





Menstrual Health Management for Adolescents with Disabilities
Best practices in Menstrual Health and Management for Adolescents with Disabilities Worldwide
Nili Amir, MD¹, Rose Goddard-Carmel², Susan Ernst, MD³, Monica Woll Rosen, MD³*
- University of Connecticut Department of Obgyn
- University of Michigan Medical School
- University of Michigan Department of Obgyn
- University of Michigan Department of Obgyn
OPEN ACCESS
PUBLISHED 31 July 2025
CITATION Amir, N., Goddard-Carmel, R., et al., 2025. Best practices in Menstrual Health and Management for Adolescents with Disabilities Worldwide. Medical Research Archives, [online] 13(7). https://doi.org/10.18103/mra.v13i7.6763
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v13i7.6763
ISSN 2375-1924
ABSTRACT
The onset of menstruation can present significant challenges, including vulnerability, abuse risk, unintended pregnancies, difficulties with managing menstrual hygiene, abnormal uterine bleeding, painful menses, behavioral and mood changes, or changes in seizure pattern. These challenges manifest in an even greater way for individuals with disabilities and are often accompanied by significant societal repercussions. While adolescents with disabilities already are disadvantaged due to medical challenges and inaccessible environments, adding the burden of menstruation with all its social, cultural, and medical challenges can be overwhelming. Menstrual suppression is a way to reduce menstrual frequency, duration and intensity. It is used for a variety of reasons, including to improve quality of life for those who experience significant negative impacts or restrictions in activities due to their menses. Adolescents with disabilities may seek menstrual suppression for help with irregular or heavy bleeding, dysmenorrhea, behavioral changes, or personal hygiene. While this is one way to improve quality of life surrounding menstruation, improved policies and health education globally are also needed to combat the menstrual health barriers faced by this population. The purpose of this review is to summarize best practices in menstrual health and management for adolescents with disabilities worldwide.
Keywords
- Menstrual health
- Adolescents
- Disabilities
- Menstrual suppression
- Health education
Introduction
Menstrual management encompasses all practices used to help with menstruation. This includes medications to decrease blood flow, techniques for maintaining hygiene, strategies to manage mood changes, and exercises to reduce menstrual pain. Menstrual health is defined by the United Nations International Children’s Emergency Fund (UNICEF) as encompassing “the broader impacts of the psychological, socio-political and environmental factors that accompany menstruation on mental, physical, and emotional health.” Menstruation can present significant challenges to adolescents, especially those with significant bleeding, pain, mood changes, or hygiene issues, which can lead to decreased quality of life.
For adolescents with disabilities, defined as a heterogenous group of individuals between ages 10 and 19 years old with varying physical, cognitive, sensory and developmental abilities, menstrual health can be even more challenging. The difficulty varies based on several factors, including sociocultural context, physical and cognitive abilities, and other medical comorbidities. The World Health Organization (WHO) espouses a social model of disability suggesting that multiple variables lead to impairment of function for individuals with certain health conditions, including inaccessible environments, lack of social support, and negative attitudes about individuals with disabilities in the community. According to the United Nations Children’s Fund (UNICEF) and the WHO, there are 240 million children and adolescents worldwide living with a disability. The purpose of this review is to summarize best practices in menstrual health and management for adolescents with disabilities worldwide.
DISCRIMINATION AND REPRODUCTIVE AUTONOMY:
In many countries, girls and women are still treated as second class citizens. Children with disabilities are some of the most marginalized people globally. Therefore, adolescent girls with disabilities often experience double discrimination based on gender and ableism. When considering menstrual management or suppression in girls with disabilities, it is imperative to understand the history of reproductive injustice in this population, particularly with respect to intellectual and developmental disabilities.
Societal attitudes and policies have restricted the reproductive autonomy of girls and women with disabilities, denying them the right to make informed choices about their bodies and parenthood. Violence, including sexual assault, against girls with disabilities is well-documented and abuse and undesired pregnancy are often concerns for parents and caregivers of girls seeking menstrual management. It is important to emphasize that while using medication for menstrual management may provide contraception, it will not prevent abuse. This background understanding of the world in which girls with disabilities experience discrimination should inform policy and programs for both prevention of violence and medical care that emphasizes autonomy for this population.
With advances in medical care, more adolescents with disabilities are entering puberty and becoming adults. During this time, adolescents should be learning how to manage their menstruation; however, adolescents with disabilities often receive no or inadequate menstrual health education. When they do receive reproductive health education, they are often given misinformation, such as that they are infertile. While their peers without disabilities often learn about menstrual management informally through friends, the internet, or television, girls with disabilities often lack these connections and resources. Additionally, adolescents with disabilities have unique menstrual health issues that their counterparts may not experience. This has led to lower use of contraception, poor utilization of gynecologic care, unintended pregnancies, and sexual abuse. There is a significant need for better reproductive and menstrual health education in this population.
Global Perspective
The stigma surrounding disability may be amplified by menstrual stigmatization. For young women living in low- or middle-income countries, menstruation poses challenges, as menstruating girls and women may be considered dirty or impure. Consequently, young women may face restrictions on their daily activities, managing hygiene, and ability to bathe for fear of contaminating others. Specifically, in countries like India and Nepal, menstruating individuals are not allowed to participate in religious rituals or even cook or touch certain foods. Additionally, the lack of access to menstrual hygiene products, sanitation facilities, and relevant education surrounding menstruation has been shown to negatively impact school participation, health, and well-being of young women worldwide. Period poverty disproportionately affects individuals in low-income communities and developing countries, leading to various health, social, and economic challenges. Menstrual health, education, safety, and autonomy highlight the critical role of menstrual health within human rights agendas aimed at promoting well-being.
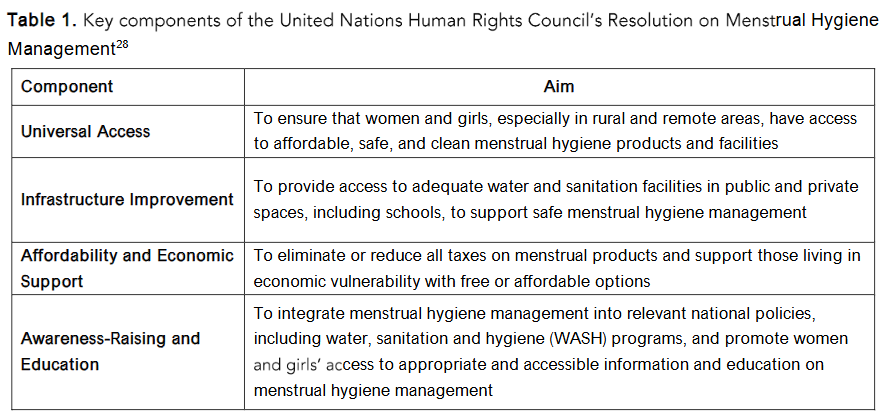
In July 2024, the United Nations Human Rights Council declared that addressing menstrual hygiene management is essential for advancing the human right to health and gender equity and impacts the overall health, well-being, and dignity of girls and women. The resolution specifically recommended the items listed in Table 1. Following are some examples of initiatives that aim to improve menstrual health education and hygiene globally, many of which help to address stigmas and cultural misperceptions surrounding menstruation. These initiatives suggest that individuals should be able to manage menstruation in a dignified and healthy way. Although many of these programs are not specifically targeted to adolescents with disabilities, they have an indirect benefit for this patient population. For example, the United Nations Population Fund and the WHO have developed guidelines to integrate menstrual health research into health services and policies. India, Kenya, and the United Kingdom have provided policies, guidelines, and programs to promote education and awareness on menstruation in schools. Several non-governmental organizations have similar programs, such as WASH United in Germany, which holds a menstrual hygiene day to educate the public on menstrual health needs.
Barriers to Care
In addition to cultural attitudes surrounding menstrual health, there are several barriers adolescents with disabilities may face that lead to additional challenges. Communication may be a barrier to care for girls and women with disabilities. Effective communication may require creativity and adjustments based on the patient’s cognitive abilities or hearing and visual limitations. The Americans with Disabilities Act (ADA) requires that clinicians ensure effective communication with persons with disabilities; however, it does not mandate specific modalities to achieve this goal. Instead, the ADA requires prioritization of patient preferences when choosing options for effective communication. Providing options for how information is presented (visual, written, or verbal) allows adolescents with disabilities and their caregivers or family members to select the most accessible format. Patients who are deaf or hard of hearing may prefer Sign Language and an interpreter may be needed to facilitate the preferred method of communication will allow them to be fully engaged in their own care. Additionally, bias may lead to barriers to healthcare for people with disabilities. Healthcare professionals may make inaccurate assumptions about the cognitive and physical abilities of girls or women with disabilities. Therefore, it is imperative that the clinician enter a healthcare encounter with an open mind and involve the patient by directly addressing them. Though the patient’s family or caregiver are often present, it does not necessarily mean that the patient is dependent on them. Therefore, it is important to assess an adolescent’s competence and ability to communicate to allow for appropriate patient autonomy based on the individual’s age and level of competence.
Physical barriers vary based on the type of disability and may be present in the community or in healthcare facilities. For patients in wheelchairs, public restrooms may not be equipped to accommodate space for maneuvering a wheelchair and stores where menstrual products are sold may lack ramps that would allow a wheelchair to enter. In healthcare facilities, buildings may not be designed for wheelchair accessibility and exam rooms may not have accessible exam tables, making it challenging to examine a patient with a physical disability.
Lastly, menstrual hygiene can be a significant problem for adolescents with disabilities. Adolescents with limited dexterity may not be able to open packages to use menstrual products or to clean themselves during menses. Caregivers should be taught to assist these adolescents in a respectful way. Some other opportunities to improve menstrual hygiene management include equipping restrooms with adaptations and supports, such as grab bars, lower sinks, and wider doorways; using period absorbing underwear; and utilizing menstrual cycle tracker apps to prepare for when menses will commence. Additionally, menstrual suppression can be used as a tactic to help with hygiene.
Menstrual Suppression
Menstrual suppression is reducing menstrual frequency, duration, or intensity. It is used for a variety of reasons, including to improve quality of life for those who experience significant negative impacts or restrictions in activities due to their menses. If menstrual suppression is desired, treatment should be individualized based on the reason for initiation and other comorbidities the patient has. Adolescents with disabilities may seek menstrual suppression due to concerns with irregular or heavy bleeding, dysmenorrhea, behavioral changes, personal hygiene, and medical comorbidities exacerbated by menstruation, including catamenial epilepsy and menstrual migraines. Clinicians should use a patient-centered approach to counseling adolescents and their families or caregivers about the option for menstrual suppression. The American College of Obstetricians and Gynecologists (ACOG) states that gynecologic healthcare for women and adolescents with disabilities is comprehensive; maintains confidentiality; is an act of dignity and respect toward the patient; maximizes the patient’s autonomy; avoids harm; and assesses and addresses the patient’s knowledge of puberty, menstruation, sexuality, and consent. In regions where clinical care is accessible, medications or devices are available, and it is culturally acceptable to manipulate menses, adolescents should be counseled regarding options for menstrual suppression. Any treatment should align with their reproductive and sexual goals and minimize side effects and complications of treatment.
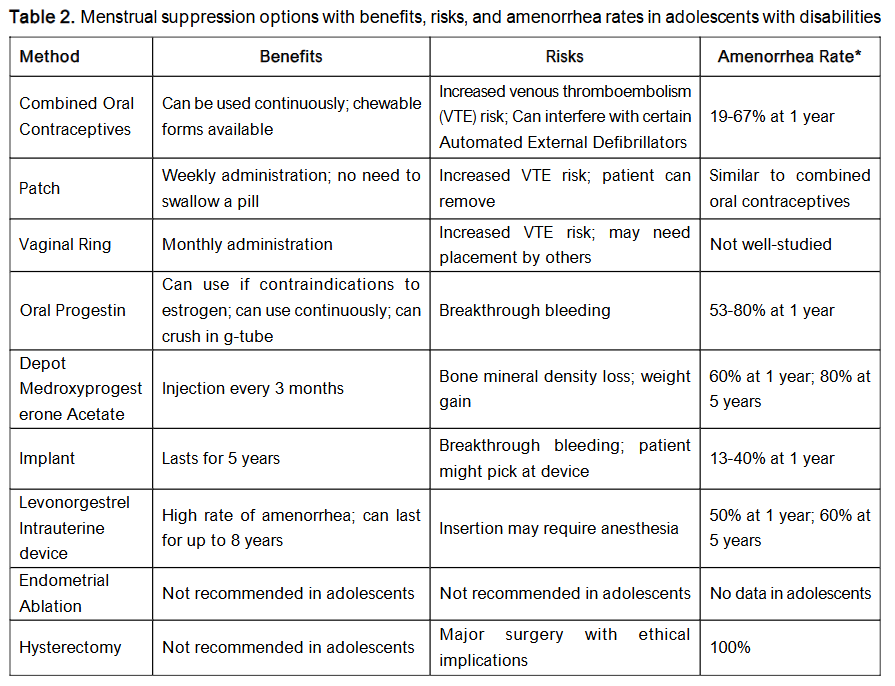
Medications for menstrual suppression should not be initiated prior to menarche, as this could expose the patient to years of hormonal medication unnecessarily. Awaiting menarche also confirms normal hormonal function and absence of hormonal imbalance or an obstructive anomaly. When a decision is made to pursue treatment, shared decision-making should be used to determine the best method for menstrual management. Surgical or permanent interventions may involve ethical and legal concerns and are rarely required to achieve desired clinical outcomes. Table 2 outlines menstrual suppression options and their associated benefits, risks, and amenorrhea rates.
NON-HORMONAL OPTIONS
Non-Steroidal Anti-inflammatory Drugs (NSAIDs) For patients with heavy menstrual bleeding, NSAIDs may decrease bleeding volume by 30-40%. This treatment may also be useful in patients experiencing dysmenorrhea. Although this treatment will not stop menses, it may be preferred for those hoping to avoid hormonal therapy.
Tranexamic Acid (TXA) Antifibrinolytic drugs, such as TXA, are effective in decreasing excessive menstrual bleeding by about 50%. Unlike NSAIDs, TXA will have minimal effect on pain associated with menses. Similar to NSAIDs, this treatment may be preferred for individuals hoping to avoid hormonal therapy. TXA may not be appropriate for those at risk of VTE and should be avoided in patients with known clotting disorders, though data from a systematic review did not demonstrate an increased rate of VTE for patients treated with TXA.
COMBINED HORMONAL OPTIONS
Options for menstrual management with both estrogen and progestin may be offered in the form of a combined oral contraceptive pill, a transdermal patch, or a vaginal ring. In addition to menstrual suppression, combined hormonal contraceptive methods may be useful in treating dysmenorrhea, cyclic mood changes, or menstrual migraines. Depending on duration of use, these may also be effective as contraception. Combined hormonal contraception is contraindicated in patients with history of VTE, diabetes with microvascular complications, history of estrogen-dependent cancers, migraines with aura, tobacco use in those aged 35 or older, hypertension, or liver disease. Additionally, enzyme-inducing anti-epileptic drugs may affect the metabolism of estrogen and progesterone, which may necessitate dose adjustment and discussion of efficacy for those who choose estrogen and progesterone systemic medications as an option.
Combined oral contraceptive pills can be used in a cyclic or continuous manner. With the continuous method, complete amenorrhea is achieved in 66-88% of patients after one year. Other advantages of combined oral contraceptive pills include decreased risk of premenstrual mood disorders. There are many formulations, which include different dosages of estrogen and various types of progestins that allow for adjustments to increase benefits and desired results while decreasing side effects. The combined oral pill is a good option for those looking for a non-invasive method or who already take other daily medications. If an individual is unable to swallow pills, there are chewable options or pills that can be crushed and administered through a gastrostomy tube.
Transdermal patches can also be offered in a continuous fashion. Continuous absorption of estrogen with use of the contraceptive patch increases circulating concentrations of estrogen compared to standard-dose combined oral contraceptive pills. Due to the elevated estrogen concentrations, there is a theoretical increased risk of VTE associated with the patch, though this is not proven. Patients with sensory issues may attempt to pick at the patch or remove it. If sensory issues are relevant, the patient or caregiver can place the patch in a location where it is less accessible, such as between the shoulder blades.
The vaginal ring may also be offered. It can be used continuously or inserted in the vagina and removed after three weeks for withdrawal menses; however, considerations around ease and ability of insertion and removal may need to be addressed for patients with limitations in mobility or fine motor control. In the general population, the risk of VTE is very low in adolescents and young adults. Use of combined hormonal contraception doubles this risk, but overall, the risk remains low. Still, it would not be unreasonable to consider progesterone-only alternatives in patients with limitations in mobility who may have increased risk of VTE.
PROGESTIN-ONLY OPTIONS
Options for menstrual management with a progestin-only method include pills, an injection, or an implant. These are more suitable options for patients for whom estrogen is contraindicated. Avoidance of estrogen would minimize the risk of VTE. Similar to combined hormonal contraception, these options may also be used for contraception depending on duration and consistency of use.
Progestin-only pills, when used continuously, are another option for menstrual management. A variety of progesterone formulations can be used, including norethindrone, norethindrone acetate, drospirenone, megestrol acetate, and medroxyprogesterone. They can be administered orally or given through a feeding tube. The benefits of pills are that dose adjustments can be made to attempt complete amenorrhea. For low-dose norethindrone, the rate of complete amenorrhea can be as low as 20%; however, data from our clinic show that with increasing doses of norethindrone acetate, rates are closer to 54%. Progestin-only pills decrease menstrual flow, though breakthrough bleeding is common and can be challenging for caregivers to manage due to its unpredictability. Other side effects can include weight gain, changes in mood, acne, and breast tenderness.
Depot Medroxyprogesterone Acetate (DMPA) is a type of medication for menstrual management that is injected intramuscularly every 12 weeks. DMPA is a useful option for those who have difficulty swallowing pills, have contraindications to estrogen, or do not want to take a daily medication. Around 90% of patients reach amenorrhea following their fourth dose, although spotting is not uncommon. The main risk factor for DMPA is loss of bone mineral density, which may increase risk of fracture in women with developmental disabilities. Attenuation of bone mineral density can be particularly worrisome in teenage populations, when bone mass is actively accruing. Among all patients, the rate of bone loss has been shown to decrease the longer DMPA is used and is reversible once the medication is stopped regardless of duration of use. Special consideration should be given to patients with a seizure disorder and on certain anti-epileptic drugs, as these patients have a higher risk of falling, predisposing them to fractures. Additionally, certain seizure medications such as valproic acid may lower bone density. Patients with disabilities may have existing decreased bone density due to limited mobility secondary to disuse osteoporosis and anticonvulsant medications. While adequate intake of calcium and vitamin D is important for everybody, it can be particularly important for this population to help mitigate some of these risks.
Another challenge with DMPA use is weight gain. On average, women gain 13 pounds over the course of four years while using DMPA; this can be a unique challenge in patients with mobility limitations, because even minimal weight gain can make transfers more difficult and impede independent functioning.
Etonogestrel Implants are a subcutaneous device placed in the arm that has demonstrated efficacy for up to five years. These implants are not suggested as first-line therapy, as irregular bleeding is not uncommon and the amenorrhea rate is only about 20% through five years. Additionally, patients with disabilities may struggle with the insertion of the device in the office, so sedation may be required. Those with sensory issues might not tolerate its placement or may struggle with being able to feel the device underneath their skin.
Levonorgestrel Intrauterine Device (IUD) are a form of long-acting reversible contraception that are inserted into the uterus. The 52mg levonorgestrel IUD formulations are effective for up to eight years. IUDs are very effective as contraception and reported amenorrhea rates among adolescents with disabilities are as high as 60%. Systemic side effects are minimal and the IUD progressively decreases bleeding and pain associated with menstruation. Though expulsion is possible, the recorded risk is low, at around 8.5%. Similarly, elective removal for bleeding or discomfort is around 5.7%. Breakthrough bleeding is a possibility particularly around the time of insertion. One of the unique challenges of the IUD is the possible need for sedation or general anesthesia to insert the device into the uterus. Some patients may be able to tolerate insertion without sedation; however, potential communication barriers and mobility challenges can require the need for sedation for muscle relaxation.
Surgical Management
ENDOMETRIAL ABLATION
An endometrial ablation is a minor surgical procedure that causes destruction of the endometrial lining of the uterus to eliminate menses or decrease the amount of bleeding with menses. The reported rates of amenorrhea range from 13-83%, with typically lower rates for women under age 45. Pregnancy is still possible after endometrial ablation, so contraception would be necessary. It is only considered in patients who have completed childbearing, and according to ACOG, should not be performed in any adolescent, regardless of disability status.
HYSTERECTOMY
Although a hysterectomy would result in complete amenorrhea and some parents and caregivers of children with disabilities may request it for menstrual management, it is a major surgical procedure with a 4-10% rate of complications and should only be offered for the same clinical indications as for patients without disabilities. Additionally, there are complex legal and ethical concerns with sterilization procedures and the legal consent process must follow sterilization laws, which vary by country.
Conclusion
Menstrual health includes a range of needs, from access to clean water and accessible facilities for proper hygiene, to medical treatment for conditions such as heavy bleeding. The onset of menstruation can be a challenging time for all adolescents, but globally, those with disabilities may experience additional burdens. Adolescents with disabilities may face hardships managing the social, cultural, and medical aspects of menstruation, which may be compounded by other challenges from medical conditions and inaccessible environments. Improved policies on menstrual health management, along with more robust menstrual health education worldwide, would greatly benefit this community.
Future research should include defining best practices for delivering accessible health and medical education for clinicians providing care for adolescents with physical, cognitive, and sensory disabilities. In addition, studies should be conducted to affirm which policies best improve communities’ access to clean water, reduce cost for menstrual supplies, and improve infrastructure for accessibility.
Conflict of Interest Statement: The authors have no conflicts of interest to declare.
Funding Statement: None.
Acknowledgements: The terms girls and women may be used in this article, though we acknowledge that individuals assigned female at birth may also identify as transgender or non-binary.
References:
- UNICEF. Guidance on Menstrual Health and Hygiene. 2019; https://www.unicef.org/media/91341/file/UNICEF-Guidance-menstrual-health-hygiene-2019.pdf. Accessed December 23, 2024.
- Sommer M, Caruso BA, Sahin M, et al. A Time for Global Action: Addressing Girls’ Menstrual Hygiene Management Needs in Schools. PLoS Med. 2016;13(2):e1001962.
- World Health Organization. New report highlights neglected health needs of children with developmental disabilities. https://www.who.int/news/item/15-09-2023-new-reports-highlights-neglected-health-needs-of-children-with-developmental-disabilities. Accessed June 2, 2024.
- UNICEF. Nearly 240 million children with comprehensive statistical analysis finds. 2021; www.unicef.org/press-releases/nearly-240-million-children-disabilities-around-world-unicefs-most-comprehensive. Accessed June 2, 2024.
- Dural O, Tas IS, Akhan SE. Management of Menstrual and Gynecologic Concerns in Girls with Special Needs. J Clin Res Pediatr Endocrinol. 2020;12(Suppl 1):41-45.
- O’Brien KE, Rosen MW, Ernst SD. Obstetric and Gynecologic Care for Individuals with Disabilities. Obstet Gynecol Clin North Am. 2024;51(1):43-56.
- Crimmins EM, Zhang Y, Saito Y. Trends Over 4 Decades in Disability-Free Life Expectancy in the United States. Am J Public Health. 2016;106(7):1287-1293.
- Centers for Disease Control and Prevention. Disability and Health Data System (DHDS). https://dhds.cdc.gov/SP. Accessed December 23, 2024.
- Streur CS, Schafer CL, Garcia VP, Quint EH, Sandberg DE, Wittmann DA. “If Everyone Else Is Having This Talk With Their Doctor, Why Am I Not Having This Talk With Mine?”: The Experiences of Sexuality and Sexual Health Education of Young Women With Spina Bifida. J Sex Med. 2019; 16(6):853-859.
- Leanage A, Burgess R, Ogrodnik M, Malik P. Sexual Health and Sexual Education for Women with Disabilities: Challenges & Opportunities. 2018; https://docs.wixstatic.com/ugd/b2d084_4b5e683f5921486f9a76a7a5bc4dad8b.pdf. Accessed December 23, 2024.
- World Health Organization. Promoting sexual and reproductive health for persons with disabilities: WHO/UNFPA guidance note. 2009; https://www.unfpa.org/sites/default/files/pub-pdf/srh_for_disabilities.pdf Accessed December 23, 2024.
- Gatti C, Del Rossi C, Ferrari A, Casolari E, Casadio G, Scire G. Predictors of successful sexual partnering of adults with spina bifida. J Urol. 2009;182(4 Suppl):1911-1916.
- Streur CS, Schafer CL, Garcia VP, et al. “He told me it would be extremely selfish of me to even consider [having kids]”: The importance of reproductive health to women with spina bifida and the lack of support from their providers. Disabil Health J. 2020;13(2):100815.
- Iezzoni LI, Wint AJ, Smeltzer SC, Ecker JL. “How did that happen?” Public responses to women with mobility disability during pregnancy. Disabil Health J. 2015;8(3):380-387.
- Gray SH, Byrne R, Christensen S, et al. Women with cerebral palsy: A qualitative study about their experiences with sexual and reproductive health education and services. J Pediatr Rehabil Med. 2021;14(2):285-293.
- Esmail S, Darry K, Walter A, Knupp H. Attitudes and perceptions towards disability and sexuality. Disabil Rehabil. 2010;32(14):1148-1155.
- Nosek MA, Howland C, Rintala DH, Young ME, Chanpong GF. National Study of Women with Physical Disabilities: Final Report. Sex Disabil. 2001;19(1):5-40.
- Casteel C, Martin SL, Smith JB, Gurka KK, Kupper LL. National study of physical and sexual assault among women with disabilities. Inj Prev. 2008;14(2):87-90.
- Basile KC, Breiding MJ, Smith SG. Disability and Risk of Recent Sexual Violence in the United States. Am J Public Health. 2016;106(5):928-933.
- Rowen TS, Stein S, Tepper M. Sexual health care for people with physical disabilities. J Sex Med. 2015;12(3):584-589.
- McRee AL, Haydon AA, Halpern CT. Reproductive health of young adults with physical disabilities in the U.S. Prev Med. 2010;51(6):502-504.
- Jones L, Bellis MA, Wood S, et al. Prevalence and risk of violence against children with disabilities: a systematic review and meta-analysis of observational studies. Lancet. 2012;380(9845):899-907.
- Boosey R, Prestwich G, Deave T. Menstrual hygiene management amongst schoolgirls in the Rukungiri district of Uganda and the impact on their education: a cross-sectional study. Pan Afr Med J. 2014;19:253.
- Garg S, Anand T. Menstruation related myths in India: strategies for combating it. J Family Med Prim Care. 2015;4(2):184-186.
- Mukherjee A, Lama M, Khakurel U, et al. Perception and practices of menstruation restrictions among urban adolescent girls and women in Nepal: a cross-sectional survey. Reprod Health. 2020;17(1):81.
- Alenizy H, Aleyeidi N, Almutairi R, et al. Assessment of the Readiness, Beliefs, and Practices Regarding Menstruation Among Women in Saudi Arabia. Int J Womens Health. 2024;16:1875-1887.
- Hennegan J, Shannon AK, Rubli J, Schwab KJ, Melendez-Torres GJ. Women’s and girls’ experiences of menstruation in low- and middle-income countries: A systematic review and qualitative metasynthesis. PLoS Med. 2019;16(5):e1002803.
- World Health Organization. Menstrual health is a fundamental human right. 2024; https://www.who.int/europe/news-room/15-08-2024-menstrual-health-is-a-fundamental-human-right. Accessed January 11, 2025.
- Smiles D, Short S, Sommer M. “I Didn’t Tell Anyone Because I Was Very Afraid”: Girls’ Experiences of Menstruation in Contemporary Ethiopia. Womens Reprod Health (Phila). 2017;4(3):185-197.
- The Lancet Child Adolescent Health. Normalising menstruation, empowering girls. Lancet Child Adolesc Health. 2018;2(6):379.
- Agaronnik N, Campbell EG, Ressalam J, Iezzoni LI. Communicating with Patients with Disability: Perspectives of Practicing Physicians. J Gen Intern Med. 2019;34(7):1139-1145.
- Iezzoni LI, Rao SR, Ressalam J, et al. Physicians’ Perceptions Of People With Disability And Their Health Care. Health Aff (Millwood). 2021;40(2):297-306.
- NASPAG Essentials of Pediatric and Adolescent Gynecology. Amsterdam: Elsevier Health Sciences; 2024.
- World Health Organization. World Report on Disability. 2011; https://www.who.int/publications/i/item/9789241564182. Accessed December 23, 2024.
- Kantartzis KL, Sucato GS. Menstrual suppression in the adolescent. J Pediatr Adolesc Gynecol. 2013;26(3):132-137.
- American College of Obstetricians Gynecologists’ Committee on Adolescent Health Care. Committee Opinion No. 668: Menstrual Manipulation for Adolescents With Physical and Developmental Disabilities. Obstet Gynecol. 2016;128(2):e20-25.
- Kirkham YA, Ornstein MP, Aggarwal A, McQuillan S. No. 313-Menstrual Suppression in Special Circumstances. J Obstet Gynaecol Can. 2019;41(2):e7-e17.
- Bradley LD, Gueye NA. The medical management of abnormal uterine bleeding in reproductive-aged women. Am J Obstet Gynecol. 2016;214(1):31-44.
- Bofill Rodriguez M, Lethaby A, Farquhar C. Non-steroidal anti-inflammatory drugs for heavy menstrual bleeding. Cochrane Database Syst Rev. 2019;9(9):CD000400.
- Lukes AS, Freeman EW, Van Drie D, Baker J, Adomako TL. Safety of tranexamic acid in women with heavy menstrual bleeding: an open-label extension study. Womens Health (Lond). 2011;7(5):591-598.
- Bonnar J, Sheppard BL. Treatment of menorrhagia during menstruation: randomised controlled trial of ethamsylate, mefenamic acid, and tranexamic acid. BMJ. 1996;313(7057):579-582.
- Leminen H, Hurskainen R. Tranexamic acid for the treatment of heavy menstrual bleeding: efficacy and safety. Int J Womens Health. 2012;4:413-421.
- Quint EH. Adolescents with Special Needs: Clinical Challenges in Reproductive Health Care. J Pediatr Adolesc Gynecol. 2016;29(1):2-6.
- Reddy DS. Clinical pharmacokinetic interactions between antiepileptic drugs and hormonal contraceptives. Expert Rev Clin Pharmacol. 2010;3(2):183-192.
- Wright JD, Herzog TJ, Tsui J, et al. Nationwide trends in the performance of inpatient hysterectomy in the United States. Obstet Gynecol. 2013;122(2 Pt 1):233-241.
- Wright KP, Johnson JV. Evaluation of extended and continuous use oral contraceptives. Ther Clin Risk Manag. 2008;4(5):905-911.
- de Bastos M, Stegeman BH, Rosendaal FR, et al. Combined oral contraceptives: venous thrombosis. Cochrane Database Syst Rev. 2014;2014(3):CD010813.
- Daunov M, Rondinelli J, Ahuja SP, Stehouwer NR. Prevalence of Venous Thromboembolism in Ambulatory and Non-Ambulatory Patients with Cerebral Palsy. Blood. 2019;134(Supplement 1):2428.
- Quint EH, O’Brien RF, Committee On A, North American Society for P, Adolescent G. Menstrual Management for Adolescents With Disabilities. Pediatrics. 2016;138(1).
- Fei YF, Ernst SD, Dendrinos ML, Quint EH. Satisfaction With Hormonal Treatment for Menstrual Suppression in Adolescents and Young Women With Disabilities. J Adolesc Health. 2021;69(3):482-488.
- Watson KC, Lentz MJ, Cain KC. Associations between fracture incidence and use of depot medroxyprogesterone acetate and anti-epileptic drugs in women with developmental disabilities. Womens Health Issues. 2006;16(6):346-352.
- Fan D, Miao J, Fan X, Wang Q, Sun M. Effects of valproic acid on bone mineral density and bone metabolism: A meta-analysis. Seizure. 2019;73:56-63.
- Dussault PM, Lazzari AA. Epilepsy and osteoporosis risk. Curr Opin Endocrinol Diabetes Obes. 2017;24(6):395-401.
- Verrotti A, Di Corcia G, Morgese G, Trotta D, Chiarelli F. Epilepsy and adolescents. Panminerva Med. 2003;45(4):231-240.
- Ali M, Akin A, Bahamondes L, et al. Extended use up to 5 years of the etonogestrel-releasing subdermal contraceptive implant: comparison to levonorgestrel-releasing subdermal implant. Hum Reprod. 2016;31(11):2491-2498.
- McNicholas C, Swor E, Wan L, Peipert JF. Prolonged use of the etonogestrel implant and levonorgestrel intrauterine device: 2 years beyond Food and Drug Administration-approved duration. Am J Obstet Gynecol. 2017;216(6):586 e581-586 e586.
- Deokar AM, Jackson W, Omar HA. Menstrual bleeding patterns in adolescents using etonogestrel (ENG) implant. Int J Adolesc Med Health. 2011;23(1):75-77.
- Berlan E, Mizraji K, Bonny AE. Twelve-month discontinuation of etonogestrel implant in an outpatient pediatric setting. Contraception. 2016;94(1):81-86.
- McNicholas C, Maddipati R, Zhao Q, Swor E, Peipert JF. Use of the etonogestrel implant and levonorgestrel intrauterine device beyond the U.S. Food and Drug Administration-approved duration. Obstet Gynecol. 2015;125(3):599-604.
- Schwartz BI, Alexander M, Breech LL. Intrauterine Device Use in Adolescents With Disabilities. Pediatrics. 2020;146(2).
- Hillard PJ. Menstrual suppression with the levonorgestrel intrauterine system in girls with developmental delay. J Pediatr Adolesc Gynecol. 2012;25(5):308-313.
- Pillai M, O’Brien K, Hill E. The levonorgestrel intrauterine system (Mirena) for the treatment of menstrual problems in adolescents with medical disorders, or physical or learning disabilities. BJOG. 2010;117(2):216-221.
- Savasi I, Jayasinghe K, Moore P, Jayasinghe Y, Grover SR. Complication rates associated with levonorgestrel intrauterine system use in adolescents with developmental disabilities. J Pediatr Adolesc Gynecol. 2014;27(1):25-28.
- Settnes A, Moeller C, Topsoee MF, et al. Complications after benign hysterectomy, according to procedure: a population-based prospective cohort study from the Danish hysterectomy database, 2004-2015. BJOG. 2020;127(10):1269-1279.