






Ischemic Stroke and Antiphospholipid Antibody Syndrome
Clinical and Radiological Features of Ischemic Stroke in Patients with Antiphospholipid Antibody Syndrome
Pournamy Sarathchandran1, Ahlam Almarzooqi1, Ahmed Alawadhi2, Ajith Kumar BV1
- Department of Neurology, Al Qassimi Hospital, Emirates Health Services , Sharjah, UAE
- Department of Neurology, Dubai Health, UAE
OPEN ACCESS
PUBLISHED: 30 December 2024
CITATION: SARATHCHANDRAN, Pournamy et al. Clinical and Radiological Features of Ischemic Stroke in Patients with Antiphospholipid Antibody Syndrome: A Case Series Report. Medical Research Archives, [S.l.], v. 12, n. 12, dec. 2024. Available at: <https://esmed.org/MRA/mra/article/view/6150>.
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v12i12.6150
ISSN 2375-1924
ABSTRACT
Objective: To describe the clinical, radiological, and laboratory characteristics of ischemic strokes associated with antiphospholipid antibody syndrome.
Antiphospholipid antibody syndrome (APS) is a systemic autoimmune disorder characterized by thrombotic events in both arterial and venous territories, as well as obstetric morbidity. APS is distinguished by the presence of antiphospholipid antibodies (aPLs) at moderate to high titers, which include lupus anticoagulant (LA), anticardiolipin (ACL), and anti-β2 glycoprotein I (β2GP1) antibodies. According to the Sydney-revised Sapporo criteria, APS is diagnosed when at least one clinical criterion (vascular thrombosis or pregnancy morbidity) and one laboratory criterion (persistent aPL positivity confirmed by two positive tests at least 12 weeks apart) are met.
This retrospective study reviewed medical records of patients under 45 years of age who were discharged from the stroke units of two major government hospitals in the United Arab Emirates. As part of the hospital’s acute ischemic stroke management protocol, all young patients admitted with a stroke were routinely screened for aPLs.
To ensure diagnostic accuracy, young patients with a stroke were excluded only if they attended a follow-up visit within 3 to 5 months, during which repeat aPL testing was performed to confirm the diagnosis of APS. Exclusion criteria included patients lacking
Keywords
Antiphospholipid antibody syndrome, ischemic stroke, clinical features, radiological features.
Introduction
Antiphospholipid syndrome (APS) is a systemic autoimmune disorder defined by thrombotic events in both arterial and venous territories, as well as obstetric morbidity. APS is distinguished by the presence of antiphospholipid antibodies (aPLs) at moderate to high titers, which include lupus anticoagulant (LA), anticardiolipin (aCL), and anti-β2 glycoprotein I (aβ2GPI) antibodies. According to the Sydney-revised Sapporo criteria, APS is diagnosed when at least one clinical criterion (vascular thrombosis, or pregnancy morbidity) and one laboratory criterion (persistent aPL positivity confirmed by two positive tests at least 12 weeks apart) are met. Recently, the 2023 ACR/EULAR classification criteria refined these guidelines, allowing APS classification based on a single positive aPL antibody test within three years, provided a relevant clinical criterion is present. This approach emphasizes the importance of identifying high-risk APS cases based on specific antibody profiles, such as “triple aPL positivity” (positive for LA, aCL, and aβ2GPI), which strongly predict recurrent thrombotic events and may necessitate more intensive anticoagulation strategies.
APS-associated cerebral involvement is common, with ischemic stroke or transient ischemic attack (TIA) as frequent initial presentations, occurring in up to 30% of adults with APS. Cerebrovascular events account for nearly half of the arterial manifestations in APS, with ischemic strokes constituting up to 20% of strokes in individuals under 45 years of age. Though less common, APS is more frequently associated with stroke in older males, where cerebrovascular complications are a significant concern. Additionally, APS can present with cerebral vein thrombosis (CVT), which is often the first clinical sign in roughly 80% of APS-related CVT cases.
The pathophysiology of APS-related stroke is multifaceted, with thrombosis as the most prevalent mechanism. Circulating aPLs are known to interfere with coagulation pathways, endothelial cell function, and platelet activity, leading to a pro-thrombotic state that promotes clot formation and recurrent thromboembolic events. The “two-hit hypothesis” is often cited to explain this process: the first “hit” is the asymptomatic presence of aPL antibodies in a small portion of the population, while the second “hit” is a triggering condition—such as pregnancy or infection—that initiates thrombosis. The antibodies are not only markers but active contributors to APS pathophysiology by binding to phospholipids and phospholipid-binding proteins, activating endothelial cells, platelets, and myeloid cells.
In APS patients who experience stroke, intracranial arterial occlusions or stenoses are observed in approximately 50% of cases, with the middle cerebral artery (MCA) most frequently involved. Clinical presentations of MCA involvement often include hemiparesis, dysarthria, and, if the lesion is located in the dominant hemisphere, aphasia. Stroke mechanisms also include cardioembolism, frequently linked to left-sided cardiac valve abnormalities, such as irregular valve thickening, vegetations, and dysfunction due to immune complex deposition. Chronic vasculopathy affecting small-to-medium-sized intracerebral arteries is also common, leading to lacunar or subcortical strokes. Other cerebrovascular abnormalities, including carotid or vertebral artery dissection, Sneddon’s syndrome, and Moyamoya disease, have been associated with APS.
Considering the severe risk of mortality and long-term disability in APS-related strokes, there is a pressing need to accurately identify APS patients who are at elevated risk for stroke and recurrent cerebrovascular events. Stratified treatment approaches, as recommended by recent EULAR guidelines, advocate for lifelong anticoagulation therapy in high-risk patients, while tailored management is recommended for women during pregnancy to reduce both maternal and fetal risks. This case series aims to document the clinical, radiological, and laboratory characteristics of APS-related ischemic strokes, contributing insights that align with the latest classification and management guidelines to support early identification and optimized treatment of this complex syndrome.
Materials and Methods
This retrospective study reviewed medical records of patients under 45 years of age who were discharged with a diagnosis of antiphospholipid antibody syndrome (APS) from the stroke units of two major government hospitals in the United Arab Emirates. As part of the hospital’s acute ischemic stroke management protocol, all young patients admitted with a stroke were routinely screened for aPLs.
To ensure diagnostic accuracy, inclusion criteria were set to include only patients who attended a follow-up visit within 3 to 5 months, during which repeat aPLs testing was performed to confirm the diagnosis of APS. Exclusion criteria included patients lacking follow-up antibody testing or those with incomplete clinical records.
Data were systematically collected on clinical presentation, laboratory findings, and radiological features of each patient confirmed with APS. Clinical variables included age, sex, stroke symptoms, and accompanying conditions, while laboratory parameters focused on aPLs antibody titers, platelet counts, and activated partial thromboplastin time (aPTT). Radiological data from CT and MRI scans, as well as CT angiography where available, were analyzed to characterize stroke localization and vascular occlusion patterns.
All data were handled in compliance with patient confidentiality standards, and institutional review board (IRB) approval was obtained prior to conducting the study.
Ten patients were identified with antiphospholipid antibody syndrome (APS) as the etiology of ischemic stroke, with a mean age ranging from 26 to 52 years. Among them, only one patient was more than 45 years old and had APS diagnosed with Systemic Lupus Erythematosus. The male-to-female ratio was 4:1, with eight males and two females. Majority of patients were of Asian descent. Seven patients had systemic lupus erythematosus (SLE) while the remaining nine cases were identified as primary APS.

Vascular risk factors present in patients with APS
All data were handled in compliance with patient confidentiality standards, and institutional review board (IRB) approval was obtained prior to conducting the study.
Results
Ten patients were identified with antiphospholipid antibody syndrome (APS) as the etiology of ischemic stroke, with ages ranging from 26 to 52 years (median age 34). Only one patient was more than 45 years and APL antibodies were checked since she was known with Systemic Lupus Erythematosus. The male-to-female ratio was 4:1, with eight males and two females. The majority of patients were of Asian descent. Secondary APS associated with systemic lupus erythematosus (SLE) was observed in one patient, while the remaining nine cases involved primary APS.
Vascular risk factors were present in 4 patients. One patient had diabetes mellitus and three had dyslipidemia. One patient had comorbid hypothyroidism. Lupus anticoagulant was detected in four patients, anticardiolipin antibodies in five, and β2-glycoprotein antibodies in two. The patient with SLE was positive for lupus anticoagulant and anticardiolipin and remained positive after 12 weeks. Serum C3 and C4 levels were normal, indicating that she did not have an SLE flare when she presented with stroke.
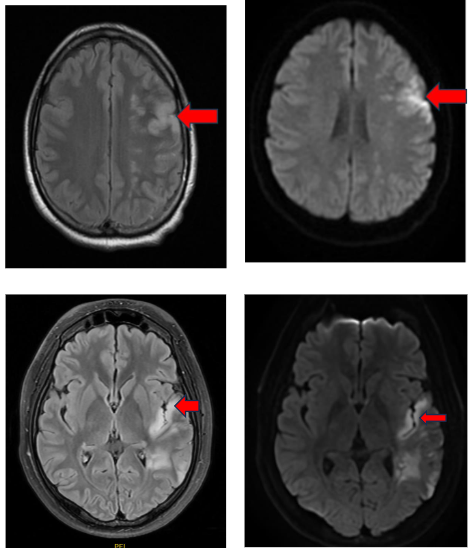
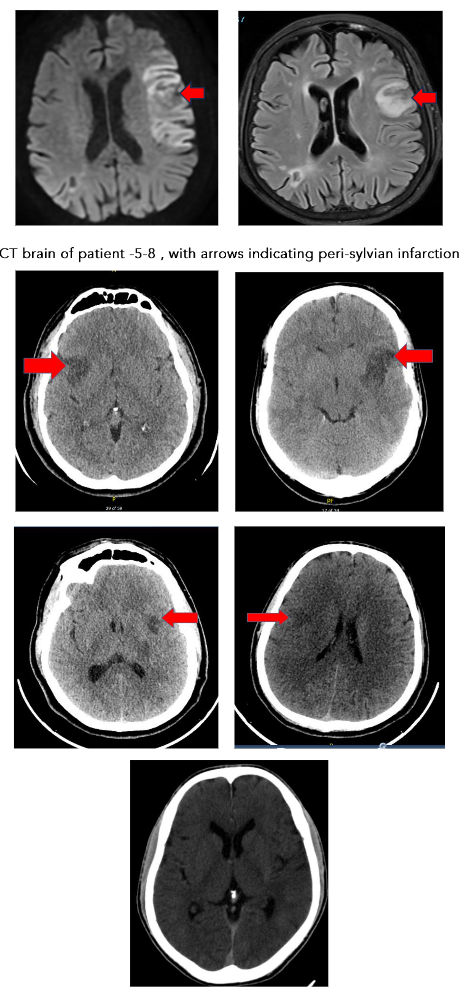
Aphasia was the most common clinical presentation, appearing in seven out of ten cases, with accompanying hemiparesis noted in four patients. Nine of the ten patients with primary APS experienced strokes in the M2 segment of the middle cerebral artery, predominantly resulting in peri-sylvian infarcts.
With a notable prevalence in the left peri-sylvian region (6 out of nine patients). Only one patient presented with a posterior circulation stroke, exhibiting a top of basilar syndrome. CT angiography revealed a left M2 occlusion in one case and distal basilar occlusion in another, while the remaining cases had no significant angiographic findings. 2D Echo was normal in all patients. TEE was done in 3 patients, which was normal. Holter study was normal in all patients.
Two patients presented within 4.5 hours of onset of symptoms. They were eligible for thrombolysis and received intravenous tissue plasminogen activator (tPA).
During hospitalization, one patient developed a pulmonary embolism characterized by pulmonary branch vein occlusion, highlighting the systemic thrombotic risks associated with APS.
Mild thrombocytopenia was observed in three patients, and six patients exhibited mild elevations in activated partial thromboplastin time (aPTT), with values ranging from 42 to 48 seconds. These findings suggest that elevated aPTT, together with thrombocytopenia, may be a sensitive indicator of underlying APS in stroke patients.
All patients were initially started on low molecular weight heparin which was switched to warfarin with target INR of 2.5–3.5. Warfarin therapy was complicated with Stevens–Johnson syndrome in one patient and changed to Rivaroxaban.
At the three-month follow-up, most had good recovery, with complete recovery noted in 7 patients.
Table 1: Demographic characteristics of patients presenting with APLA-related stroke
| Patient characteristics | Number |
|---|---|
| Age | 26 to 52 years (median age 34) |
| Sex | Male: 8 — Female: 2 |
| Ethnicity | Arab: 2 — Asian: 8 |
Table 2: Clinical characteristics of patients presenting with APLA-related stroke
| Patient characteristics | Number |
|---|---|
| Vascular risk factors | |
| Diabetes mellitus | 1 |
| Dyslipidemia | 3 |
| Comorbidities | |
| SLE | 1 |
| Hypothyroidism | 1 |
| Clinical features | |
| Aphasia | 6 |
| Dysarthria | 9 |
| Altered sensorium | 1 |
| Hemiparesis | 3 |
Arterial Territory
| Arterial Territory | Number |
|---|---|
| Left MCA (M2 segment) | 6 |
| Right MCA (M2 segment) | 3 |
| Basilar artery | 1 |
APL Antibodies
| Antibody Type | Number |
|---|---|
| Lupus anticoagulant | 4 |
| Anticardiolipin antibodies | 5 |
| β2-glycoprotein antibodies | 2 |
Lab
| Test | Range/Notes |
|---|---|
| Hemoglobin | 11 – 15.6 g/dl |
| WBC | 3600 – 13,000 /cmm |
| Platelet count (abnormal in 6) | 1.2 – 1.4 L/cmm |
| aPTT (abnormal in 6) | 42 to 56 seconds (normal 25–35 sec) |
Treatment
| Medication | Number of Patients |
|---|---|
| Warfarin | 9 |
| Rivaroxaban | 1 |
Clinical Status on Follow-up at 3 Months
| Outcome | Number of Patients |
|---|---|
| Complete recovery | 7 |
| Partial recovery | 3 |
(APL – antiphospholipid): One patient was positive for both anticardiolipin and lupus anticoagulant.
Discussion
The clinical and radiological profile of ischemic strokes associated with APS, as observed in this case series, reveals distinctive patterns in symptomatology and imaging that reinforce previous studies yet also highlight unique characteristics. The predominance of peri-sylvian infarcts in the M2/M3 segments of the middle cerebral artery, especially affecting the left hemisphere, aligns with findings that cortical strokes with aphasia as the primary presentation are often linked to embolic strokes. Studies have similarly observed that ischemic events in APS patients tend to exhibit neuroimaging patterns indicative of embolic mechanisms, often resembling cardioembolic stroke distributions. This correlation emphasizes the role of APS as a prothrombotic condition with implications for early detection and management of stroke in young patients, regardless of traditional vascular risk factors.
Although APS is recognized as a significant risk factor for cerebrovascular events, detailed data characterizing CNS-specific manifestations are sparse, especially regarding how APS-related thrombotic patterns differ from other prothrombotic conditions. Liu et al. recently highlighted that CNS involvement in APS is both common and complex, identifying several risk factors that influence prognosis in patients with CNS manifestations of APS, including stroke. Their findings underscore the importance of thorough diagnostic evaluation, as CNS presentations of APS are often heterogeneous and may involve multiple cerebrovascular territories or atypical patterns not typically observed in other forms of stroke.
However, this complexity in presentation also complicates establishing a standardized neuroimaging profile for APS-related strokes—a gap this case series partially addresses by highlighting the peri-sylvian and left MCA (M2/M3) dominance seen in our patients. While promising, further studies are needed to validate these neuroimaging patterns as diagnostic markers for APS-related stroke and to understand how different risk factors, such as antibody profiles, impact stroke severity and recurrence risk.
The “two-hit” hypothesis, where the presence of aPLs represents the first “hit,” followed by a secondary trigger like infection or inflammation, is often cited
To explain thrombotic events in APS. However, this model is largely theoretical in the context of CNS thrombotic involvement, and clinical evidence directly supporting it in cerebral APS remains sparse. The precise role of circulating aPLs and other biomarkers (e.g., elevated aPTT, thrombocytopenia) in CNS thrombosis is also unclear, as most data on these markers stem from systemic rather than CNS-specific studies. In this case series, elevated aPTT and mild thrombocytopenia were frequently observed, suggesting that these markers may have diagnostic value. Nonetheless, the sensitivity and specificity of these laboratory findings in predicting APS-related strokes, particularly among young patients with unexplained ischemic events, require further validation.
Despite a growing understanding of APS, there remains no unified approach to diagnosis and management of APS-related ischemic events, as highlighted in a recent survey conducted by the International Society on Thrombosis and Haemostasis (ISTH) Subcommittee on Lupus Anticoagulant/Antiphospholipid Antibodies. This survey, led by Cohen et al., revealed significant variability in antithrombotic treatment strategies for APS patients with ischemic stroke, underscoring the need for standardized guidelines specific to APS-related CNS involvement. The study further emphasized the clinical importance of differentiating APS-related thrombotic events from other types of arterial thromboembolism, as therapeutic responses can vary greatly based on etiology. For instance, APS patients often require higher-intensity anticoagulation, and the choice between warfarin and direct oral anticoagulants (DOACs) remains controversial. In our cohort, one patient who developed Stevens–Johnson syndrome following warfarin therapy had to switch to rivaroxaban, reflecting the complexities involved in long-term management for APS stroke patients.
The current reliance on generalized stroke protocols for neuroimaging in APS patients may overlook subtle yet potentially characteristic imaging findings associated with APS-related strokes. For example, small lesion size and the absence of major artery occlusions, as noted in our series, suggest a possible distinction from classic cardioembolic or large artery atherosclerotic strokes. Pierik et al. highlighted similar variability in cardioembolic stroke presentations, suggesting a need for tailored imaging protocols for APS-related strokes to capture these nuances. The work by Cohen et al. underscores that APS diagnosis and treatment lack uniform protocols, especially regarding specific neuroimaging features or biomarkers. They suggest standardized imaging protocols for APS-related stroke, particularly those combining vessel wall imaging and perfusion studies, which could advance diagnostic accuracy.
This case series emphasizes the need for larger, multicenter studies to establish a more detailed clinical and imaging profile for APS-associated CNS involvement. Such research could explore whether specific antibody profiles or laboratory markers (e.g., elevated aPTT, triple positivity) correlate with distinct neuroimaging findings, ultimately aiding clinicians in distinguishing APS-related stroke from other causes. Insights from both Liu et al. and Cohen et al. underscore the urgency of this work, as variability in treatment strategies reflects the need for clearer guidelines that can standardize the approach to APS in stroke patients. Integrating aPL testing into the diagnostic workup could enhance early detection and allow for timely intervention.
Recent studies emphasize the importance of specific MRI findings in diagnosing APS-related CNS involvement. Graf (2017) underscores the role of MRI in detecting small, scattered ischemic lesions, often located in cortical and subcortical regions, which are indicative of embolic phenomena. These findings align with the peri-sylvian infarct patterns noted in this case series.
Advanced imaging techniques, such as diffusion-weighted imaging (DWI), provide additional diagnostic value. DWI often reveals acute ischemic lesions in multiple vascular territories, which are characteristic of APS-related strokes and highlight the embolic origin associated with aPLs.
White matter hyperintensities (WMHs) on T2-weighted MRI are also frequently observed in APS patients, even among those without conventional vascular risk factors. Zhao et al. (2024) suggest integrating vessel wall imaging and perfusion studies into routine practice to enhance diagnostic accuracy.
Conclusion
Ischemic strokes associated with antiphospholipid antibody syndrome (APS) predominantly localize to the peri-sylvian region within the M2/M3 branches of the middle cerebral artery, exhibiting clinical and radiological features that closely resemble those of cardioembolic strokes. Elevated aPTT and thrombocytopenia were observed as potentially sensitive laboratory markers indicative of APS. Early identification and management of APS in these patients may reduce the risk of recurrent thrombotic events and improve clinical outcomes.
Conflict of interest:
The authors have no conflicts of interest to declare.
Funding statement:
No funding received.
References
1. Miyakis, Spiros, Michael D. Lockshin, Tsutomu Atsumi, D. Ware Branch, Rebecca L. Brey, Ricard Cervera, Robbert H. W. M. Derksen, Pieter G. DE Groot, Tsuyoshi Koike, Pier Luigi Meroni, Gilles Reber, Yehuda Shoenfeld, Angela Tincani, Panayiotis G. Vlachoyiannopoulos, and Samuel A. Krilis. “International Consensus Statement on an Update of the Classification Criteria for Definite Antiphospholipid Syndrome (APS).” Journal of Thrombosis and Haemostasis 4, no. 2 (2006): 295-306. https://doi.org/10.1111/j.1538-7836.2006.01753.x.
2. Gaspar, Paulo, Hannah Cohen, and David A. Isenberg. “The Assessment of Patients with the Antiphospholipid Antibody Syndrome: Where Are We Now?” Rheumatology 59, no. 7 (2020): 1489-1494. https://doi.org/10.1093/rheumatology/keaa172.
3. Xourgia, Eleni, and Maria G. Tektonidou. “An Update on Antiphospholipid Syndrome.” Current Rheumatology Reports 23, no. 12 (2022): 84. https://doi.org/10.1007/s11926-021-01051-5.
4. Cervera, Ricard, Maria Chiara Boffa, Munther A. Khamashta, and Graham R. Hughes. “The Euro-Phospholipid Project: Epidemiology of the Antiphospholipid Syndrome in Europe.” Lupus 18, no. 10 (2009): 889-893.
https://doi.org/10.1177/0961203309106832.
5. Barbhaiya, Medha, Sylvie Zuily, Rodney Naden, Allan Hendry, Fanny Manneville, Maria C. Amigo, Zahir Amoura, et al. “2023 ACR/EULAR Antiphospholipid Syndrome Classification Criteria.” Annals of the Rheumatic Diseases 82, no. 10 (2023): 1258-1270. https://doi.org/10.1136/ard-2023-224609.
6. Tektonidou, Maria G., Laura Andreoli, Zahir Amoura, Ricard Cervera, Nathalie Costedoat-Chalumeau, Munther A. Khamashta, Marc J. Cuadrado, et al. “EULAR Recommendations for the Management of Antiphospholipid Syndrome in Adults.” Annals of the Rheumatic Diseases 78, no. 10 (2019): 1296-1304.
https://doi.org/10.1136/annrheumdis-2019-215213.
7. Jerez-Lienas, Alicia, Amelie Mathian, Julien Aboab, Isabelle Crassard, Marc Hie, Florence Cohen-Aubart, Jérôme Haroche, et al. “Cerebral Vein Thrombosis in the Antiphospholipid Syndrome: Analysis of a Series of 27 Patients and Review of the Literature.” Brain Sciences 11, no. 12 (2021): 1641. https://doi.org/10.3390/brainsci11121641.
8. Fan, Yangyi, Yicheng Xu, Sifan Zhang, Xiaodong Song, Zunjing Liu, Wenjun Tu, and Chun Li. “Stroke and Risk Factors in Antiphospholipid Syndrome.” Journal of Personalized Medicine 14, no. 1 (2024): 24.
https://doi.org/10.3390/jpm14010024.
9. Knight, Jason S., and Yogesh Kanthi. “Mechanisms of Immunothrombosis and Vasculopathy in Antiphospholipid Syndrome.” Seminars in Immunopathology 44, no. 3 (2022): 347-362. https://doi.org/10.1007/s00281-022-00916-w.
10. Cohen, Hannah, David J. Werring, Amit Chandratheva, Paras Mittal, Koen M. J. Devreese, David A. Isenberg, and the ISTH SSC Lupus Anticoagulant/Antiphospholipid Antibodies Subcommittee Study Group. “Survey on Antiphospholipid Syndrome Diagnosis and Antithrombotic Treatment in Patients with Ischemic Stroke, Other Brain Ischemic Injury, or Arterial Thromboembolism in Other Sites: Communication from ISTH SSC Subcommittee on Lupus Anticoagulant/Antiphospholipid Antibodies.” Journal of Thrombosis and Haemostasis 21, no. 10 (2023): 2963-2976. https://doi.org/10.1016/j.jtha.2023.06.020.
11. Leal Rato, Margarida, Mariana Bandeira, Vanessa C. Romão, and Diana Aguiar de Sousa. “Neurologic Manifestations of the Antiphospholipid Syndrome – an Update.” Current Neurology and Neuroscience Reports 21, no. 8 (2021): 41. https://doi.org/10.1007/s11910-021-01124-z.
12. Ricarte, Isabel F., Cecilia Marino, Maria Rosa Maccarrone, Roberto Testa, Giacomo Lana-Peixoto, Graciela S. Alarcon, and Gustavo C. Alonso. “Neurologic Manifestations of Antiphospholipid Syndrome.” Lupus 27, no. 9 (2018): 1404–1414. https://doi.org/10.1177/096120331877611.
13. Liu, Min, Gaoming Li, Xun Song, Yangyi Fan, and Chun Li. “Prevalence, Risk Factors, and Prognosis of Central Nervous System Manifestations in Antiphospholipid Syndrome.” Scientific Reports 13, no. 1 (2023): 8915.
https://doi.org/10.1038/s41598-023-35955-2.
14. Engelter, Stefan T., Matthias Gostynski, Steffen Papa, Mirjam Frei, Christoph Born, Vladeta Ajdacic-Gross, Hans Peter Schroth, et al. “Epidemiology of Aphasia Attributable to First Ischemic Stroke: Incidence, Severity, Fluency, Etiology, and Thrombolysis.” Stroke 37, no. 5 (2006): 1379-1384. https://doi.org/10.1161/01.STR.0000221815.64093.8c.
15. Pierik, Ramon, Ale Algra, Ewoud van Dijk, Michiel E. Erasmus, Isabella C. van Gelder, Peter J. Koudstaal, Gert-Jan R. Luijckx, et al. “Distribution of Cardioembolic Stroke: A Cohort Study.” Cerebrovascular Diseases 49, no. 1 (2020): 97-104. https://doi.org/10.1159/000505616.
16. Graf, J. “Central Nervous System Manifestations of Antiphospholipid Syndrome.” Rheumatic Diseases Clinics of North America, vol. 43, no. 4, 2017, pp. 547-560. https://doi.org/10.1016/j.rdc.2017.06.004.
17. Charitha, K., et al. “Precision Imaging in Neurodegeneration: The Superiority of Diffusion Tensor Imaging Over Conventional MRI in Differentiating Parkinson’s Disease From Atypical Parkinsonian Syndromes.” Cureus, vol. 16, no. 9, 2024, e68933. https://doi.org/10.7759/cureus.68933.
18. Zhao, J., et al. “Dancing with Disorder: Chorea – an Unusual and Neglected Manifestation of Antiphospholipid Syndrome.” Lupus Science & Medicine, vol. 11, no. 2, 2024. https://doi.org/10.1136/lupus-2024-001332.