

Lessons from India’s COVID-19 Management for Health Pros
Lessons from India’s Experience Managing the COVID-19 Pandemic
R.V. Rajeev Gowda1, Tanika Chand Thangiah2, and Saumya Varma3
- Former Member of Parliament, Rajya Sabha;
- Public Health and Policy Researcher
- Public Policy Consultant
OPEN ACCESS
PUBLISHED: 31 October 2024
CITATION: Gowda, MVR., Chandna, T., et al., 2024. Lessons from India’s Experience Managing the COVID-19 Pandemic. Medical Research Archives, [online] 12(10).
https://doi.org/10.18103/mra.v12i10.5778
COPYRIGHT © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i10.5778
ISSN 2375-1924
Abstract
The Indian government’s initial narrative on its response to the COVID-19 pandemic paints a picture of commendable crisis management and effective governance, lauded globally. This narrative ignores the flaws in the government’s coping strategies, which resulted in unprecedented levels of morbidity and mortality among millions of Indians and a massive underreporting of deaths. The government’s actions during the pandemic highlight its success and challenges. This paper draws attention to systemic shortcomings and the lessons learned from the COVID-19 pandemic in order to improve future responses to manage crises.
Keywords
- COVID-19
- India
- Public Health
- Crisis Management
- Vaccination
1. Introduction, Scope, and Methodology
India’s first confirmed case of COVID-19 on January 30, 2020, was a student who had returned from Wuhan, China, the epicentre of the global outbreak. As of August 18, 2024, India reported a total of 45.04 million confirmed cases¹ and 533,638 deaths², the third-highest number of confirmed cases globally. However, the World Health Organization (WHO) estimates that COVID-19 resulted in approximately 4.7 million excess deaths in India³.
India’s response to the COVID-19 pandemic is a tale of two narratives. The government’s account highlights its success and global leadership; our approach pays attention to systemic shortcomings and punctures propaganda so policymakers can learn appropriate lessons to manage future crises.
This article critically examines India’s response to the COVID-19 pandemic with a focus on the research question of what lessons can be learned to inform resilient policymaking to cope with future health crises. Its methodology is qualitative, primarily based on the authors’ insights as policy professionals analysing the pandemic response in real-time and generating constructive policy intelligence. These observations are supported by secondary research.
2. The Indian Government’s Pandemic Response
The Indian government had the advantage of observing the course of the outbreak in other countries for a few weeks. Yet, it did not act with urgency, learn lessons from other countries’ experiences, and implement the 3Ts – Testing at scale, Tracing with diligence, and Treating with precision. Thereafter, its response was marked by inefficiency, inconsistency, extravagant claims, and ad-hoc crisis management.
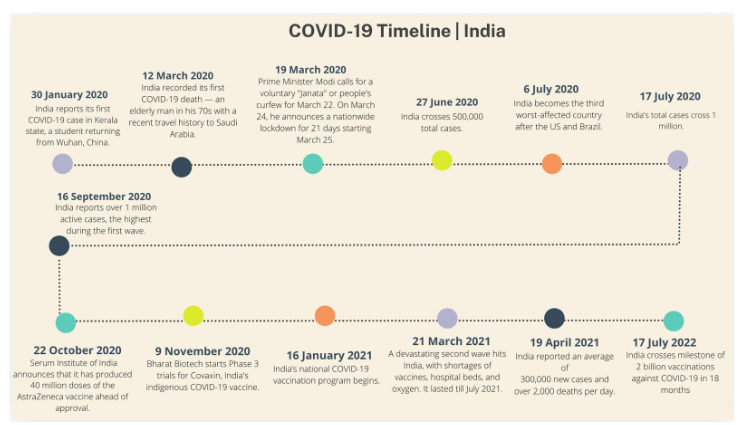
Figure 1: Timeline of key milestones during the COVID-19 pandemic in India
Early Inaction
In January 2020, as the virus was spreading in China and Hong Kong, the Indian government initiated screenings for international passengers arriving from those regions. However, according to World Health Organization (WHO) guidelines, airport screenings are not considered epidemiologically effective. A more effective approach would have involved screening all international passengers, imposing quarantines when necessary, and coordinating with state governments to share information about individuals at risk, allowing for appropriate follow-up actions. Experts, at that time, had recommended testing symptomatic individuals regardless of travel history, but this was not implemented, leading to serious lapses in case. According to the Indian Council of Medical Research’s (ICMR) mathematical model in February 2020, this approach could have identified 50% of all infections in India during the early months of the pandemic. The study also acknowledged that India was utilising only up to 10% of its COVID-19 testing capacity at that time⁴.
Right from the pandemic’s onset, the government ignored warnings from experts and political leaders from the Opposition⁵. Allegedly, the government chose to defer action until it had succeeded in destabilising the opposition-led government in Madhya Pradesh state⁶. The government also dragged its feet on a response plan⁷. Only on March 3, 2020, did Prime Minister (PM) Narendra Modi publicly acknowledge the COVID-19 issue, despite cases already being reported in India.
Ill-Planned Lockdown
On the evening of March 24, 2020, PM Modi announced a sudden, strict lockdown from midnight, which would be effective from the next morning⁸˒⁵. The decision to implement a lockdown was not based on the advice of any public health experts. The lockdown was deemed as the ‘strictest’ across the globe, earning a score of 100 on Oxford University’s Stringency Index⁹. The lockdown resulted in the closure of all non-essential services, public transport, and educational institutions. While the government framed this as a proactive measure to protect public health, the abruptness of the lockdown led to significant chaos, particularly among migrant workers living and working in major cities. Millions were stranded without jobs or means to return home, leading to one of the largest migrations¹⁰ since India’s partition in 1947, as workers attempted to walk long distances to their native villages.
The government disregarded epidemiologists’ recommendations to conduct door-to-door screenings to detect the virus early¹¹. It also overlooked expert advice on the limited effectiveness of lockdowns. Although the lockdown provided the government with time to improve testing and hospital facilities, it resulted in significant social costs without corresponding gains in disease control.
The government projected this as resilience. News headlines were filled with messages of effective crisis management and successful governance. The government proclaimed¹² India’s response as exemplary, a model for other nations to follow. In October 2020, PM Modi, in an interview, stated, “We not only got the broad timing of various phases of lockdown right, we also got the unlock process right”¹³. However, the reality was different on the ground. Critics argue that the government’s narrative deliberately overlooked systemic failures, including inadequate healthcare infrastructure, delayed responses, and a lack of support for vulnerable populations, leading to severe humanitarian crises.
Unplanned Unlock: Inadequate Preparedness
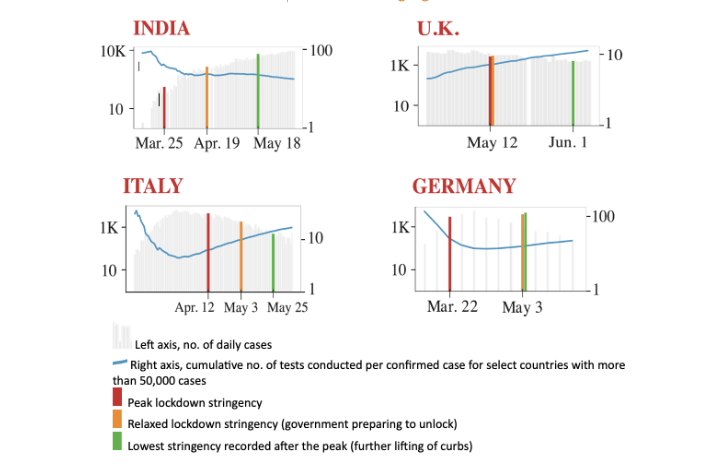
Compounding the sudden, stringent lockdown was the government’s unplanned and ill-prepared unlock strategy, which began in June 2020 at a time when cases were rising at a startling rate. A comparison of India’s lockdown and unlock in relation to the trends in other countries reveal that no caution was exercised, nor were lessons learned from other countries’ experiences.
INADEQUATE TESTING AND HEALTHCARE FACILITIES
During the early phase of the pandemic, India had limited testing capacity. By the end of March 2020, the daily testing capacity was approximately 5,500 tests¹⁵ across all laboratories, which was drastically insufficient for a nation of 1.4 billion people and the nature of the virus’s spread. The ICMR initially restricted testing to individuals with a travel history to high-risk countries or those showing symptoms. This meant many cases went undetected, particularly in the early stages of community transmission.
The low number of tests conducted resulted in a significant underreporting of COVID-19 cases. As of early June 2020, India had conducted approximately 3.8 million tests, far below the recommended levels to monitor the outbreak adequately¹⁶. The testing rate in India was only 0.08 tests per 1,000 people. In comparison, the United States and Italy had rates of 1.16 and 1.02 respectively¹⁶. This disparity highlights the inadequacy of India’s testing strategy.
During this period, Indian hospitals and healthcare workers struggled to access basic supplies like PPE, as India imported most PPE components and permitted the export of these products with a view toward revenues¹⁷. Domestic production was scaled up only much later. An online survey conducted amongst healthcare professionals found only 20% had regular access to N95 masks, and over 35% of respondents expressed fears over the quality and safety of PPE kits they had received¹⁸.
As a result, by October 2020, with 8 million confirmed cases, India became the second most affected country globally¹⁹. The government claimed that the pandemic had peaked in India and that the number of cases would soon decline. Experts, health economists, and epidemiologists countered that the true peak could only be determined by analysing factors such as serological surveys and testing patterns. Based on such data, they contended that the first wave had not yet peaked.
Serological surveys revealed a significant discrepancy between the expected number of COVID-19 cases and the official numbers reported through RT-PCR and rapid antigen tests. As reported in the Indian National Congress party in June 2021²⁰, the first national seroprevalence survey in June 2020 showed that seroprevalence stood around 0.73%
early May 2020, compared to 52,592 cases reported. This alarming contrast was likely due to restricted generalised testing and the low number of tests conducted until July 2020, whereby many asymptomatic individuals were not tested.
A crucial gap was the inadequate communication regarding the prevention of virus spread through asymptomatic individuals. More effective behaviour change-oriented communication was necessary to ensure that people consistently avoided crowds, wore masks at all times, and isolated themselves at the first sign of any symptoms. The lack of strong messaging in these areas contributed to the virus spreading unchecked, particularly through asymptomatic carriers.
The absence of investment in urban primary care, including the virtual abandonment of the National Urban Health Mission, significantly hindered the early detection and containment of COVID-19. The virus, which initially spread through large cities, warranted intensive primary care efforts to detect and stall its progression. The lack of symptom-based syndromic surveillance by primary care teams was particularly damaging, as it allowed the virus to spread unchecked in cities. Despite testing, the absence of such surveillance weakened containment, contributing to the rapid spread of the virus. Additionally, there is no clear correlation between high COVID-19 testing rates and lower mortality, highlighting the limitations of relying solely on testing.
Lack of Consistent and Appropriate Leadership
The government designated ICMR, a government research organisation, as the primary agency to manage the pandemic instead of the more appropriate and experienced National Centre for Disease Control (NCDC). The ICMR was asked to procure test kits centrally rather than decentralising procurement to states. This effort failed and cost precious time.
Initially, ICMR representatives attended briefings of the Ministry of Health and Family Welfare (MoHFW) and provided essential medical expertise. However, when journalists began questioning the accuracy of rapid diagnostic test kits procured from China, the ICMR representatives stopped attending these briefings. Bureaucrats without medical expertise were left to field questions, leading to a significant gap in authoritative medical communication.
From mid-May, the briefings by the Ministry of Health became increasingly irregular, without any explanation. At times, the gap between live briefings stretched as long as 12 days. In lieu of live sessions, written updates were released, which failed to provide the same level of engagement and immediate response that live briefings could offer.
In May, after only a month of operation, the ICMR disbanded an expert panel that had been appointed to investigate COVID-19 drugs and vaccines. This panel was part of the National COVID-19 Task Force and had convened only three times before being disbanded. This abrupt decision removed a key mechanism for expert scientific input during critical efforts to combat the pandemic.
On May 30, the Indian Public Health Association, Indian Association of Preventive and Social Medicine, and Indian Association of Epidemiologists issued a critical statement²¹. They suggested that if the government had consulted epidemiologists with a better understanding of disease transmission dynamics, rather than relying primarily on clinicians and academic epidemiologists with limited field training, its response might have been more effective.
Moreover, the decision to have the National Disaster Management Authority (NDMA) manage the pandemic response resulted in suboptimal outcomes. Instead of trained public health personnel, police officers were tasked with conducting contact tracing, leading to inefficiencies and a lack of effective disease control measures.
3. The Second Wave
Despite data emerging from the United Kingdom (UK) in December 2020 of a virulent strain, the government ignored warning signs. In February 2021, the Indian SARS-CoV-2 Genomics Consortium (INSACOG), even warned the government about the impending second wave. Despite scientific advice, the government refused to consider cessation of public events or another lockdown and continued with the Kumbh Mela festival and elections to the legislative assembly in West Bengal state. The Kumbh Mela saw approximately 9.1 million pilgrims, with thousands testing positive for COVID-19²², while election rallies in West Bengal led to daily cases surging from around 200 in mid-March to over 17,000 by late April 2021²³.
The second wave started in March 2021, straining the healthcare system, leading to shortages of oxygen, hospital beds, and essential medicines. By April 19, 2021, India reported an average of 300,000 new cases and over 2,000 deaths per day. The wave peaked on April 30, 2021, when over 400,000 new cases were recorded and more than 3,500 people died²⁴. The more transmissible Delta variant, massive public gatherings for festivals and elections, and complacency following the decline of cases after the first wave were key factors that led to the surge. The Delta variant spread rapidly, particularly in the states of Maharashtra, Delhi, Uttar Pradesh, and Karnataka.
Testing infrastructure, though significantly ramped up after the first wave, struggled to keep pace with the surge. Despite conducting over 1.5 million tests daily, the sheer volume of cases led to a testing positivity rate exceeding 30% in several states, indicating widespread community transmission. The lag in obtaining results of testing further exacerbated the situation, as many infected individuals continued to interact within their communities, unknowingly spreading the virus.
Hospitals in major cities were quickly overwhelmed and faced critical shortages of Intensive Care Unit (ICU) beds, ventilators, and essential medicines like Remdesivir. The oxygen crisis became the most alarming aspect of the second wave. As demand for medical oxygen surged, hospitals began to run out of supplies, resulting in preventable deaths. The government attempted to address this by setting up “oxygen express” trains, importing oxygen concentrators, and repurposing industrial oxygen for medical use, but these efforts were too late to prevent the loss of lives.
It is also relevant to briefly mention the immense economic impact of the lockdown on the country. Except for agriculture, there was a significant downturn in economic activities, and the economy contracted by 7.3% during the 2020–21 financial year²⁵. In response, the government announced special fiscal packages to revive the economy. These packages failed to provide adequate, urgently required support to the health sector and social protection for vulnerable populations. The actual fiscal cost of the package announced during the first wave in 2020 was likely just over 10% of what was announced by the government and equivalent to only 1% of GDP²⁶. During the second wave in 2021, the Union government announced a few short-term measures, most notably credit guarantees, but there were no substantial long-term measures to enhance economic growth.
Despite the weaknesses of the public health system revealed by the pandemic, only one measure was announced for strengthening public health. This was an INR 232.2 billion credit guarantee scheme for public health infrastructure and human resources, of which the Union government’s share was INR 150 billion²⁷. This scheme focused on short-term emergency preparedness, personnel augmentation, equipment, medicines, tele-consultations, ambulance services, testing and diagnostics capacity, and surveillance and genome sequencing.
By mid-April, India was reporting over 2,000 deaths per day, with the highest single-day death toll reaching 3,523 on April 30, 2021²⁸. These numbers reflected only reported deaths. There was significant underreporting, particularly in rural areas where healthcare access and record-keeping were more limited²⁹. The WHO later estimated that excess mortality during this period could be several times higher than the reported figures, and millions of deaths gone may have gone unreported.
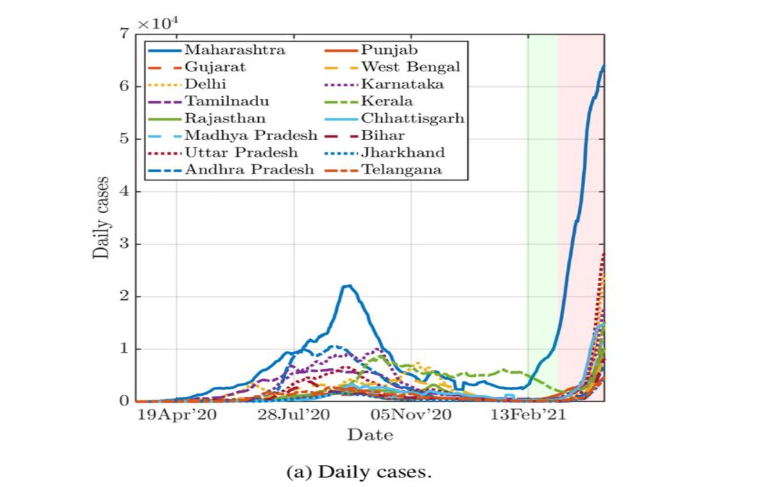
Figure 3 illustrates that the second wave’s impact was more severe and widespread than the first, as indicated by the steep upward trajectories across multiple states.
The vaccination campaign, which began in January 2021, was initially slow to scale up. By mid-April, less than 8% of the population had received at least one dose of the vaccine. As the second wave escalated, the government expanded vaccine eligibility, but supply shortages and logistical challenges hampered the campaign’s effectiveness (analysed in detail in Section 5). The decision to open vaccinations to all adults on May 1 led to increased demand that the system was not prepared to meet, resulting in frustration and delays.
The government had not adequately anticipated the need for increased oxygen production and distribution. The centralised approach to oxygen allocation caused delays in getting supplies to the states most in need, leading to tragic consequences as hospitals ran out of oxygen, causing patient deaths.
Lack of coordination between the Union and state governments further complicated the response. States were often left to manage the crisis on their own, leading to discrepancies in the availability of resources, testing, and treatment, contributing to the uneven impact of the second wave. Some states fared worse than others due to inadequate support and resources. Further, the introduction of wastewater surveillance, a crucial tool for monitoring viral spread, was delayed until a late stage of the pandemic.
4. The Vaccine Programme
India is renowned for its Universal Immunisation Programme. This strength, from research and development to final deployment of one of the largest vaccination drives in the world, was not harnessed fully. Scientific planning and preparation could have avoided months of missed opportunities, vaccine shortages, and policy flip-flops across all four dimensions of an effective immunisation strategy — development and production; procurement and affordability; allocation; and deployment³².
drew up a tentative timeline for its vaccine programme only by early October 2020 and placed its first orders in January 2021. Despite knowing in October that only two entities, Serum Institute of India (SII) and Bharat Biotech, could produce the first doses of the vaccines, the government failed to provide financial support to either institute to scale up production capacity in anticipation of demand³³. Initially, the government only funded the mandatory bridging trial for SII’s Covishield in India³⁴ despite SII, the world’s largest vaccine manufacturer, expected to be a major producer for vaccination drives globally.
Figure 4: Early Procurement Deals for Covid-19 Vaccines.
Data: Madur GS, 2021³⁵
| Country | Timeline | Vaccine Candidates | Total Doses Procured Early (Millions) |
|---|---|---|---|
| UK | May to Aug 14 2020 | 3 | 150 |
| USA | Jul to Aug 2020 | 4 | 400 |
| EU | Aug to Nov 2020 | 3 | 800 |
| Australia | Sep 2020 | 1 | 33.8 |
| Brazil | Aug 2020 | 1 | 90 |
| Germany | Sep 2020 | 1 | 30 |
| Japan | Jul to Oct 2020 | 3 | 220 |
| India | Jan 2021 | 2 | 16.5 (first order) |
In hindsight, the government’s lack of urgency may be partly explained by the “smart vaccination strategy” reported in December 2020³⁶, whereby only targeted groups would be vaccinated to break the chain of transmission. This strategy possibly resulted in the subsequent failure to plan and procure sufficient doses of vaccines²⁰.
There were also concerns and policy flip-flops with the vaccine candidates being considered. For example, the government approved Emergency Use Authorisation (EUA) for both Covishield and Bharat Biotech’s COVAXIN by January 2021 before either had concluded Phase III trials, and before efficacy data for these Phase III trials were made public³⁷.
Finally, while global restrictions on exports of raw materials impacted their availability, this was foreseeable and could have been addressed through proactive diplomacy. Only after the Chief Executive Officer of SII tweeted a direct request to the President of the United States of America (USA) on April 16, 2021, to lift export restrictions, did the government take up the issue. President Biden lifted the ban 10 days later³⁸.
Ignoring Early Warnings
As early as February 2021, government officials had informed the Parliamentary Standing Committee on Science and Technology that there would be vaccine shortages if the vaccination programme was extended beyond priority groups³⁹. The Committee recommended that the Department of Biotechnology strengthen efforts for ramping up production capacity for the two approved vaccines⁴⁰. It also recommended that the Department “provide all research, laboratory infrastructure and capacity building support to the other vaccine candidates in the pipeline.” However, the government did not take concrete action until late April 2021 when an acute shortage of vaccines became evident.
Procurement issues notwithstanding, the government proactively leveraged India’s existing public digital platforms and invited private sector innovation to develop the COVID Vaccine Intelligence Network (CoWIN) system. This digital platform, launched in January 2021, provided end-to-end functionality for India’s vaccination programme. For administrators, it supported stock management, real-time publication of vaccine schedules, and real-time data reporting. For citizens, it supported registration, appointment booking, and instant vaccination certifications. Its features were also updated at every phase of the vaccination programme to increase its efficiency. For example, online-only registration was replaced with blended registration to cater to walk-ins.
Modified Vaccine Strategy
The government’s vaccination policies were often inconsistent. It abruptly changed course on April 19, 2021, with two unprecedented decisions under the “Liberalised Pricing and Accelerated National COVID-19 Vaccination Strategy.” First, it opened vaccination for people in the 18–44 age group alongside existing priority groups. (Initially, vaccination was limited to health care workers, people above 60 years and those below 60 years with comorbidities)⁴¹. Second, it made states partly responsible for procuring their own doses. This deviated from international best practice wherein national governments procured vaccines and state and local authorities ensured deployment. Over-reliance on the private sector for vaccine distribution led to inequities in access.
Figure 5: Vaccine prioritisation and allocation plan in India.
Source: Singh, K., Verma, A., & Lakshminarayan, M. (2022)⁴¹
| Phase | Commencement date | Priority group | Eligible population (million) | % of total population |
|---|---|---|---|---|
| 1a | January 16, 2021 | Health care workers | 10 | 0.73 |
| 1b | February 2, 2021 | Frontline workers | 20 | 1.46 |
| 2a | March 1, 2021 | Senior citizens (≥60 years) & those above 45 years with defined comorbidities | 138 | 10.07 |
| 2b | April 1, 2021 | Population 45–59 years of age | 209 | 15.27 |
| 3 | May 1, 2021 | Population 18–44 years of age | 597 | 43.57 |
| 4a | January 3, 2022 | Population 15–18 years of age | 74 | 5.41 |
| Total | 1,018.81 | 74.32 | ||
| 4b | January 10, 2022 | Health care workers and frontline workers | 28⁴¹ | |
| Senior citizens (≥60 years) | 137 | |||
| 5 | March 16, 2022 | Population 12–14 years of age | 46 | 3.39 |
| Total Doses Required | 77.71 |
The Union government announced it would procure 50% of vaccine doses from manufacturers while the remaining 50% would be sold in the open market to state governments and private entities. State governments were not given any priority over private hospitals. The sharing ratio of vaccines between the three entities was 50:25:25⁴², placing private hospitals at par with state governments despite the latter providing an essential public service by administering vaccines at low cost or for free.
This ill-conceived policy resulted in a drop in daily vaccination rates in May 2021. States failed to procure their supply directly from vaccine producers, and vaccine supply was concentrated among corporate hospitals in big cities⁴³.
Supreme Court Review Order
Concern over the lack of a clear vaccine programme and a disorganised vaccination drive led to the Supreme Court questioning the Union government and ordering a review of its vaccine policy in June 2021. The Supreme Court termed the Modified Vaccination Strategy “arbitrary and irrational” on May 31, 2021, and ordered the Union Government to review it by June 13, 2021⁴⁴.
policy was partially rolled back on June 7, 2021, when PM Modi announced that the sharing ratio would be changed to 75:25 with 75% direct procurement by the Union government and the remainder for direct purchase by private hospitals. The government’s policy flip flops cost the country two-and-a-half months of avoidable confusion.
Vaccine Shortages in Supply to States
Following the partial rollback of the liberalised vaccine policy, states like West Bengal, Delhi, Gujarat, Jharkhand, Maharashtra, Tamil Nadu, and Orissa continued to face a shortage of vaccines due to slow supply from the Union government.
Unscientific Estimations
The government significantly overestimated the country’s capacity to produce vaccine doses. In May 2021, it claimed that India would produce 2.16 billion vaccine doses between August–December 2021⁴⁵. Just one month later, the MoHFW stated in its affidavit to the Supreme Court that 1.86 to 1.88 billion doses would be required to fully vaccinate all adults with two doses by the end of 2021. Of this requirement, 516 million would be made available by July 31, 2021. 1.35 billion doses would be required for the rest of the year⁴⁶.
This was 810 million doses less than the original estimate of 2.16 billion doses to be manufactured during this period. Further, the calculation was based on exactly twice the eligible population, failing to account for the extra doses needed due to vaccine wastage (MoHFW admitted that the national vaccine wastage rate was 6.3%, and even 37.3% in Jharkhand state)⁴⁷. The Chairman of the National Empowered Group on Vaccine acknowledged in November that the original estimate was an “optimistic, aspirational assessment” based on the word of vaccine manufacturers⁴⁸.
Distribution Failures
The distribution of the vaccine was inequitable. First, the vaccination drive had a consistent urban bias. In May 2021, 30.3 doses were administered per 100 persons in urban areas against just 12.7 in rural areas⁴⁹. This 2.5 times gap between the two remained constant from January 2021, highlighting consistent neglect of rural India, even as the pandemic spread to villages.
Second, there was a digital and class divide among vaccine recipients. The online registration process and lack of awareness resulted in class-based exclusion. Even where on-the-spot registration was conducted, participation from the poorer sections was low,⁵⁰ highlighting limited community outreach in slums and working-class settlements⁵¹. Language exacerbated the digital divide — CoWIN was initially only available in English and expanded to include 11 other languages only in June 2021⁵².
Adverse Impacts of Vaccines
In May 2024, the developers of the AstraZeneca vaccine (Covishield in India) admitted in a UK class action lawsuit on vaccine deaths that it was aware of a very rare side effect known as Thrombosis with Thrombocytopenia Syndrome (TTS). Covishield had approximately 1.8 billion doses administered globally⁵³.
While, from 2021 onwards, SII disclosed all possible side-effects, including TTS, in its package inserts and on its website, governments, including India’s, did not publicise the possible side-effects widely⁵³.
Shortly after the publicity on the adverse impacts of Covishield, a study on the long-term safety of COVAXIN on adults and adolescents was published. It concluded that nearly one-third of persons who were vaccinated with COVAXIN reported adverse events of special interest (AESI) after a one-year follow up⁵⁴. Both Bharat Biotech and ICMR, co-owners and co-inventors of Covaxin, and experts, have faulted this study, citing several reasons to treat its findings with caution⁵⁵˒⁵⁶.
During a pandemic, the advantages of vaccination outweigh possible risks, given that adverse events are rare. However, these risks must still be communicated to the public, and the government should play a proactive and transparent role in monitoring adverse impacts. India did not constitute a mechanism to monitor and address impacts of the vaccines, despite the UK and USA showing that
Given that COVAXIN had not completed its Phase III trials at the time of its approval, nor had SII completed the bridge trial for Covishield, such a mechanism should have been established as a matter of priority. The MoHFW did create a toll-free number for reporting adverse impacts, but it was not widely publicised⁵³. The failure to ensure widespread dissemination about information on vaccine side effects is an abrogation of the trust placed in the government and can affect people’s decision to vaccinate voluntarily during future epidemics.
5. Policy Recommendations
The COVID-19 pandemic highlighted critical gaps in the government’s capacity to respond to serious health crises, revealing the urgent need for comprehensive policy reforms to better manage future health emergencies. Several political, administrative, economic and structural measures must be implemented to build a more resilient health system.
At the political and institutional level, to effectively manage future pandemics, collaboration is crucial. A national-level committee which includes members from all political parties should be mandated to advise, review, and monitor pandemic management nationwide.
Investing in research and development is crucial for developing vaccines, treatments, and diagnostic tools. Stronger mechanisms are needed to ensure that expert advice is prioritised instead of political agendas taking precedence. Health emergency responses should be led by public health practitioners and involve multi-stakeholder coordination, drawing on the strengths of civil society, the private sector, healthcare institutions, and international organisations.
During the COVID-19 pandemic, civil society organisations played a vital role in reaching marginalised communities with critical information and support, such as distributing masks and sanitisers in remote areas. Leveraging each stakeholder’s unique capabilities makes pandemic response more holistic and effective, addresses the needs of all communities and strengthens resilience. Decentralising decision-making and empowering local governments by transferring funds and authority to the district level will enable efficient management of critical resources and improved delivery of essential health services.
The pandemic has also highlighted the gravity of India’s per capita public health expenditure, which is among the lowest in the world, leading to high out-of-pocket expenses that push households further into poverty when faced with a health crisis.
Increasing public health investment to 2.5% of GDP by 2025 will still fall short compared to global standards. Significant investment in healthcare infrastructure, especially in rural areas, is needed to bridge the urban-rural divide and ensure equitable access to quality healthcare.
The pandemic disproportionately affected the elderly, disabled, low-income groups, and those living in rural or underserved areas, who face significant barriers in accessing healthcare. Healthcare programmes that prioritise such vulnerable populations are needed along with mechanisms to track their health outcomes. This involves collecting disaggregated data on health indicators such as disease prevalence, vaccination rates, and mortality rates among different demographic groups. Such data would help identify gaps in healthcare provision and help target interventions more effectively and equitably.
The 2024–25 Union Budget missed a critical opportunity to strengthen India’s healthcare system, in light of lessons learned from the COVID-19 pandemic. When adjusted for inflation, funding for the health ministry, and the National Health Mission declined in real terms. This shortfall is concerning given the high expectations set during the pandemic for increased healthcare investment.
Higher investments are needed to address India’s shortfall in healthcare infrastructure and personnel. To achieve the ideal ratio of 3 hospital beds per 1,000 people, the country needs an additional 2.4 million beds⁵⁷. When it comes to medical professionals, the government claims a ratio of 1:834, but this figure is inflated by including AYUSH (non-allopathic) practitioners⁵⁸. As of March 2021, community health centres in rural India faced a significant shortfall, with nearly 80% of positions for surgeons, physicians, gynaecologists, and paediatricians remaining unfilled⁵⁸. Additionally, with only 1.96 nurses per 1,000 people, India does not meet the WHO’s guideline of 3 nurses per 1,000 people⁵⁹. With respect to infrastructure, with just 2000 accredited (regulated) laboratories, testing capabilities fall severely short for a population of 1.4 billion people⁶⁰.
Strengthening primary health centres and rural health infrastructure and building the capacity of community health workers are crucial. Additionally, emergency preparedness plans and protocols must be designed and tested for future pandemics, especially in densely populated cities, where the spread of diseases can be rapid and devastating. The lauded “Dharavi model” implemented by a bureaucrat (Iqbal Singh Chahal) helped contain the potentially devastating spread of the virus in one of the world’s largest urban slums through meticulous screening, testing and isolating measures⁶¹.
The migrant workers’ crisis revealed the necessity of adequate social safety nets to mitigate the social and economic fallout disproportionately affecting these groups. Fine tuning direct benefit transfer programmes and instituting a minimum income guarantee scheme for the poorest and most vulnerable populations, similar to the Nyuntam Aay Yojana (NYAY) proposed by the Indian National Congress party can alleviate short-term financial calamity faced by vulnerable populations⁶².
Sharing information transparently on cases, spread, trends, and trials and on deaths can instil stronger accountability and inform future strategies – this is highlighted in the disparity between India’s official death numbers and those of the WHO, as mentioned previously³. Many industries cited issues with ambiguous and infrequent updates from the government, particularly concerning support measures and regulations. Further, criticisms of vaccination strategies should not be attacked as anti-vaccination agendas.
Updated and improved Standard Operating Procedures (SOPs) for handling deceased individuals during a pandemic are needed. During COVID-19, mishandling, such as failing to properly wrap bodies or conducting open cremations near water bodies, led to further spread of the virus.
Planned lockdowns require carefully designed protocols to minimise disruption while effectively controlling disease spread. Strategic trade-offs must be considered to buffer economic losses, balancing public health needs with economic stability. Frameworks for rapid fund mobilisation towards vaccine research and development are essential, as are international collaborations, including protocols for contact tracing. Such measures could help avoid the mistakes of previous outbreaks and future epidemics.
The surge of Mpox in Africa by August 2024 prompted the Karnataka State Technical Advisory Committee to recommend sewage surveillance for early detection from airport arrival terminals, establishment of isolation facilities, training of rapid response teams, and screening of patients at airports.⁶³ Such a proactive model should become the norm in future disease control.
6. Conclusion
In conclusion, the COVID-19 pandemic was an unprecedented challenge marked by uncertainties, particularly in understanding the virus’s spread, impact, and effective containment strategies. Strategic shifts and confusion were perhaps inevitable, given the complexities of managing a health crisis of this scale. We provided a critical examination of India’s policy responses to the COVID-19 pandemic by going beyond prevalent official narratives to derive lessons that can improve future preparedness, response, and resilience. Going forward, we recommend the passage of a Public Health Act to balance the roles of the central and state governments. We recommend substantial investment in a public health cadre and in public health infrastructure to enhance India’s preparedness and ensure a more coordinated response in the face of future public health challenges.
Conflict of Interest:
None.
Funding Statement:
None.
Acknowledgements:
The authors thank Ms. K Sujatha Rao, and Dr. K Srinath Reddy for their input
References
1. World Health Organization. Covid-19 cases | WHO COVID-19 Dashboard. World Health Organization. Accessed August 31, 2024. https://data.who.int/dashboards/covid19/cases.
2. World Health Organization. Covid-19 deaths reported to WHO | WHO COVID-19 Dashboard. World Health Organization. Accessed August 31, 2024. https://data.who.int/dashboards/covid19/deaths?n=o
3. Jacob Koshy. WHO estimates 4.7 million COVID-linked deaths in India, 10 times official count. The Hindu. https://www.thehindu.com/sci-tech/health/who-estimates-47-million-covid-linked-deaths-in-india-10-times-official-count/article65385669.ece. Published May 6, 2022. Accessed August 26, 2024.
4. Priyanka Pulla. Coronavirus testing: ICMR’s strategy and diagnostic kits amidst community transmission. The Wire. https://science.thewire.in/health/coronavirus-testing-icmr-testing-strategy-covid-19-diagnostic-kits-community-transmission/. Published July 31, 2020. Accessed August 26, 2024.
5. HT Correspondents. Parliament steps up efforts, checks legislators to contain virus spread. Hindustan Times. https://www.hindustantimes.com/india-news/parliament-steps-up-efforts-checks-legislators-to-contain-virus-spread/story-ON2fj83JNIcuthMKjd4a0M.html. Published March 19, 2020. Accessed August 26, 2024.
6. ANI. COVID lockdown delayed to bring down Congress govt in MP: Jairam Ramesh. Business Standard. https://www.business-standard.com/elections/madhya-pradesh-elections/covid-lockdown-delayed-to-bring-down-congress-govt-in-mp-jairam-ramesh-123110501017_1.html. Published November 6, 2023. Accessed August 26, 2024.
7. Business Today. Warned Centre about COVID-19: China, they rubbished it, says Rahul Gandhi. Business Today. https://www.businesstoday.in/latest/economy-politics/story/warned-centre-about-covid-19-china-they-rubbished-it-says-rahul-gandhi-268113-2020-07-24. Published July 24, 2020. Accessed August 26, 2024.
8. Press Information Bureau. India’s response to COVID-19: Measures taken by the government. Press Information Bureau. https://pib.gov.in/newsite/PrintRelease.aspx?relid=200658. Published March 24, 2020. Accessed August 26, 2024.
9. India Today Bureau. India scores high on COVID-19 response tracker made by Oxford University. India Today. https://www.indiatoday.in/india/story/india-scores-high-on-covid-19-response-tracker-made-by-oxford-university-1665573-2020-04-10. Published April 10, 2020. Accessed August 26, 2024.
10. Ellis-Peterson H, Chaurasia M. India racked by greatest exodus since partition due to coronavirus. The Guardian. https://www.theguardian.com/world/2020/mar/30/india-wracked-by-greatest-exodus-since-partition-due-to-coronavirus. Published March 30, 2020. Accessed August 26, 2024.
11. Sethi, N., & Shrivastava, K. S. Govt knew lockdown would delay, not control pandemic. Article 14. https://www.article-14.com/post/govt-knew-lockdown-would-delay-not-control-pandemic. Published on April 23, 2020. Accessed August 28, 2024,
12. Raj Y. Timely lockdown helped India fight COVID-19, PM Modi tells Indian-descent US doctors. Hindustan Times. https://www.hindustantimes.com/india-news/timely-lockdown-helped-india-fight-covid-19-pm-modi-tells-indian-descent-us-doctors/story-kppk81Lj2L27kYyPAD3UsL.html. Published June 28, 2020. Accessed August 26, 2024.
13. High Commission of India, Brunei Darussalam. COVID-19 update: Information on preventive measures and protocols. High Commission of India, Brunei Darussalam. https://www.hcindiabrunei.gov.in/docs/16040525671.pdf. Published October 29, 2020. Accessed August 26, 2024.
14. Radhakrishnan, V. Data | How effective was India’s COVID-19 lockdown compared to other countries?. The Hindu. https://www.thehindu.com/data/data-how-effective-was-indias-covid-19-lockdown-compared-to-other-countries/article31785553.ece Published June 10, 2020. Accessed September 28, 2024.
15. Gupta N., Bhatnagar T, et al. Strategic planning to augment the testing capacity for COVID-19. Indian Journal of Medical Research. https://journals.lww.com/ijmr/fulltext/2020/51020/strategic_planning_to_augment_the_testing_capacity.17.aspx. Published March 2020. Accessed August 26, 2024.
16. Yadav P., Mehndiratta A., et al. India’s COVID-19 testing capacity must grow by a factor of 10: Here’s how it can happen. Center for Global Development. https://www.cgdev.org/publication/indias-covid-19-testing-capacity-must-grow-factor-10-heres-how-can-happen. Published June 4, 2020. Accessed August 26, 2024.
17. New Indian Express. Centre lifts curbs on export of masks, PPE coveralls. New Indian Express. https://www.newindianexpress.com/business/2020/Aug/26/centre-lifts-curbs-on-export-of-masks-ppe-coveralls-2188372.html. Published August 26, 2020. Accessed August 26, 2024.
18. Joel P. Joseph. India’s COVID-19 response: Online survey reveals PPE availability, training, and containment zones. The Wire. https://science.thewire.in/health/india-covid-19-online-survey-ppe-availability-training-containment-zones/. Published August 11, 2020. Accessed August 26, 2024.
19. Al Jazeera. India crosses grim landmark of 8 million coronavirus cases. Al Jazeera. https://www.aljazeera.com/news/2020/10/29/india-crosses-grim-landmark-of-8-million-coronavirus-cases. Published October 29, 2020. Accessed August 26, 2024.
20. Indian National Congress. White paper on the management of COVID-19 by the Government of India. INC.in. Published June 22, 2021. Retrieved August 30, 2024, https://inc.in/media/press-releases/white-paper-on-the-management-of-covid-19-by-the-goi
21. Indian Public Health Association, Indian Association of Preventive and Social Medicine & Indian Association of Epidemiologists. Full text: Draconian lockdown, incoherent strategies led to India paying a heavy price, say experts. Scroll.in. https://scroll.in/article/963384/full-text-draconian-lockdown-incoherent-strategies-led-to-india-paying-a-heavy-price-say-experts. Published May 31, 2020. Accessed August 26, 2024.
22. Rawat S. 9.1 million thronged Mahakumbh despite Covid-19 surge: Govt data. Hindustan Times. https://www.hindustantimes.com/cities/dehradun-news/91-million-thronged-mahakumbh-despite-covid-19-surge-govt-data-101619729096750.html. Published online April 30, 2021
23. Yengkhom S. West Bengal: Covid daily case count rises 21 times from poll start to now. Times of India. https://timesofindia.indiatimes.com/city/kolkata/covid-daily-case-count-rises-21-times-from-poll-start-to-now/articleshow/82333510.cms. Published May 1, 2021.
24. Special Correspondent. Coronavirus | India becomes first country in the world to report over 4 lakh new cases in a single day on April 30, 2021. The Hindu. https://www.thehindu.com/news/national/coronavirus-india-becomes-first-country-in-the-world-to-report-over-400000-new-cases-on-april-30-2021/article61817889.ece. Published April 30, 2021.
25. Dhingra S, Ghatak M. (2022). India: the economic impact of Covid-19. CentrePiece – The magazine for economic performance, 619. https://cep.lse.ac.uk/_new/publications/abstract.asp?index=9101. Published February 22, 2022. Accessed on August 26, 2024
26. The Times of India. Government’s economic package only 1% of GDP, say analysts The Times of India https://timesofindia.indiatimes.com/business/india-business/govts-eco-package-only-1-of-gdp-say-analysts/articleshow/75837840.cms. Published on May 20, 2020. Accessed on August 31, 2024
27. Press Trust of India. Cabinet approves “India COVID 19 Emergency Response and Health Systems Preparedness Package: Phase II.” at a cost of Rs 23,123 crore. Press Information Bureau.https://www.pib.gov.in/PressReleasePage.aspx?PRID=1733841#:~:text=%22India%20COVID%2D19%20Emergency%20Response,the%20ECRP%2DII%20%E2%80%93Rs. Published July 8, 2021. Accessed August 26, 2024.
28. The Times of India. Covid-19: India records highest-ever 4,01,993 new cases, 3,523 deaths. The Times of India. https://timesofindia.indiatimes.com/india/covid-19-india-records-highest-ever-401993-new-cases-3523-deaths/articleshow/82339160.cms Published May 1, 2021. Accessed August 29, 2024
29. Jha P, Deshmukh Y, Tumbe C, et al. COVID mortality in India: National survey data and health facility deaths. Science. 2022;375(6581):667-671. doi:10.1126/science.abm5154.
30. Biswas S. Why India’s real COVID toll may never be known. BBC News. https://www.bbc.com/news/world-asia-india-60981318. Published May 5, 2022.
31. Rajan R, Sharma A, Verma M. Characterization of the Second Wave of COVID-19 in India. medRxiv. Preprint. Published online April 21, 2021. doi.org/10.1101/2021.04.17.21255665
32. Wouters OJ, Shadlen KC, Salcher-Konrad M, et al. Challenges in ensuring global access to COVID-19 vaccines: Production, affordability, allocation, and deployment. The Lancet. 2021;397(10278):1023-1034. doi:10.1016/s0140-6736(21)00306-8
33. Department-Related Parliamentary Standing Committee on Health and Family Welfare. One Hundred Twenty Third Report on The Outbreak of Pandemic COVID-19 and its Management. Parliament of India. Published November 2020. Accessed August 24, 2024. https://sansad.in/getFile/rsnew/Committee_site/Committee_File/ReportFile/14/142/123_2021_2_13.pdf?source=rajyasabha
34. BusinessToday.In. “Serum won’t have to take full loss” if Covid vaccine not approved: Bill Gates on sharing risk. Business Today. https://www.businesstoday.in/current/world/serum-wont-have-to-take-full-loss-bill-gates-says-his-foundation-shares-financial-risk-for-vaccine/story/425802.html. Published December 25, 2020. Accessed August 24, 2024.
35. Madur GS. How India landed in Covid vaccine mess. Telegraph India. https://www.telegraphindia.com/india/how-we-landed-in-covid-vaccine-mess/cid/1812969. Published April 19, 2021. Accessed August 24, 2024.
36. Ray K. Now, smart Covid-19 vaccination strategy to check spread. Deccan Herald. https://www.deccanherald.com/india/now-smart-covid-19-vaccination-strategy-to-check-spread-922636.html. Published December 3, 2020. Accessed August 24, 2024.
37. Special Correspondent. Coronavirus | India approves COVID-19 vaccines Covishield and Covaxin for emergency use. The Hindu. https://www.thehindu.com/news/national/drug-controller-general-approves-covishield-and-covaxin-in-india-for-emergency-use/article33485539.ece. Published January 3, 2021. Accessed August 31, 2024.
38. Press Trust of India. “Determined to support India in COVID fight, ensure supply of vaccine raw materials”: Biden to Modi. The New Indian Express. https://www.newindianexpress.com/nation/2021/apr/26/determined-to-support-india-in-covid-fight-ensure-supply-of-vaccine-raw-materials-biden-to-modi-2295174.html. Published April 27, 2021. Accessed August 24, 2024.
39. Press Trust of India. Parliamentary panel had asked govt in March to ramp up vaccine production capacity. The Economic Times. https://economictimes.indiatimes.com/news/india/parliamentary-panel-had-asked-govt-in-march-to-ramp-up-vaccine-production-capacity/articleshow/82574740.cms?from=mdr. Published May 12, 2021. Accessed August 24, 2021
40. Department-Related Parliamentary Standing Committee on Science and Technology, Environment, Forests and Climate Change. One Hundred Forty Second Report on Demands for Grants (2021-2022) of the Department of Biotechnology. Parliament of India. Published March 2021. Accessed August 24, 2024. https://sansad.in/getFile/rsnew/Committee_site/Committee_File/ReportFile/19/147/342_2021_7_12.pdf?source=rajyasabha
41. Singh, K., Verma, A., & Lakshminarayan, M. (2022). India’s efforts to achieve 1.5 billion COVID-19 vaccinations: A narrative review. Osong Public Health and Research Perspectives, 13(5), 316. https://doi.org/10.24171/j.phrp.2022.0104
42. Ramakumar R. State governments can purchase only 25% of vaccines – belying Centre’s claim of equitable policy. Scroll. https://scroll.in/article/994606/state-governments-can-purchase-only-25-of-vaccines-belying-centres-claim-of-equitable-policy. Published May 11, 2021. Accessed August 24, 2024.
43. Ramakumar R. As Govt Vastly Downscales Availability, India’s Vaccine Prospects Continue to Look Bleak. The Wire. https://thewire.in/government/india-covid-19-vaccines-supply-covishield-covaxin-sputnik. Published July 4, 2021. Accessed August 24, 2024.
44. Press Trust of India. Days before PM’s announcement for free COVID jabs to 18+, SC asked for review of vaccination policy. The Economic Times. https://economictimes.indiatimes.com/news/india/days-before-pms-announcement-for-free-covid-jabs-to-18-sc-asked-for-review-of-vaccination-policy/articleshow/83311679.cms. Published June 7, 2021. Accessed August 24, 2024.
45. Perappadan BS. Coronavirus | Sputnik V to be available in Indian markets by next week. The Hindu. https://www.thehindu.com/news/national/coronavirus-sputnik-v-to-be-available-in-indian-markets-by-next-week/article34550845.ece. Published May 14, 2021. Accessed August 24, 2024.
46. Bhalla V. Centre’s affidavits in SC exposes its hollow claims of both Covid vaccine availability and spending on its research and development. The Leaflet. https://theleaflet.in/centres-affidavits-in-sc-exposes-its-hollow-claims-of-both-covid-vaccine-availability-and-spending-on-its-research-and-development/. Published July 18, 2021. Accessed August 24, 2024.
47. Sharma NC. Covid-19 vaccine wastage as high as 37% in some states: Centre. Mint. https://www.livemint.com/news/india/covid19-vaccine-wastage-as-high-as-37-in-some-states-centre-11621956664973.html. Published May 25, 2021. Accessed August 24, 2024.
48. Special Correspondent. Estimate of 216 crore vaccine doses was aspirational, says V.K. Paul. The Hindu https://www.thehindu.com/news/national/estimate-of-216-crore-vaccine-doses-in-august-december-was-aspirational-says-vk-paul/article61447055.ece. Published November 26, 2021. Accessed August 24, 2021.
49. Radhakrishnan V. Vaccination in rural India trails urban areas even as cases surge. The Hindu. https://www.thehindu.com/news/national/vaccination-in-rural-india-trails-urban-areas-even-as-cases-surge/article34589734.ece. Published May 19, 2021. Accessed August 25, 2024
50. Rao SR. Elders from poorer sections yet to join vaccination drive in Bengaluru. The Times of India. https://timesofindia.indiatimes.com/city/bengaluru/elders-from-poorer-sections-yet-to-join-vaccination-drive-in-bengaluru/articleshow/81387920.cms. Published March 8, 2021. Accessed August 24, 2024.
51. Iyer M. Mumbai: Poor not among vaccine-seekers, awareness need of hour. The Times of India. https://timesofindia.indiatimes.com/city/mumbai/mumbai-poor-not-among-vaccine-seekers-awareness-need-of-hour/articleshow/81319222.cms Published March 4, 2021. Accessed August 24, 2024.
52. News18.com. CoWIN portal is now available in Hindi, 10 regional languages including Punjabi, Telugu. News18. https://www.news18.com/news/india/cowin-portal-is-now-available-in-hindi-10-regional-languages-including-punjabi-telugu-3808481.html Published June 4, 2021. Accessed August 24, 2024.
53. Kaur B. Report on rare adverse side effects of Covishield causes panic. But should it? The Wire. https://thewire.in/health/report-on-rare-adverse-side-effects-of-covishield-causes-panic-but-should-it. Published May 1, 2024. Accessed August 24, 2024.
54. Kaur U, Jaiswal A, Jaiswal A, et al. Long-term safety analysis of the BBV152 coronavirus vaccine in adolescents and adults: Findings from a 1-year prospective study in North India. Drug Safety. Published online May 13, 2024. doi:10.1007/s402 64-024-01432-6
55. Kumar P. Top medical body slams study on Covaxin safety, side-effects, wants apology. NDTV. https://www.ndtv.com/india-news/covaxin-safety-benares-hindu-university-icmr-top-medical-body-slams-study-on-covaxin-safety-side-effects-wants-apology-5704823. Published May 20, 2024. Accessed August 24, 2024.
56. Kaur. B. BHU’s Covaxin safety study: Cautious interpretation of results needed. The Wire. https://thewire.in/health/bhu-covaxin-study-cautious-interpretation Published May 18, 2024. Accessed August 24, 2024.
57. The Economic Times. India needs additional 2.4 million hospital beds to reach recommended ratio: Report. The Economic Times. https://economictimes.indiatimes.com/news/india/india-needs-additional-2-4-million-hospital-beds-to-reach-recommended-ratio-report/articleshow/105450555.cms?from=mdr. Published September 19, 2023. Accessed August 26, 2024.
58. Divyani Dubey. Has India really achieved WHO-recommended doctor-population ratio? FactChecker. https://www.factchecker.in/context-check/has-india-really-achieved-who-recommended-doctor-population-ratio-829064#google_vignette. Published April 17, 2023. Accessed August 26, 2024.
59. Press Trust of India. Shortage of nurses in India, their emigration for jobs abroad cause of worry: Experts. Hindustan Times. https://www.hindustantimes.com/india-news/shortage-of-nurses-in-india-their-emigration-for-jobs-abroad-cause-of-worry-experts-101716385215844.html. Published April 3, 2023. Accessed August 26, 2024.
60. Bhuyan A. Labs that test for COVID-19 aren’t all accredited. The Wire Science. https://science.thewire.in/health/nabl-covid-19-labs-testing-accreditation-quality-control/. Published June 15, 2020. Accessed August 27, 2024.
61. Banjot Kaur. At the heart of Dharavi model: Basic public health, resolve in community to beat COVID-19. Down To Earth. https://www.downtoearth.org.in/health/at-the-heart-of-dharavi-model-basic-public-health-resolve-in-community-to-beat-covid-19-72771. Published August 11, 2020. Accessed August 26, 2024.
62. Bhalchandra Mungekar. The NYAY scheme is a game changer. The Hindu Business Line. https://www.thehindubusinessline.com/opinion/the-nyay-scheme-is-a-game-changer/article26822386.ece. Published April 13, 2019. Accessed August 26, 2024.
63. Yasmeen A. Technical Advisory Committee recommends sewage surveillance for early detection of Mpox in Karnataka. The Hindu. https://www.thehindu.com/news/cities/bangalore/technical-advisory-committee-recommends-sewage-surveillance-for-early-detection-of-monkeypox-in-karnataka/article68559434.ece. Published August 26, 2024. Accessed August 27, 2024.