervertebral de-tethering releases (IDTR) are performed under general anesthesia with the patient in a prone position. The anterior longitudinal ligament and annular disc complex are approached through a lateral thoracotomy. For patients with double curves, the intervertebral de-tethering releases are performed where necessary to improve curve correction and increase curve derotation for correction of thoracic hypokyphosis.
The intervertebral de-tethering releases are intended to preserve the disc complex; we do not remove the cartilaginous end plate nor do we extend from the T10-L2 region.
3.0 Results
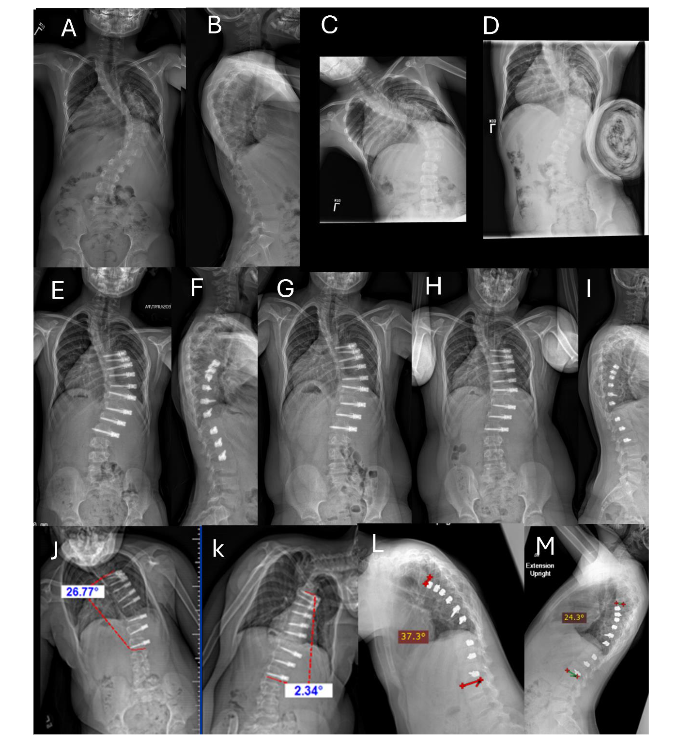
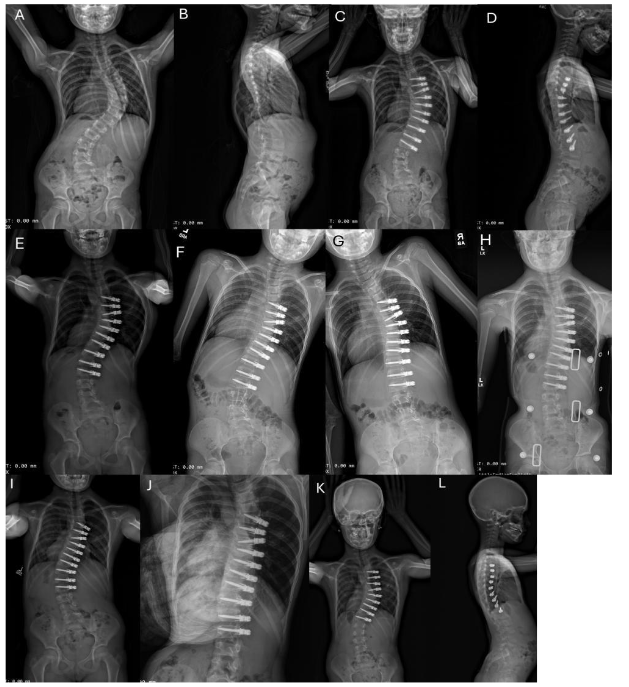
We present a cohort of 15 patients (17 curves) with early onset scoliosis. The mean follow-up was 48.3 months (range 25 to 86 months). In terms of the surgical construct, 9 patients (53%) received a simple line construct, while the remaining 8 patients (47%) were treated with a dual line construct. The placement of one or two screws per vertebra was a subjective determination by surgeon MDA depending on the size of the patient’s vertebrae.
4.0 Revision and Subsequent Stage Surgery
Six of 15 patients (40%) required a subsequent stage ASC for additional curve correction. The other two patients (13%) required spinal fusion. One patient with a stiff curve measuring 106° had a fusion for persistent crankshaft. The instrumented curve corrected to 36°, but the curve crankshafted below the L2 instrumentation necessitating a fusion 3.5 years after initial ASC surgery.
5.0 Discussion
There is a trend that the 11 patients who required second surgeries had fewer intervertebral de-tethering releases compared to the 4 patients who underwent ASC without subsequent surgeries. The average age of the patients undergoing ASC was 8 years old. It is expected that the curve will continue to grow and the spinal column to function correctly.
6.0 Authors’ Current Recommendations
At this time, we have no further recommendations for authors: consideration of ASC for patients with EOS should be age 5 to 10 years, no preexisting proximal kyphosis, curve size up to 80°, and possibly 10° of intervertebral de-tethering releases. We recommend correction of 10 vertebrae in Cobb angle, and curve flexibility down to 30° and possibly 50° if willing to do intervertebral de-tethering releases.
7.0 Conflicts of Interest
RRB has received royalties from DePuy Synthes Spine, Globus NuVasive, SpineGuard, and Therma Medical Publishers; Consulting fees from Globus NuVasive and SpineGuard; and stock options from ApiFix, Orthofix, SpineGuard, and Wishbone Medical. The other coauthors report no conflicts of interest.
8.0 Funding Sources
None
9.0 IRB Approval
This retrospective study was approved by the St. Joseph’s University Hospital Human Subjects in Research Review Board.
10.0 References
- Petersohn K, Larsson S, Oden A, Nachamson A. Long-term survival of patients with untreated scoliosis. A study of mortality, causes of death, and symptoms. Spine (Phila Pa 1976). 1992;17(10):1091-1096.
- Jones RS, Kennedy JJD, Hasham F, Owen R, Taylor JF. Mechanical inefficiency of the thoracic cage in scoliosis. Thorax. 1981;36(6):456-461. DOI:10.1136/thx.36.6.456.
- Fernandes P, Weinstein SL. Natural history of early onset scoliosis. J Bone Joint Surg Am. 2007;89(Suppl 1):21-33. DOI:10.2106/JBJS.F.0754.
- Wunder RB, Moe JH, Heller L, Helvock A. Growth of the thoracic spine in a three year old. J Bone Joint Surg Am. 1982;64:413-419.
“`