





Invaluable Role of CEUS in HCC Imaging and Management
The Invaluable Role of CEUS in HCC Imaging: Diagnosis, Management Planning, and Follow-Up
Christine Merrill Bsc, CRGS, MD1, David P. Burrows MD, FRCP2, Deepak Bhayana MD3, Stephanie R. Wilson MD, FRCP2
- Department of Radiology, Cumming School of Medicine, University of Calgary
- Department of Medicine, Division of Gastroenterology, Cumming School of Medicine, University of Calgary
- Department of Radiology, Cumming School of Medicine, University of Calgary; Department of Medicine, Division of Gastroenterology, Cumming School of Medicine, University of Calgary
OPEN ACCESS
PUBLISHED: 30 NOVEMBER 2024
CITATION: Wilson, S. R., et al., 2024. The Invaluable Role of CEUS in HCC Imaging: Diagnosis, Management Planning, and Follow-Up. European Journal of Medicine, 12(1). https://doi.org/10.18103/mra.v12i1.4173
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v12i12.6175
ISSN 2375-1924
Introduction
Hepatocellular carcinoma (HCC) represents the third leading cause of cancer-related mortality worldwide. While it can occur in patients without risk factors, it usually develops in patients with a background of chronic liver disease, with the highest rates found in patients with cirrhosis. Historically, this predominantly developed secondary to viral hepatitis or alcoholic steatoshepatitis; however, the incidence of non-alcoholic associated fatty liver disease, recently renamed metabolic associated fatty liver disease (MAFLD) has been steadily increasing as a major contributor to the incidence of both cirrhosis and HCC, especially in Western society.
There is a high incidence rate of HCC in patients with cirrhosis, necessitating the development of surveillance protocols to identify HCC at an early stage. Current guidelines recommend surveillance with ultrasound (US) and alpha-fetoprotein (AFP) testing every 6 months for patients with cirrhosis. However, the sensitivity of US is limited, particularly in patients with obesity or fatty liver disease. In this context, contrast-enhanced ultrasound (CEUS) has emerged as a valuable adjunct in the diagnosis and management of HCC.
Diagnosis
The Ultrasound Liver Imaging and Reporting Data System (US LI-RADS) is a framework that allows for standardized imaging, interpretation, and reporting of identified nodules.
It is divided into subcategories beginning with surveillance US, performed looking for nodules with high potential to be HCC. Primary surveillance programs for those at high risk for HCC comprise greyscale ultrasound performed at 6-month intervals. High quality scans require good equipment and meticulous attention to technique including multi-frame acquisition of scans performed with a sweeping motion through the liver to cover all the hepatic segments during a breath hold. These sweeps should include both liver lobes in sagittal and axial planes making a total number of at least four sweeps. More detailed single frame imaging is then included of all suspicious areas.
Prior to interpreting observations, a visualization score is assigned to the US images. This encompasses a visualization score with no limitations (VIS-A) or one with moderate limitations because of parenchymal heterogeneity (VIS-B). VIS-C is assigned when < 50% of the liver is captured in the evaluation or when the portion of captured liver exhibits severe heterogeneity so as to mask any meaningful observations.
Once a visualization score is provided, LI-RADS US subdivides findings into three general observation categories:
-
US-1 negative
-
US-2 subthreshold
-
US-3 positive
US-1 negative includes examinations with no observations or definitely benign findings.
such as simple hepatic cysts. US-2 includes not definitely benign findings < 10 mm in diameter. Lastly, US-3 includes observations ≥ 10 mm or the presence of a new thrombus in the portal and hepatic veins. While patients with US-3 designations automatically need to undergo further characterization, patients with US-2 usually receive repeat US in 3–6 months for a total of two times to assess for interval stability of size. This algorithm may be different in the presence of a positive alpha-fetoprotein with no US-3 observations, where these patients automatically receive diagnostic multiphase CT or MRI for further workup.
Any new nodule suspicious for HCC on greyscale US based on the LI-RADS US necessitates further multiphase contrast-enhanced imaging with either MR, CT, or CEUS. HCC presents with a characteristic hemodynamic enhancement pattern of arterial phase hyperenhancement (APHE) and late mild washout in the delayed phase. Beyond creating a standardized reporting system, the LI-RADS framework is an accurate probabilistic model with the objective of providing a non-invasive means of specifically diagnosing HCC.
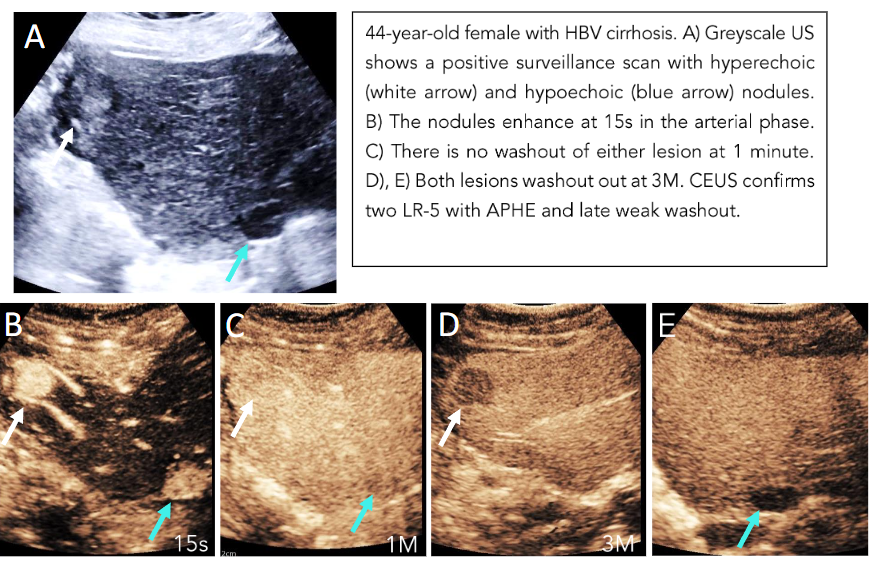
Through a five-category classification system, it grades observed lesions using specific criteria to be “definitely benign” (LI-RADS 1) to “definitely HCC” (LI-RADS 5). This results in a clear reporting system with high inter-observer reliability for the clinical team to base their management decisions on. For example, the designation of LI-RADS 5 given to a nodule greater than 1 cm with APHE and late and weak washout does not require a biopsy for a definite diagnosis (Figure 1).
There are two time points that we keep in mind when looking for washout relative to time zero, which is when the microbubble contrast is flushed with normal saline. Any washout that occurs prior to 1 minute is considered early or rapid and consistent with non-hepatocellular malignancies. Washout that is marked and occurs by 2 minutes is also indicative of a malignant non-HCC lesion.
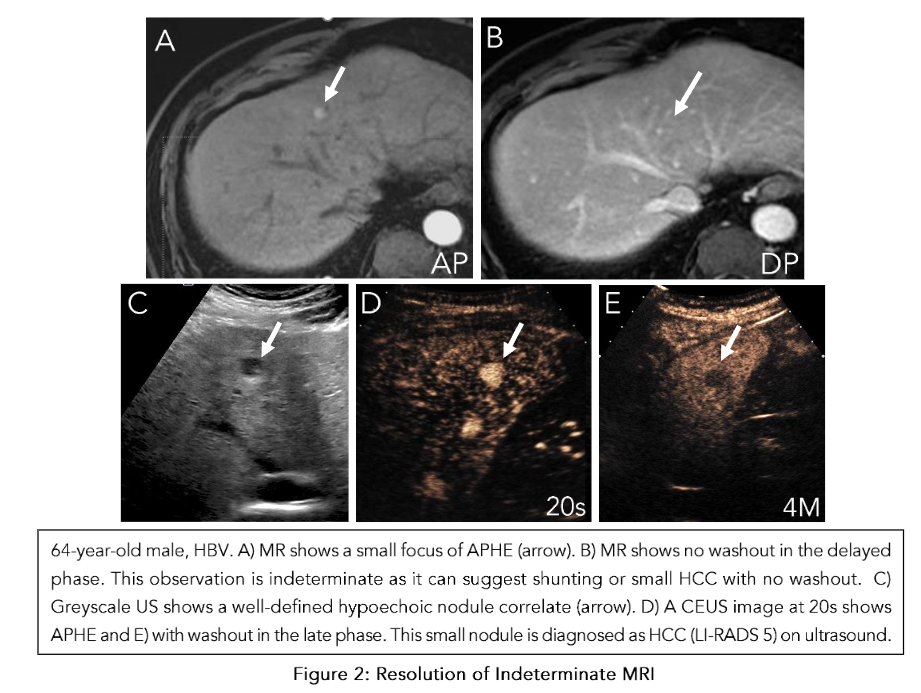
Additionally, care needs to be taken when interpreting APHE on CT and MRI in cirrhotic livers because they may represent pseudolesions such as nontumorous arterioportal shunts (Figure 2). These pseudolesions can be evaluated with US as a problem-solving tool to determine the presence of a true nodule and then characterize its enhancement and washout pattern.
When we consider lesions that are “probably HCC” (LI-RADS 4), a biopsy is warranted as the incidence of HCC has been shown to be 48% in a study of 175 nodules (Figure 3). This threshold to biopsy is informed by the specificity of the LI-RADS 5 criteria, which is supported by a meta-analysis of fourteen studies showing a pooled per-observation specificity of 91% (95% CI, 89%-93%).
Another important category to consider is LI-RADS M (malignancy), which describes a lesion to be “probably or definitely malignant,” but not necessarily in keeping with HCC. These lesions may exhibit a characteristic rim of APHE or early washout (less than 1 minute) or marked washout within 2 minutes. Any of these features will classify the lesion as LI-RADS M.
Pathologies within this category can include metastases, intrahepatic cholangiocarcinoma (ICC), or in a minority of cases, benign lesions. The prospective identification of metastases or ICC, the second most common malignancy found in patients with chronic liver disease, is of the utmost importance as management strategies and prognoses differ between these pathologies and HCC.
Alongside these non-HCC lesions, pathological correlation has interestingly shown 28.2% (95% CI, 23.8%-33.1%) of LI-RADS M lesions to ultimately be HCC (Figure 4). This is in part due to the stringent criteria set forth for a LI-RADS 5 lesion and the considerably higher incidence of HCC compared to pathologies like ICC.
Overall, LI-RADS has been shown to be an effective framework for risk stratifying hepatic lesions concerning increased risk of HCC.

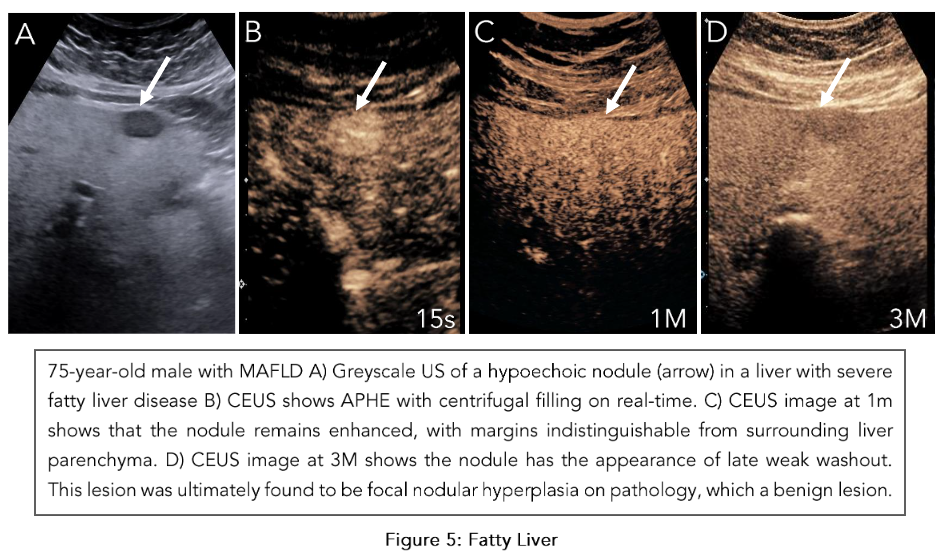
Although LI-RADS was originally validated with CT and MRI, CEUS has similarly been shown to be an accurate imaging method for categorization of liver nodules. In a multi-center prospective study, CEUS of 545 nodules with confirmed reference standards demonstrated LI-RADS 5 to have a specificity of 95.1% (95% CI, 94.5%–98.7%). These contrast-based imaging evaluations broadly share similar criteria given the intrinsic enhancement and washout patterns observed in HCC. However, these imaging modalities mutually share challenges in characterizing focal liver lesions like HCC when the liver parenchyma has undergone diffuse fatty changes. Our experience and literature have suggested that although APHE is usually preserved, it is difficult to appreciate washout properties of HCC on MRI with increasing steatosis. This absent washout may be secondary to increased background liver hypointensity in fatty liver, which gives the relative appearance of persistent enhancement or isoenhancement when trying to characterize washout in the delayed phase. Our experience has shown that CEUS can perform well in identifying nodules and their APHE in fatty liver but can be misleading when assessing for washout in the late phases. We believe this is because of the augmented surrounding enhancement in the late phases caused by the fat, which can portray a picture of “pseudowashout” (Figure 5).
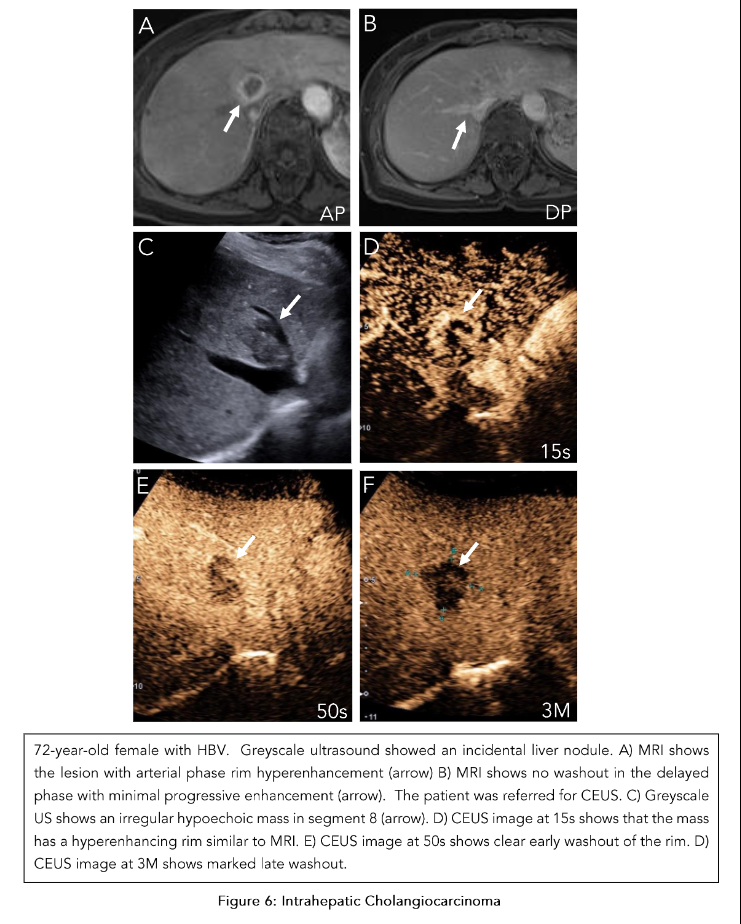
Short interval follow-up, repeat injection with a high-frequency transducer, and consideration of liver-specific contrast-enhanced MR are warranted in these situations. Moreover, there is a critical difference that differentiates CEUS from CT/MRI when considering LI-RADS M lesions. In cases of ICC, CEUS and CT/MRI both show APHE, but in the portal venous phase, CEUS shows rapid washout whereas CT/MRI show progressive enhancement (Figure 6). This discordance is thought to be secondary to the purely intravascular nature of microbubbles used in CEUS, which is unique compared to the recognized interstitial phase of iodinated and gadolinium-based contrast agents. Although this has yet to be considered in formulating the criteria for LI-RADS M lesions, this finding may further improve the accuracy of CEUS in the diagnosis of focal liver masses.
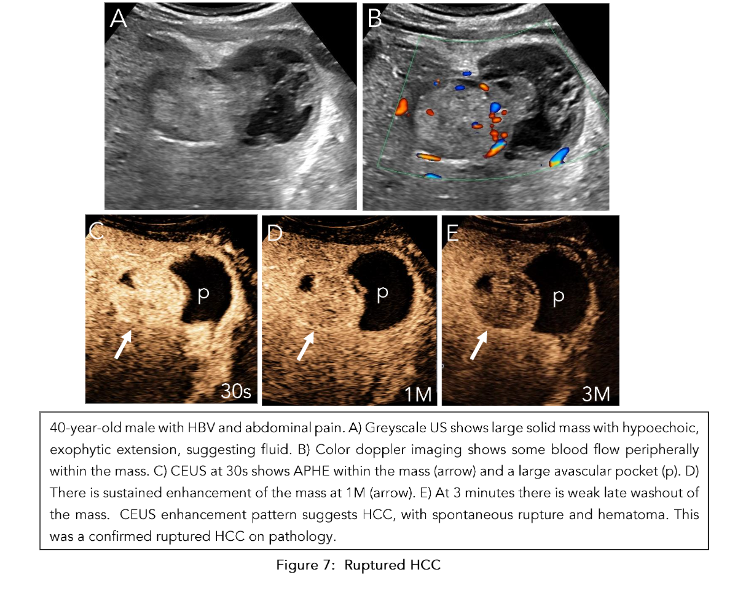
Our validated provincial protocol uses CEUS as the first test to characterize focal liver lesions, with many not requiring MRI prior to management planning. In a prospective study of 195 at-risk patients receiving routine surveillance with greyscale US, CEUS LI-RADS categorization demonstrated equal if not superior efficacy to MRI in diagnosing HCC when used as a first-line test following positive surveillance ultrasound. Moreover, when we maintain ultrasound as the foundational imaging mechanism for both surveillance and nodule characterization, we can achieve better correlation of surveillance findings with CEUS than MRI. When it concerns sub-centimeter nodules flagged on surveillance for further characterization, CEUS also excels in characterizing the enhancement and washout properties given its high spatial resolution and purely intravascular contrast agent. In the event a sub-centimeter nodule demonstrates APHE and late and weak washout, it is categorized as LI-RADS 4, but individual discretion dictates whether a short interval follow-up (less than 3 months) or immediate treatment is appropriate. CEUS also plays an important role when evaluating complications such as HCC rupture (Figure 7). Outside of following up positive surveillance findings, CEUS plays an important role in clarifying indeterminate findings on CT or MRI. In a prospective study of 27 indeterminate hepatic nodules characterized on CT, CEUS was able to accurately diagnose HCC in 7 cases. CEUS and MRI are also able to comparatively supplement each other in cases where there is no definitive diagnosis of HCC. Overall, a complementary framework where these imaging modalities are used in a multidisciplinary approach to HCC diagnosis is critical when forming management strategies.
Management Planning
Once a diagnosis of HCC is established, a multidisciplinary team including hepatologists, medical and radiation oncologists, diagnostic radiologists, interventionalists, and surgeons review the case to devise the optimal treatment strategy. CEUS can be further used to assist with the management planning. At baseline, the goal of greyscale ultrasound is to identify a greyscale target for planning and targeting purposes. This pre-procedure step is critical in guiding the interventionist to perform a percutaneous ablation on the target nodule. However, this pre-procedure step may not easily identify the target nodule using greyscale ultrasound alone, especially when the lesion is situated in a difficult-to-visualize anatomic location or when the nodule is occult. In fact, in a study of 109 patients, 29.4% of cases were deemed unfeasible for performing ultrasound-guided percutaneous RF ablation because of tumour invisibility. However, CEUS can help overcome these limitations. Specifically, it allows for correct identification of the target nodule in the presence of multiple nodules and improves visualization of occult nodules on greyscale ultrasound. To further explore the practical application of CEUS in these settings, consider a scenario where a patient with confirmed HCC is found to have multiple nodules on greyscale ultrasound. On greyscale ultrasound, it is unfeasible to differentiate which of the nodules is the target nodule, especially if they are in close proximity. CEUS can overcome this limitation by visualizing the enhancement and washout properties of the nodules to correctly identify the target nodule. Once the target nodule is identified, we can aid the interventionalist by documenting the patient and probe position, degree of inspiration, type of probe, and proximity to vital structures like the gallbladder, central bile ducts, bowel, and vessels. These details are critical because if the lesion is found to be subcapsular and only accessible with full inspiration, ablation can carry a higher risk of complications and be less effective. Alternatively, ablation may simply be contraindicated when the procedure risks injuring the aforementioned vital structures. Proximity to vessels also decreases the efficacy of ablation secondary to the “heat-sink” effect. Another potential scenario where CEUS is helpful includes settings where greyscale ultrasound cannot reveal any potential correlates to MRI findings. Here, CEUS can identify the lesion by performing an injection within the area of concern. Essentially, the previously occult nodule can be illuminated with the administration of contrast as we forego identification based on echogenicity to rely on enhancement and washout properties (Figure 8). In the event only a nodular focus of washout is observed in the late phase, a repeat injection can be performed in the washout region to characterize the arterial phase properties of the suspicious correlate. Thus, if no nodule can be visualized on greyscale ultrasound, CEUS can provide value by clearly delineating the target nodules to facilitate potential ablation. Outside of our institution, independent studies by Maruyama et al. and Chan et al. both support the value of CEUS in detecting occult nodules on greyscale ultrasound. Beyond identifying the likely HCC correlates on ultrasound, CEUS can also reveal surprise findings that can change management. Potential surprise findings can include a size discrepancy or additional liver lesions not previously seen on prior MRI. Depending on the size and number of total lesions, ablation therapy may not be indicated. Although there is no universally agreed upon size cut-off, commonly cited thresholds include up to 5 cm for one unilobar lesion or 3 cm for multiple unilobar lesions. Furthermore, ablation may also not be indicated if there is any evidence of tumor in vein (TIV), which needs to be differentiated from a morphologically similar benign portal vein thrombus (PVT) (Figure 9). With an incidence of 9.8% in patients with cirrhosis, PVT is a relatively common complication that can be present in the patient population undergoing pre-ablation planning CEUS.

Guidance of Ablative Therapy
There are different types of ablative therapies that can be chosen depending on the clinical scenario. Microwave (MW) ablation and radiofrequency (RF) ablation are two well-studied local ablative techniques used by interventionists treating HCC. The former has the advantage of larger ablation volumes, faster ablation time, and higher intra-tumoral temperatures; however, RF ablations are considered safer as they result in lower rates of severe adverse events. This could be secondary to the multi-pronged structure of RF ablation probes minimizing risk of retraction during a burn or the risks associated with a wider burn radius in the case of MW ablation. Beyond ablation, other treatment strategies may be considered. Percutaneous ethanol injection (PEI) is a cost-effective method of locally treating HCC. However, the non-uniform distribution of ethanol leads to heterogeneous tumor necrosis and is suggested to have inferior outcomes compared to RF ablation. Transarterial chemoembolization (TACE) capitalizes on the concept of localizing delivery of a cytotoxic agent but combines it with embolization to create an ischemic effect by limiting the tumoral blood supply. It is recognized as the gold standard treatment for intermediate-stage HCC. Another entirely different category of treatment includes radiation therapies such as transarterial radioembolization (TARE) or stereotactic body radiation therapy (SBRT). TARE is a locoregional radiotherapy that is also indicated in patients with intermediate-stage HCC, with relatively equivalent survival rates when compared to TACE. Each of these treatment methods carries certain benefits, with the optimal treatment strategy dependent on each patient’s unique clinical presentation. On the day of the ablative procedure, the previously recorded parameters such as the patient probe, position, and phase of inspiration are referenced to orient the interventionalist. The performance of the procedure may be successful with greyscale ultrasound alone; however, the presence of multiple or occult nodules can present a challenge in successfully ablating the target lesion. CEUS is a valuable tool in the guidance of the ablation probe during this stage as it can be used to target areas of arterial phase hyperenhancement and/or washout. The late phase with washout is generally preferred as it lasts longer than the arterial phase. This allows the operator more time to place the ablation probe and adjust as needed. However, the washout phase may not always be ideal for probe guidance. Some lesions may exhibit a very subtle area of washout. In these cases, the arterially enhancing component can be used as the target with repeat contrast injections to re-enhance the target area.
Immediate Post-Ablation Assessment
Once the ablation is performed, it is crucial to assess for any evidence of residual HCC, which will require re-ablation. Post-ablation, the ablation bed may be obscured by echogenic gas bubbles from water vaporization. These bubbles can be burst using high mechanical index ultrasound techniques. Essentially, a high mechanical index leads to increased acoustic pressure to overcome the surface tension of the contrast bubbles resulting in their cavitation. To achieve this, one can keep the ultrasound machine in regular B-mode ultrasound and manually increase the mechanical index, use the CEUS flash button, or the Doppler mode. After eradication of the gas bubbles, CEUS offers the ability to conduct immediate assessment of the ablation bed to identify a non-target ablation or incomplete ablation. Of note, CEUS assessment provides relatively higher contrast of the enhanced signal to background tissue compared to enhanced CT and MRI. This is because CEUS benefits from a pulse inversion technique to subtract linear echoes of background tissue from the non-linear signal from microbubbles, giving maximum contrast differential. When a complete ablation is performed, the avascular treatment bed usually has a smooth contour with no discrete APHE despite generalized hyperemia in the surrounding liver. A non-target ablation presents adjacent to the avascular site as an area of APHE with late mild washout in the late phase. An incomplete ablation occurs when there is residual APHE within the ablation site. Usually, the ablation probe is left in place during the immediate post-ablation assessment period. Thus, with repositioning, the interventionalist can re-ablate the remaining lesion to achieve complete ablation. This process is repeated until the area is confirmed to be free of residual disease. Notably, there are cases where the vascular properties of the HCC nodule are isovascular or hypovascular in nature. As such, APHE cannot be relied upon and observation for any washout is necessary to confirm complete ablation. Ultimately, the process of immediate post-ablation assessment with CEUS has been shown to improve outcomes by reducing the rate of incomplete or non-ablations.
Secondary Surveillance
Despite curative intent percutaneous ablation, there is a high risk of local and distant HCC recurrence with respective reported rates of 34.3% and 45.3% over a median follow-up time of 78 months. In the first 2 years, recurrence is likely from the treated primary whereas lesions detected beyond 2 years are likely de novo lesions. Secondary surveillance strategies can vary by institution, but studies have shown CEUS to be a valuable complementary addition to CT or MR-based surveillance strategies. Given that access to MRI is resource limited, CEUS not only offers increased accessibility, but it also limits the cumulative radiation risk of CT and nephrotoxicity of contrast agents. At our institution, we employ the use of MRI at 1 month after treatment, followed by alternating CEUS and MRI every 3 months for 2 years, with a return to greyscale ultrasound surveillance every 6 months thereafter. Through a prospective study investigating the efficacy of this strategy, there was no difference in the sensitivity or specificity between the two imaging modalities. CEUS and MRI served as mutually reinforcing modalities that allowed equivocal cases detected by either modality to be confirmed or disproved by the other.
The observations in the secondary surveillance period follow the CEUS LI-RADS treatment response algorithm (TRA). In a technically adequate exam, the ablation site is assessed for both intralesional and perilesional tumor viability.
-
Intralesional viability:
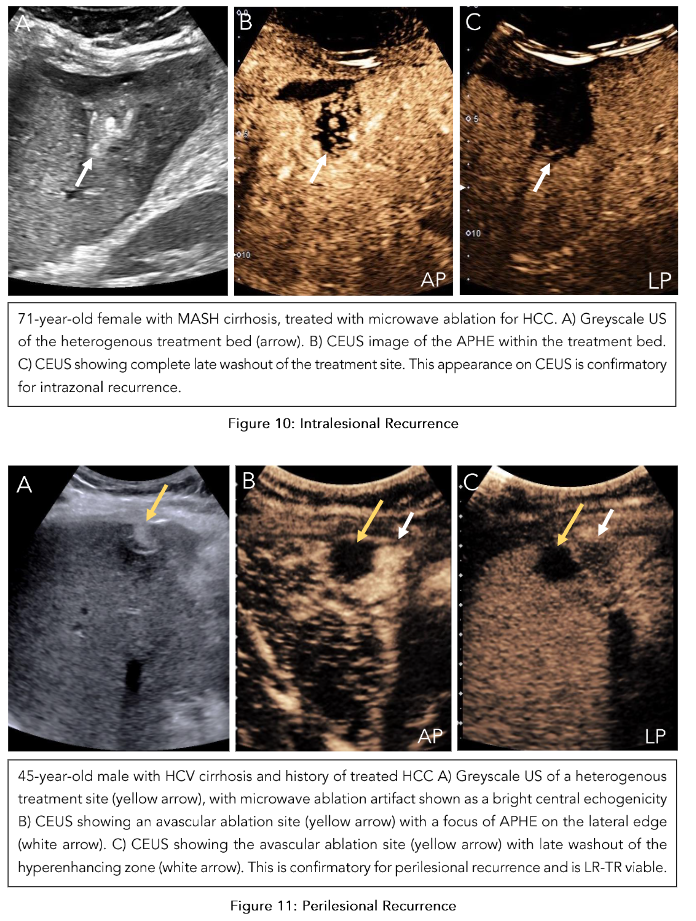
If there is no enhancement within the ablation bed, it indicates the absence of a viable tumor. Uncertain viability is characterized by arterial phase hypoenhancement (with or without washout), while hyperenhancement or isoenhancement (with or without washout) suggests the presence of a viable tumor (Figure 10). -
Perilesional viability:
Absent viability is characterized by homogeneous enhancement of the ablation margins compared to the rest of the liver. Uncertain viability is characterized by arterial phase hyperenhancement without washout, isoenhancement with washout, or hypoenhancement. The presence of a viable tumor is confirmed by hyperenhancement with washout (Figure 11). Once both these categories are assessed, an overall treatment response score is determined based on their respective contributions:
-
If there is any intralesional or perilesional viability, the overall treatment response score is LR-TR viable.
-
If there is any uncertainty in one without viability present in the other, the overall treatment response score is LR-TR equivocal. Here, an alternative imaging modality like MRI would be useful in clarifying the viability.
-
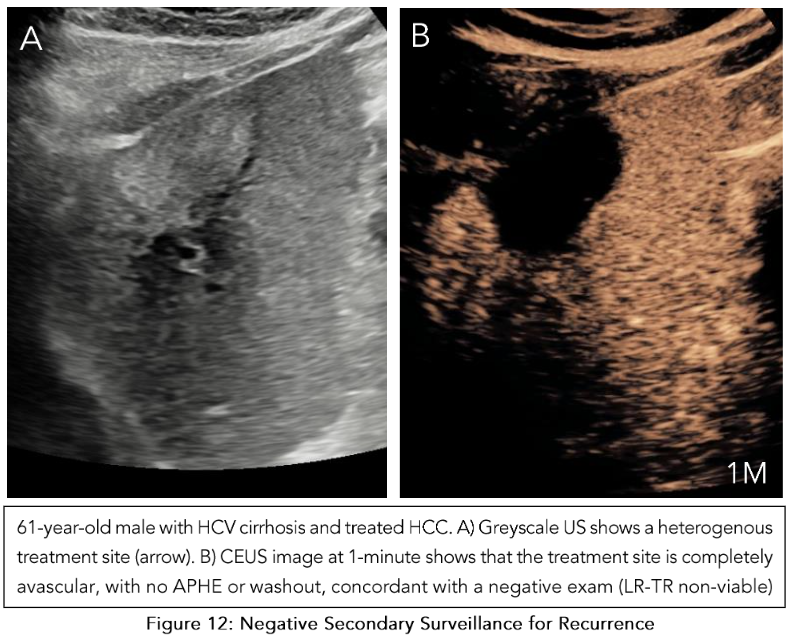
Only when there is absent viability in both intralesional and perilesional viability is the final category designated as LR-TR nonviable (Figure 12).
CEUS offers considerable benefit. As discussed, it offers relatively higher spatial resolution in the absence of volume averaging, higher contrast differential secondary to pulse inversion techniques, and increased sensitivity to contrast agents given the purely intravascular nature of microbubble contrast material. However, it is not without its own limitations. Compared to CT or MRI, it is a relatively labor-intensive process that has variable performance depending on the operator and the patient’s body habitus. Moreover, as the severity of cirrhosis advances and the number of therapeutic procedures increases, the echotexture of the liver becomes progressively heterogeneous, which results in difficult visualization and assessment. Furthermore, although our departmental experience outlined above is based on the performance of 25,000 CEUS scans since 2010, with the overwhelming majority focused on hepatic imaging, it is nonetheless a single center’s experience. Thus, the generalizability of our statements is limited as we have not captured the viewpoints of the experiences from other centers.
Conclusion
Spanning diagnosis to ablation planning and guidance to secondary surveillance, CEUS plays a pivotal role in caring for patients with HCC. It provides an accurate diagnosis in patients at risk for HCC and can also clarify equivocal findings on CT or MRI. When undergoing management planning, pre-ablation CEUS scans can assist in identifying the correct greyscale target and even reveal findings that change management. Its real-time ability to visualize hepatic enhancement patterns is a great asset in both targeting HCC lesions and their immediate post-ablation assessment. Additionally, it serves as a complementary modality in secondary surveillance with a key role in detecting recurrence. Despite the present resistance to its widespread adoption, the evidence behind its utility in the entire breadth of HCC care is encouraging for broader acceptance and gradual integration into standard clinical practice.
Keywords
Hepatocellular carcinoma, CEUS, imaging, diagnosis, management, planning, follow-up
References
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71(3):209-49.
2. Fattovich G, Stroffolini T, Zagni I, Donato F. Hepatocellular carcinoma in cirrhosis: incidence and risk factors. Gastroenterology. 2004;127(5):S3 5-S50.
3. McIntyre CA, Chou JF, Gonen M, Shia J, Gambarin-Gelwan M, Balachandran VP, et al. Hepatocellular carcinoma in patients with no identifiable risk factors. HPB (Oxford). 2021;23(1):1 18-26.
4. Chen H, Zhan Y, Zhang J, Cheng S, Zhou Y, Chen L, et al. The Global, Regional, and National Burden and Trends of NAFLD in 204 Countries and Territories: An Analysis From Global Burden of Disease 2019. JMIR Public Health Surveill. 2022;8 (12):e34809.
5. Fung A, Shanbhogue KP, Taffel MT, Brinkerhoff BT, Theise ND. Hepatocarcinogenesis. Magnetic resonance imaging clinics of North America. 2021;29(3):359-74.
6. Tsilimigras DI, Bagante F, Moris D, Hyer JM, Sahara K, Paredes AZ, et al. Recurrence patterns and outcomes after resection of hepatocellular carcinoma within and beyond the Barcelona clinic liver cancer criteria. Annals of surgical oncology. 2020;27:2321-31.
7. Zhang J, Yu Y, Li Y, Wei L. Diagnostic value of contrast-enhanced ultrasound in hepatocellular carcinoma: a meta-analysis with evidence from 1998 to 2016. Oncotarget. 2017;8(43):75418.
8. Huang J-Y, Li J-W, Lu Q, Luo Y, Lin L, Shi Y-J, et al. Diagnostic accuracy of CEUS LI-RADS for the characterization of liver nodules 20 mm or smaller in patients at risk for hepatocellular carcinoma. Radiology. 2020;294(2):329-39.
9. Hanna RF, Miloushev VZ, Tang A, Finklestone LA, Brejt SZ, Sandhu RS, et al. Comparative 13-year meta-analysis of the sensitivity and positive predictive value of ultrasound, CT, and MRI for detecting hepatocellular carcinoma. Abdominal radiology. 2016;41:71-90.
10. Wang G, Zhu S, Li X. Comparison of values of CT and MRI imaging in the diagnosis of hepatocellular carcinoma and analysis of prognostic factors. Oncology letters. 2019;17(1):1184-8.
11. Hu J, Burrowes DP, Caine BA, Gibson N, Bhayana D, Medellin A, et al. Nodules Identified on Surveillance Ultrasound for HCC: CEUS or MRI as the Initial Test? Journal of Ultrasound in Medicine. 2023;42(6):1181-90.
12. Eisenbrey JR, Gabriel H, Savsani E, Lyshchik A. Contrast-enhanced ultrasound (CEUS) in HCC diagnosis and assessment of tumor response to locoregional therapies. Abdominal Radiology. 2021;46:3579-95.
13. Bansal S, Gui J, Merrill C, Wong JK, Burak KW, Wilson SR. Contrast-enhanced US in Local Ablative Therapy and Secondary Surveillance for Hepatocellular Carcinoma. RadioGraphics. 2019;3 9(5):1302-22.
14. Bansal S, Lu F, Frehlich L, Wong JK, Burak KW, Wilson SR. A new proposal for secondary surveillance following potentially curative therapy of HCC: alternating MRI and CEUS. Abdominal Radiology. 2022:1-12.
15. Radiology ACo. CEUS LI-RADS® v2017 CORE. 2020.
16. Radiology ACo. CT/MRI LI-RADS v2018 core. Liver Imaging Reporting and Data System. 2018.
17. Radiology ACo. LI-RADS® Ultrasound Surveillance v2024 Core. 2024.
18. Radiology ACo. Quality and safety resources: Liver Imaging–Reporting and Data System. Reston, VA: ACR. 2012.
19. Choi J-Y, Cho HC, Sun M, Kim HC, Sirlin CB. Indeterminate observations (liver imaging reporting and data system category 3) on MRI in the cirrhotic liver: fate and clinical implications. American Journal of Roentgenology. 2013;201(5): 993-1001.
20. Hu J, Bhayana D, Burak KW, Wilson SR. Resolution of indeterminate MRI with CEUS in patients at high risk for hepatocellular carcinoma. Abdominal Radiology. 2020;45:123-33.
21. Lee S, Kim YY, Shin J, Hwang SH, Roh YH, Chung YE, et al. CT and MRI Liver Imaging Reporting and Data System Version 2018 for Hepatocellular Carcinoma: A Systematic Review With Meta-Analysis. J Am Coll Radiol. 2020;17(10):1199-206.
22. Mavros MN, Economopoulos KP, Alexiou VG, Pawlik TM. Treatment and prognosis for patients with intrahepatic cholangiocarcinoma: systematic review and meta-analysis. JAMA surgery. 2014;149 (6):565-74.
23. Bridgewater J, Galle PR, Khan SA, Llovet JM, Park J-W, Patel T, et al. Guidelines for the diagnosis and management of intrahepatic cholangiocarcinoma. Journal of Hepatology. 2014;60(6):1268-89.
24. Lyshchik A, Wessner CE, Bradigan K, Eisenbrey JR, Forsberg F, Yi M, et al. Contrast-enhanced ultrasound liver imaging reporting and data system: clinical validation in a prospective multinational study in North America and Europe. Hepatology. 2024;79(2):380-91.
25. Venkatesh SK, Hennedige T, Johnson GB, Hough DM, Fletcher JG. Imaging patterns and focal lesions in fatty liver: a pictorial review. Abdominal radiology (New York). 2017;42(5):1374-92.
26. Botros SM, Ahmed KS, Ismail MZ, Ali WKIH. Non-Alcoholic Fatty Liver Disease-Associated Hepatocellular Carcinoma: Effect of Hepatic Steatosis on Major Hepatocellular Carcinoma Features at MRI. QJM : An International Journal of Medicine. 2023;116(Supplement_1).
27. Wilson SR, Burrowes DP, Merrill C, Caine BA, Gupta S, Burak KW. Unique portal venous phase imaging discordance between CEUS and MRI: a valuable predictor of intrahepatic cholangiocarcinoma? Abdom Radiol (NY). 2024;49 (1):11-20.
28. Wang DC, Jang H-J, Kim TK. Characterization of indeterminate liver lesions on CT and MRI with contrast-enhanced ultrasound: what is the evidence? American Journal of Roentgenology. 2020;214(6): 1295-304.
29. Maruyama H, Takahashi M, Ishibashi H, Yoshikawa M, Yokosuka O. Contrast-enhanced ultrasound for characterisation of hepatic lesions appearing non-hypervascular on CT in chronic liver diseases. The British journal of radiology. 2012;85 (1012):351-7.
30. Kim J-E, Kim Y-s, Rhim H, Lim HK, Lee MW, Choi D, et al. Outcomes of patients with hepatocellular carcinoma referred for percutaneous radiofrequency ablation at a tertiary center: analysis focused on the feasibility with the use of ultrasonography guidance. European Journal of Radiology. 2011;79(2):e80-e4.
31. Renzulli M, Tovoli F, Clemente A, Ierardi AM, Pettinari I, Peta G, et al. Ablation for hepatocellular carcinoma: beyond the standard indications. Med Oncol. 2020;37(4):23.
32. Iezzi R, Pompili M, Posa A, Coppola G, Gasbarrini A, Bonomo L. Combined locoregional treatment of patients with hepatocellular carcinoma: State of the art. World J Gastroenterol. 2016;22(6):1935-42.
33. Qiao A, Samuel AS, Merrill C, Brahmania M, Wilson SR. Occult Liver Nodules: their Detection and Characterization with CEUS Abdominal Radiology. 2024;In print.
34. Maruyama H, Takahashi M, Ishibashi H, Okugawa H, Okabe S, Yoshikawa M, et al. Ultrasound‐guided treatments under low acoustic power contrast harmonic imaging for hepatocellular carcinomas undetected by B‐mode ultrasonography. Liver International. 2009;29(5):708-14.
35. Chan AK, Hegarty C, Klass D, Yoshida E, Chung S, Liu DM, et al. The Role of Contrast-Enhanced Ultrasound in Guiding Radiofrequency Ablation of Hepatocellular Carcinoma. Canadian Association of Radiologists Journal. 2015;66 (2):171-8.
36. Lencioni R, Della Pina C, Bartolozzi C. Percutaneous image-guided radiofrequency ablation in the therapeutic management of hepatocellular carcinoma. Abdominal imaging. 2005;30:401-8.
37. Heimbach JK, Kulik LM, Finn RS, Sirlin CB, Abecassis MM, Roberts LR, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018;67(1):358-80.
38. Facciorusso A, Di Maso M, Muscatiello N. Microwave ablation versus radiofrequency ablation for the treatment of hepatocellular carcinoma: A systematic review and meta-analysis. Int J Hyperthermia. 2016;32(3):339-44.
39. Germani G, Pleguezuelo M, Gurusamy K, Meyer T, Isgrò G, Burroughs AK. Clinical outcomes of radiofrequency ablation, percutaneous alcohol and acetic acid injection for hepatocelullar carcinoma: a meta-analysis. J Hepatol. 2010;52(3):380-8.
40. Raoul J-L, Forner A, Bolondi L, Cheung TT, Kloeckner R, de Baere T. Updated use of TACE for hepatocellular carcinoma treatment: How and when to use it based on clinical evidence. Cancer Treatment Reviews. 2019;72:28-36.
41. EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2012;56(4):908-43.
42. Salem R, Lewandowski RJ, Kulik L, Wang E, Riaz A, Ryu RK, et al. Radioembolization results in longer time-to-progression and reduced toxicity compared with chemoembolization in patients with hepatocellular carcinoma. Gastroenterology. 2011; 140(2):497-507.e2.
43. Şen T, Tüfekçioğlu O, Koza Y. Mechanical index. Anatol J Cardiol. 2015;15(4):334-6.
44. Pang EHT, Chan A, Ho SG, Harris AC. Contrast-Enhanced Ultrasound of the Liver: Optimizing Technique and Clinical Applications. American Journal of Roentgenology. 2018;210 (2):320-32.
45. Mauri G, Porazzi E, Cova L, Restelli U, Tondolo T, Bonfanti M, et al. Intraprocedural contrast-enhanced ultrasound (CEUS) in liver percutaneous radiofrequency ablation: clinical impact and health technology assessment. Insights into imaging. 2014;5:209-16.
46. Lekht I, Gulati M, Nayyar M, Katz MD, Ter-Oganesyan R, Marx M, et al. Role of contrast-enhanced ultrasound (CEUS) in evaluation of thermal ablation zone. Abdominal radiology. 2016;41:1511-21.
47. Meloni MF, Andreano A, Franza E, Passamonti M, Lazzaroni S. Contrast enhanced ultrasound: Should it play a role in immediate evaluation of liver tumors following thermal ablation? European journal of Radiology. 2012;81(8):e897-e902.
48. Facciorusso A, Del Prete V, Antonino M, Crucinio N, Neve V, Di Leo A, et al. Post-recurrence survival in hepatocellular carcinoma after percutaneous radiofrequency ablation. Digestive and Liver Disease. 2014;46(11):1014-9.
49. Catalano O, Lobianco R, Esposito M, Siani A. Hepatocellular carcinoma recurrence after percutaneous ablation therapy: helical CT patterns. Abdominal imaging. 2001;26:375-83.
50. Kei SK, Rhim H, Choi D, Lee WJ, Lim HK, Kim Y-s. Local tumor progression after radiofrequency ablation of liver tumors: analysis of morphologic pattern and site of recurrence. American Journal of Roentgenology. 2008;190(6):1544-51.
51. Catalano O, Izzo F, Vallone P, Sandomenico F, Albino V, Nunziata A, et al. Integrating contrast-enhanced sonography in the follow-up algorithm of hepatocellular carcinoma treated with radiofrequency ablation: single cancer center experience. Acta Radiologica. 2015;56(2):133-42.
52. Radiology ACo. LI-RADS® CEUS Nonradiation TRA v2024 Core. 2024.