





Long-Term Outcomes of Mosaicplasty for SONK
Long-Term Outcomes of Mosaicplasty for Spontaneous Osteonecrosis of the Knee with Varus Alignment: A Retrospective Study with Up to 15 Years of Follow-up
Shogo Mukai1, Yasuaki Nakagawa2, Kohei Nishitani3,
- Department of Orthopedic Surgery, National Hospital Organization Kyoto Medical Center, Kyoto, Japan
- Department of Orthopedic Surgery, Japan Baptist Hospital, Kyoto, Japan
- Department of Orthopedic Surgery, Graduate School of Medicine, Kyoto University, Kyoto Japan
OPEN ACCESS
PUBLISHED: 31 July 2025
CITATION: Mukai, S., Nakagawa, Y., Nishitani, K., 2025. Long-Term Outcomes of Mosaicplasty for Spontaneous Osteonecrosis of the Knee with Varus Alignment: A Retrospective Study with Up to 15 Years of Follow-up. Medical Research Archives, [online] 13(7). https://doi.org/10.18103/mra.v13i7.6647
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v13i7.6647
ISSN 2375-1924
ABSTRACT
Background: Spontaneous osteonecrosis of the knee (SONK) commonly affects middle-aged and elderly individuals, and its management varies depending on disease progression. While joint replacement is often required in advanced cases, joint-preserving procedures such as mosaicplasty remain an option for early-stage lesions. However, clinical and radiological outcomes of mosaicplasty in this population remain unclear.
Methods: This retrospective study included 39 knees in 37 patients (mean age 69.1 ± 6.8 years) with SONK and femoro-tibial angle (FTA) <180° who underwent mosaicplasty alone. Patients were followed for a mean of 90 months. Clinical outcomes were assessed using the Lysholm score preoperatively, at 1 year postoperatively, and at final follow-up. Examination of MRI at 1 year was evaluated using the magnetic resonance observation of cartilage repair tissue (MOCART) scoring system. Conversion to total knee arthroplasty (TKA) was the primary endpoint, and survivorship analysis was conducted. Univariate and logistic regression analyses were used to identify risk factors for TKA.
Results: The mean Lysholm score significantly improved from 60.7 ± 6.4 preoperatively to 89.6 ± 6.6 at 1 year, and remained favorable at final follow-up (83.6 ± 12.7, P < 0.0001). No cases required revision surgery due to graft failure. However, 5 knees (13%) required conversion to TKA at a mean of 136 months. The 10-year and 15-year survival rates were 97% and 50%, respectively, with a median survival time of 188 months. Postoperative MOCART scores did not significantly correlate with clinical improvement. Among female patients, a higher body mass index (BMI) was identified as a significant risk factor for TKA conversion (odds ratio 1.66).
Conclusion: Mosaicplasty alone is an effective joint-preserving treatment for SONK in patients with FTA <180°, yielding significant long-term clinical improvement without graft failure. While MRI findings at one year may not predict outcomes, careful postoperative monitoring is warranted, particularly in female patients with higher BMI due to increased risk of late conversion to TKA.
Keywords: spontaneous osteonecrosis of the knee SONK, mosaicplasty, survivorship.
Introduction
Spontaneous osteonecrosis of the knee (SONK) is a known cause of knee pain in middle-aged and elderly individuals. While it shares several clinical and radiographic features with primary osteoarthritis, it is distinguished by pain at rest and during the night. Radiographic findings typically reveal subchondral bone collapse and cavitation resulting from insufficiency fractures, which can progress to osteochondral defects due to detachment of the affected area. These pathological changes are thought to result from bone marrow edema caused by insufficient fractures in the weight-bearing zones. More recently, this condition has been referred to as subchondral insufficiency fracture of the knee (SIFK).
Although conservative treatment is often the first line of management, many cases show rapid progression of deformity, and it has been reported that up to 30% of patients may require total knee arthroplasty (TKA) within three years. In early stages, high tibial osteotomy (HTO) aimed at joint preservation has been reported to be effective in preventing further deformation of the lesion. Moreover, several reports have suggested that combining HTO with autologous osteochondral transplantation (AOT; mosaicplasty, MOS) results in favorable cartilage repair at the lesion site, raising interest in whether this approach influences long-term outcomes.
On the other hand, in cases without significant varus malalignment, core decompression has been reported to be effective in alleviating symptoms caused by persistent bone marrow edema unresponsive to conservative management. Given this, mosaicplasty may potentially serve as a form of core decompression, making it a promising joint-preserving surgical option. However, the long-term feasibility and durability of joint preservation with this technique remain unclear. While mosaicplasty is well-established for treating cartilage defects in younger patients, its effectiveness in older patients with osteochondral lesions is still uncertain. Few reports have addressed whether graft integration and cartilage repair can be achieved in such cases. While favorable MRI findings showing good cartilage coverage have been correlated with clinical improvement in younger patients, other studies have reported persistent bone marrow edema or signs of osteonecrosis even after surgery. In particular, bone marrow edema in SONK is known to result from subchondral insufficiency fractures, and realignment via HTO has been shown to alleviate this condition. However, in cases treated with mosaicplasty alone, MRI findings often reveal persistent bone marrow edema and delayed or impaired integration of the osteochondral plugs.
Despite these findings, the relationship between imaging features, clinical symptoms, and long-term prognosis remains inadequately understood. The aim of this study is to evaluate the efficacy of mosaicplasty as a joint-preserving surgical procedure for SONK in patients without severe varus deformity. In the short term, we aim to assess whether osteochondral plugs can successfully integrate and lead to symptomatic improvement. In the long term, we aim to determine the rate of eventual conversion to total knee arthroplasty (TKA).
Patients and Methods
This study included patients diagnosed with SONK who underwent surgery at our institution between 2008 and 2020. Eligible patients were years old, had no prior knee surgery, underwent surgical intervention after failed conservative treatment, and were followed for at least two years postoperatively. The study protocol was approved by our institutional ethics committee, and informed consent was obtained from all participants prior to surgery and follow-up.
Initial diagnosis was made using plain radiographs and MRI. Conservative treatment included partial weight-bearing, orthotic support, and intra-articular injections. Surgical options were considered when conservative treatment failed and included total knee arthroplasty (TKA), mosaicplasty alone (Mos), or high tibial osteotomy combined with mosaicplasty (HTO+Mos). This study focused exclusively on patients treated with mosaicplasty alone.
All procedures were performed by two experienced surgeons (Y.N. and S.M.). After diagnostic arthroscopy and meniscal treatment, a medial parapatellar approach was used to expose the lesion. The area of necrosis was calculated as the product of its anteroposterior and mediolateral dimensions. Osteochondral plugs were harvested from the trochlea using the OATS system (Arthrex, Naples, Florida, the USA) and implanted into the lesion site. Postoperatively, a joint drain was placed, and non-weight-bearing was maintained for two weeks. Full weight-bearing was permitted at five weeks, with patients discharged upon regaining assisted ambulation using a cane. Follow-up evaluations were conducted every two months, with MRI and clinical assessment performed at one year and at regular intervals thereafter. Total knee arthroplasty was considered the endpoint in cases requiring further surgical intervention.
Collected data included sex, affected side, age at surgery, age at final follow-up, and body mass index (BMI). Femoro-tibial angle (FTA) was measured on full-length standing radiographs. Osteoarthritis severity was graded using the Kellgren Lawrence classification. Intraoperative findings included lesion area and the number and size of grafted plugs. Clinical outcomes were assessed using the Lysholm score preoperatively, one year postoperatively, and at the final follow-up. MRI evaluations at one year were scored using the magnetic resonance observation of cartilage repair tissue (MOCART) system, which includes cartilage surface integrity (0-20 points), graft integration (0-15), presence of osteonecrosis (0-10), and bone marrow edema (0-10), for a maximum score of 55. Statistical analyses were conducted using SPSS version 22 (IBM, Chicago, IL). Continuous variables were presented as mean ± standard deviation. The Wilcoxon signed-rank test was used for paired comparisons. Correlations between clinical and radiological scores were analyzed using rank correlation coefficient, and logistic regression analysis was performed to identify factors associated with TKA conversion. A p-value of <0.05 was considered statistically significant.
Results
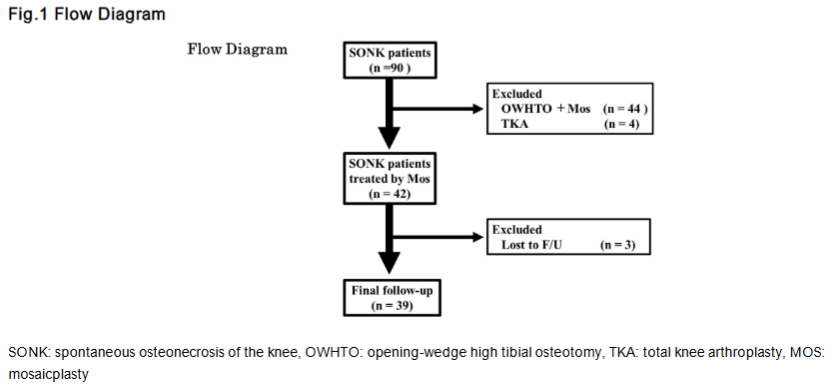
During the study period, 90 knees were diagnosed with SONK. Of these, 44 underwent HTO+Mos due to varus alignment (FTA >180°), 4 underwent TKA, and 42 received Mos alone. After excluding 3 cases lost to follow-up, 39 knees in 37 patients were followed for at least three years.
The cohort included 7 males (7 knees) and 30 females (32 knees), with 13 right and 26 left knees. The mean age at surgery was 69.1 ± 6.8 years (range, 52-79), and the mean follow-up duration was 90 months (range, 36-190). The mean age at final follow-up was 76.9 ± 7.1 years, and the mean BMI was 23.8 ± 4.2 kg/m². The average lesion area was 336 ± 100 mm², with a mean of 3.2 ± 1.0 plugs used per case.
| Parameter | Value |
|---|---|
| Age at surgery (years) | 69.1 ± 6.8 |
| Sex | 7 males, 30 females |
| Body mass index (kg/m²) | 23.8 ± 4.2 |
| Average lesion area (mm²) | 336 ± 100 |
| Mean follow-up duration (months) | 90 |
At surgery, OA severity was graded as KL2 in 18 knees, KL3 in 19, and KL4 in 2. At final follow-up, this distribution shifted to KL2 in 4, KL3 in 28, and KL4 in 7, with the average grade increasing from 2.6 ± 0.6 to 3.1 ± 0.5. The FTA significantly increased from 177 ± 2.5° preoperatively to 179 ± 2.9° at final follow-up. These changes in both KL grade and FTA were statistically significant (P = 0.0002 and P = 0.0001, respectively).
| Parameter | Preoperative | Final Follow-up |
|---|---|---|
| Kellgren-Lawrence Grade | 2.6 ± 0.6 | 3.1 ± 0.5 |
| Femoro-tibial Angle (°) | 177 ± 2.5 | 179 ± 2.9 |
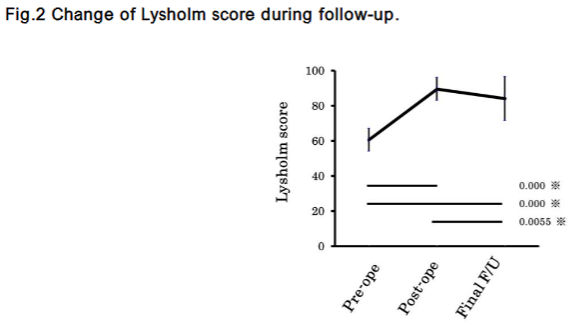
The mean Lysholm score improved from 60.7 ± 6.4 preoperatively to 89.6 ± 6.6 at one year postoperatively (P < 0.0001). At final follow-up, it slightly declined to 83.6 ± 12.7 but remained significantly improved compared to preoperative values (P < 0.0001 vs pre-op; P = 0.0055 vs 1-year post-op).
Examination of MRI at one year postoperatively yielded the following MOCART subscores: osteonecrosis, 3.2 ± 3.4/10; graft integration, 6.2 ± 6.0/15; bone marrow edema, 3.7 ± 3.2/10; cartilage surface, 9.7 ± 4.9/20; total MOCART score, 22.8 ± 13/55.
| Parameter | Value |
|---|---|
| Age at surgery | Not significant |
| Sex | Not significant |
| Body mass index | Trend toward significance (P = 0.062) |
| Lesion area | Not significant |
| Kellgren-Lawrence grade | Not significant |
| MOCART score | Not significant |
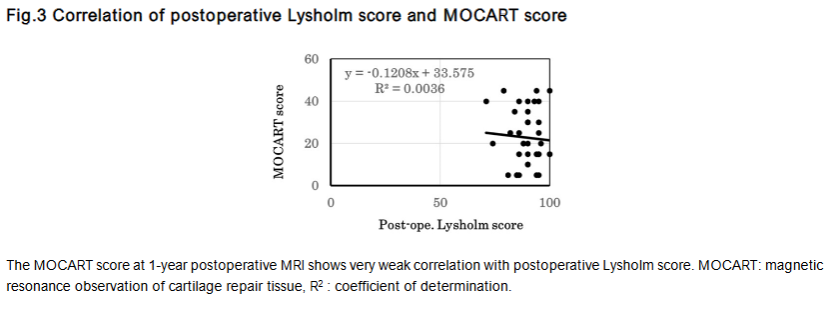
The correlation between the Lysholm and MOCART scores at 1 year was minimal (R² = 0.0036).
Similarly, weak correlations were observed for age (R² = 0.22), sex (R² = 0.23), BMI (R² = 0.14), lesion size (R² = 0.12), and KL grade (R² = 0.18) with MOCART scores. BMI showed the strongest (yet nonsignificant) correlation with Lysholm score (R²= 0.31).
| Parameter | Value |
|---|---|
| Age at surgery | Not significant |
| Sex | Not significant |
| Body mass index | Not significant |
| Lesion size | Not significant |
| Kellgren-Lawrence grade | Not significant |
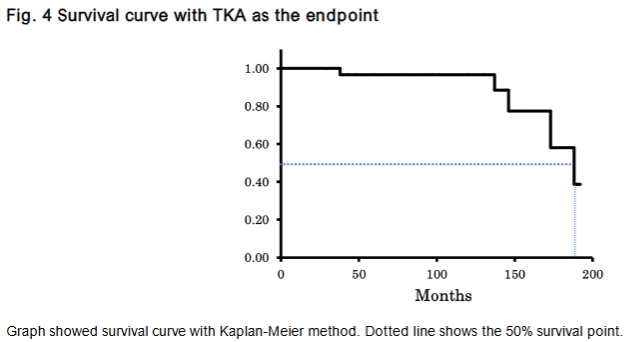
During the follow-up period, five knees required conversion to TKA all in female patients. The mean age at surgery in these cases was 65.2 years, and the mean duration to TKA was 136 months, with a mean age at conversion of 76.2 years. The 10-year and 15-year survival rates were 97% and 50%, respectively.
Among the 32 female cases, those who required TKA had a lower mean age at surgery (65.2 ± 5.8 vs. 69.7 ± 6.8 years), higher BMI (27.8 ± 3.5 vs. 23.3 ± 4.0 kg/m²), and lower MOCART scores (14.1 ± 8.9 vs. 26.2 ± 13.6) than those who did not require TKA. Logistic regression identified BMI as the most influential factor, with an odds ratio of 1.66.
| Parameter | Value |
|---|---|
| Age at surgery | Not significant |
| Body mass index | Odds ratio 1.66 |
| MOCART score | Not significant |
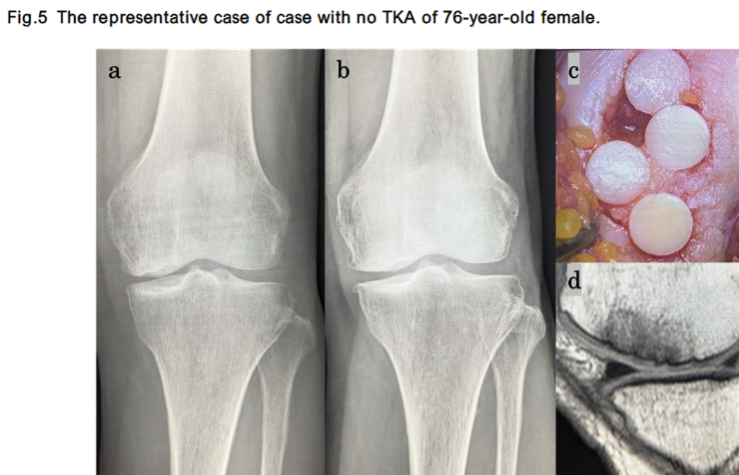
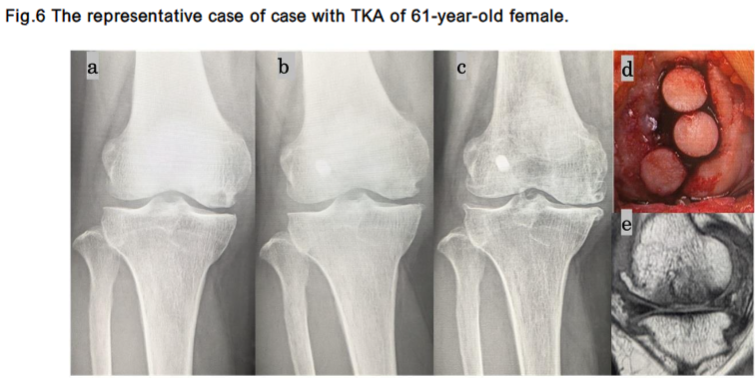
The changes in X-ray findings, intraoperative findings, and MRI findings are shown for two representative cases.
Discussion
The present study demonstrates that among the 39 knees diagnosed with spontaneous osteonecrosis of the knee (SONK) and treated with mosaicplasty (Mos) with a femorotibial angle (FTA) less than 180°, all cases showed improved Lysholm scores at one year postoperatively. However, no correlation was observed between clinical outcomes and MOCART scores. Over an average follow-up of 90 months, a significant progression of joint deformity and an increase in FTA were noted. Thirteen percent of cases required conversion to total knee arthroplasty (TKA), with a 50% joint survival rate at 188 months. All five knees that progressed to TKA were female, reaching the endpoint at an average of 120 months postoperatively. In addition to female sex, higher BMI was considered a risk factor for TKA conversion.
In SONK, patients often report severe pain even at rest or during the night, which is thought to result from bone marrow edema centered in the weight-bearing region. Several reports on the natural course of SONK have shown high rates of progression to TKA, with Jureus reporting TKA in 15 out of 40 patients and Nashi in 9 out of 42 cases (21%). Pareek noted that 30% of cases required TKA within 3 years, highlighting the rapid deterioration associated with SONK. In contrast, Duany reported a joint preservation rate of 87% at 40 months in patients treated with core decompression or autograft procedures.
In our current series limited to patients with an FTA less than 180°, all cases showed gradual radiographic progression of osteoarthritis and varus alignment over time. Thirteen percent underwent TKA after an average of 90 months. These patients had initially received Mos at an average age of 65 and progressed to Kellgren-Lawrence grade 4 within a decade. These findings suggest that Mos contributes to the structural restoration of the articular surface and may help return the joint to a more natural degenerative pathway, thus prolonging joint preservation.
Secondary osteonecrosis tends to affect younger patients and present with milder osteoarthritis, but with a larger necrotic area. Even in such cases, long-term joint preservation has been reported with Mos. These reports, along with our findings, suggest that the repair of the cartilage surface may slow the progression of joint deformity. In our study, even in cases of primary osteonecrosis in middle-aged and elderly patients with poor bone quality and bone marrow edema, the transplanted osteochondral plugs remained stable, showed good bone integration, and no recurrence of necrosis on radiographs. These outcomes indicate that Mos grafts can survive under various conditions, and Mos should be considered a critical surgical option for joint preservation. From a technical standpoint, it is essential to remove all necrotic bone and thoroughly debride down to healthy cancellous bone to ensure optimal graft integration.
SONK is increasingly recognized as a condition initiated by medial meniscus (MM) extrusion, which causes localized mechanical overload and insufficiency fractures, ultimately triggering bone marrow edema and pain. Pareek identified additional TKA risk factors including MM extrusion, femoral condyle involvement, bone marrow edema, and lateral meniscal injury. In patients with increased FTA, lateral compartment stress may increase, making concomitant high tibial osteotomy (HTO) a reasonable consideration. Our previous work showed that HTO could reduce bone marrow edema at the graft site. However, as also observed in this study, MOCART scores at one year postoperatively showed little correlation with clinical outcomes.
In this series, no male patients progressed to TKA, possibly because the majority (34 out of 41 knees) underwent concurrent HTO due to an FTA >180°. Therefore, risk factors specific to males could not be evaluated. Some reports suggest that women may have lower bone mineral density and are more likely to develop subchondral insufficiency fractures (SIFK) before FTA increases significantly.
Regarding TKA risk factors in SONK, Nashi found no significant association with lesion size, sex, or age on MRI, while Jureus reported larger lesion size as a risk factor. Pareek identified older age and the presence of mirror lesions as predictive. For long-term outcomes of Mos, Nishitani reported 100% joint survival at 14 years in younger patients with secondary osteonecrosis, and Ehman reported an 87% 10-year survival rate for patients with a mean age of 38 who underwent HTO plus Mos for cartilage injury.
Our study focused on middle-aged to elderly patients with SONK and an FTA <180°, treated solely with Mos. Over a mean of 90 months, 13% underwent TKA, and the 50% survival point was reached at 188 months, indicating a favorable long-term joint preservation outcome. These results suggest that SONK involves not only cartilage injury but also osteochondral defects, and Mos is a highly effective treatment in such cases. Notably, all patients who progressed to TKA in our study were female. Among female patients, high BMI emerged as a significant risk factor for TKA progression, while younger age at surgery and lower MOCART scores also trended toward higher risk. The association between high BMI and TKA is well established in osteoarthritis. Interestingly, younger surgical age may imply higher postoperative activity levels and increased mechanical stress, contributing to earlier degeneration. While higher MOCART scores may be protective, further investigation is needed.
Limitations
This study is a retrospective case series with a limited sample size, restricting the ability to draw definitive conclusions regarding risk factors. Furthermore, Mos alone for SONK is relatively uncommon, and the use of osteochondral allografts is increasing. Long-term follow-up studies for such cases remain scarce, which gives this report added value. Additionally, no control group was included, and the decision to undergo TKA ultimately rests with the patient, meaning that some patients with poor function may have declined surgery.
To address these issues, larger case numbers are required. Although we continue to consider Mos a viable option for SONK with FTA <180°, in practice, cases where the mechanical axis falls below 50% of the tibial plateau may still require concurrent HTO. Given the 50% 15-year survival rate observed, Mos may be a suitable option for elderly patients with lower activity levels.
Conclusion
In SONK cases with FTA <180° treated with Mos alone, no cases required revision surgery due to graft failure, and clinical outcomes significantly improved. However, postoperative MRI findings showed no significant correlation with clinical improvement. Thirteen percent of cases required TKA after a mean of 90 months, and the 50% survival time was 188 months, indicating that long-term joint preservation is achievable. Among female patients, high BMI was identified as a significant risk factor for TKA conversion.
Conflict of Interest Statement:
None.
Funding Statement:
None.
Acknowledgements:
None.
References:
- Ahlback S, Bauer GC, Bohne WH. Spontaneous osteonecrosis of the knee. Arthritis Rheum. 1968; 11(6):705-733.
- Koshino T, Okamoto R, Takamura K, et al. Arthroscopy in spontaneous osteonecrosis of the knee. Orthop Clin North Am. 1979;10(3):609-618.
- Yamamoto T, Bullough PG. Spontaneous osteonecrosis of the knee: the result of subchondral insufficiency fracture. J Bone Joint Surg Am. 2000;82(6):858-866.
- Motohashi M, Morii T, Koshino T. Clinical course and roentgenographic changes of osteonecrosis in the femoral condyle under conservative treatment. Clin Orthop Relat Res. 1991;(266):156-161.
- Yates PJ, Calder JD, Stranks GJ, et al. Early MRI diagnosis and non-surgical management of spontaneous osteonecrosis of the knee. Knee. 2007;14(2):112-116.
- Pareek A, Parkes CW, Bernard C, et al. Spontaneous Osteonecrosis/subchondral insufficiency fractures of the knee: high rates of conversion to surgical treatment and arthroplasty. J Bone Joint Surg Am. 2020;102(9):821-829.
- Koshino T. The treatment of spontaneous osteonecrosis of the knee by high tibial osteotomy with and without bone-grafting or drilling of the lesion. J Bone Joint Surg Am. 1982;64(1):47-58.
- Takeuchi R, Aratake M, Bito H, et al. Clinical results and radiographical evaluation of opening wedge high tibial osteotomy for spontaneous osteonecrosis of the knee. Knee Surg Sports Traumatol Arthrosc. 2009;17(4):361-368.
- Kumagai K, Akamatsu Y, Kobayashi H, et al. Mosaic osteochondral autograft transplantation versus bone marrow stimulation technique as a concomitant procedure with opening-wedge high tibial osteotomy for spontaneous osteonecrosis of the medial femoral condyle. Arthroscopy. 2018;34(1):233-240.
- Berger C, Kroner AH, Kristen KH, et al. Transient bone marrow edema syndrome of the knee: clinical and magnetic resonance imaging results at 5 years after core decompression. Arthroscopy. 2006;22(8):866-871.
- Villari E, Digennaro V, Panciera A, et al. Bone marrow edema of the knee: a narrative review. Arch Orthop Trauma Surg. 2024 May;144(5):2305-2316.
- Hangody L, Fules P. Autologous osteochondral mosaicplasty for the treatment of full-thickness defects of weight-bearing joints: ten years of experimental and clinical experience. J Bone Joint Surg Am. 2003;85(Suppl 2):25-32.
- Gudas R, Kalėnsinskas RJ, Kimtys V, et al. A prospective randomized clinical study of mosaic osteochondral autologous transplantation versus microfracture for the treatment of osteochondral defects in the knee joint in young athletes. Arthroscopy. 2005;21(9):1066-1075.
- Gudas R, Guadaite A, Pocius A, et al. Ten-year follow-up of a prospective, randomized clinical study of mosaic osteochondral autologous transplantation versus microfracture for the treatment of osteochondral defects in the knee joint of athletes. Am J Sports Med. 2012;40(11):2499-2508.
- Marcacci M, Kon E, Delcogliano M, et al. Arthroscopic autologous osteochondral grafting for cartilage defects of the knee: prospective study results at a minimum 7-year follow-up. Am J Sports Med. 2007;35(12):2014-2021.
- Kotani A, Ishii Y, Sasaki S. Autogenous osteochondral grafts for osteonecrosis of the femoral condyle. J Orthop Surg (Hong Kong). 2003;11(2):117-122.
- Tanaka Y, Mima H, Yonetani Y, et al. Histological evaluation of spontaneous osteonecrosis of the medial femoral condyle and short-term clinical results of osteochondral autografting: a case series. Knee. 2009;16(2):130-135.
- Ma J, Ren Y, Wang B, et al. Autologous Osteochondral Transplantation for Young Patients with Postcollapse Osteonecrosis of the Knee: A Retrospective Cohort Study with an Average 7-Year Follow-Up. Cartilage. 2021 Dec;13(1_suppl):1291S-1297S.
- Tetta C, Busacca M, Moio A, et al. Knee osteochondral autologous transplantation: long-term MR findings and clinical correlations. Eur J Radiol. 2010;76(1):117-123.
- Nemec SF, Marlovits S, Trattnig S. Persistent bone marrow edema after osteochondral autograft transplantation in the knee joint. Eur J Radiol. 2009;71:159-163.
- Link TM, Mischung J, Wortler K, et al. Normal and pathological MR findings in osteochondral autografts with longitudinal follow-up. Eur Radiol. 2006;16:88-96.
- Kroner AH, Berger CE, Kluger R, et al. Influence of high tibial osteotomy on bone marrow edema in the knee. Clinic. Orthop. Rel. Res. 2006;454:155-162.
- Marti CB, Rodriguez M, Zanetti M, et al. Spontaneous osteonecrosis of the medial compartment of the knee: a MRI follow-up after conservative and operative treatment, preliminary results. Knee Surg Sports Traumatol Arthrosc. 2000;8(2):83-88.
- Choi HG, Kim JS, Yoo HJ, et al. The fate of bone marrow lesions after open wedge high tibial osteotomy: a comparison between knees with primary osteoarthritis and subchondral insufficiency fractures. Am J Sports Med. 2021;49(6):1551-1560.
- Mukai S, Nakagawa Y, Nishitani K, et al. Mosaicplasty with high tibial osteotomy for knee subchondral insufficiency fracture had better magnetic resonance observation of cartilage repair tissue scores with less bone marrow edema and better plug union and less plug necrosis compared with mosaicplasty alone. Arthroscopy. 2023;39(2):337-346.
- Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957;16:494-502.
- Lysholm J, Gillquist J. Evaluation of knee ligament surgery results with special emphasis on use of a scoring scale. Am J Sports Med. 1982;10(3):150-154.
- Marlovits S, Striessnig G, Resinger CT, et al. Definition of pertinent parameters for the evaluation of articular cartilage repair tissue with high-resolution magnetic resonance imaging. Eur J Radiol. 2004;52(3):310-319.
- Marlovits S, Singer P, Zeller P, et al. Magnetic resonance observation of cartilage repair tissue (MOCART) for the evaluation of autologous chondrocyte transplantation: determination of interobserver variability and correlation to clinical outcome after 2 years. Eur J Radiol. 2006;57:16-23.
- Ochi J, Nozaki T, Nimura A, et al. Subchondral insufficiency fracture of the knee: review of current concepts and radiological differential diagnoses. Jpn J Radiol. 2022;40(5):443-457.
- Juréus J, Lindstrand A, Geijer M, et al. The natural course of spontaneous osteonecrosis of the knee (SPONK): a 1- to 27-year follow-up of 40 patients. Acta Orthop. 2013;84(4):410-414.
- Nashi N, Chan CX, Choo SX, et al. Does the osteonecrotic volume/other factors predict progression to total knee arthroplasty in spontaneous osteonecrosis of the knee? An MRI study. J Clin Orthop Trauma. 2024;53:102442.
- Duanny GD, Zywiel MG, McGrath MS, et al. Joint-preserving surgical treatment of spontaneous osteonecrosis of the knee. Arch Orthop Trauma Surg. 2010;130(1):11-16.
- Nishitani K, Nakagawa Y, Kobayashi M, et al. Clinical and radiological outcomes of osteochondral autograft transfer for spontaneous osteonecrosis of the knee. Cartilage. 2021;13(1_suppl):1156S-1164S.
- Jungmann PM, Gersing AS, Baumann F, et al. Cartilage repair surgery prevents progression of knee degeneration. Knee Surg Sports Traumatol Arthrosc. 2019;27(9):3001-3013.
- Hussain ZB, Chahla J, Mandelbaum BR, et al. The role of meniscal tears in spontaneous osteonecrosis of the knee: a systematic review of suspected etiology and a call to revisit nomenclature. Am J Sports Med. 2019;47(2):501-507.
- Fujisawa T, Choe H, Kusaba Y, et al. Medial meniscus extrusion and stage are related to the size of spontaneous osteonecrosis of the knee in patients who underwent high tibial osteotomy. Knee. 2022;36:72-79.
- Pareek A, Parkes CW, Bernard CD, et al. The SIFK score: a validated predictive model for arthroplasty progression after subchondral insufficiency fracture of the knee. Knee Surg Sports Traumatol Arthrosc. 2020;28(10):3149-3155.
- Akamatsu Y, Mitsugi N, Hayashi N, et al. Low bone mineral density is associated with the onset of spontaneous osteonecrosis of the knee. Acta Orthop. 2012;83(3):249-255.
- Zanetti M, Romero J, Dambacher MA, et al. Osteonecrosis diagnosed on MR images of the knee: relationship to reduced bone mineral density determined by high resolution peripheral quantitative CT. Acta Radiol. 2003;44(5):525-531.
- Ehmann YJ, Esser T, Vieider RP, et al. Clinical outcomes and long-term survivorship after osteochondral autologous transfer combined with valgus high tibial osteotomy: an analysis after 19 years with 56 patients. Arthroscopy. 2024;39(2):337-346.
- Tirico LEP, Early SA, McCauley JC, et al. Fresh osteochondral allograft transplantation for spontaneous osteonecrosis of the knee: a case series. Orthop J Sports Med. 2017;5(10):2325967117730540.