






Mid-Term Results of Lower Trapezius Tendon Transfer
Arthroscopic-assisted lower trapezius tendon transfer for posterosuperior irreparable massive rotator cuff tears: Mid-term results
Santiago Ordoñez¹, Santiago Vanegas², Carlos Afanador³, Oscar Alejandro Mejía⁴, Juan Carlos Jaramillo¹⁰, Victor Alfonso Avendaño⁵, Ana Milena Herrera⁶*
- Orthopaedic surgeon. Shoulder and elbow orthopedics. Clínica del Campestre and Hospital Pablo Tobón Uribe. Medellín, Colombia.
- Orthopaedic surgeon. Shoulder and elbow fellow. Universidad Pontificia Bolivariana. Centro de Ortopedia el Poblado and Clínica Las Américas AUNA. Medellín, Colombia.
- Orthopaedic surgeon. Shoulder and elbow orthopedics. Clínica del Campestre and Clínica Universitaria Bolivariana. Medellín, Colombia.
- Orthopaedic surgeon. Shoulder and elbow orthopedics. Clínica Universitaria Bolivariana. Medellín, Colombia.
- Orthopaedic resident. Universidad Pontificia Bolivariana. Medellín, Colombia.
- Epidemiology Unit, Clínica del Campestre, Medellín, Colombia.
ABSTRACT
Background:
Massive and irreparable rotator cuff tears (MIRCTs) cause destabilization of the glenohumeral joint by altering the anteroposterior force coupling, compromising the shoulder function, especially at the expense of the active external rotation and significant pain. Among the therapeutic alternatives, lower trapezius transfer has shown promising results in the short term, with only a few studies providing evidence of the lasting integrity of the repair.
Aims:
The purpose of this study was to describe the mid-term clinical, radiologic, and patient-reported outcomes of lower trapezius transfer in patients with MIRCTs.
Methods:
This was a prospective longitudinal study of patients with MIRCT with more than six months of symptoms with no response to conservative management and treated with lower trapezius transfer in three specialized centers between 2018 and 2022. Data about the range of movement, imaging studies, functional assessment through the American Shoulder and Elbow Surgeons score, and pain level evaluation through a visual analog scale was collected during follow-ups at 12, 24, 48, and 60 months. Descriptive and comparative analyses of before and after surgery outcomes are presented.
Results:
Fifteen patients were included in the series, with a median age of 59 years and 66.7% males. At 48 and 60 months postoperatively, patients who were assessed presented significant improvement in the range of movement, American Shoulder and Elbow Surgeons score, and pain level concerning the presurgical parameters. There was no retearing, and only one patient presented a 20% progression of glenohumeral arthrosis at about 30 months postoperatively.
Conclusion:
Lower trapezius transfer in patients with MIRCTs showed satisfactory clinical, radiologic, and functional outcomes in the mid-term, with no retearing and very low progression of degenerative changes. These results provide evidence of the lasting effects of lower trapezius transfer in treating MIRCTs.
Keywords:
Rotator Cuff Injuries; Arthroscopy; Muscle, Trapezius; Tendon Transfer; Functional Status.
Introduction
Massive and irreparable rotator cuff tears (MIRCTs) are complex and difficult-to-manage injuries that comprise about 10 to 40% of all rotator cuff tears¹.
MIRCTs have different definitions, according to Zumstein et al.², two or more tendons must be torn entirely²’³, while Cofield et al.⁴ determined that the total tear diameter must be ≥ 5 cm in either the anterior-posterior or medial-lateral dimension⁵’⁶.
Other authors considered that in a MIRCT, the percentage of the exposed humeral head had to be ≥ 67% in the sagittal plane⁷, and there is the impossibility of advancing the tendon stump to the footprint and performing a tension-free repair⁸’⁹.
The posterosuperior MIRCTs involve tearing of the supraspinatus and infraspinatus, and of the teres minor, type D and E, respectively, according to Collin et al.¹⁰ classification, which causes significant pain and compromise of the abduction and external rotation movements of the shoulder¹⁰ secondary to the consequent dynamic destabilization of the glenohumeral joint⁸’⁹’¹¹.
In addition to clinical evaluation, imaging studies are essential for diagnosis and therapeutic approaches considering variables such as acromiohumeral distance, atrophy, and fatty infiltration¹.
The therapeutic alternatives for posterosuperior MIRCTs aim at restoring the horizontal force couple with options that range from pain-relieving procedures such as simple debridement and subacromial decompression¹²–¹⁵; cuff biomechanics restoration performing partial repair and margin convergence sutures¹⁶’¹⁷; anatomical restoration and stabilization of the humeral head superior translation through a superior capsule reconstruction or complete repair with scaffolds or tissue augmentation¹⁸–²¹; and to anterior-posterior force couple rebalancing with tendon transfers (TT)²²–²⁴.
The adequate management option for each patient will depend on the severity of the tear and functional compromise, as well as the expectations according to the functional demands¹.
TT is an attractive surgical option for young and driven patients with MIRCTs in which considerable fatty infiltration according to the Goutallier classification and small degenerative glenohumeral changes according to the radiological Hamada classification are present²⁵. The arthroscopic-assisted latissimus dorsi transfer (LDT) has been considered a favorable alternative for posterosuperior MIRCTs treatment as it replaces the posterior component for dynamic balance of the anterior-posterior force couple of the glenohumeral joint²⁶–²⁸.
The LDT acts as a stabilizer of the humeral head translation, contributing to the abduction and external rotation of the shoulder and improving the pain, showing satisfactory mid and long-term results²³.
Lower trapezius transfer (LTT) is another promising TT option considered for posterosuperior MIRCTs treatment²⁴.
Recent biomechanical studies have shown that LTT is more advantageous for increasing external rotation (ER), and overall glenohumeral joint stabilization²⁹’³⁰.
The clinical outcomes using LTT reported up to date for posterosuperior MIRCTs are encouraging²⁴.
However, few studies have reported mid-term follow-up beyond four years in which it is shown that the clinical results are maintained and there is no progression of osteoarthritis over time³¹–³³.
The purpose of this study was to describe the mid-term clinical, radiologic, and patient-reported outcomes of LTT in patients with MIRCTs.
Methods
PATIENTS AND FOLLOW-UPS
After institutional review board approval, a prospective observational study of adult patients with posterosuperior irreparable massive rotator cuff tears surgically treated with arthroscopic-assisted lower trapezius tendon transfer was carried out.
The surgeries took place in three specialized centers between 2018 and 2022.
The patients were intervened with this technique if the
MIRCT had more than six months of symptoms with no response to conservative treatment, no concomitant irreparable subscapularis tears, and grade ≥ 3 of the supraspinatus or infraspinatus muscle fatty infiltration according to the Goutallier classification³⁴. Patients were excluded if they were > 65 years, had less than 12 months postoperative, and presented one of the following: pseudoparalysis, radiological Hamada classification grade > 3, adhesive capsulitis or passive joint motion restriction, neurologic deficits axillary nerve, deltoid dysfunction.
Collected demographic and basal data included age, sex, involvement in physical activities, duration of symptoms, comorbidities, and previous surgical history on the affected shoulder. Radiographic data consisted of the extent of the subscapular lesion, Hamada and Goutallier classifications, supraspinatus and teres minor atrophy, Patte classification, and acromiohumeral distance.
Preoperative and postoperative clinical, radiological, and patient-reported outcomes (PRO) included assessment of the affected and contralateral shoulders’ range of movement (ROM), imaging studies (radiographs or magnetic resonance), functional assessment through the American Shoulder and Elbow Surgeons (ASES) score, and pain level evaluation through a visual analog scale (VAS). Patients were followed up according to the author’s clinical protocol at 3 and 6 months and every year up to 5 years. Here, we report data on 12, 24, 48 and 60 months (POP1 to POP4). The return to physical activities after the sixth month was also inquired about.
Surgical Technique and Rehabilitation Protocol
The surgical technique, according to the description by Elhassan et al.³²’³⁵, is a procedure in which the lower trapezius tendon is harvested using an open approach and then arthroscopically transferred to the greater tuberosity using an intercalary allograft.
For the tendon harvest, the patient is placed in a lateral decubitus position, and skin markings are made over the medial and superior border of the scapula.Figure 1. Patient position and markings.

The patient is in a lateral decubitus position with skin markings on the scapular spine and the medial and lateral borders of the scapula. The transverse skin incision is 2 cm inferior and parallel to the medial half of the spine of the scapula. The directions of the lower trapezius muscle fibers are also drawn.
A triangular fat pad covering the tendon is identified and resected. The inferior edge of the lower trapezius is lifted and bluntly dissected; it is followed laterally to its insertion on the inferior and dorsal aspect of the spine of the scapula. The lower trapezius tendon is detached from the periosteum in a lateral to medial direction and secured with two rows of nonabsorbable sutures in a Krakow configuration, avoiding the neurovascular pedicle in proximity (Figure 2).
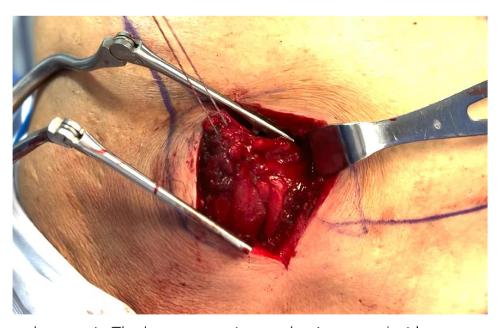
Figure 2. Lower trapezius tendon repair.
The lower trapezius tendon is secured with two rows of nonabsorbable sutures in a Krakow configuration.The spinal accessory nerve lies within the fascial layer underneath the trapezius tendon, approximately 2 cm medial to the medial border of the scapula; deep dissection should be avoided.Then, the Achilles tendon allograft is prepared using two non-absorbable sutures in a Krakow configuration in the narrower portion. We use a marker to identify the side of the allograft facing superiorly (Figure 3).
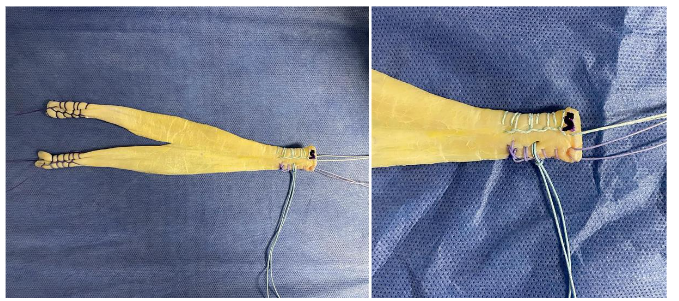
Figure 3. Tendon allograft preparation.
Achilles tendon allograft with two non-absorbable sutures in the narrower portion that will be repaired to the greater tuberosity. The posterior, posterolateral, anterior, and lateral arthroscopic portals are made for the arthroscopic transfer. According to the findings, the subscapularis muscle is repaired, and extensive bursectomy is performed. The footprint is prepared using a shaver in the greater tuberosity (Figure 4).
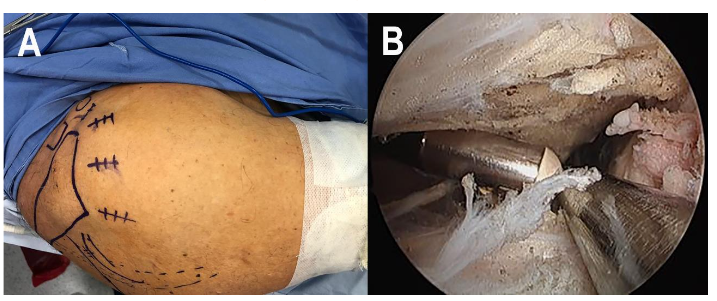
Figure 4. Arthroscopy portals and bursectomy. A. The posterior, posterolateral, anterior, and lateral arthroscopic portals are marked. B. An extensive bursectomy is made, and the footprint is prepared.
Next, through the open approach, the infraspinatus fascia is identified and open to communicate the subacromial space with the lower trapezius harvest site. The sutures placed at the narrower end of the graft are passed through the infraspinatus using a long grasper or a Bozeman clamp inserted through the anterior or lateral arthroscopic portal.
Then, the graft is fixed into the greater tuberosity using the sutures of the graft into three knotless anchors in the anteromedial, anterolateral, and posterolateral portion of the greater tuberosity while keeping tension in the graft, covering most of the greater tuberosity area (Figure 5).
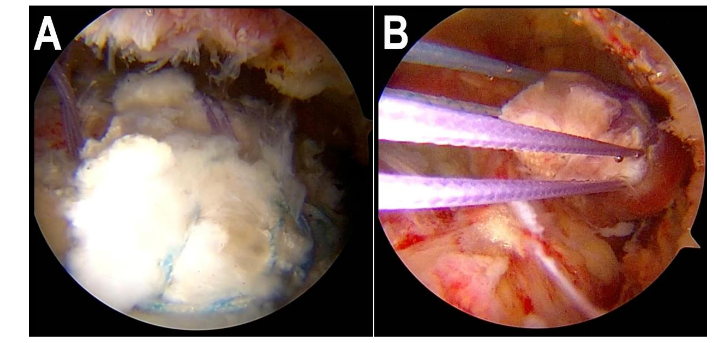
Figure 5. Arthroscopic-assisted tendon transfer. A. Fixation of the graft using knotless anchors. B. The final view is through a lateral portal after the allograft fixation has ended.
When possible, the residual rotator cuff is repaired to the graft using side-to-side stitches.
Finally, in the open approach, the graft is repaired to the lower trapezius. With the arm in maximal abduction and external rotation, the graft is secured to the lower trapezius in a Pulvertaft fashion, and multiple stitches are added to complete the repair using non-absorbable sutures (Figure 6).
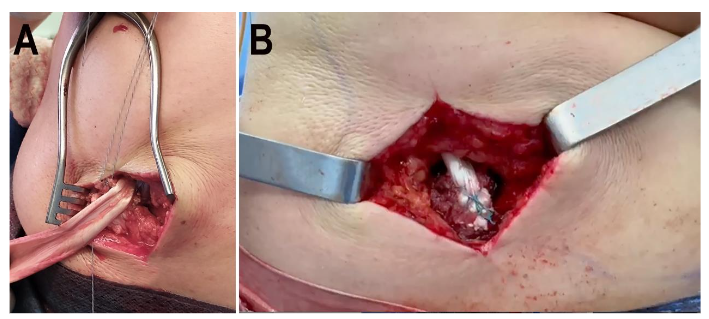
Figure 6. Graft repairing and securing. A. Allograft is secured to the lower trapezius tendon using a Pulvertaft. B. Final repair after cutting the residual allograft.
The rehabilitation protocol consists of shoulder joint immobilization in 40° – 60° of external rotation, with elbow, wrist, and finger mobilization for the first six to eight weeks. Afterward, passive and active assisted mobility arcs are permitted for six weeks, progressing to active movements with restriction to internal rotation. Between 12 and 16 weeks of POP, gradual active internal rotation is initiated with a slow return to normal daily activities. In week 16, patients start progressive strengthening by completing unrestricted activities by the 6th month. After six months of the procedure, the patients return to normal activities without restrictions.
STATISTICAL ANALYSIS
Statistical descriptive analysis of all measurements was conducted using SPSS statistical software (version 25.0; IBM Corp, Armonk, NY, USA). Sample distribution was assessed through a Shapiro-Wilk test. The continuous variables are presented as median and range of minimum and maximum. Categorical parameters are presented as absolute and relative frequencies. The clinical variables evolution throughout follow-ups in the affected shoulder are plotted against the contralateral shoulder and expressed as a percentage. A one-way ANOVA test was used to evaluate the changes in the parameters in each follow-up. Stratified analysis was performed to assess the influence of independent variables such as sex, age groups, and preoperative Hamada classification on the changes in the clinical variables. A p-value < 0.05 was set for statistical significance.
Results
The study included fifteen (n = 15) patients, with a median age of 59 and 66.7% males. Table 1 summarizes the demographic and presurgical characteristics.
Table 1. Demographic and presurgical characteristics
| Median | Frequency (%) | |
|---|---|---|
| Age (years) | 59 (40–64) | |
| < 60 years | 9 (60) | |
| ≥ 60 years | 6 (40) | |
| Sex | ||
| Male | 10 (66.7) | |
| Female | 5 (33.3) | |
| Affected shoulder | ||
| Right | 9 (60) |
| Median | Frequency (%) | |
|---|---|---|
| Left | 6 (40) | |
| Dominant side affected | 9 (60) | |
| Physical activity | 7 (46.7) | |
| Times per week (n = 7) | 2 (1–3) | |
| Symptoms duration (months) | 12 (6–18) | |
| Comorbidities | ||
| Parkinson disease | 1 (6.7) | |
| Hypertension | 1 (6.7) | |
| Previous surgeries in the affected shoulder | ||
| Rotator cuff repair | 4 (26.7) | |
| Greater tuberosity osteosynthesis | 1 (6.7) | |
| Imaging findings | ||
| Repairable subscapularis tear | ||
| Upper 1/3 of the tendon | 5 (33.3) | |
| Upper 2/3 of the tendon | 4 (26.7) | |
| No subscapularis lesion | 6 (40) | |
| Hamada classification | ||
| Grade 1 | 6 (40) | |
| Grade 2 | 8 (53.3) | |
| Grade 3 | 1 (6.7) | |
| Goutallier classification (Supraspinatus) | ||
| Stage 2 | 1 (6.7) | |
| Stage 3 | 12 (80) | |
| Stage 4 | 2 (13.3) | |
| Infraspinatus | ||
| Stage 2 | 1 (6.7) | |
| Stage 3 | 9 (60) | |
| Stage 4 | 5 (33.3) | |
| Supraspinatus atrophy | ||
| Grade 1 | 2 (13.3) | |
| Grade 2 | 7 (46.7) | |
| Grade 3 | 6 (40) | |
| Patte classification | ||
| Stage 1 | 1 (6.7) | |
| Stage 2 | 5 (33.3) | |
| Stage 3 | 9 (60) | |
| Teres minor atrophy | 1 (6.7) | |
| Acromiohumeral distance (mm) | 7 (5–10) |
Follow-up Description
All patients completed the required follow-up according to the date of surgery. As such, all fifteen (n = 15) patients were eligible for the first-year follow-up, fourteen (n = 14) for two years, ten (n = 10) for a four-year follow-up, and lastly, four (n = 4) patients for a postoperative evaluation at five years.
Clinical parameters such as ROM and PRO, as well as pain level and ASES score, showed significant changes from the preoperative values at all follow-ups. However, after 12 months of POP, all parameters stabilized and did not change significantly from the previous evaluation (Table 2).
Table 2. Clinical postoperative evolution
| PreOP | POP1 (n=15) | POP2 (n=14) | POP3 (n=10) | POP4 (n=4) | P-value | |
|---|---|---|---|---|---|---|
| POP time (months) | — | 12 (11–15) | 24.5 (24–28) | 48.5 (47–50) | 59 (55–65) | — |
| VAS | 8 (6–9) | 1 (0–5) | 1 (0–7) | 1 (0–7) | 0 (0–3) | 0.000* |
| ASES | 48 (40–52) | 85 (78–90) | 84.5 (70–90) | 86 (84–92) | 91 (84–95) | 0.000* |
| %ASESᵃ | 50 (42.9–57.8) | 88 (78–112) | 88.2 (77.8–112) | 90.1 (85–112) | 96.4 (88.4–102.2) | — |
| Anterior flexion | 110 (80–130) | 150 (120–160) | 150 (130–160) | 150 (130–160) | 155 (130–160) | 0.000* |
| %Anterior flexionᵃ | 75 (53.3–86.7) | 93.75 (80–100) | 100 (81.25–100) | 100 (81.25–100) | 96.9 (81.25–100) | — |
| Abduction | 100 (70–120) | 140 (120–160) | 140 (120–160) | 140 (120–150) | 140 (120–160) | 0.000* |
| %Abductionᵃ | 69.2 (46.7–92.3) | 100 (81.25–116.7) | 100 (81.25–116.7) | 100 (81.25–116.7) | 96.15 (86.7–100) | — |
| External rotation | 20 (15–40) | 45 (35–60) | 45 (35–60) | 45 (35–50) | 45 (40–45) | 0.000* |
| %External rotationᵃ | 41.7 (25–66.7) | 85.7 (66.7–100) | 86.6 (66.7–100) | 81.25 (66.7–100) | 87.5 (66.7–100) | — |
POP: Postoperative
All values expressed as median (range)
ᵃAffected shoulder concerning the contralateral shoulder
Statistically significant values of presurgical assessment compared with the last registered follow-up.
Clinical summary under the table
The POP values of ASES scores and ROM showed a gradual improvement, reaching almost the values of the contralateral shoulder, which stabilized after a year of follow-up. The ASES score and shoulder anterior flexion showed a non-significant increase at the fourth follow-up compared to the third (Figure 4).
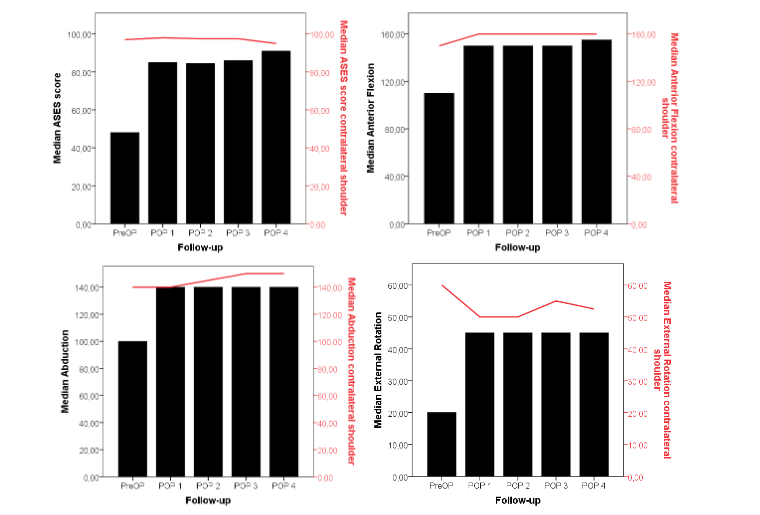
The functional score (ASES) and ROM of the affected shoulder were plotted against the contralateral shoulder through all follow-ups. A significant and steady recovery of all parameters after the procedure can be observed.
Arthroscopic lower trapezius tendon transfer
Seven patients (n = 7) preoperatively referred to involvement in any physical activity; of those, four (n = 4) had returned to activities by 12 months POP. Of the three remaining, two (n = 2) were eligible for follow-ups beyond a year POP; both had returned to activities by 48 months POP.
Variables such as sex, age group (< 60 years and ≥ 60 years), and the presurgical Hamada classification did not influence the significant changes in pain level, ASES scores, and ROM in each follow-up (p > 0.05) (Figure 5).
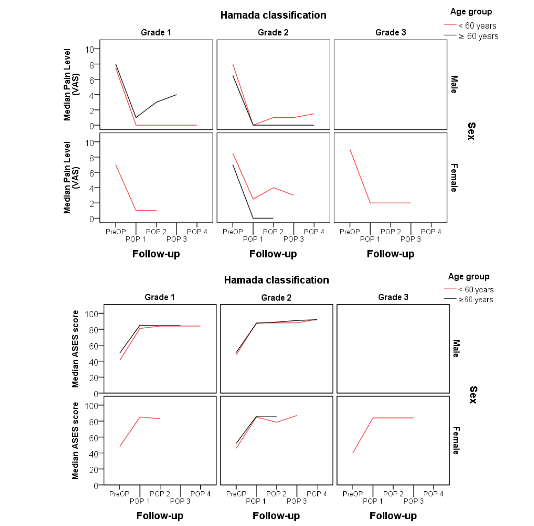
Figure 5. Pain level and ASES evolution through follow-ups according to age groups, sex, and presurgical Hamada classification.
No significant difference was detected in pain level and functional scores between males and females, age groups, or Hamada grade.
In imaging studies, the assessed patients presented graft integrity at the last reported follow-up. The Hamada classification remained in six (n = 6) patients with grade 1 and seven (n = 7) with grade 2; only one patient showed 20% progression of glenohumeral arthrosis from Hamada grade 2 to Hamada grade 3 at 31 months POP. One patient with preoperative Hamada grade 3 showed no degenerative progression after 60 months of POP. No complications related to the procedure or revision surgeries occurred during the study period.
Discussion
Lower trapezius transfer surgical technique has been proposed as a favorable alternative for posterosuperior MIRCTs treatment with tendon transfer, but only a few reports have shown outcomes after four years of POP³¹–³³. The results of this study add up to the body of evidence showing that in patients evaluated after 48 months of the procedure, the clinical and functional outcomes were sustained, and no progression of
Osteoarthritis was observed. Additionally, no complications or retears occurred in this series. Posterosuperior MIRCT treatment represents a challenge given the variability in outcomes with uncertain durability, high rates of retear, and the consequent degenerative changes of the shoulder joint.¹²⁵ The current findings’ importance lies in the constant and satisfactory clinical and functional outcomes that persisted over time, the absence of retearing, and the very low progression of degenerative changes in the mid-term.
Tendon transfers, nowadays a widely used treatment method for posterosuperior MIRCTs, restore shoulder functions and relieve symptoms by rebalancing the anterior–posterior force couple.²²–²⁴ These procedures seek to reinstate the shoulder joint mechanics to stop the course of degenerative changes secondary to the eccentric forces occurring in the glenohumeral joint due to the alteration of the coupled pair forces.²⁵˒²⁶ Candidates for TT are young and motivated patients with considerable impaired function at the expense of loss of external rotation but without or with low-grade glenohumeral arthritis.¹²⁵ The selection of a TT as the surgical option for a MIRCT treatment must follow the postulates that the tendons, recipient and transferred, have similar lines of pull and musculotendinous excursion and that the transferred tendon has a strength grade ≥4, its function is nonessential, will not have a negative impact on the donor site, and it substitutes one function of the recipient.³⁶
In the literature, the most used and described TT alternatives for MIRCT surgical repair are the LDT and LTT.¹²⁵ The Latissimus Dorsi transfer was first described as an open technique by Gerber et al.³⁷; since then, many authors have reported long-term consistent and satisfactory results with arthroscopically assisted LDT in terms of significantly improved ROM and functional outcomes, with a low rate of complications.³⁸–⁴⁰ Nonetheless, in the mid- and long-term, close to 50% of the patients showed progression of osteoarthritis in a high-demand independent series.²⁶
Hamada grading, mainly in the presence of teres minor atrophy and fatty degeneration, and in 4 to 13% of the patients a conversion to reverse shoulder arthroplasty (RSA) was necessary.³⁸˒⁴⁰˒⁴¹ On the other hand, the Lower Trapezius transfer is a procedure described initially by Elhassan et al.⁴², who used an open approach for the paralytic shoulder, but in recent years, the arthroscopically assisted procedure has arisen as an alternative treatment in patients with MIRCT, especially in those with a lag of external rotation who seek strength recovery.⁴³–⁴⁵ In the setting of a MIRCT, the LTT has shown short-term significant improvements in ROM, especially external rotation, pain relief, and functional recovery.²⁴˒³³˒⁴⁴˒⁴⁶ Reteaaring and revision surgery with conversion to RSA in some instances was reported in about 4 to 12% and 10%, respectively.³²˒⁴⁶
The choice of LDT or LTT is based on surgeon preference and the patient’s age, activity level, and expectations⁴⁶, as no clinical superiority of these techniques has been established in a comparative randomized trial.³⁶ The LTT has gained attention as a more anatomic alternative; despite not being inherent to the glenohumeral joint, its line of pull runs parallel to the infraspinatus tendon, synergistically exerting scapular retraction and shoulder external rotation, easing the recovery process by reducing the requirement for exhaustive retraining.²⁹˒⁴⁷–⁴⁹ An observational retrospective clinical study comparing short-term outcomes of LDT versus LTT at two years of follow-up performed by Baek et al.⁵⁰ showed that both techniques significantly improved overall ROM, function, and pain, with the recovery of ER and functional scores better with LTT. Additionally, there was a significantly higher rate of progression of arthritis in the LDT patients.⁵⁰
A recent cost comparison of treatment options for MIRCT by Marigi et al.⁵¹ demonstrated that compared to superior capsular reconstruction and RSA, LTT is a competitive alternative considering costs incurred up to 3 months postoperatively.⁵¹Anatomically and biomechanically, the LTT procedure offers some advantages over the LDT.⁴⁷
The trapezius muscle comprises three segments: upper, middle, and lower; the lower portion of the muscle is inserted on the spine of the scapula and medial acromion.⁵² When detached and transferred, the lines of pull of the lower trapezius tendon offer the advantage of mimicking the vector of the infraspinatus tendon, making it more anatomical than any other TT.¹¹ Furthermore, in the native shoulder, the lower trapezius muscle functions on elevation, abduction, and external rotation, having better moment arms in the latter two movements compared to the latissimus dorsi tendon, which is activated during adduction and internal rotation.²²˒²⁹˒⁴⁸ Clouette et al.²⁴ systematically analyzed several comparative biomechanical studies of LTT versus LDT, finding that, in general, the LTT displays superiority in the moment arms during ER mostly when transferred to the site of insertion of the infraspinatus, emulating closely the strength of an intact cuff during ER and abduction.²⁴ More recently, in a cadaveric study, Clouette et al.²⁶ demonstrated that even though both LDT and LTT significantly increased the maximum abduction angle, producing low superior humeral head migration, LTT was more efficient in restoring the native glenohumeral kinematics.³⁰ One disadvantage, however, could be the requirement of a graft for the LTT procedure. Herzberg et al.⁵³ found that the lower trapezius has a relatively short excursion (14.8 cm) and very low relative tension (2.7%) compared to the large potential excursion (33.9 cm) and low relative tension (5.9%) of the LDT, which represents the need for augmentation with a graft when performing an LTT to treat a MIRCT.⁵³ Nonetheless, the LTT surgical technique is technically easier to perform when compared to that of the LDT; the harvesting of tendon autografts or the use of tendon allografts according to the available resources and intended total tendon length for bridging of the lower trapezius tendon does not add technical difficulty to the procedure.²⁴˒⁵³
Despite the biomechanical advantages and good clinical outcomes in the short-term of the LTT in the setting of a MIRCT, only a few studies have addressed the question about the mid and long-term durability of the procedure and progression of degenerative changes.³¹–³³ Elhassan et al.³² reported outcomes on 33 patients with a range of follow-up of 24 to 73 months. Although the authors do not declare how many patients were followed for more than 48 months, the results of the whole series indicated a significant improvement in the shoulder ROM and functional score maintained up to the last follow-up. Additionally, during the last radiographic assessment, no signs of progressive arthritis were observed.³² Marigi et al. performed a comparison of arthroscopic superior capsular reconstruction versus arthroscopy-assisted LTT with a mean follow-up of 3.1 ± 1.4 years in the latter group. Like in the study by Elhassan et al.³², there is no clarity on how many of the 72 LTT patients were followed beyond four years; the results showed significant improvement in ROM, especially ER and strength recovery, with a survivorship of 89.9% at 4 years.³³ In contrast, the study by Baek et al.³¹ exclusively reported mid-term outcomes of LTT performed in 36 patients with follow-ups ranging from 48 to 70 months. The authors showed that compared to the preoperative parameters, during the final follow-up, there was still a significant improvement in the active ROM and functional scores, showing that clinically, the results are maintained in time and favoring the LTT as an effective treatment for MIRCT. The authors observed parameters indicating progression in arthritis, such as a significant decrease in the acromiohumeral distance and an increase in the Hamada grade; however, those significant changes occurred at the expense of three patients who presented retearing or infection; the remaining 33 patients did not have degenerative progression.³¹˒⁵
In our series of 15 patients, ten and four patients were followed up for about 48 and 60 months, respectively. Like the findings of Baek et al.³¹, in our patients, the significant improvement of ROM, pain level, and functional scores was sustained over time; in fact, the parameters significantly changed
during the first year of POP, reaching the functional level of the contralateral shoulder and remaining stable up to the last follow-up. Our series had no complications, revision surgeries, or conversion to RSA. Only two patients presented Hamada grade 3; one patient showed progression in arthritis around the third year POP, and the other one did not progress after five years but remained with the same preoperative degenerative signs. We did not find relationships between age, sex, or preoperative Hamada grading with the mid-term outcomes.
It has been suggested that an ideal age for TT is less than 60 years⁵⁵, however, we did not observe any difference in outcomes between patients < 60 years and those ≥ 60 years. This could be due to the careful selection of patients for the LTT, complying with all eligibility criteria. Nonetheless, in some exceptional cases, all the eligibility criteria might not be met. For instance, one patient in our series presented grade 3 fatty infiltration and reabsorption of the greater tuberosity after a proximal humerus fracture; kinematically and functionally, it emulated an irreparable massive tear of the rotator cuff. Clinically and radiologically, this patient had no different outcomes from the rest.
The findings of this study should be analyzed considering some important limitations. In the first place, the study is observational and lacks a control or comparison group; then, no conclusions about the effectiveness of LTT can be drawn, nor can associations with covariables be determined. Second, the sample size is small and not powered to undoubtedly conclude that the observed significant changes are not due to chance. Additionally, only a fraction of the patients were followed up for over 60 months. Nevertheless, the findings contribute to the body of evidence about the durability of the surgical repair of MIRCT with LTT showing graft integrity and preserved function beyond 48 months POP. Whether the LTT long-term outcomes are still favorable in patients with moderate degenerative changes (Hamada > 3) remains to be demonstrated.
Conclusion
Lower trapezius transfer in patients with MIRCTs showed satisfactory clinical, radiologic, and functional outcomes in the mid-term, with no retearing and very low progression of degenerative changes. These results provide evidence of the lasting effects of the LTT in treating MIRCTs.
Conflict of Interest
The authors have no conflicts of interest to declare.
Funding Statement
None.
Acknowledgements
None.
ORCID ID
Santiago Ordoñez: 0000-0001-5659-1469
Email: [email protected]
Santiago Vanegas: 0000-0003-0244-8960
Email: [email protected]
Carlos Afanador: 0000-0002-2229-4834
Email: [email protected]
Oscar Alejandro Mejía: 0000-0001-8107-288X
Email: [email protected]
Juan Carlos Jaramillo: 0009-0008-1910-6952
Email: [email protected]
Victor Alfonso Avendaño: 0000-0002-2976-3269
Email: [email protected]
Ana Milena Herrera: 0000-0002-7382-5631
Email: [email protected]
References
1. Bedi A, Dines J, Warren RF, Dines DM. Massive tears of the rotator cuff. Journal of Bone and Joint Surgery. 2010;92(9):1894-1908. doi:10.2106/JBJS. I.01531
2. Zumstein MA, Jost B, Hempel J, Hodler J, Gerber C. The Clinical and Structural Long-Term Results of Open Repair of Massive Tears of the Rotator Cuff. The Journal of Bone and Joint Surgery-American Volume. 2008;90(11):2423-2431. doi:10.2106/JBJS.G.00677
3. GERBER C, FUCHS B, HODLER J. The Results of Repair of Massive Tears of the Rotator Cuff*†. The Journal of Bone and Joint Surgery-American Volume. 2000;82(4):505-515. doi:10.2106/000046 23-200004000-00006
4. Cofield RH, Parvizi J, Hoffmeyer PJ, Lanzer WL, Ilstrup DM, Rowland CM. Surgical Repair of Chronic Rotator Cuff Tears. The Journal of Bone and Joint Surgery-American Volume. 2001;83(1) :71-77. doi:10.2106/00004623-200101000-00010
5. Cofield RH. Subscapular muscle transposition for repair of chronic rotator cuff tears. Surg Gynecol Obstet. 1982;154(5):667-672.
6. DeOrio JK, Cofield RH. Results of a second attempt at surgical repair of a failed initial rotator-cuff repair. J Bone Joint Surg Am. 1984;66(4):563-567.
7. Schumaier A, Kovacevic D, Schmidt C, et al. Defining massive rotator cuff tears: a Delphi consensus study. J Shoulder Elbow Surg. 2020;29(4):674-680. doi:10.1016/j.jse.2019.10.024
8. Sheth MM, Shah AA. Massive and Irreparable Rotator Cuff Tears: A Review of Current Definitions and Concepts. Orthop J Sports Med. 2023;11(5). doi:10.1177/23259671231154452
9. Burkhart SS. Arthroscopic treatment of massive rotator cuff tears. Clinical results and biomechanical rationale. Clin Orthop Relat Res. 1991;(267):45-56.
10. Collin P, Matsumura N, Lädermann A, Denard PJ, Walch G. Relationship between massive chronic rotator cuff tear pattern and loss of active shoulder range of motion. J Shoulder Elbow Surg. 2014;23 (8):1195-1202. doi:10.1016/j.jse.2013.11.019
11. Wagner ER, Elhassan BT. Surgical Management of Massive Irreparable Posterosuperior Rotator Cuff Tears: Arthroscopic-Assisted Lower Trapezius Transfer. Curr Rev Musculoskelet Med. 2020;13(5): 592-604. doi:10.1007/s12178-020-09657-5
12. Srikumaran U, Roden C, Rogusky E, Lapner P, Abboud J, Verma N. Subacromial Balloon Spacer versus Partial Repair for Massive Rotator Cuff Tears: A Prospective, Randomized, Multi-center Trial. Orthop J Sports Med. 2021;9(7_suppl4):2325967 121S0024. doi:10.1177/2325967121S00244
13. Soderlund M, Boren M, O’Reilly A, San Juan A, Mahylis JM. Arthroscopic debridement for management of massive, irreparable rotator cuff tears: a systematic review of outcomes. JSES Reviews, Reports, and Techniques. 2022;2(1):1-7. doi:10.1016/j.xrrt.2021.08.012
14. Montgomery TJ, Yerger B, Savoie FH. Management of rotator cuff tears: A comparison of arthroscopic debridement and surgical repair. J Shoulder Elbow Surg. 1994;3(2):70-78. doi:10.10 16/S1058-2746(09)80113-4
15. Holschen M, Brand F, Agneskirchner JD. Subacromial spacer implantation for massive rotator cuff tears. Obere Extrem. 2017;12(1):38-45. doi:10.1007/s11678-016-0386-9
16. Burkhart SS, Nottage WM, Ogilvie-Harris DJ, Kohn HS, Pachelli A. Partial repair of irreparable rotator cuff tears. Arthroscopy: The Journal of Arthroscopic & Related Surgery. 1994;10(4):363-370. doi:10.1016/S0749-8063(05)80186-0
17. Porcellini G, Castagna A, Cesari E, Merolla G, Pellegrini A, Paladini P. Partial repair of irreparable supraspinatus tendon tears: clinical and radiographic evaluations at long-term follow-up. J Shoulder Elbow Surg. 2011;20(7):1170-1177. doi: 10.1016/j.jse.2010.11.002
18. Farazdaghi A, Paschos NK, Kelly JD. Comparison between partial and full coverage repair in massive rotator cuff tears. A minimum five year follow-up. Orthopaedics & Traumatology: Surgery & Research. 2021;107(4):102911. doi:10. 1016/j.otsr.2021.102911
19. Burkhart SS, Denard PJ, Adams CR, Brady PC, Hartzler RU. Arthroscopic Superior Capsular Reconstruction for Massive Irreparable Rotator Cuff Repair. Arthrosc Tech. 2016;5(6):e1407-e1418. doi:10.1016/j.eats.2016.08.024
20. Kim DM, Shin MJ, Kim H, et al. Comparison Between Autografts and Allografts in Superior Capsular Reconstruction: A Systematic Review of Outcomes. Orthop J Sports Med. 2020;8(3):23259 6712090493. doi:10.1177/2325967120904937
21. Kim D, Um J, Lee J, Kim J. Improved Clinical and Radiologic Outcomes Seen after Superior Capsule Reconstruction using Long Head Biceps Tendon Autograft. Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2021;37(9):2756-2767. doi:10.1016/j.arthro.2021.04.006
22. Hartzler RU, Barlow JD, An KN, Elhassan BT. Biomechanical effectiveness of different types of tendon transfers to the shoulder for external rotation. J Shoulder Elbow Surg. 2012;21(10):1370-1376. doi:10.1016/j.jse.2012.01.026
23. Velasquez Garcia A, Nieboer MJ, de Marinis R, Morrey ME, Valenti P, Sanchez-Sotelo J. Mid- to long-term outcomes of latissimus dorsi tendon transfer for massive irreparable posterosuperior rotator cuff tears: a systematic review and meta-analysis. J Shoulder Elbow Surg. 2024;33(4):959-974. doi:10.1016/j.jse.2023.10.002
24. Clouette J, Leroux T, Shanmugaraj A, et al. The lower trapezius transfer: a systematic review of biomechanical data, techniques, and clinical outcomes. J Shoulder Elbow Surg. 2020;29(7):150 5-1512. doi:10.1016/j.jse.2019.12.019
25. Cartucho A. Tendon transfers for massive rotator cuff tears. EFORT Open Rev. 2022;7(6):404-413. doi:10.1530/EOR-22-0023
26. Oh JH, Tilan J, Chen YJ, Chung KC, McGarry MH, Lee TQ. Biomechanical effect of latissimus dorsi tendon transfer for irreparable massive cuff tear. J Shoulder Elbow Surg. 2013;22(2):150-157. doi:10.1016/j.jse.2012.01.022
27. Galasso O, Mantovani M, Muraccini M, et al. The latissimus dorsi tendon functions as an external rotator after arthroscopic-assisted transfer for massive irreparable posterosuperior rotator cuff tears. Knee Surgery, Sports Traumatology, Arthroscopy. 2020;28(7):2367-2376. doi:10.1007/s 00167-019-05819-2
28. Longo UG, Franceschetti E, Petrillo S, Maffulli N, Denaro V. Latissimus Dorsi Tendon Transfer for Massive Irreparable Rotator Cuff Tears. Sports Med Arthrosc Rev. 2011;19(4):428-437. doi:10.1097/ JSA.0b013e3182390639
29. Reddy A, Gulotta L V., Chen X, et al. Biomechanics of lower trapezius and latissimus dorsi transfers in rotator cuff–deficient shoulders. J Shoulder Elbow Surg. 2019;28(7):1257-1264. doi: 10.1016/j.jse.2018.11.066
30. Muench LN, Berthold DP, Kia C, et al. Biomechanical comparison of lower trapezius and latissimus dorsi transfer for irreparable posterosuperior rotator cuff tears using a dynamic shoulder model. J Shoulder Elbow Surg. 2022;31 (11):2392-2401. doi:10.1016/j.jse.2022.05.003
31. Baek CH, Kim BT, Kim JG, Kim SJ. Mid-term outcomes of arthroscopically assisted lower trapezius tendon transfer using Achilles allograft in treatment of posterior-superior irreparable rotator cuff tear. J Shoulder Elbow Surg. 2024;33(6):1293-1305. doi:10.1016/j.jse.2023.09.013
32. Elhassan BT, Wagner ER, Werthel JD. Outcome of lower trapezius transfer to reconstruct massive irreparable posterior-superior rotator cuff tear. J Shoulder Elbow Surg. 2016;25(8):1346-1353. doi:10.1016/j.jse.2015.12.006
33. Marigi EM, Jackowski JR, Elahi MA, et al. Improved Yet Varied Clinical Outcomes Observed With Comparison of Arthroscopic Superior Capsular Reconstruction Versus Arthroscopy-Assisted Lower Trapezius Transfer for Patients With Irreparable Rotator Cuff Tears. Arthroscopy – Journal of Arthroscopic and Related Surgery. 2023;39(10) :2133-2141. doi:10.1016/j.arthro.2023.04.012
34. Somerson JS, Hsu JE, Gorbaty JD, Gee AO. Classifications in Brief: Goutallier Classification of Fatty Infiltration of the Rotator Cuff Musculature. Clin Orthop Relat Res. 2016;474(5):1328-1332. doi:10.1007/s11999-015-4630-1
35. Elhassan BT, Sanchez-Sotelo J, Wagner ER. Outcome of arthroscopically assisted lower trapezius transfer to reconstruct massive irreparable posterior-superior rotator cuff tears. J Shoulder Elbow Surg. 2020;29(10):2135-2142. doi:10.1016/j.jse.2020.02.018
36. Wagner ER, Woodmass JM, Welp KM, et al. Novel arthroscopic tendon transfers for posterosuperior rotator cuff tears latissimus dorsi and lower trapezius transfers. JBJS Essent Surg Tech. 2018;8(2). doi:10.2106/JBJS.ST.17.00062
37. Gerber C. Latissimus Dorsi Transfer for the Treatment of Irreparable Rotator Cuff Tears. The Journal of Bone and Joint Surgery (American). 2006;88(1):113. doi:10.2106/JBJS.E.00282
38. Memon M, Kay J, Quick E, et al. Arthroscopic-Assisted Latissimus Dorsi Tendon Transfer for Massive Rotator Cuff Tears: A Systematic Review. Orthop J Sports Med. 2018;6(6):23259671187777 3. doi:10.1177/2325967118777735
39. Gerber C, Rahm SA, Catanzaro S, Farshad M, Moor BK. Latissimus Dorsi Tendon Transfer for Treatment of Irreparable Posterosuperior Rotator Cuff Tears. Journal of Bone and Joint Surgery. 2013;95(21):1920-1926. doi:10.2106/JBJS.M.00122
40. Waltenspül M, Jochum B, Filli L, et al. Mid-term results of arthroscopically assisted latissimus dorsi transfer for irreparable posterosuperior rotator cuff tears. J Shoulder Elbow Surg. 2021;30 (11):e676-e688. doi:10.1016/j.jse.2021.03.149
41. El-Azab HM, Rott O, Irlenbusch U. Long-Term Follow-up After Latissimus Dorsi Transfer for Irreparable Posterosuperior Rotator Cuff Tears. Journal of Bone and Joint Surgery. 2015;97(6):462-469. doi:10.2106/JBJS.M.00235
42. Elhassan B, Bishop A, Shin A. Trapezius Transfer to Restore External Rotation in a Patient with a Brachial Plexus Injury. The Journal of Bone and Joint Surgery-American Volume. 2009;91(4): 939-944. doi:10.2106/JBJS.H.00745
43. Sanchez-Sotelo J. Lower Trapezius Transfer for Irreparable Posterosuperior Rotator Cuff Tears. Curr Rev Musculoskelet Med. 2024;17(4):93-100. doi:10.1007/s12178-024-09885-z
44. Ye L, Han D, Zhang Q, Yang X, Tung TH, Zhou X. Early Efficacy Assessment of Arthroscopic Lower Trapezius Transfer With Tendon Autograft in the Management of Massive Irreparable Posterosuperior Rotator Cuff Tears. Front Surg. 2022;8. doi:10.3389 /fsurg.2021.796359
45. Valenti P, Werthel JD. Lower trapezius transfer with semitendinosus tendon augmentation. Obere Extrem. 2018;13(4):261-268. doi:10.1007/s11678-018-0495-8
46. Chopra A, Wright MA, Murthi AM. Outcomes after arthroscopically assisted lower trapezius transfer with Achilles tendon allograft. J Shoulder Elbow Surg. 2024;33(2):321-327. doi:10.1016/j.jse. 2023.06.029
47. Clark NJ, Elhassan B. Tendon Transfer for Irreparable Rotator Cuff Tears. Oper Tech Sports Med. 2018;26(1):58-69. doi:10.1053/j.otsm.2017.10.009
48. Omid R, Heckmann N, Wang L, McGarry MH, Vangsness CT, Lee TQ. Biomechanical comparison between the trapezius transfer and latissimus transfer for irreparable posterosuperior rotator cuff tears. J Shoulder Elbow Surg. 2015;24(10):1635-1643. doi:10.1016/j.jse.2015.02.008
49. Stoll LE, Codding JL. Lower Trapezius Tendon Transfer for Massive Irreparable Rotator Cuff Tears. Orthopedic Clinics of North America. 2019;50 (3):375-382. doi:10.1016/j.ocl.2019.03.004
50. Baek CH, Lee DH, Kim JG. Latissimus dorsi transfer vs. lower trapezius transfer for posterosuperior irreparable rotator cuff tears. J Shoulder Elbow Surg. 2022;31(9):1810-1822. doi: 10.1016/j.jse.2022.02.020
51. Marigi EM, Johnson QJ, Dholakia R, Borah BJ, Sanchez-Sotelo J, Sperling JW. Cost comparison and complication profiles of superior capsular reconstruction, lower trapezius transfer, and reverse shoulder arthroplasty for irreparable rotator cuff tears. J Shoulder Elbow Surg. 2022;3 1(4):847-854. doi:10.1016/j.jse.2021.08.027
52. Omid R, Cavallero MJ, Granholm D, Villacis DC, Yi AM. Surgical anatomy of the lower trapezius tendon transfer. J Shoulder Elbow Surg. 2015;24(9) :1353-1358. doi:10.1016/j.jse.2014.12.033
53. Herzberg G, Urien JP, Dimnet J. Potential excursion and relative tension of muscles in the shoulder girdle: Relevance to tendon transfers. J Shoulder Elbow Surg. 1999;8(5):430-437. doi:10. 1016/S1058-2746(99)90072-1
54. Tang J, Zhao J. Arthroscopic Humeral Bone Tunnel–Based Tendon Grafting and Trapezius Transfer for Irreparable Posterior Superior Rotator Cuff Tear. Arthrosc Tech. 2021;10(4):e1079-e1087. doi:10.1016/j.eats.2020.12.011
55. Namdari S, Voleti P, Baldwin K, Glaser D, Huffman GR. Latissimus Dorsi Tendon Transfer for Irreparable Rotator Cuff Tears. Journal of Bone and Joint Surgery. 2012;94(10):891-898. doi:10.2106/ JBJS.K.00841