






Modified Tests for Diagnosing Primary Aldosteronism
Appraisal of Modified Tests for Diagnosis and Treatment of Primary Aldosteronism: A Single Center Experience
Piaditis G¹, Kaltsas G², Papanastasiou L¹, Gravvanis Ch¹, Gouli A¹, Voulgaris N¹, Tsiavos V¹, Tyfoxilou E¹, Vlachou S¹, Vamvakidis K³, Zografos G³, Chrousos G⁴, Markou A¹
- Department of Endocrinology and Diabetes Center, “G. Gennimatas”, General Hospital of Athens, Athens, Greece
- 1st Department of Propaedeutic Internal Medicine, National and Kapodistrian University of Athens, Greece
- Third Department of Surgery, Athens General Hospital “G. Gennimatas”, Athens, Greece
- University Research Institute of Maternal and Child Health and Precision Medicine, National and Kapodistrian University of Athens, Medical School, Athens, Greece
OPEN ACCESS
PUBLISHED: 31 December 2024
CITATION: G. Piaditis, G. Kaltsas, et al., 2024. Appraisal of Modified Tests for Diagnosis and Treatment of Primary Aldosteronism: A Single Center Experience. Medical Research Archives, (online) 12(12).https://doi.org/10.18103/mra.v12i12.6161
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v12i12.6161
ISSN 2375-1924
Abstract
Introduction: Primary aldosteronism (PA), the most common endocrine cause of secondary hypertension, is generally under diagnosed using current diagnostic tests.
Objective: To present our findings, based on studies using modified diagnostic tests, on the diagnosis, prevalence and treatment of PA.
Design and Methods: We prospectively studied 992 hypertensive patients and 278 matched controls. Participants underwent conventional confirmatory tests for the diagnosis of PA modified by the addition of dexamethasone including the Fludrocortisone Dexamethasone Suppression Test (FDST), the Dexamethasone Captopril Valsartan Test (DCVT) and the Dexamethasone Saline Infusion Test (DSIT). Normal cut-offs of basal aldosterone-to-renin ratio and post-test (FDST, DCVT and DSIT) aldosterone levels and aldosterone-to-renin ratio were calculated from the control groups, who had normal adrenal imaging.
Results: Hypertensive patients had significantly higher baseline blood pressure and lower serum potassium levels compared to controls. Using the basal aldosterone-to-renin ratio as screening test, the prevalence of PA was 17.8%. After applying the modified tests to all patients, the prevalence of PA was 33.4%. Targeted treatment with Mineralocorticoid Receptor Antagonists was administered in 252 hypertensives, with bilateral PA; 188 (74.6%) of them obtained a biochemical response and normalization of blood pressure. Unilateral disease had 48 patients who underwent laparoscopic adrenalectomy obtaining a biochemical success rate was 94%.
Conclusion: Our modified methodology and the use of normotensive controls for calculation of normal cut-offs of aldosterone suppression, significantly improves the sensitivity and specificity of the existing tests on the diagnosis of PA, allowing the detection of milder forms.
Keywords
Primary aldosteronism, hypertension, aldosterone, diagnosis, treatment
Introduction
Primary aldosteronism (PA) was first described in 1955 and since then it has been considered as the most common cause of endocrine hypertension. Based on the diagnostic workup recommended by the Endocrine Society Clinical Practice Guidelines, the aldosterone to renin ratio (ARR) serves as a screening test, followed by a confirmatory test, such as the oral sodium loading test (OSL), saline infusion test (SIT), fludrocortisone suppression test (FST), or captopril challenge test (CCT). Consequently, the estimated prevalence of PA ranges between 4.6-16.6%.
However, emerging data support the concept that the prevalence of PA in arterial hypertension could be much higher. This is in line with observational clinical studies where mineralocorticoid receptor antagonists (MRAs) administration can decrease Blood Pressure (BP) levels by 20-30 mmHg in 80% of patients with essential hypertension.
In previous publications we have identified some potential reasons that could account for the lower prevalence rates of PA in previous compared to recent studies. Such factors are the use of ARR as a screening test, the unaccounted adrenocorticotrophin (ACTH) effect on aldosterone secretion and the absence of appropriate control groups in studies that validated the diagnostic tests of PA.
Over the last 14 years, we have modified the currently recommended confirmatory PA diagnostic tests by performing all tests following dexamethasone administration and by keeping serum potassium levels within strict normal limits, in a normotensive population with normal adrenal imaging. This approach enabled us to obtain normal cut-off levels of adequate aldosterone suppression. After applying these cut-offs in hypertensive patients the prevalence of PA increased to 28-32%.
In the present manuscript, we present an overview of the results of 14-year duration of prospective studies on the diagnosis and prevalence of PA that were validated by the outcomes of targeted treatment.
Subjects and methods
During the period between 2007 to 2021, we studied 992 hypertensive patients (631 women, 63.6%) and 278 (185 women, 66.5%) age -, sex- and body mass index (BMI) matched controls (Figure 1, Table 1). The modified tests used and the selection of patients have been described in our previous publications.

| FDST | PATIENTS MEAN±SD | FDST CONTROLS MEAN±SD | p | DCVT | PATIENTS MEAN±SD | DCVT CONTROLS MEAN±SD | p | DSIT | PATIENTS MEAN±SD | DSIT CONTROLS MEAN±SD | p |
|---|---|---|---|---|---|---|---|---|---|---|---|
| N | 444 | 113 | N | 548 | 104 | N | 133 | 61 | |||
| AGE (years) | 54.7±9.0 | 53.8±8.4 | NS | AGE (years) | 55.4±10.8 | 54.0±12.4 | NS | AGE (years) | 54.1±8.8 | 53.5±1.6 | NS |
| BMI (Kg/m2) | 29.0±4.7 | 28.0±6.7 | NS | BMI (Kg/m2) | 29.7±5.0 | 29.5±5.2 | NS | BMI (Kg/m2) | 29.8±4.9 | 27.7±3.9 | NS |
| SBP (mmHg) | 151±16.0 | 119.0±12.0 | <0.001 | SBP (mmHg) | 152.9±21.3 | 138.4±14.7 | <0.001 | SBP (mmHg) | 150.0±15.9 | 125.8±1.1 | <0.001 |
| DBP (mmHg) | 91.9±10.0 | 77.0±7.5 | <0.001 | DBP (mmHg) | 91.4±13.5 | 84.0±10.7 | <0.001 | DBP (mmHg) | 89.7±11.2 | 78.3±0.7 | <0.001 |
| K+ (mmol/L) | 4.03±0.4 | 4.2±0.4 | 0.01 | K+ (mmol/L) | 3.9±0.4 | 4.0±0.3 | 0.01 | K+ (mmol/L) | 4.0±0.4 | 4.3±0.1 | <0.001 |
| Na+ (mmol/L) | 141±3.0 | 142.0±2.2 | 0.01 | Na+ (mmol/L) | 140±2.5 | 139.4±1.6 | 0.04 | Na+ (mmol/L) | 140.9±2.5 | 142.8±0.4 | 0.01 |
| UrNa+ (mEq/24h) | 142.0±61.0 | 149.0±57.0 | NS | UrNa+ (mEq/24h) | 141.6±62.8 | 140.6±56.7 | NS | UrNa+ (mEq/24h) | 145.9±70.6 | 121.6±8.0 | <0.001 |
| UrK+ (mEq/24h) | 65.6±37.0 | 57.0±20.0 | NS | UrK+ (mEq/24h) | 62.9±24.3 | 58.8±21.3 | NS | UrK+ (mEq/24h) | 72.6±56.2 | 59.1±3.1 | <0.001 |
| UrK+/UrNa+-24h | 0.5±0.2 | 0.4±0.1 | 0.01 | UrK+/UrNa+-24h | 0.5±0.2 | 0.5±0.2 | NS | UrK+/UrNa+-24h | 0.5±0.3 | 0.5±0.2 | NS |
Controls
All participants who served as controls had normal adrenal morphology on abdominal computerized tomography (CT) or magnetic resonance imaging (MRI). Among the 278 controls, 174 had normal BP (normotensive control group: NC) and 104 were hypertensive (hypertensive control group: HC), (66 women, 63.5%). Normal BP was defined as a systolic BP (SBP) of less than 135mmHg and diastolic BP (DBP) less than 85mmHg, measured at the outpatient unit on at least 3 consecutive visits (mean of 3 measurements).
One-hundred and thirteen subjects of the normotensive control group (77 women, 68.2%), underwent the Fludrocortisone-Dexamethasone-Saline loading Test (FDST) and were used to establish the cut-off levels of normal aldosterone suppression, also serving as controls (C-FDST) for hypertensive patients who underwent the FDST. A further 61 subjects (42 females, 68.6%), underwent a Dexamethasone-Saline infusion Test (DSIT) and were used to define the cut-off levels of normal aldosterone suppression on DSIT, also serving as controls (C-DSIT) for the DSIT-group of hypertensive patients.
One hundred and four patients of the hypertensive control group (66 women, 63.5%) served as controls (C-DCVT) for the Dexamethasone-Captopril-Valsartan-Test (DCVT)-group of hypertensive patients, as the DCVT can only be applied in hypertensive individuals to avoid further lowering of BP in normotensives. DCVT is performed as follows: all participants received 2mg dexamethasone, 50mg captopril and 320mg valsartan at midnight. Next morning, an extra dose of 50mg captopril was given 1-hour before blood sampling, for measurement of cortisol (COR), aldosterone (ALD), renin (REN), ACTH, and potassium levels. All blood samples were drawn with the participants remaining seated in a non-stressful environment for at least 30 min. In this subgroup of hypertensive controls PA had been excluded as they were first tested for adequate aldosterone suppression on the FDST which is considered the gold standard test as it had been validated with normotensive controls.
Hypertensive patients
Among the 992 hypertensive patients, 444 (301 women, 67.8%) underwent the FDST (H-FDST group), 548 (320 women, 58.4%) the DCVT (H-DCVT group) whereas 133 patients (87 women, 65.4%) from the FDST group also underwent the DSIT (H-DSIT group).
Adrenal venous sampling (AVS) was not available in our department. Therefore, following hormonal evaluation, treatment with MRAs was offered to patients with a diagnosis of PA, with or without bilateral adrenal adenomas or in those with a single adrenal adenoma who were not operated upon. Treatment with laparoscopic adrenalectomy was offered in patients with PA who were thought to have unilateral disease based on the following criteria: 1) history of hypertension at an age < 35 years, regardless of the time that anti-hypertensive treatment was initiated. 2) two consecutive CT scans, at least one year apart showing normal morphology of the contralateral adrenal gland and 3) failure of medical treatment with MRAs to control BP at doses higher than 200mg. They were all re-evaluated regarding persistence of autonomous aldosterone secretion postoperatively.
Further antihypertensive treatment with calcium channel blockers (CCB) or/and small doses of β-blockers was administered in patients with inadequate BP control on MRAs. Patients were asked to monitor their BP at home for 7 days before their regular appointments and they were followed up every 6 months for 26 to 30 months (range 4–127).
All patients had the basal ARR calculated pre- and post-operatively. Post-operatively, the DSIT was used to diagnose persistent PA, only in those PA patients where the renin-angiotensin-aldosterone system (RAAS) had completely recovered. In addition, the use of dexamethasone in all modified tests permitted the simultaneous investigation for autonomous cortisol secretion, in all hypertensive patients. Following testing, cortisol levels > 50 nmol/L without signs and symptoms of overt Cushing’s syndrome indicated mild autonomous cortisol secretion (MACS), as recently defined. Home BP monitoring was used to assess the BP status as described previously.
Hormonal measurements
Hormonal measurements for ALD, REN, ACTH and cortisol were performed as described previously.
Statistical analysis
Statistical analysis was performed using the IBM SPSS v. 25 (IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0, Armonk, NY: IBM Corp). Continuous variables are presented as mean ± SD. Categorical variables are presented as absolute and relative (%) frequencies. Kolmogorov–Smirnov test was used to test normality of the data. The student t-test and the Mann–Whitney test was used to compare continuous variables between 2 groups, while one-way ANOVA and Kruskal–Wallis test were used for comparisons between 3 or more groups. Categorical variables were compared with the chi-squared test. Pearson and Spearman’s correlation coefficients were obtained to evaluate correlations between continuous variables. Univariate and multivariate linear regression models were performed to search for variables associated with basal ALD, basal ARR, basal ACTH and basal F, as well as ALD and ARR- post-DCVT, post-FDST and post-DSIT. Receiver operating characteristic (ROC) curves have been applied to assess the sensitivity and specificity of the post-FDST, post-DSIT and DVCT ARR and ALD levels. In all cases, a two tailed p value <0.05 was considered as statistically significant.
Results
The characteristics of all the hypertensive patients who underwent the modified tests to document PA, divided in three groups according to the test applied (FDST, DCVT and DSIT) and their corresponding control groups are shown in Table 1. Overall, patients of all these three groups had significantly higher baseline SBP/DBP and lower serum K+ levels compared with their corresponding controls.
A significant reduction in ALD, ACTH and COR levels, as well as the ARR in both hypertensive patients and controls was observed after the application of all modified tests.
| FDST | BEFORE MEAN±SD | AFTER MEAN±SD | p | DCVT | BEFORE MEAN±SD | AFTER MEAN±SD | p | DSIT | BEFORE MEAN±SD | AFTER MEAN±SD | p |
|---|---|---|---|---|---|---|---|---|---|---|---|
| N | 444 | 444 | N | 548 | 548 | N | 137 | 137 | |||
| REN (mU/L) | 12.4±11.5 | 6.1±5.5 | <0.001 | REN (mU/L) | 12.4±12.6 | 41.4±74.5 | <0.001 | REN (mU/L) | 13.0±13.3 | 7.6±5.7 | <0.001 |
| ALD (pmol/L) | 392.0±343.0 | 131.6±140.7 | <0.001 | ALD (pmol/L) | 310.0±245.0 | 135.5±159.0 | <0.001 | ALD (pmol/L) | 453.0±537.5 | 140.0±156 | <0.001 |
| ARR (mU/L) | 45.1±44.4 | 26.5±31.0 | <0.001 | ARR (mU/L) | 37.0±35.3 | 17.9±32.5 | <0.001 | ARR (mU/L) | 63.7±115.0 | 26.9±46.0 | <0.001 |
| ACTH (pg/ml) | 22.0±13.5 | 5.8±1.7 | <0.001 | ACTH (pg/ml) | 20.5±13.6 | 6.0±1.9 | <0.001 | ACTH (pg/ml) | 21.2±13.5 | 6.2±4.5 | <0.001 |
| COR (nmol/L) | 436.0±162.0 | 42.3±55.6 | <0.001 | COR (nmol/L) | 397.0±149.5 | 55.0±46.0 | <0.001 | COR (nmol/L) | 456.0±190.0 | 37.4±31.9 | <0.001 |
Hormonal levels in control groups before and after FDST, DCVT and DSIT.
| N | BEFORE | MEAN±SD | AFTER | MEAN±SD | p |
|---|---|---|---|---|---|
| 113 | REN (mU/L) | 15.3±10.6 | 5.1±2.4 | <0.001 | |
| 104 | ALD (pmol/L) | 227.0±161.0 | 47.3±18.2 | <0.001 | |
| 61 | ARR (mU/L) | 19.2±14.8 | 10.5±4.7 | <0.001 | |
| 113 | ACTH (pg/ml) | 23.8±15.7 | 5.6±1.7 | <0.001 | |
| 61 | COR (nmol/L) | 487.0±174.6 | 31.0±17.0 | <0.001 |
Imaging studies
Among the 332 hypertensive patients with PA, 65 (19.5%) had a single (25 left adrenal), 15 (4.5%) bilateral adrenal adenomas and 252 had normal adrenal morphology.
Normal cut offs.
The normal cut-offs of basal ARR and post-test (FDST, DCVT and DSIT) ALD levels and ARR indicative of normal ALD secretory dynamics were calculated using the 97.5 percentiles, based on the hormonal measurements obtained from the three control groups (278 participants).
The normal cut-off for basal ARR was 64 pmol/ mU; post-FDST ALD levels 85pmol/L and ARR 25 pmol/mU; post-DCVT ALD levels 85 pmol/L and ARR 9 pmol/mU; post-DSIT ALD levels 67 pmol/L and ARR 9 pmol/mU.
| N | UNL | PA PATIENTS >UNL | SENSITIVITY (%) | NO-PA PATIENTS <UNL | SPECIFICITY (%) | PREVALENCE (%) | ||
|---|---|---|---|---|---|---|---|---|
| FDST | POST-FDST ALD (pmol/L)/ POST-FDST ARR (pmol/mU) | 444 | 85/25 | 146 | 146/146 (100) | 298 | 298/298 (100) | 146/444 (32.90) |
| POST-FDST ALD (pmol/L) | 444 | 85 | 146 | 146/146 (100) | 206 | 206/298 (69.00) | 146/444 (32.90) | |
| POST-FDST ARR (pmol/mU) | 444 | 25 | 146 | 146/146 (100) | 293 | 295/298 (98.30) | 146/444 (32.90) | |
| BASAL ARR (pmol/mU) | 444 | 64 | 83 | 83/146 (56.80) | 268 | 268/298 (90.00) | 83/444 (18.70) | |
| DCVT | POST-DCVT ALD (pmol/L)/ ARR (pmol/mU) | 548 | 85/9 | 186 | 186/186 (100) | 362 | 362/362 (100) | 186/548 (34.00) |
| POST-DCVT ALD (pmol/L) | 548 | 85 | 186 | 186/186 (100) | 276 | 276/362 (76.20) | 186/548 (34.00) | |
| POST-DCVT ARR (pmol/mU) | 548 | 9 | 186 | 186/186 (100) | 347 | 347/362 (96.00) | 186/548 (34.00) | |
| BASAL ARR (pmol/mU) | 548 | 64 | 95 | 95/186 (51.00) | 346 | 346/362 (95.60) | 95/548 (17.30) | |
| DSIT | POST-DSIT ALD + ARR (pmol/mU) + (pmol/L) | 133 | 67/9 | 46 | 46/46 (100) | 87 | 87/87 (100) | 45/133 (34.50) |
| POST-DSIT ALD (pmol/L) | 133 | 67 | 46 | 46/46 (100) | 59 | 59/87 (67.80) | 45/133 (33.80) | |
| POST-DSIT ARR (pmol/mU) | 133 | 9 | 46 | 46/46 (100) | 76 | 76/87 (87.30) | 46/133 (33.80) | |
| BASAL ARR (pmol/mU) | 133 | 64 | 25 | 25/46 (54.30) | 80 | 80/87 (91.20) | 25/133 (18.70) |
The diagnosis of PA was made when both the post-test ALD and ARR levels were higher than the normal cut-off levels for each test separately. Ninety-two (30.9%) hypertensives had elevated post-FDST ALD levels with normal post-FDST ARR ratio and 5 (1.7%) had elevated post-FDST ARR ratios and normal post-FDST ALD. Eighty-six (23.7%) hypertensives had elevated post-DCVT ALD with normal post-DCVT ARR ratios and 5 (1.4%) had elevated post-DCVT ARR ratios and normal post-DCVT ALD. Twenty-eight (32.2%) hypertensives had elevated post-DSIT ALD with normal post-DSIT ARR ratios and 11 (12.6%) had elevated post-DSIT ARR ratios and normal post-DSIT ALD. Based on our diagnostic criteria, PA in these patients was excluded.
Twenty-three out of 65 (35%) hypertensive patients with PA and a single adrenal adenoma had concomitant MACS on either DSIT or DCVT.
Prevalence of PA
A total of 332 hypertensive patients tested with either FDST, DCVT or DSIT, were diagnosed with PA giving a prevalence of 32.9%, 34%, and 34.5% respectively and an overall prevalence of PA of 33.47% (sensitivity and specificity 100%). Using the basal ARR as a screening test and following the FDST, DCVT and DSIT, the prevalence of PA was 18.7%, 17.3% and 18.7% respectively, associated with a low sensitivity of 51-56.8% and a high specificity of 90-95.6%.
Correlations
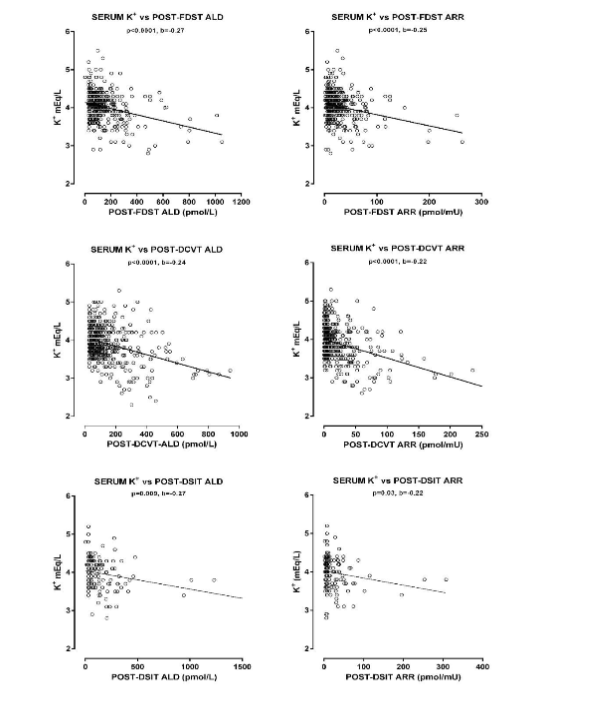
Univariate and multivariate linear regression models were performed to search for variables associated with basal, as well as post-tests (DCVT, FDST, DSIT) ALD levels and ARR.
<td<0.001
| Univariate linear regression model | Multivariate regression model | |
|---|---|---|
| SBP | 0.08 | 0.06 |
| DPB | 0.01 | 0.09 |
| K+ | <0.001 | -0.20 |
| Na+ | 0.04 | 0.07 |
| UrK+-24h | <0.001 | 0.17 |
| UrNa+-24h | 0.6 | 0.03 |
| UrK+/UrNa+-24h | 0.27 | |
| K+ | -0.16 | <0.001 |
| UrK+/UrNa+-24h | 0.27 |
Post-DCVT ALD levels and ARR. In the univariate linear regression model, SBP, DBP, K+, Na+, UrK+, UrK+/UrNa+ independently correlated with both post-DCVT ALD levels and ARR. In the multivariate model only K+ and UrK+/UrNa+ still remained significant.
Post-FDST ALD levels and ARR. In the univariate linear regression model, DBP, K+, UrK+ and UrK+/UrNa+ independently correlated with both post-FDST ALD levels and ARR, while SBP additionally correlated with post-FDST ARR. In the multivariate model, only K+ and UrK+/UrNa+ correlated with both post-FDST ALD levels and ARR.
Post-DSIT ALD levels and ARR. In the univariate linear regression model, DBP, K+, UrK+ and UrK+/UrNa+ independently correlated with post-DSIT ALD levels, while only K+ and UrK+/UrNa+ correlated with the post-DSIT ARR. In the multivariate model K+ and UrK+/UrNa+ correlated with post-DSIT ALD levels and ARR.
Treatment
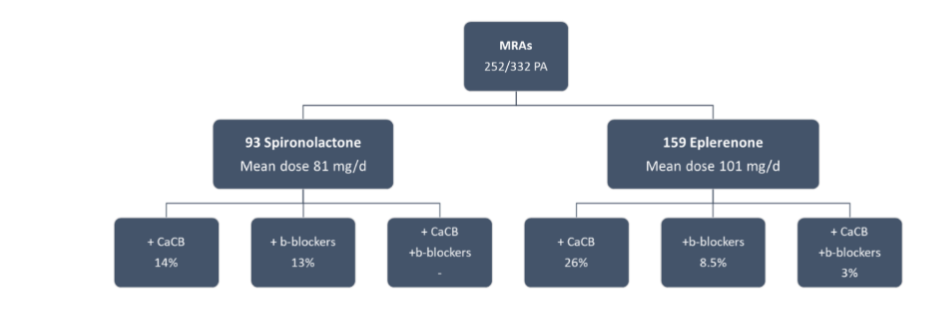
Of the 332 patients with PA 252 (76%) were treated with MRAs, 48 (15%) with adrenalectomy and 32 (10%) were lost to follow up.

Targeted antihypertensive therapy with MRAs was given to 252 PA patients, mainly without adrenal adenomas, aiming to maintain BP, serum K+ and renin levels within the normal limits. The observed complete success rate was 89.3% (225/252), which is very close to that observed in PA patients who underwent surgical treatment.
A cohort of 48 hypertensive patients with PA who were thought to have unilateral disease, received treatment with laparoscopic adrenalectomy and were re-evaluated postoperatively. The BP control, pre- and post-surgery, in patients with biochemical control is shown in Table 5.
| Number of antihypertensive tablets | Pre-surgery | Post-surgery |
|---|---|---|
| 0 | 15 | 26 |
| 1 | 23 | 13 |
| 2 | 7 | 5 |
| 3 | 3 | 1 |
| 48 | 45 |
27/48 (56%): Normal BP without treatment
21/48 (44%): Normal BP with either
- Decrease of dose or number of tablets (11)
- No change in treatment (4)
- Increase of dose or number of tablets (5)
- Use of MRAs (1)
Discussion
In the present study, the prevalence of PA in the general hypertensive population was found to be much higher approximately 33.5%, than the 4.6-16.6% currently reported. This finding is of clinical significance, since hypertension is quite common in the general population, while elevated aldosterone levels, may induce significant damage to peripheral organs, either through the elevated BP and/or by direct action. These deleterious aldosterone effects could be prevented with earlier diagnosis and administration of specific therapy.
Indeed, in our studies complete biochemical and clinical control was achieved in 188/252 (74.6%) of patients with bilateral disease who were treated with MRA and in 45/48 (93.8%) of patients with unilateral disease who were treated with adrenalectomy.
A relevant innovation in the methodology employed in our studies is that all diagnostic tests were validated with the use of appropriately selected control groups including normotensive and hypertensive individuals with normal adrenal imaging, considering the high prevalence of adrenocortical adenomas in the general population and the presence of AAS in 13-14%.
In addition, we also consider the potential effect of ACTH, that is a natural regulator of aldosterone secretion, in the performance characteristics of the tests used to document AAS. It is known that even under mild stressful conditions, such as daily physical activities or psychological stressful events, ACTH induces a significant rise in aldosterone secretion. It can thus be speculated that the presence of fluctuating ACTH levels during the application of current diagnostic tests for PA may exert a continuous stimulatory effect in aldosterone secretion, shifting the normal cut-offs of post-test aldosterone levels upwards.
This has clearly been shown in one of our studies where the diagnostic accuracy of the conventional SIT was compared with the modified DSIT test showing that the post-DSIT aldosterone levels and the ARR were approximately two-fold and three-fold lower, respectively, than the corresponding post-SIT values leading to lower cut-offs of aldosterone suppression.
Furthermore, current practice to interpret conventional diagnostic tests of PA by the post-test aldosterone levels alone, without concomitant consideration of the renin levels may also affect the performance characteristics of the tests. As aldosterone secretion is directly depended mainly on serum renin-angiotensin-II levels, the saline loading during the SIT is expected to expand extracellular volume and suppress the post-SIT aldosterone levels. However, the 4-hour saline loading may not be sufficient to induce adequate expansion of the extracellular volume and complete suppression of the RAAS, in all cases. We have recently showed that both the SIT and DSIT failed to suppress renin levels in 23% of controls and 27% of hypertensive patients tested.
Interestingly, in these patients their 24-hour urinary sodium was relatively low (<90 mmol/24h), suggesting that they were under long-standing sodium intake restriction. However, the sensitivity of the tests could also be affected, if not only the post-test aldosterone levels but also the post-test ARR were applied separately. Specifically, using the post-test aldosterone levels alone, a proportion of the patients without PA, ranging from 31%-34%, exhibited inappropriately elevated aldosterone levels diagnostic of PA (false positive results), whereas using the post-test ARR alone this proportion was between 1.7%-12.7%. These patients would have erroneously been considered as having PA if following the suppressive tests aldosterone levels or ARR were employed separately. Similar findings were also observed when employing the same tests in the controls. Therefore, only patients who had both post-test aldosterone levels and post-test ARR higher than the defined normal cut-offs were considered to have PA.
The use of the basal ARR as a screening test is based on the assumption of its high sensitivity. However, ARR normal cut-offs have never been precisely defined using appropriately selected controls. All our modified tests were applied to all controls and hypertensive participants, regardless of the basal ARR. After obtaining normal cut-off values of basal ARR from the NC group we evaluated its diagnostic accuracy and the results showed a sensitivity ranging from 51-57%, whereas the specificity was high, ranging from 90 to 95%. We can thus conclude that the basal ARR cannot be used systematically as a screening test, as a number of patients with PA will remain undiagnosed.
Our results also show that all the modified tests can be used effectively for diagnosing both PA and autonomous cortisol secretion simultaneously. This is of additional importance since there are convincing data showing that autonomous cortisol secretion coexists with PA in a significant percentage of adrenal incidentalomas, ranging from 18%-26.8%. This is further reinforced by a recent study which showed that patients with PA due to an adrenal adenoma have a significant increase in the daily urinary cortisol excretion rate and total glucocorticoid metabolites, compared to normal controls. Hypercortisolaemia, either in the form of autonomous overproduction or in the form of stress hyper-response is related to adverse metabolic and cardiovascular risk factors causing damage to the peripheral organs. Even more, there are recent data showing that the coexistence of autonomous cortisol secretion and PA further enhances the damages caused to peripheral organs. Thus, the secretion of cortisol and aldosterone should be studied simultaneously in all hypertensive patients with PA and an adrenal adenoma, as it is the case with all modified PA diagnostic tests.
The validity of the modified tests is further supported by robust evidence. The multivariate regression analysis of our results showed that both, aldosterone levels and ARR obtained from any modified tests, correlated significantly with serum K+ levels and 24h-urinary K+/Na+ ratio which are directly depended on aldosterone action. Similar correlations were observed in a recent study where the 24-hour urinary aldosterone excretion rate was used for PA diagnosis. Such correlations have never been observed in patients with essential hypertension.
Adrenalectomy performed after AVS is widely accepted as the treatment of choice for unilateral PA, as it is highly effective to cure or mitigate aldosterone excess directly minimizing the associated cardiometabolic risk. However, AVS is cumbersome and not widely available and the decision for adrenalectomy is based on clinical and biochemical indices suggestive of a unilateral source of aldosterone excess. Indications commonly employed are the initiation of arterial hypertension earlier than the 35 years of age, the presence of a single adrenal adenoma at subsequent imaging and the failure of medical treatment with MRAs, at doses higher than 200 mg/day, to normalize the blood pressure and basal plasma renin levels in PA patients. This approach is in agreement with the findings of the PASO study which reported that the patients who were more likely to obtain clinical benefit from adrenalectomy were those with the higher SBP and higher antihypertensive medication use at baseline. Laparoscopic adrenalectomy in the 48 patients who were considered to have unilateral disease, based on these indications, resulted in restoring their BP, serum K+ and plasma renin levels to normal with a success rate of 94%, which is close to the success rate obtained by the use of AVS for lateralization, ranging from 83 to 100%. Although this observation is promising, further studies are required for better validation.
Targeting medical treatment with either spironolactone or eplerenone was applied to 252 PA patients, mainly without adrenal adenomas, aiming to maintain BP, serum K+ and renin levels within the normal limits. The observed complete success rate was 89.3% (225/252), which is very close to that observed in PA patients who underwent surgical treatment.
Conclusion
We have used a number of modified diagnostic tests to detect of autonomous aldosterone secretion in unselected patients with arterial hypertension. The introduced modifications improved significantly the sensitivity and specificity of the diagnostic tests increasing the prevalence of PA with or without simultaneous cortisol secretion. This permits early diagnosis and targeted treatment of the disease, allowing effective prevention of tissue damage of the target organs.
Conflicts of Interest Statement
The authors have no conflicts of interest to declare.
Funding: None
References
- Conn JW, Louis LH. Primary aldosteronism: a new clinical entity. Trans Assoc Am Physicians. 1955;68:215-231; discussion, 231-233.
- Schirpenbach C, Reincke M. Primary aldosteronism: current knowledge and controversies in Conn’s syndrome. Nat Clin Pract Endocrinol Metab. 2007;3(3):220-227. doi:10.1038/ncpendmet0430
- Funder JW, Carey RM, Mantero F, et al. The Management of Primary Aldosteronism: Case Detection, Diagnosis, and Treatment: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2016;101(5):1889-1916. doi:10.1210/JC.2015-4061
- Stowasser M, Gordon RD, Gunasekera TG, et al. High rate of detection of primary aldosteronism, including surgically treatable forms, after ???non-selective??? screening of hypertensive patients. J Hypertens. 2003;21(11):2149-2157. doi:10.1097/00004872-200311000-00025
- Rossi GP, Bernini G, Caliumi C, et al. A Prospective Study of the Prevalence of Primary Aldosteronism in 1,125 Hypertensive Patients. J Am Coll Cardiol. 2006;48(11):2293-2300. doi:10.1016/j.jacc.2006.07.059
- Young WF. Primary aldosteronism: renaissance of a syndrome. Clin Endocrinol (Oxf). 2007;66(5):607-618. doi:10.1111/j.1365-2265.2007.02775.x
- Douma S, Petidis K, Doumas M, et al. Prevalence of primary hyperaldosteronism in resistant hypertension: a retrospective observational study. The Lancet. 2008;371(9628):1921-1926. doi:10.1016/S0140-6736(08)60834-X
- Stowasser M. Update in Primary Aldosteronism. J Clin Endocrinol Metab. 2009;94(10):3623-3630. doi:10.1210/jc.2009-1399
- Piaditis G, Markou A, Papanastasiou L, Androulakis II, Kaltsas G. PROGRESS IN ALDOSTERONISM: A review of the prevalence of primary aldosteronism in pre-hypertension and hypertension. Eur J Endocrinol. 2015;172(5):R191-R203. doi:10.1530/EJE-14-0537
- Baudrand R, Guarda FJ, Fardella C, et al. Continuum of Renin-Independent Aldosteronism in Normotension. Hypertension. 2017;69(5):950-956. doi:10.1161/HYPERTENSIONAHA.116.08952
- Brown JM, Siddiqui M, Calhoun DA, et al. The Unrecognized Prevalence of Primary Aldosteronism. Ann Intern Med. 2020;173(1):10-20. doi:10.7326/M20-0065
- Levy DG, Rocha R, Funder JW. Distinguishing the Antihypertensive and Electrolyte Effects of Eplerenone. J Clin Endocrinol Metab. 2004;89(6):2736-2740. doi:10.1210/jc.2003-032149
- Piaditis GP, Kaltsas G, Markou A, Chrousos GP. Five Reasons for the Failure to Diagnose Aldosterone Excess in Hypertension. Hormone and Metabolic Research. 2020;52(12):827-833. doi:10.1055/a-1236-4869
- Piaditis GP, Kaltsas GA, Androulakis II, et al. High prevalence of autonomous cortisol and aldosterone secretion from adrenal adenomas. Clin Endocrinol (Oxf). 2009;71(6):772-778. doi:10.1111/j.1365-2265.2009.03551.x
- Gouli A, Kaltsas G, Tzonou A, et al. High prevalence of autonomous aldosterone secretion among patients with essential hypertension. Eur J Clin Invest. 2011;41(11):1227-1236. doi:10.1111/j.1365-2362.2011.02531.x
- Tsiavos V, Markou A, Papanastasiou L, et al. A new highly sensitive and specific overnight combined screening and diagnostic test for primary aldosteronism. Eur J Endocrinol. 2016;175(1):21-28. doi:10.1530/EJE-16-0003
- Markou A, Pappa T, Kaltsas G, et al. Evidence of primary aldosteronism in a predominantly female cohort of normotensive individuals: a very high odds ratio for progression into arterial hypertension. J Clin Endocrinol Metab. 2013;98(4):1409-1416. doi:10.1210/JC.2012-3353
- Fassnacht M, Tsagarakis S, Terzolo M, et al. European Society of Endocrinology clinical practice guidelines on the management of adrenal incidentalomas, in collaboration with the European Network for the Study of Adrenal Tumors. Eur J Endocrinol. 2023;189(1):G1-G42. doi:10.1093/EJENDO/LVAD066
- Fountoulakis S, Papanastasiou L, Voulgaris N, et al. Salt intake in mineralocorticoid receptor antagonist-treated primary aldosteronism: foe or ally? Hormones. 2020;19(2):223-232. doi:10.1007/s42000-019-00167-9
- Papanastasiou L, Markou A, Pappa T, et al. Primary aldosteronism in hypertensive patients: clinical implications and target therapy. Eur J Clin Invest. 2014;44(8):697-706. doi:10.1111/eci.12286
- Stowasser M, Gordon RD, Gunasekera TG, et al. High rate of detection of primary aldosteronism, including surgically treatable forms, after ???non-selective??? screening of hypertensive patients. J Hypertens. 2003;21(11):2149-2157. doi:10.1097/00004872-200311000-00025
- Rossi GP, Bernini G, Caliumi C, et al. A Prospective Study of the Prevalence of Primary Aldosteronism in 1,125 Hypertensive Patients. J Am Coll Cardiol. 2006;48(11):2293-2300. doi:10.1016/j.jacc.2006.07.059
- Young WF. Primary aldosteronism: renaissance of a syndrome. Clin Endocrinol (Oxf). 2007;66(5):607-618. doi:10.1111/j.1365-2265.2007.02775.x
- Stowasser M. Update in Primary Aldosteronism. J Clin Endocrinol Metab. 2009;94(10):3623-3630. doi:10.1210/jc.2009-1399
- Ferreira NS, Tostes RC, Paradis P, Schiffrin EL. Aldosterone, Inflammation, Immune System, and Hypertension. Am J Hypertens. 2021;34(1):15-27. doi:10.1093/ajh/hpaa137
- Turcu AF, Yang J, Vaidya A. Primary aldosteronism — a multidimensional syndrome. Nat Rev Endocrinol. 2022;18(11):665-682. doi:10.1038/s41574-022-00730-2
- Mansmann G, Lau J, Balk E, Rothberg M, Miyachi Y, Bornstein SR. The Clinically Inapparent Adrenal Mass: Update in Diagnosis and Management. Endocr Rev. 2004;25(2):309-340. doi:10.1210/er.2002-0031
- KLOOS RT, GROSS MD, FRANCIS IR, KOROBKIN M, SHAPIRO B. Incidentally Discovered Adrenal Masses*. Endocr Rev. 1995;16(4):460-484. doi:10.1210/edrv-16-4-460
- Arvat E, Di Vito L, Lanfranco F, et al. Stimulatory Effect of Adrenocorticotropin on Cortisol, Aldosterone, and Dehydroepiandrosterone Secretion in Normal Humans: Dose-Response Study*. J Clin Endocrinol Metab. 2000;85(9):3141-3146. doi:10.1210/jcem.85.9.6784
- Markou A, Kaltsas GA, Papanastasiou L, et al. Enhanced performance of a modified diagnostic test of primary aldosteronism in patients with adrenal adenomas. Eur J Endocrinol. 2022;186(2):265-273. doi:10.1530/EJE-21-0625
- Baudrand R, Guarda FJ, Torrey J, Williams G, Vaidya A. Dietary Sodium Restriction Increases the Risk of Misinterpreting Mild Cases of Primary Aldosteronism. J Clin Endocrinol Metab. 2016;101(11):3989-3996. doi:10.1210/jc.2016-1963
- Nakamura Y, Maekawa T, Felizola SJA, et al. Adrenal CYP11B1/2 expression in primary aldosteronism: Immunohistochemical analysis using novel monoclonal antibodies. Mol Cell Endocrinol. 2014;392(1-2):73-79. doi:10.1016/j.mce.2014.05.002
- Arlt W, Lang K, Sitch AJ, et al. Steroid metabolome analysis reveals prevalent glucocorticoid excess in primary aldosteronism. JCI Insight. 2017;2(8). doi:10.1172/jci.insight.93136
- Fallout F, Sonino N. Should we evaluate for cardiovascular disease in patients with Cushing’s syndrome? Clin Endocrinol (Oxf). 2009;71(6):768-771. doi:10.1111/j.1365-2265.2009.03610.x
- Androulakis II, Kaltsas GA, Kollias GE, et al. Patients with apparently nonfunctioning adrenal incidentalomas may be at increased cardiovascular risk due to excessive cortisol secretion. J Clin Endocrinol Metab. 2014;99(8):2754-2762. doi:10.1210/JC.2013-4064
- Nakajima Y, Yamada M, Taguchi R, et al. Cardiovascular complications of patients with aldosteronism associated with autonomous cortisol secretion. J Clin Endocrinol Metab. 2011;96(8):2512-2518. doi:10.1210/JC.2010-2743
- Tang L, Li X, Wang B, et al. Clinical Characteristics of Aldosterone- and Cortisol-Coproducing Adrenal Adenoma in Primary Aldosteronism. Int J Endocrinol. 2018;2018:1-9. doi:10.1155/2018/4920841
- Ohno Y, Sone M, Inagaki N, et al. Latent Autonomous Cortisol Secretion From Apparently Nonfunctioning Adrenal Tumor in Nonlateralized Hyperaldosteronism. J Clin Endocrinol Metab. 2019;104(10):4382-4389. doi:10.1210/jc.2018-02790
- Inoue K, Kitamoto T, Tsurutani Y, Saito J, Omura M, Nishikawa T. Cortisol Co-Secretion and Clinical Usefulness of ACTH Stimulation Test in Primary Aldosteronism: A Systematic Review and Biases in Epidemiological Studies. Front Endocrinol (Lausanne). 2021;12. doi:10.3389/fendo.2021.645488
- Williams TA, Lenders JWM, Mulatero P, et al. Outcomes after adrenalectomy for unilateral primary aldosteronism: an international consensus on outcome measures and analysis of remission rates in an international cohort. Lancet Diabetes Endocrinol. 2017;5(9):689-699. doi:10.1016/S2213-8587(17)30135-3
- Schneider H, Williams TA, Heinrich DA, Lechner B, Reincke M. Primary aldosteronism long-term outcome: Medical versus surgical therapy. Curr Opin Endocr Metab Res. 2019;8:132-138. doi:10.1016/j.coemr.2019.08.008
- Funder JW, Carey RM, Mantero F, et al. The Management of Primary Aldosteronism: Case Detection, Diagnosis, and Treatment: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2016;101(5):1889-1916. doi:10.1210/jc.2015-4061
- Williams TA, Burrello J, Sechi LA, et al. Computed Tomography and Adrenal Venous Sampling in the Diagnosis of Unilateral Primary Aldosteronism. Hypertension. 2018;72(3):641-649. doi:10.1161/HYPERTENSIONAHA.118.11382