

Lived Experience of Protection in Early COVID-19 Pandemic
The Lived Experience of Protection During the Early Days of the COVID-19 Pandemic
Florence M. Weierbach, PhD, MPH, RN 1; Jean Croce Hemphill, PhD, MSN, FNP-BC 1; Katherine C. Hall, PhD, RN-BC, CNE 1; Holly Berry-Price, PhD, FNP-BC 2
- College of Nursing, East Tennessee State University, Johnson City, TN 37614
- Blue Sky MD Health 317 N. King Street Hendersonville, NC 28792
OPEN ACCESS
PUBLISHED: 30 November 2024
CITATION: Weierbach, FM., Hemphill, JC., et al., 2024. The Lived Experience of Protection During the Early Days of the COVID-19 Pandemic. Medical Research Archives, [online] 12(11). https://doi.org/10.18103/mra.v12i11.6080
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v12i11.6080
ISSN 2375-1924
ABSTRACT
The COVID-19 pandemic, declared by the World Health Organization in March 2020, brought unprecedented challenges to public health communication, adherence to guidelines, and personal protection practices. This study explored the lived experience of protection during the pandemic’s early stages, before vaccines or antiviral treatments were available, to understand factors influencing individual protective behaviors. Using existential phenomenology, the research focused on “environment” as a key element, examining how participants experienced protection within their unique contexts. A sample of 37 U.S. adults was recruited through social media from May to June 2020, and 12 completed virtual, unstructured interviews. Guided by an initial question — “When you think about protection during this time, what comes to mind?”— participants shared narratives of their protective practices. Data analysis, beginning with the first interview and continuing iteratively, involved identifying and grouping meaning units into themes. Two primary themes emerged: Communication and Actions. The Communication theme included subthemes of “Science Literacy and Mixed Messaging,” as participants expressed challenges in discerning credible information and frustrations with inconsistent public health messaging. The Actions theme comprised “Connections and Routines,” highlighting how participants adapted daily routines to protect themselves while managing disruptions in social interactions and maintaining personal connections. Findings revealed that protection during the pandemic was influenced by the interplay between communication and actions, shaped by perceptions of scientific information and the need for social connections within modified routines. This study underscores the need for clear, consistent, and contextually relevant communication strategies in public health crises, highlighting that factors such as science literacy, social connectivity, and routine adjustments play a critical role in shaping protective behaviors. Future research should continue to explore the role of effective communication and social support in encouraging protective behaviors, providing insights to improve public health messaging and resilience in future health crises.
Keywords
protection, phenomenology, COVID-19
Introduction
The novel coronavirus, COVID-19, was declared a pandemic by the World Health Organization (WHO) on March 11, 2020. At that time, there was no known preventive method, effective treatment, or cure. The US declared a national emergency on March 13, 2020, resulting in a nationwide shutdown and closed borders. In the early days, public health messages in the USA focused on large-scale mortality and ways to mitigate the spread of the virus. The message from healthcare professionals was on physical protective measures as people were asked to stay home, wear masks, and practice social distancing to prevent the virus’s spread. However, inconsistent messaging was rampant. Adherence to the CDC recommendations varied, COVID-19 continued to spread, and by June 1, 2020, fatalities in the USA attributed to the disease exceeded twenty-three thousand. The lack of adherence to physical protective recommendations was surprising for many, as the concept of protection is inherent in healthcare. The definition of protection includes processes that occur on behalf of an individual or group, mitigation of actual and potential threats, and the provision of protective physical measures, information, and education. The researchers, who are nurses, were driven to explore the wide range of adherence to public health information and recommendations, seeking to understand the underlying factors in people’s lives that prompted such varied responses.
The Situational Model of Nurse Protection provides a broad framework outlining the importance of nurses in supporting the protection of others based on the assessment of actual and perceived threats. There are three phases of the framework: pre-protective, protective, and post-protective. In each phase, specific interventions can be implemented to maintain physiological and psychological homeostasis when facing threats. The model emphasizes the importance of the environment on the vulnerability of persons, indicating that the environment itself can pose a risk to homeostasis and can include the global community. While the model is tailored to nursing, its scope is sufficiently comprehensive to be applicable across various disciplines and settings. Through this model, one might assume that the public would widely accept and adopt protective measures against COVID-19, achieving physiological and psychological homeostasis. However, the public’s lack of adherence and willingness to accept information about COVID-19 underscored the need to closely examine protection within the context of the lived experience of pandemic response to uncover additional factors influencing behavioral responses during global crises. Furthermore, identifying these additional factors can provide nurses and public health workers with crucial information to shape future guidance. This study therefore aimed to explore the lived experience of protection during the early days of the COVID-19 pandemic.
Methods
The study was informed by existential phenomenology with the environment as a core concept. The environmental context brings the understanding of place which is where nursing care occurs. The phenomenological framework provided understanding of the person’s experience of protection during the pandemic in their day-to-day lives. The intentionality of the protection experience was described in the context of the invisible health threat. After institutional human subject/ethics approval was obtained, recruitment was initiated through the researchers’ Facebook pages and Twitter accounts. Inclusion criteria included English speaking adults age 18 years and older who were willing to talk about the experience and who lived in the United States, US territories or military bases. Participants self-selected, accessed the informed consent document, and a short demographic and screening questionnaire through a secure link to the Research Electronic Data Capture server (REDCap) available through the researchers’ institutional email accounts and distributed through the researchers’ Facebook pages and Twitter accounts. Individuals who did not meet inclusion criteria were not able to access the informed consent and were thus not included. From May to June 2020, thirty-seven adults over age 18 were recruited and met inclusion criteria. Once participants provided their contact information within the secure research site, one of the researchers contacted the participant and scheduled an interview via secure Zoom. Twelve of the thirty-seven adults met criteria and completed interviews. The remaining 25 adults who met criteria either did not complete the REDCap survey, were not available, did not have the technology to participate, or chose not to be interviewed.
Research protocols were in place to assure scientific rigor to address researcher bias, maintain data integrity and assure results represented the voice of the participants. Prior to participant interviews for data collection, the researchers participated in bracketing interviews. During bracketing interviews, one member of the research team interviews another member of the research team using the same process guided by the same opening interview question. Bracketing allows researchers to elucidate biases they may have regarding the phenomena under investigation with the intent of suspending them during participant interviews and subsequent data analysis. These confidential interviews were audio or video recorded and lasted approximately one hour. Recordings were then transcribed verbatim by a member of the research team and reviewed by the researcher who conducted the interview. During the reading of the researchers’ bracketing interviews, multiple biases were identified, ranging from lack of understanding for not adhering to public health guidelines to disillusionment with political messaging. Results from bracketing interviews were noted and revisited as needed during the analytic process.
In keeping with phenomenological research, an unstructured interview process was used. The phenomenological dialogue (i.e., the interview) started with the unstructured question, “When you think about protection during this time, what comes to mind?” and, if needed, a clarifying follow up question, “Tell me about how you protect yourself during the COVID-19 pandemic.” Subsequent questions were guided by participants’ stories as they shared their lived experiences. As interviews unfolded, fieldnotes were maintained by the researcher, and included information such as details regarding the virtual environment, participant-researcher interactions, participant overall appearance, and demeanor. Interviews were recorded and transcribed verbatim by a member of the research team.
Data analysis began after completion of the first interview, and participant interviews were conducted until data saturation was determined by the research team. Saturation occurs when nothing new emerges in subsequent interviews. The research team adhered to an iterative analytic process for phenomenology. During the weekly research team meetings, members read each transcript in its entirety. Participant words and phrases were identified that captured the essence of the lived experience of protection. These words and phrases were then grouped together and, through the iterative process of identifying, separating, isolating and grouping, themes and sub-themes were elucidated. As themes and subthemes were identified, results were presented and discussed with the College of Nursing qualitative research group, an experienced group of qualitative researchers. This process was also iterative in nature, as the research team moved back and forth between transcripts, words, and phrases to verify thematic analysis. Rigor was maintained throughout the analysis. Data, including transcripts, research journal, and field notes, were maintained through storage in a secure password university protected internet cloud. The research team adhered to principles of trustworthiness. Credibility was established through bracketing interviews, faithful interpretation of participants’ words, qualitative research group discussion and consensus, purposeful sampling, and data saturation. A research journal was used to record decisions throughout data collection and analysis. An audit trail was also created and maintained. The audit trail included a timeline to capture dates of initial analysis for each transcript, and notes on subsequent discussion and decisions regarding text as related to identification of meaning units and themes. The audit trail was included as part of the research journal. Transferability was established by including participants from across the US and through the researchers’ analysis of participants’ words and stories across their varied settings. Confirmability was established with the bracketing interview, completed before starting the interviews, and during hermeneutic analysis by the research team and consultation with the College of Nursing qualitative research group.
Results
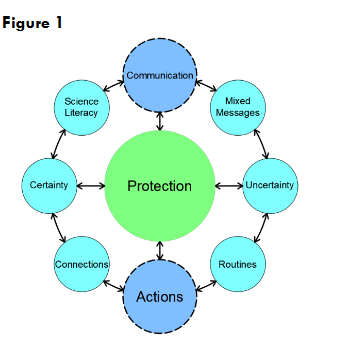
Results suggest protection is contextually structured into two global, yet inextricably linked, themes: Communication and Actions. Communication encompasses individuals’ understanding of scientific terminology and how they interpret messages from multiple sources including scientists, health care professionals, news media, social media, family and friends. Actions focus on behaviors individuals adopt in response to the pandemic, emphasizing an interplay between daily routines, personal connections, and communications. The two global themes present in Figure 1 are further organized into a structure of interrelated reciprocal subthemes. Each subtheme is connected to the concept of protection through the global themes of communication and actions.
THEME: COMMUNICATION
Subtheme: Science Literacy & Mixed Messaging
The subtheme Science Literacy and Mixed Messages are intertwined with participants expressing challenges in discerning credible information and reporting confusion due to inconsistent messaging. Concerns around scientific literacy were identified in statements such as “I think some people kind of had this misconception that, oh healthcare is great in America, it’s not going to come here and so maybe that false perception is gone” and “…half of them think it’s all been cooked up…. I don’t want to be part of that mentality. I don’t feel safe”. Participants often followed issues related to science literacy with statements about mixed messaging. For example, one participant said “I find it concerning when you get mixed messages….” While another participant shared “… even though they said to shut the office down. They didn’t lock the doors. Basically, there was no signage”.
Subtheme: Uncertainty
Many participants expressed feelings of uncertainty regarding protection. Several participants reported that these feelings were a result of the mixed messaging from communications they received. For example, uncertainty was revealed as a standalone concept in statements such as “the media and the news is [sic] telling that, that we’ve got problems. So, you know, the news media is, is…they’re either correct, or they’re not correct…I don’t have a clue.” Others expressed similar thoughts with statements such as “what is going on in the grocery store? Is it a panic? …What am I walking into?” and “I don’t know if wearing a mask is important. I mean, I, I’ve read things and it seems like it is. But I don’t know, I don’t know exactly what, what we should all be doing.” However, the simultaneous expression of certainty and uncertainty was also evident in statements such as “You hear about this in other countries, but I guess you hear about this, and I’m amazed that we are more vulnerable than we thought we were.”
THEME: ACTIONS
Subtheme: Connections and Routines
In the subtheme Connections and Routines, participants described how routines, and changes in them, affected their ability to connect with others. Within those connections, participants reported how important maintaining or establishing new routines were to support their protection. Routines, and subsequent impact of changes to routines, were often described in the context of work or tasks that needed to be done. For example, one participant said, “there were so many things that had to happen…We don’t care what management says, this has to get done and we did it” while another participant shared “It took me a while but I got into like a routine. I’d do the same things every day. It was everything is on the list, that I made sure I did and I take them off.” Others were focused on the day-to-day routine tasks that were impacted due to the need to protect themselves. For example, participants shared comments such as “I’m retired, so, so my rules of engagement are a little different. I don’t have to go to work, I don’t have to get on the train and commute, I don’t have to, ah, take a taxi. I don’t have to take a bus, and I’m sure if I was, if I was, ah, in a position of having to do that, I would be thinking a little differently”; “we do grocery pick-up and…we shop online”; and “We have had to have the cable people in the house…and they were mostly outside.”
Outside of mundane daily tasks or work-related routines, participants described how their routines were laced with ties to human connection and how important that was for them. For example, one participant was bothered by how the change in routine impacted her ability to engage in human contact by sharing “I do not think I have touched another human being, since…since we went into pandemic mode…and I, and that’s bothersome to me” and another said “I do work with probably a high-risk population…. I feel less safe at church than I do at work.” The need to self-protect also gave some the opportunity to reflect on how the alteration in routine impacted their human connections. One participant expressed “the ability to actually slow down and not have to do all the things and not feel obligated … I’m like, well, I hate we had to have a global pandemic to experience this, but it’s not. It’s… it’s been kind of relaxed and it’s been kind of nice actually.” Still another described how the change in the pace of daily routine provided space for reflection about life’s connections: “I just tried to stay connected, not isolate, uh, not…my pace slowed down… I’ve been asking “what is, what am I really rushin’ [sic]?”
Discussion
The lived experience of protection in this study was described by participants as one that is grounded by communications and actions which are linked together and influenced by messaging especially related to science literacy, feelings of uncertainty, personal routines, and the power of human connections. Taken with the wide variability among participants’ lived experiences, these interwoven themes and sub-themes suggest that interventions designed to address protective factors may need to be viewed through a lens with increased consideration on context. Protection is a complex concept that includes action involving processes for intervention and outcomes based on goals. This study, conducted prior to the introduction of the COVID-19 vaccine, reveals that poorly communicated interventions, goals, and outcomes impact perceptions of the need to engage in protective actions. Participants reported consistent mixed messages from leaders, including those in governmental healthcare. Compounded by uncertainty and, in some cases, limited scientific literacy, participants were clearly confused about what protective measures they needed to take. The relationship between trust from the American public and health communication manifested in COVID-19 vaccine hesitancy. Additionally, vaccine uptake or hesitancy behaviors associated with COVID-19 were present across populations with differences identified in trusting health care officials’ messaging, health literacy levels, and political affiliations.
The uncertainty reported by participants was abundantly clear. Participants were not able to discern valid media information from invalid media information, leading them to second-guess scientific information and question protective measures. Media literacy underscores the ability to discern information that is available, however it is suggested that science literacy is foundational for understanding. Populations impacted by low educational attainment and access to health care tend to have lower health literacy which requires different messaging from health care officials. Additionally, protective behaviors are mixed due to inability to discern misinformation from the media, family, friends and community members. In contrast, the results of this study challenge the limitations of health and science literacy only in terms of educational levels. The juxtaposition of the subthemes of science literacy and mixed messages demonstrated that in the midst of overwhelming fear of the unknown and uncertainty people processed information using their perceptions rather than through critical thinking. However, uncertainty present in protective behaviors also manifested through actions aimed to adhere to recommendations from the CDC. Clear messaging is paramount for combatting vaccine misinformation and uptake in preventing the spread of COVID-19. Whitehead et al. identified nine effective communication strategies aimed at interventions to counter vaccine misinformation with emphasis placed on the content of the intervention or message. Further, the importance of uncertainty is also elucidated by Whitehead et al. who reported that messages delivered with certainty were less impactful than messaging that acknowledged uncertainty.
Finally, the focus on connections and routines was threaded throughout participant stories. Personal connections were deeply rooted in participants’ communities and included family, friends, colleagues, and others. New routines were established to support personal connections and to engage in protective behaviors. As participants engaged in new routines, they created new meaning about the connections that were important in their lives. Many of the participants described how connections impacted their perceptions of the information they were receiving, which subsequently affected their protective health behaviors. From a community health perspective, the connections between health care officials and communities make community health care workers a valuable asset in the provision of accurate information addressing the spread and prevention of COVID-19. Oliver et al. assert that these connections encourage trust and allow health care information to be presented to individuals and groups through means that are acceptable to the individual communities. The results from this study support current literature regarding the importance of acknowledging uncertainty as a contributing factor to engaging in protective health behaviors, but also open the door for consideration of other factors that may impact individual health behaviors such as connections that extend beyond personal or social ones. This may include targeted interventions and messaging provided specifically by community health workers. Therefore, ensuring a robust public and community health system is integral to instituting and supporting actions that aim to support protective health behaviors for the next public health crisis.
Limitations
Study limitations are present and center on two areas, use of technology and time. Technology limitations include the use of social media, virtual platforms for interviews and technology access. Study recruitment occurred through social media which did not allow those without internet access the opportunity for participation. This may have impacted inclusion of vulnerable populations due to technology access. Additionally, social media has the potential to reach people in geographic areas beyond where researchers live; however, participant location was not included on the demographic survey. Since the researchers were in two states in the southeastern United States, there was an assumption that geographic diversity was limited.
An additional limitation associated with technology was the use of a virtual platform for interviews. Virtual platforms for a phenomenological study can provide challenges associated with researcher participant engagement. Technology access limitations included unstable internet connections during interviews that interrupted participants and researchers’ communication flow, and participant discomfort using the camera feature of the virtual platform. Cameras were tuned off for participants who requested them to be off. Both the unstable internet connections and inconsistent use of the camera limited the researchers’ abilities to assess participant body language. A separate limitation addresses the inability to capture the phenomenon of protection after vaccine availability as all participants were recruited and interviewed in a 4-week time period from Mid-May to Mid-June 2020.
Conclusion
In conclusion, this study revealed that protection is context based and that, for some, in times of crises protective factors may be lost due to uncertainty, changes in routines, mixed messaging, and one’s ability to engage in meaningful human connections. In reflecting on the public’s response to adherence to COVID-19 prevention messaging from public health officials, results reinforce the importance of providing information that individuals can relate to. Nurses address the holistic human condition and as members of the comprehensive health care team should be included in designing, implementing and evaluating community health interventions. Future research should continue to examine who delivers, how information is delivered and the impact of the message in addressing protective health-related behaviors. Additionally, researchers should explore the power of human connections other than personal and social ones on protective health behaviors for individuals, groups, and broader communities.
Conflicts of Interest: The authors have no conflicts of interest to disclose.
Funding: There was no funding for this research.
Acknowledgements: The authors have no acknowledgements.
References
- A timeline of WHO’s COVID-19 Response in the WHO European Region: a living document (version 3.0, from 31 December 2019 to 31 December 2021). Published February 14, 2022. Accessed October 10, 2024. https://www.who.int/europe/publications/i/item/WHO-EURO-2022-1772-41523-63024
- CDC. COVID-19 Timeline. Centers for Disease Control and Prevention. Published March 15, 2023. Accessed November 7, 2024. https://www.cdc.gov/museum/timeline/covid19.html
- Haffajee RL, Mello MM. Thinking Globally, Acting Locally — The U.S. Response to Covid-19. N Eng J Med. 2020;382(22). doi:10.1056/nejmp2006740
- AJMC. A Timeline of COVID-19 Developments in 2020. AJMC. Updated January 1, 2021. Accessed October 10, 2024. https://www.ajmc.com/view/a-timeline-of-covid19-developments-in-2020
- World Health Organization. COVID-19 deaths | WHO COVID-19 dashboard. Published 2024. Accessed October 10, 2024. https://data.who.int/dashboards/covid19/deaths
- Shearer JE. The Concept of Protection: A Dimensional Analysis and Critique of a Theory of Protection. Adv Nurs Sci. 2002;25(1):65-78. doi:/10.1097/00012272-200209000-00008
- Lorenz SG. Protection: Clarifying the Concept for Use in Nursing Practice. Hol Nurs Prac. 2007; 115-123.
- Fawcett J. Editorial: But is It Nursing Research? West J Nurs Res. 2000;22(5):524-525. doi:/10.1177/01939450022044575
- Husserl E, Farin I, Hart JG. The Basic Problems of Phenomenology: From the Lectures, Winter Semester, 1910-1911. Springer; 2006.
- Pollio HR, Henley TB, Thompson CJ. The Phenomenology of Everyday Life. Cambridge University Press; 1997.
- Thomas SP, Pollio HR. Listening to Patients. Springer Publishing Company; 2002.
- O’Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for Reporting Qualitative Research. Acad Med. 2014;89(9):1245-1251. doi:/10.1097/acm.0000000000000388
- Gentles, S. J., Charles, C., Ploeg, J., McKibbon, KA. Sampling in qualitative research: insights from an overview of the methods literature. The Qualitative Report, 2015: Volume 20,11(4) 1772-1789.
- Lincoln YS, Guba, EG. Criteria for assessing naturalistic inquiries as reports. Paper presented at the Annual Meeting of American Educational Research Association, 1988.
- Lincoln YS, Guba EG. Naturalistic Inquiry. Sage Publications; 1985.
- Sandelowski M. The problem of rigor in qualitative research. Adv Nurs Sci. 1986;8(3):27-37. doi:/10.1097/00012272-198604000-00005
- Elo S, Kääriäinen M, Kanste O, Pölkki T, Utriainen K, Kyngäs H. Qualitative Content analysis: a Focus on Trustworthiness. SAGE Open. 2014;4(1):1-10. doi:/10.1177/2158244014522633
- Weerakoon SM, Henson-Garcia M, Valerio-Shewmaker MA, Messiah SE, Knell G. Contributions of Trustworthiness, Health Literacy, and Self-Efficacy in Communicating With COVID-19 Vaccine–Hesitant Audiences: Web-Based Survey Study. JMIR Form Res. 2022;6(8):e38076. doi:/10.2196/38076
- Cameron LD, Lawler S, Robbins-Hill A, Toor I, Brown PM. Political views, health literacy, and COVID-19 beliefs and behaviors: A moderated mediation model. Soc Sci & Med. 2023; 320:115672. doi:/10.1016/j.socscimed.2023.115672
- Austin EW, Austin BW, Willoughby JF, Amram O, Domgaard S. How Media Literacy and Science Media Literacy Predicted the Adoption of Protective Behaviors Amidst the COVID-19 Pandemic. Journ Health Comm. 2021;26(4):1-14. doi:/10.1080/10810730.2021.1899345
- Arigbede OM, Aladeniyi OB, Buxbaum SG, Arigbede OJ. The Use of Five Public Health Themes in Understanding the Roles of Misinformation and Education Toward Disparities in Racial and Ethnic Distribution of COVID-19. Cureus. Published online October 6, 2022. doi:/10.7759/cureus.30008
- Whitehead HS, French CE, Caldwell DM, Letley L, Mounier-Jack S. A systematic review of communication interventions for countering vaccine misinformation. Vaccine. 2023;41(5). doi:/10.1016/j.vaccine.2022.12.059
- Oliver J, Ferdinand A, Kaufman J, Allard N, Danchin M, Gibney KB. Community health workers’ dissemination of COVID-19 information and services in the early pandemic response: a systematic review. BMC Health Serv Res. 2024;24(1). doi:/10.1186/s12913-024-11165-y
- Widiasih R, Pramukti I, Sithichoksakulchai S. Editorial: Embracing a Holistic Approach for Sustainable Healthcare Collaboration. Journ Hol Nurs. Published online June 17, 2024. doi:/10.1177/08980101241258014
- Blaszko MA, Avino K, Shields D, Rosa W, Dossey, BM. Dossey & Keegan’s Holistic Nursing: A Handbook for Practice. 8th ed. Jones & Bartlett Learning; 2022.