





Minimally Invasive Osteosynthesis for Distal Humerus Fracture
Minimally invasive osteosynthesis of distal humerus fracture with commercially available pre-contoured plate using an anterolateral approach: a cadaveric study
ABSTRACT
Background: Minimally invasive plate osteosynthesis for the surgical treatment of distal diaphyseal humerus fractures represents an attractive option as it minimizes the extensive soft-tissue disruption associated with the posterior open approach. A minimally invasive plate osteosynthesis through an anteromedial has been proposed as an alternative; however, it could be technically challenging due to the closeness of the median and ulnar nerves and brachial artery.
Aims: This anatomical study aimed to determine the feasibility and safety of a minimally invasive plate osteosynthesis through an anterior approach and anterolateral fixation using a pre-contoured locking plate modified to adjust to the anatomical surface of the lateral column of the humerus.
Methods: Nine arms from five fresh cadavers were used to simulate the surgical procedure of minimally invasive plate osteosynthesis through an anterior approach performing anterolateral fixation using a molded commercially available locking plate on the lateral column of the humerus of the previously created distal diaphyseal humerus fracture. Assessed measurements were the interval from the distal part of the plate to the capitellum, the interval from the plate to the lateral cortex of the humerus, and the distance from the plate to the radial nerve.
Results: The most distal location of the plate is defined by palpating the most proximal edge of the capitellum. The mean distance from the distal part of the plate to the capitellum was 10.75 ± 0.9 mm, from the plate to the lateral cortex of the humerus was 5.25 ± 0.7 mm, and from the plate to the radial nerve was 10.9 ± 0.6 mm.
Conclusion: This anterior approach for a minimally invasive plate osteosynthesis with anterolateral fixation in distal diaphyseal humerus fractures allows better visualization of the fracture site with minimal soft tissue damage while protecting the radial neurovascular structures; careful dissection is crucial to reduce potential complications.
Keywords: Humeral Fractures, Distal; Cadaver; Fracture Fixation, Internal; Bone Plates; Minimally Invasive Surgical Procedures.
Introduction
Distal diaphyseal humerus fractures (DDHF) are the less frequent fractures of the humerus, representing about 1–2% of all fractures in the adult population¹². These fractures occur in a bimodal distribution, caused by high-energy traumas in males aged 12–19 years and by low-energy trauma and falls in elderly females¹–⁴. Most DHFs are extra-articular and often comminuted, making surgical treatment a challenge due to the complex joint surface anatomy, the poor bone quality frequently associated, and the proximity of neurovascular structures¹²⁴⁵.
Although open reduction and internal fixation (ORIF) is the current standard of care for DDHF with the objective of satisfactory restoration of elbow function, stable fixation of all fracture fragments and low rate of complications³–⁶, there is still controversy about the ideal approach and plate fixation that minimizes short-term and long-term treatment-related complications such as iatrogenic injuries to the radial and ulnar nerves while reducing the soft-tissue trauma and scarring¹⁴⁵⁹.
The posterior approach with single-column fixation or dual plating are the techniques of choice of many authors as they allow important articular exposure but at the expense of osteotomy and extensive soft-tissue disruption; nonetheless, the outcomes with this approach have been clinically and radiographically satisfactory¹²⁴⁶⁷¹⁰–¹². Medial and lateral approaches have also been evaluated with acceptable results regarding the speed of restoration of elbow function comparable to those of the posterior approach¹³¹⁴. Parmaksizoglu et al.¹⁴ described a lateral approach in patients with extra-articular DDHF that allowed a rigid fixation using enough screws in the distal fragment with satisfactory results without compromising elbow flexion and decreasing the risk of iatrogenic radial nerve injury¹⁴. Yet, the full open approach causes extensive soft-tissue trauma and large scar.
Minimally invasive plate osteosynthesis (MIPO) using different approaches for DDHF has been proposed as a method that creates less soft-tissue disruption¹⁵–²⁰. Two anatomical studies performed by Cañada-Oya et al.¹⁶, and Yang et al.¹⁷, have suggested that a MIPO, through an anteromedial approach, could minimize the risk of injury to radial neurovascular structures. However, this approach involves a high degree of difficulty since anatomical structures such as the median and ulnar nerves and the brachial artery are at risk¹⁶¹⁷. An anterior approach with anterolateral fixation could represent less risk due to trauma surgeons’ familiarity with the anatomical structures involved and the avoidance of medial neurovascular structures.
In this study, we conducted an anatomical study to determine the feasibility of applying the MIPO technique to treat DDHF using the anterior approach with anterolateral fixation with a modified commercially available pre-contoured locking plate. We assessed the anatomical safety of the radial neurovascular structures when placing and fixing the plate.
Methods
ANATOMICAL STUDY
This anatomical study was performed on nine arms from five fresh cadavers – two males and three females – at the National Institute of Legal Medicine and Forensic Sciences (Medellin, Colombia) and after our Institutional Review Board (IRB) provided its approval. All methods were carried out following guidelines and regulations.
As a first step, the plate is molded to accommodate the anatomical surface of the humerus. A contralateral, LCP® Extra-articular Distal Humerus Plate (DePuy Synthes, Johnson & Johnson) was used for each side. The plate molding is carried out on two levels using the system’s forceps. The first molding is performed between the 4th and 5th distal hole to facilitate adequate adaptation to the anterior cortex of the distal humerus, and the second, between the 3rd and 4th most distal hole for correction of the curvature of the plate. A plastic humeral bone model was used to assess the plate position after molding to the desired shape, observing the bony anatomical relations (Figure 1).
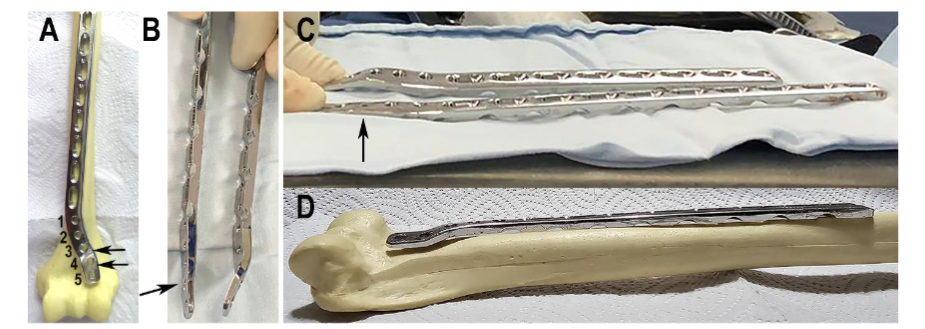
Figure 1. Molding of the plate. (A) The arrows indicate the levels where the molding takes place. (B and C) The molded plate indicated by the arrow is placed side by side to the original for comparison. (D) The molded plate is placed on the anterior surface of the humerus to show the plate’s fit for the bone anatomy.
The cadavers’ arms were thoroughly inspected (palpation and x-rays) to rule out actual traumas, fractures, previous surgical procedures, or malformations in the anatomic area of interest. One arm from a female cadaver, not included in the measurements, served as a pilot specimen to define landmarks, skin incisions, and stepwise dissections needed for the proposed anterolateral approach.
First, a distal diaphyseal fracture was created in each humerus (n=8). A transverse fracture of the distal third of the humeral shaft was recreated by a direct posterior approach, about 9 cm proximal to the articular surface, with the epicondyles as the reference point (Figure 2).
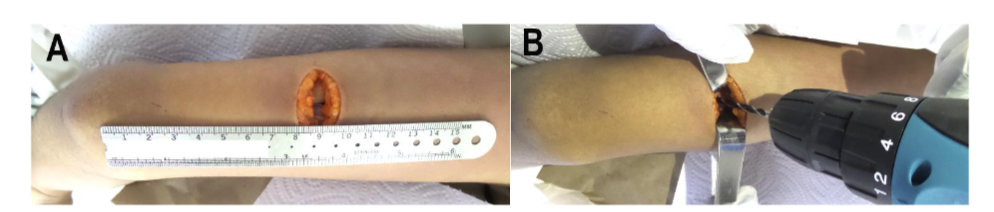
Figure 2. Distal fracture creation. (A) Incision location for the posterior approach for fracture creation. (B) Controlled fracture creation at distal humerus.
With the arm supine, the anterior approach begins by marking the antecubital fold. Then, the site of the first incision is marked perpendicular and 2 cm proximal to the antecubital fold at the midpoint of the anterior surface of the distal third of the arm; taking the epicondyles as a reference, there, a 3 cm skin incision was made (Figure 3).

Figure 3. Anterior distal approach. (A) The antecubital fold is marked. (B) The distance between the fold and the distal starting point of the incision. (C) Length and location of the distal anterior incision.
The dissection of the subcutaneous cellular tissue is continued up to the arm fascia. The biceps muscle is rejected medially, and the brachialis muscle is exposed. The lateral antebrachial cutaneous nerve that runs between both muscles is identified; that nerve does not require manipulation (Figure 4).
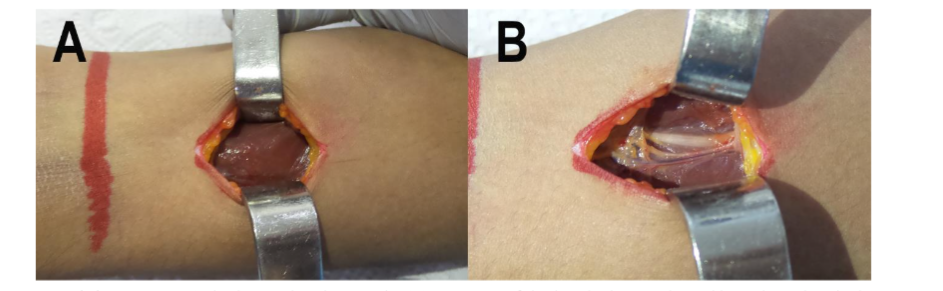
Figure 4. Initial dissection. (A) The biceps brachii muscle. (B) Exposure of the brachialis muscle and lateral antebrachial cutaneous nerve after rejecting the biceps brachii.
The biceps brachii muscle is rejected medially, and the brachialis muscle is bluntly dissected in the same orientation of its fibers until the distal third of the humeral shaft is exposed using a double-ended US Army type retractor (long), identifying the coronoid fossa and the lateral column of the distal humerus. Then, an anterior approach with a 4–5 cm skin incision is performed on the proximal third of the arm in the deltopectoral interval until the humeral shaft is exposed, keeping in mind the length of the chosen plate (Figure 5).
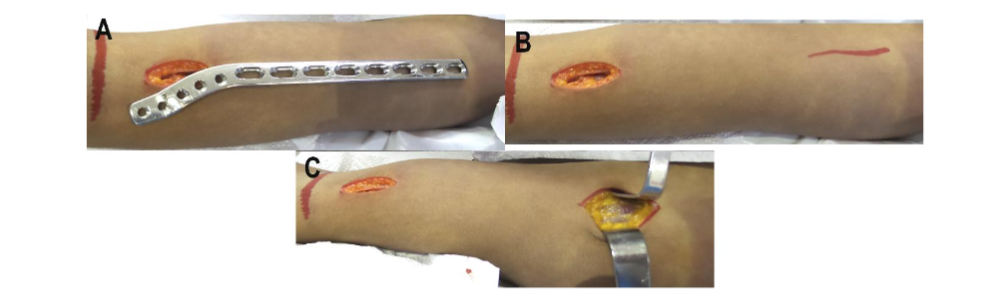
Figure 5. Anterior proximal approach. (A) The plate length is used to define the proximal approach. (B) The position of the proximal incision is marked. (C) After the skin incision, the distal deltopectoral interval is searched for.
Fracture reduction is performed using elbow traction movements, with about 60 degrees of shoulder abduction and always keeping the elbow flexed at 90 degrees with the forearm supinated.
Both approaches are communicated submuscularly, and the molded plate is slid from distal to proximal (Figure 6).

Figure 6. Plate insertion. The retrograde plate slipped through the distal incision up to the location of the proximal incision.
The location of the plate should be 1 cm proximal to the most proximal part of the capitellum to avoid blocking elbow flexion. With the help of the image intensifier, the plate should be in the center of the lateral column of the distal humerus with equidistant distances between the lateral cortex and the coronoid fossa (Figure 7).
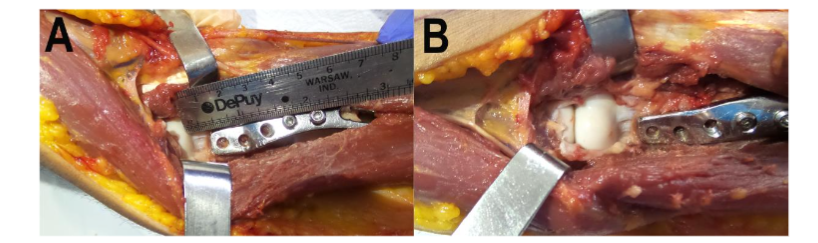
Figure 7. Plate distal position. (A and B). Images of the specimen after removing skin and biceps brachii muscle and completely separating the brachialis muscle allow observing the optimal distance of at least 1 cm from the most distal edge of the plate to the most proximal edge of the capitellum.
Distal fixation should occur with all five screws locked to obtain maximum benefit from the stability of the distal segment. Proximal fixation is performed with three screws, and fracture reduction and fixation are evaluated (Figure 8).
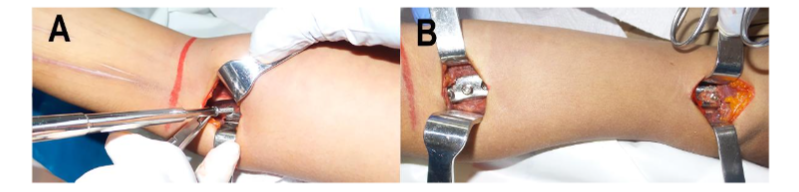
Figure 8. Plate fixation. (A) Distal fixation. (B) Appearance after complete fixation of the plate. An intraoperative C-arm verifies the reduction and position of the osteosynthesis material. Conventional closure is carried out by planes.
MEASUREMENTS
To develop a minimally invasive surgical approach, a plane dissection was first performed in the distal third of the arm for the identification and characterization of structures at risk. The proximity and course of the radial nerve and its relationship with the anterior cortex of the distal third of the humerus were evaluated (Figure 9).
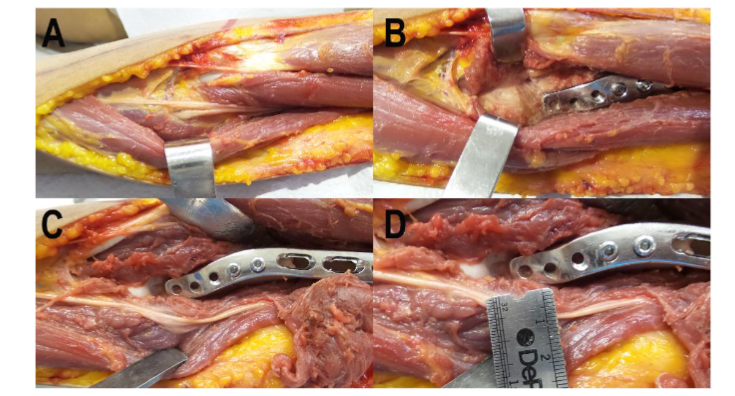
Figure 9. Anatomical relations with the plate (specimen deprived of skin and the biceps brachii muscle).
(A) Exposure of the radial nerve before its bifurcation by the supinator muscle.
(B) Separation of the brachialis muscle that contains the radial nerve in the lateral belly.
(C) Resection of the brachialis muscle to show the course of the radial nerve.
(D) The proximity of the radial nerve to the plate in the absence of the lateral portion of the brachialis.
For defining the relationships of nervous structures with osteosynthesis material, three distances were defined:
(1) Interval from distal part of plate to capitellum: considered from the distal end of the plate to the most proximal edge of the capitellum.
(2) Interval from plate to lateral cortex of humerus: measured from the distal lateral edge of the plate to the lateral cortex of the distal humerus.
(3) Distance from plate to radial nerve: estimated from the distal and lateral border of the plate to the radial nerve.
All three measurements were conducted in millimeters using a standard metric system ruler.
Figure 10 depicts schematic illustrations of the final anatomical position of the plate and its relationships with the radial nerve and capitellum.
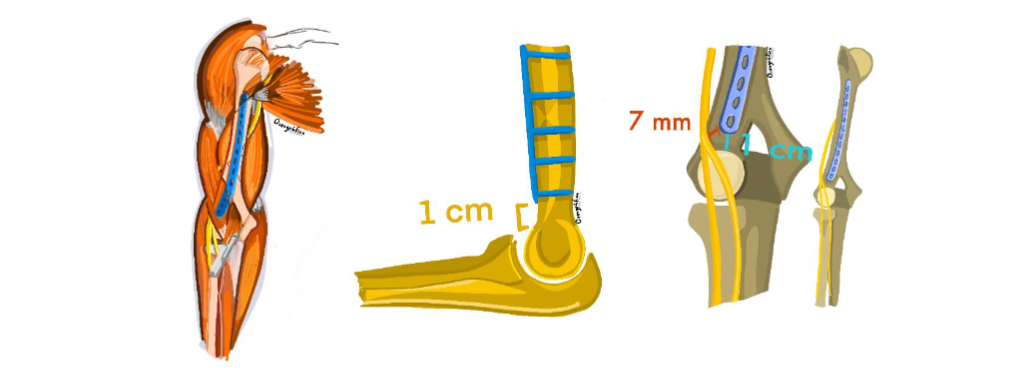
Figure 10. Anatomical illustrations. (A) Depicts the relationship of the plate with the capitellum and the radial nerve. (B) Illustrates the optimal position of the plate to avoid anterior impingement during flexion. (C) Representation of the final location and position of the plate after reduction and fixation.
STATISTICAL ANALYSIS
Statistical descriptive analysis of all measurements was conducted using SPSS statistical software (version 25.0; IBM Corp, Armonk, NY, USA). The continuous variables are presented as mean, standard deviation (SD), median, minimum, and maximum.
Results
ANATOMICAL ASSESSMENT
Through the initial distal incision, the lateral antebrachial cutaneous nerve was clearly identified in all specimens. The rejection of the biceps brachii muscle from the surgical approach and the dissection of the brachialis muscle permitted easy exposure of the distal third of the humeral shaft. Likewise, the proximal humeral shaft exposure was also easily achieved through the proximal incision. The most proximal edge of the capitellum should be palpated to define the most distal location of the plate. Once the plate was placed, the mean (SD) distance from the distal part of the plate to the capitellum was 10.75 (0.9) mm (Table 1). The anterolateral approach allowed the placement of the plate on the lateral column of the humerus in a simple way, with a mean (SD) distance from the plate to the lateral cortex of the humerus of 5.25 (0.7) mm (Table 1). These distances were consistent across all anatomic specimens.
The radial nerve runs lateral to the most lateral edge of the plate in the distal region, and a higher risk of damage was observed in the distal approach when the brachialis muscle is dissected in the middle; however, the closest distance from the plate to the radial nerve was 10 mm with a mean (SD) of 10.9 (0.6) mm.
The vascular structures are not at risk from this approach because, distally, they are in the medial part of the arm.
Table 1. Measured distances
Distances (mm)
Cadaver # | Arm # | Side | Sex | The distal part of the plate to capitellum | Plate to lateral cortex of humerus | Plate to the radial nerve
1 | 1 | Left | Male | 10 | 4 | 10
1 | 2 | Right | Male | 10 | 5 | 11
2 | 3 | Left | Female | 10 | 5 | 10
2 | 4 | Right | Female | 12 | 6 | 12
3 | 5 | Left | Male | 11 | 6 | 11
3 | 6 | Right | Male | 12 | 6 | 11
4 | 7 | Left | Female | 10 | 5 | 11
4 | 8 | Right | Female | 11 | 5 | 11
Mean: 10.75 | 5.25 | 10.9
SD: 0.9 | 0.7 | 0.6
Median: 10.5 | 5 | 11
SD: standard deviation
Discussion
Open reduction and internal fixation remain the primary treatment options for extra-articular DDHF, given the risk of malunion and nonunion of this type of fractures. Additionally, surgical treatment allows for an earlier return to everyday activities. However, plating and internal fixation are intricate due to the complex anatomy of the elbow, and complications often lead to sequelae, such as elbow stiffness and irremediable neurovascular compromise¹–⁵. Numerous surgical methods have been proposed to reach the fracture site while reducing injury to the neurovascular structures¹³,¹⁷,²¹–²⁴. Minimally invasive plate osteosynthesis (MIPO) approaches for DDHF treatment continue to develop, reporting good results and, therefore, becoming more popular¹⁶–²¹,²⁵. With this cadaveric study, we showed that MIPO through an anterior approach using the lateral column of the humerus as a fixation point for this specific plate, is feasible and anatomically safe.
The minimally invasive approach for plate osteosynthesis has been gaining acceptance as a surgical method for treating DDHF, which, by avoiding excessive dissection to reach the fracture site, produces less soft tissue damage¹⁶–²⁰,²⁶. Nonetheless, the reduction of the dissection field could come at the expense of an increased risk of neurovascular compromise. Performing postoperative ultrasound, Livani et al.²⁷ showed that the radial nerve could be at a higher risk of injury after a MIPO through an anterior approach for DDHF with plates fixed to the lateral column of the humerus, given its “critical point” of closeness to the plate, but their findings lacked statistical significance²⁷. Contrasting, in the meta-analysis performed by Beeres et al.²¹ comparing different clinical and radiological outcomes of ORIF versus MIPO for DDHF treatment, it was shown that secondary and transient radial nerve palsy occurred significantly with less frequency after MIPO than after ORIF²¹. In the search for the ideal surgical approach for a MIPO to treat middle and DDHF, several authors have proposed posterior¹⁹, anterior¹⁸,²⁰, anteromedial¹⁶,¹⁷, and anterolateral²⁶ approaches that allow exposing sufficient fixation space with less extensive surgical dissection while minimizing iatrogenic radial nerve injury.
Jitprapikulskarn et al.¹⁹ published a technical note for MIPO with a posterior approach for DDHF performed in 18 patients with type B or C fractures. According to the authors, this approach provides better exposure and visualization of the fracture site but carries an important risk of iatrogenic injury of the radial nerve. However, in that series, only two patients presented temporary radial nerve palsy that fully recovered within 12 weeks¹⁹. On the other hand, even though the anterior or anteromedial approach to the humerus may also lead to iatrogenic injury to either the radial or to the ulnar and median nerve, respectively, both anatomical¹⁶,¹⁷ and series¹⁷,¹⁹,²⁰ studies have shown that this damage while placing the plate can be avoided if the fracture-to-coronoid distance (FCD) is >2 cm; otherwise, other approaches are advisable. Zhao et al.²⁶ used the anterolateral approach with one distal incision at the fracture site in 28 patients with DDHF. The authors described how the fracture reduction and radial nerve exploration were achieved through the small incision; during follow-up, no iatrogenic neuropraxia occurred²⁶.
In our study, with the anterior approach and anterolateral fixation, the most immediate risk of radial nerve injury is in the distal approach when performing the lateral separation of the intermuscular septum, given its proximity to the nerve path; this injury is avoided by performing blunt longitudinal dissection of the brachialis muscle, maintaining separation, without tension, along the muscle. The distance from the radial nerve to the lateral column and the lateral edge of the plate was, on average, 10.9 ± 0.6 mm, as seen in Figures 9C and 9D. Then, after blunt dissection of the brachialis muscle, and to protect the nerve, the force of separation must be minimal to avoid injury due to traction of the nerve. We agree with Zhao et al.²⁶ with the suggestion that, with an adequate anterolateral approach, the radial nerve can be easily visualized and exposed between the brachialis and brachioradialis muscles, allowing for safe manipulation of the surgical field and plate placement without disturbing the nerve. However, contrary to the technique performed by Zhao et al.²⁶, our method does not involve nerve exploration or neurolysis, which could decrease accidental nerve injury. Additionally, our double incisions permit a more controlled proximal visualization and handling of the plate.
Other studies have reported using minimally invasive approaches through anteromedial and distal incision using the medial column of the humerus as a fixation point. The surgical technique requires either an incision in the pronator teres muscle to insert the plate as described by Cañada-Oya et al.¹⁶ in their anatomical study, or the creation of a soft tissue tunnel under the brachialis muscle to avoid exposure of the neurovascular structures, as one utilized by Yang et al.¹⁷. Even though the results reported up to now by the latter are satisfactory without neurovascular injuries¹⁷, special training is required to use this surgical technique safely and avoid injuries to the median nerve, brachial artery, and ulnar nerve.
The stability of the fixation depends on several factors, such as the type of fracture, the plate’s shape and length, enough to cover the whole fracture line proximally and distally, the suitable bone surface for strong screw positioning, the position of the screws and the density of screw placement. Apivathakakul et al.²⁵ and Zhiquan et al.²⁰ explored the feasibility and safety of a MIPO with an anterior approach for middle and distal third humeral shaft fractures in cadaveric specimens and in a series of patients, showing promising results. However, in both techniques, fixation is performed with a straight plate and not placed in the lateral column of the humerus²⁰,²⁵. The thicker distal profile of a straight plate does not allow for its proximity to the capitellum, making it a challenging method for very distal fractures. Zhao et al.²⁶ utilized an anterolateral approach using a locking compression plate of 10–14 holes that was molded to fit the anterior surface of the humerus and placed at either the lateral or medial columns. The possible drawback of their technique resides in the fact that the distal fixation is performed with few screws (2 or 3)²⁶, which could provide less stability to the distal segment.
In the proximal region of humeral shaft fixation, the plate’s position will depend on the extent of the fracture line. Usually, a 10-hole LCP® Extra-articular Distal Humerus Plate (DePuy Synthes, Johnson & Johnson) will offer an appropriate working length to allow relative stability and, thus, fracture healing. With longer plates, the fixation must be immediately lateral to the path of the long head of the biceps before it enters the bicipital groove, a problem that Fernandez Dell’Oca²⁸ exposes in his study. As mentioned, previous works have already exposed the possibility of fixing distal shaft fractures of the humerus with straight plates²⁰,²⁵,²⁹, providing fixation immediately proximal to the coronoid fossa or in the most proximal region of the lateral column, with the drawback of having a low density of distal screws placing²⁴. The stability of the fixation is at risk if the line is very distal or if it can fix only those fractures at a certain distance from the coronoid fossa²⁵,³⁰. The main advantage offered by the use of this proposed surgical technique in DDHF is that by being able to perform distal fixation in the lateral column with five cortical or blocked screws, it allows stable fixation of the vast majority of distal fractures of the humerus, even fractures relatively close to the coronoid fossa, a limitation that is described in the initial development of minimally invasive osteosynthesis¹⁸,²⁵.
There are some limitations to this approach and fixation. First, in this technique, to preserve the elbow flexion, the minimum distance from the most distal edge of the plate to the most proximal part of the capitellum or the FCD should be 1 cm. However, this distance is very similar to the distance from the olecranon fossa to the fourth most distal screw reported by Yang et al.¹⁷ in their anteromedial approach and smaller than the FCD recommended by Jitprapikulskarn et al.¹⁸ in their anterior approach. Furthermore, the advantage of this technique with this specific plate is that its thinner profile in the distal end allows for closer proximity to the capitellum without interfering with elbow flexion and permits a more stable fixation because of the number of distal screws that can be placed. Second, we used a commercially available contralateral extra-articular distal humerus plate that needed to be modified into the desired shape to adapt to the anatomy of the anterior surface of the humerus. The subjectivity of the required bending or molding of the plate is part of the technique’s learning curve. However, it is still being determined if the molding of the plate could deplete its cycling, leading to failure due to loosening or fatigue of the material. Currently, we are carrying out a mid and long-term follow-up of a series of patients that could provide evidence of the stability of the fixation with the altered plate. Third, although the proximity to the distal radial nerve carries a risk with this technique, the approach allows for direct visualization of the structure without exploring it and avoiding any unintentional damage. Additionally, the distance from the plate to the radial nerve is considerably larger than the mean “critical point” of 4 mm reported by Livani et al.²⁷ in their ultrasound study.
Conclusion
We propose a new anterior approach and anterolateral fixation for minimally invasive plate osteosynthesis of distal humerus fractures using a manually molded pre-contoured modified locking plate fixated to the lateral column of the humerus. This approach allows better visualization of the fracture site with minimal soft tissue damage while protecting the radial neurovascular structures; careful dissection is crucial to reduce potential complications.
Conflict of Interest:
The authors have no conflicts of interest to declare.
Funding Statement:
None.
Acknowledgements:
The authors would like to thank Dr. Ivan Arroyave, who created the illustrations of the anatomical study through his specialized service, “Oseográfico are digital.”
Institutional Review Board (IRB):
Our IRB approved this study on March 18, 2024 (Universidad Pontificia Bolivariana, file number 5 of 2024).
References
1. Morrey ME, Morrey BF, Sanchez-Sotelo J, Barlow JD, O’Driscoll S. A review of the surgical management of distal humerus fractures and nonunions: From fixation to arthroplasty. J Clin Orthop Trauma. 2021;20. doi:10.1016/j.jcot.2021.101477
2. Beazley JC, Baraza N, Jordan R, Modi CS. Distal Humeral Fractures-Current Concepts. Open Orthop J. 2017;11(1):1353-1363. doi:10.2174/187 4325001711011353
3. Savvidou OD, Zampeli F, Koutsouradis P, et al. Complications of open reduction and internal fixation of distal humerus fractures. EFORT Open Rev. 2018;3(10):558-567. doi:10.1302/2058-5241. 3.180009
4. Nowak LL, Dehghan N, McKee MD, Schemitsch EH. Plate fixation for management of humerus fractures. Injury. 2018;49:S33-S38. doi:10.1016/S0 020-1383(18)30300-0
5. Mighell MA, Stephens B, Stone GP, Cottrell BJ. Distal Humerus Fractures. Hand Clin. 2015;31(4):59 1-604. doi:10.1016/j.hcl.2015.06.007
6. Piekarczyk P, Kwiatkowski K, Piątkowski K, Gołos J, Kuczmera P. Outcomes after Open Reduction and Plate Fixation of Distal Humerus Fractures. Ortop Traumatol Rehabil. 2015;17(6):627-636. doi: 10.5604/15093492.1193035
7. Capo JT, Debkowska MP, Liporace F, Beutel BG, Melamed E. Outcomes of distal humerus diaphyseal injuries fixed with a single-column anatomic plate. Int Orthop. 2014;38(5):1037-1043. doi:10.1007/s00264-013-2213-x
8. Han SH, Park JS, Baek JH, Kim S, Ku KH. Complications associated with open reduction and internal fixation for adult distal humerus fractures: a multicenter retrospective study. J Orthop Surg Res. 2022;17(1). doi:10.1186/s13018-022-03292-1
9. Halaç O. Distal Humerus Fractures. In: Multidisciplinary Approach to Trauma. Nova Science Publishers, Inc.; 2022:81-92. doi:10.101 6/j.hcl.2015.06.007
10. Jain D, Goyal GS, Garg R, Mahindra P, Yamin M, Selhi HS. Outcome of anatomic locking plate in extraarticular distal humeral shaft fractures. Indian J Orthop. 2017;51(1):86-92. doi:10.4103/0019-5413.197554
11. Wajnsztejn A, de Albuquerque DD, Espinola I, et al. Submuscular double bridge plating for complex distal fractures of the humerus: an alternative, safe, and efficient treatment method. European Journal of Orthopaedic Surgery and Traumatology. 2017;27(8):1069-1074. doi:10.1007 /s00590-017-1987-8
12. Saracco M, Smimmo A, De Marco D, et al. Surgical approach for fracture of distal humerus: Posterior vs lateral. Orthop Rev (Pavia). 2020;12 (1S):52-57. doi:10.4081/or.2020.8664
13. Teng L, Zhong G, Li HB, Cen S qiang, Liu DH, Li L. Combined Medial and Lateral Approach Versus Paratricipital Approach in Open Reduction and Internal Fixation for Type C Distal Humerus Fracture: A Randomized Controlled Study. Orthop Surg. 2023;15(8):2062-2073. doi:10.1111/os.13658
14. Parmaksizoglu A, Ozkaya U, Bilgili F, Mutlu H, Cetin U. Fixation of extra-articular distal humeral fractures with a lateral approach and a locked plate: an alternative method. Acta Orthop Traumatol Turc. 2016;2(50):132-138. doi:10.3944/AOTT.2015.14.0445
15. Benninger E, Meier C. Minimally invasive lateral plate placement for metadiaphyseal fractures of the humerus and its implications for the distal deltoid insertion- it is not only about the radial nerve. A cadaveric study. Injury. 2017;48 (3):615-620. doi:10.1016/j.injury.2017.01.026
16. Cañada-Oya H, Cañada-Oya S, Zarzuela-Jiménez C, Delgado-Martinez AD. New, Minimally Invasive, Anteromedial-Distal Approach for Plate Osteosynthesis of Distal-Third Humeral Shaft Fractures An Anatomical Study. JBJS Open Access. 2020;5(1). doi:10.2106/JBJS.OA.19.00056
17. Yang J, Yang Z, Liu D, Lu Z, Tao C, Liu T. Is an anteromedial minimally invasive approach for middle and distal third humeral fractures feasible? A cadaveric study and clinical case series. Journal of Orthopaedics and Traumatology. 2023;24(1). doi:10.1186/s10195-023-00684-9
18. Jitprapaikulsarn S, Neti N, Thremthakanpon W, Gromprasit A. Anterior minimally invasive plating osteosynthesis using reversed proximal humeral internal locking system plate for distal humeral shaft fractures. European Journal of Orthopaedic Surgery and Traumatology. 2020;30 (8):1515-1521. doi:10.1007/s00590-020-02708-0
19. Jitprapaikulsarn S, Gromprasit A, Sukha K, Patamamongkonchai C, Jiamton C. Minimally invasive plate osteosynthesis via posterior approach for type B and C fractures of distal humeral shaft: surgical tactics and a clinical series. European Journal of Orthopaedic Surgery and Traumatology. 2023;33(4):1431-1437. doi:10.1007 /s00590-022-03255-6
20. Zhiquan A, Bingfang Z, Yeming W, Chi Z, Peiyan H. Minimally Invasive Plating Osteosynthesis (MIPO) of Middle and Distal Third Humeral Shaft Fractures.
21. Beeres FJ, Diwersi N, Houwert MR, et al. ORIF versus MIPO for humeral shaft fractures: a meta-analysis and systematic review of randomized clinical trials and observational studies. Injury. 2021;52(4): 653-663. doi:10.1016/j.injury.2020.11.016
22. Rosenlund AMN, Søreide E, Madsen JE, Flugsrud GB, Douglass BW, Midtgaard KS. Outcomes and complications after open reduction and internal fixation of distal humeral fractures with precontoured locking plates. OTA Int. 2022;5(4) :e220. doi:10.1097/oi9.0000000000000220
23. Shimamoto Y, Tokutake K, Takegami Y, et al. Comparative Outcomes of Anterior and Posterior Plating for Distal-Third Humerus Shaft Fractures. Journal of Hand Surgery. Published online 2023. doi:10.1016/j.jhsa.2023.07.014
24. Huang Q, Lu Y, Wang ZM, et al. Anterolateral approach with two incisions versus posterior median approach in the treatment of middle- and distal-third humeral shaft fractures. J Orthop Surg Res. 2021;16(1). doi:10.1186/s13018-021-02355-z
25. Apivatthakakul T, Arpornchayanon O, Bavornratanavech S. Minimally invasive plate osteosynthesis (MIPO) of the humeral shaft fracture: Is it possible? A cadaveric study and preliminary report. Injury. 2005;36(4):530-538. doi:10.1016/j.injury.2004.05.036
26. Zhao W, Qu W, Fu C, Jiang H, Liu S, Cheng C. Antero-lateral minimally invasive plate osteosynthesis (MIPO) with the radial nerve exploration for extra-articular distal-third diaphyseal fractures of the humerus. Int Orthop. 2017;41(9):1757-1762. doi:10 .1007/s00264-017-3514-2
27. Livani B, Belangero W, Andrade K, Zuiani G, Pratali R. Is MIPO in humeral shaft fractures really safe? Postoperative ultrasonographic evaluation. Int Orthop. 2009;33(6):1719-1723. doi:10.1007/s0 0264-008-0616-x
28. Fernández Dell’Oca AA. The principle of helical implants Unusual ideas worth considering. Injury. 2002;33:1-27. doi:10.1016/S0020-1383(02) 00064-5
29. Kim SJ, Lee SH, Son H, Lee BG. Surgical result of plate osteosynthesis using a locking plate system through an anterior humeral approach for distal shaft fracture of the humerus that occurred during a throwing motion. Int Orthop. 2016;40(7):1 489-1494. doi:10.1007/s00264-015-2895-3
30. Lee T, Yoon J. Newly designed minimally invasive plating of a humerus shaft fracture; a different introduction of the plate. Int Orthop. 2016;40(12):2597-2602. doi:10.1007/s00264-015-3097-8
Most read articles by the same author(s)
- Juan Carlos Jaramillo, MD, Antonio Orrego, MD, Simón Uribe, MD, Daniela Galeano, MD, Manuel Vallejo, MD, Ana Maria Arcila, MD, Ana Milena Herrera, MD, PhD, Arthroscopic Bankart Repair with All Suture Anchors as Treatment of Anterior Shoulder Instability , Medical Research Archives: Vol 13 No 10 (2025): Vol.13, Issue 10, October 2025