

Monitoring Sepsis Outcomes with Neutrophil Biomarkers
Monitoring and outcome prediction of sepsis by neutrophil specific biomarkers
Per Venge1, Shengyuan Xu1
OPEN ACCESS
PUBLISHED: 30 December 2024
CITATION: VENGE, Per; XU, Shengyuan. Monitoring and outcome prediction of sepsis by neutrophil specific biomarkers. Medical Research Archives, [S.l.], v. 12, n. 12, dec. 2024.Available at: <https://esmed.org/MRA/mra/article/view/6202>.
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.18103/mra.v12i12.6202
ISSN 2375-1924
Abstract
HNL (human Neutrophil Lipocalin) is a protein secreted from the activated neutrophil granulocytes but also from epithelial cells. HNL is measured by sensitive immunoassays in most bodily fluids and exists in several variants of which the monomer and the dimer variants are the most abundant. Depending on the antibody configuration of the immunoassays we may detect different molecular variants of HNL, and which may have different cellular origins. The dimeric form of HNL is entirely neutrophil specific and other assays may preferentially detect HNL originating from epithelial cells such as the tubular cells of the kidney. In this brief review we have focused on the utility of HNL as a biomarker for antibiotics stewardship in patients with sepsis and show that the dimeric form of HNL is reduced within 24 hours as the response to successful antibiotic treatment in sepsis in contrast to the reduction of blood levels of procalcitonin and heparin-binding protein which takes 3-4 days. Another variant of HNL showed to be the most powerful predictor of outcome of these patients. We conclude that the measurements of these HNL variants should be considered for implementation in intensive care units and other settings with seriously ill infected patients.
Keywords
sepsis, biomarkers, neutrophil, HNL, outcome prediction
Introduction
Sepsis is probably the costliest human disease globally. The mortality is high unless treated rapidly and extensively. The diagnosis of sepsis is defined by the Sepsis3 criteria¹ and in most cases due to a bacterial infection. Outcome of the disease is determined by effective antibiotics treatment for the avoidance of organ failure. Important clinical questions asked are: is our treatment effective and can we predict the outcome of our patient? Several blood and urine biomarker assays have been developed and used clinically in the attempt to answer these questions, however, with varying success²˒³. The most commonly used biomarkers in this regard are procalcitonin and heparin-binding protein in addition to blood cell counts, CRP and biomarkers reflecting kidney function. In this short review we will summarize the results of measuring the biomarker HNL and its variants in blood and urine in various severe infections. Thus, the measurement of HNL, which is entirely neutrophil specific, shows great promise as a monitoring tool of successful antibiotics treatment in sepsis and another variant of HNL⁴˒⁵, that mainly originates from epithelial cells, appears useful in the outcome prediction due to organ failure. For more comprehensive reviews on HNL/Lipocalin2/NGAL we refer to the vast literature published in recent years³˒⁶˒¹⁸.
Human Neutrophil Lipocalin
Human Neutrophil Lipocalin was originally purified from human neutrophil granulocytes in the early 90-tieth and called Human Neutrophil Lipocalin¹⁹, since the primary structure identified the protein as a member of the lipocalin family of proteins. Other research groups also identified the protein during this period and gave the protein many different names of which LNC2(Lipocalin2)²⁰ and NGAL (Neutrophil Gelatinase Associated lipocalin)¹⁸˒²¹ are the best known as of today. The name NGAL indicated that the protein has an affinity for Gelatinase (MMP9, Matrix metalloproteinase-9). The binding of HNL to MMP9 is one reason for the apparent heterogeneity of HNL when measured in blood and other biological materials. Thus, HNL exists in various materials as a monomer of 25 kD, as a dimer of 45 kD and as heteromers in complex with MMP9 and other unidentified proteins with molecular weights exceeding 90 kD²¹. The function of HNL is still uncertain although many suggestions have been made that indicate a role in bacterial defence and iron-metabolism.
As mentioned, we originally purified HNL from human neutrophils of healthy blood donors. HNL is located in the secondary granules of these cells and secreted from neutrophils upon exposure to bacteria or bacteria-derived peptides such as the tripeptide fMLP, but also as a response to other molecules such as inflammatory cytokines²². Another source of HNL is epithelial cells in the kidney, intestine, lungs etc. The expression of HNL in these cells is very much increased in inflammation²³. The heterogeneity of HNL is a great challenge but also an opportunity when we measure the marker in biological fluids. The challenge is to secure great interpretability of the cellular origin of HNL when we measure changes in concentrations and the opportunity is the fact that different configurations of immunoassays of HNL may reflect differences in cellular origins. The most conspicuous example of this is the exclusive neutrophil origin of the dimeric form of HNL, which means that any change in concentrations of this variant specifically reflects the secretory activity of this cell⁴˒⁵. We also found that raising monoclonal and polyclonal antibodies against native HNL created antibodies with a variety of epitope specificities. When combining these antibodies in our different immunoassays we saw that the clinical performances showed great differences which likely reflect the fact that the different variants of HNL appear in different proportions in different diseases and in different biological material⁹. Most commercially available NGAL (HNL) assays seem to be based on recombinant material and preferentially measure the monomeric form of the protein.
HNL (NGAL) as biomarker of acute kidney injury
The concentrations of HNL (NGAL) in blood or urine largely reflect the condition of the kidney and have been shown highly elevated in acute kidney injury (AKI). As such the measurement of NGAL has established itself as a potentially useful clinical means to monitor kidney function. However, the usefulness of NGAL in this regard is under debate and not supported by some clinical studies which might be due to the use of different NGAL assays with differences in epitope recognitions²⁴˒²⁵. In one of our own studies on AKI in COVID-19 patients we saw that one of our HNL assays (763/8F) was superior to an established NGAL assay as one example of the importance of such differences (Table 1)²⁶. Thus, for the comparisons of performances, as reflections of kidney function, it seems important to define the NGAL/HNL assays in terms of antibody epitope recognition or alternatively compare the clinical performances of a number of NGAL/HNL immunoassays in a large set of clinical samples from patients with defined stages of AKI.
Table 1 The diagnostic performances of plasma concentrations of HNL (763/8F) and NGAL in COVID-19 patients in severe AKI, yes or no.
| Severe AKI Day 1 | Variable | AUC | 95% CI |
|---|---|---|---|
| P-HNL (763/8F) | 0.759 | 0.662 to 0.840 | |
| P-NGAL | 0.581 | 0.477 to 0.681 |
| Severe AKI Day 3 | Variable | AUC | 95% CI |
|---|---|---|---|
| P-HNL (763/8F) | 0.859 | 0.746 to 0.935 | |
| P-NGAL | 0.769 | 0.643 to 0.867 |
Plasma samples were obtained at admission day and at day 3 after admission. Area under the curve (AUC) and 95% confidence intervals (CI) are shown. The AUCs were significantly higher for P-HNL (763/764) as compared to the AUC of NGAL at both days, p=0.01 and p=0.03, respectively (Adopted from reference²⁶).
In our recent sepsis study the HNL assay (pab/765) was highly statistically and independently related to outcome of the patients in comparisons to other biomarkers including NGAL whereas the neutrophil specific dimeric form of HNL showed a weaker relation to outcome⁴.
HNL in the distinction between bacterial and viral causes of acute infections
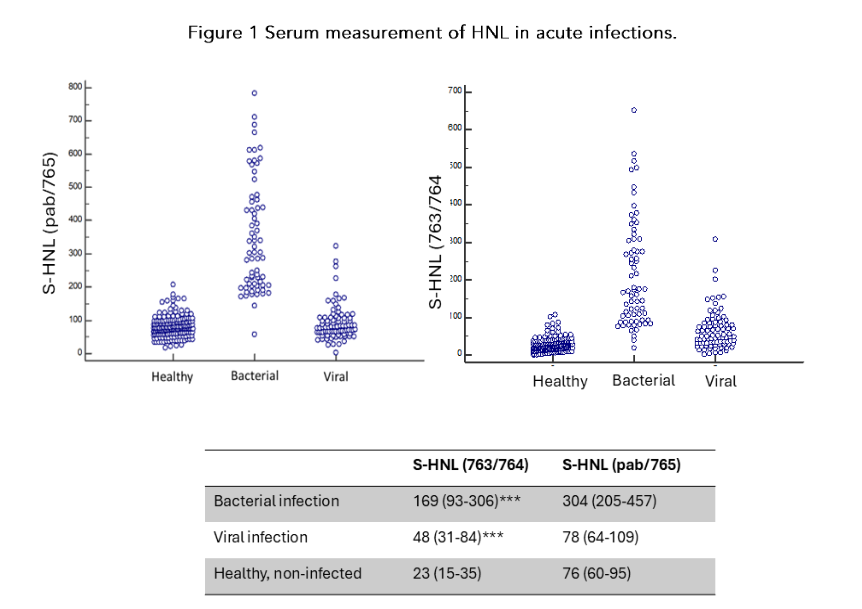
HNL has been measured in serum/plasma and after whole blood activation in patients with various kinds of infections. In the early days serum was the preferred blood material and HNL concentrations showed very good distinctions between acute bacterial and viral infections with sensitivities and specificities of about 90% and clearly superior to other biomarkers such as cell counts, procalcitonin, CRP²⁷. *This data was confirmed in large studies in China and also indicated the importance of antibody configuration of the HNL assay in order to achieve optimal discrimination (fig 1)*²⁸˒²⁹.
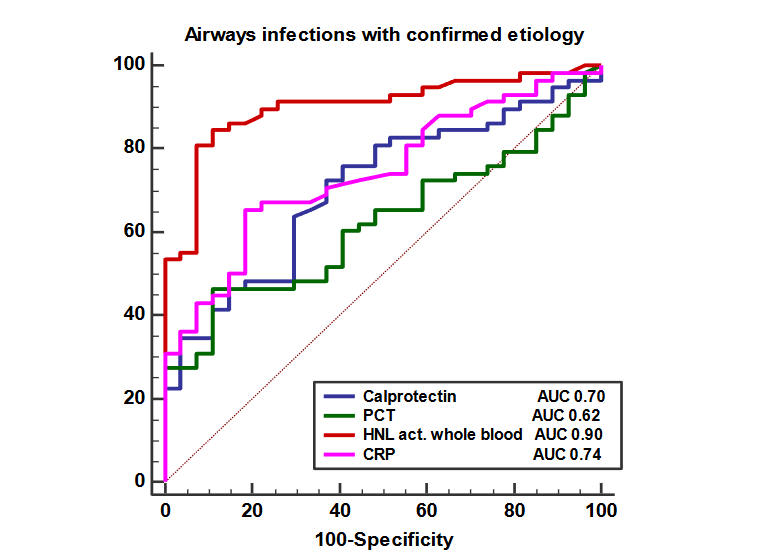
The measurement in serum requires strict standardization as to temperature and time of handling of the whole blood during clotting. This is because the neutrophils present in the blood will continue to release some of its HNL outside the cell during clotting and therefore add to HNL already present in the plasma. In the busy clinical settings such standardization requirements are difficult to cope with and we have therefore developed an alternative method that eliminates this problem, and which lends itself to the development of point-of-care devices. In this system whole blood is activated by fMLP during 5 minutes at 37°C after which HNL in plasma is measured as a reflection of the activity of the neutrophil. Adopting this procedure, we showed a high clinical performance in the distinction between bacterial and viral infections in the large Bio-X study achieving sensitivity and specificity of about 90%, i.e. in the range of serum measurements³⁰˒³¹. Also, we showed a strong correlation between the serum results and the results of fMLP activation of whole. In the figure (fig 2) the performance is illustrated by the comparison with three other biomarkers commonly measured in patients with symptoms of airways disease.
The superiority of whole blood activation for the measurements of HNL (B-HNL) is also illustrated in table 2 in which we show the comparison with PCT. Only in patients with sepsis the diagnostic performance of PCT approached B-HNL.
Figure 1 Serum measurement of HNL in acute infections.
 Serum measurement of HNL in acute infections.
Serum measurement of HNL in acute infections.
Figure 1 The figure shows the results of the concentrations of HNL in serum obtained from healthy non-infected subjects, from patients with proven bacterial infections and from patients with proven viral infections. The left panel shows the results using the HNL ELISA configured with HNL polyclonal antibody and HNL monoclonal antibody 765 and the right panel the results of using the ELISA configured with the HNL monoclonal antibodies 763 and 764. In the table below we show the actual average concentrations using the two different configurations. It is seen that the concentrations of HNL were higher using the configuration pab/765 than with the configuration 763/764. It is also indicated that in sera from patients with viral infections the HNL concentrations were elevated using the 763/764 as compared to healthy subjects as opposed to the findings with the ELISA using the pab/765 configuration. Results adopted from reference²⁸.
Figure 2 The diagnostic comparison in the distinction between bacterial and viral causes of airways infections
HNL Dimer in sepsis
Important clinically unmet needs in the management of sepsis are tools which quickly indicate the successful response to antibiotic treatment. For this purpose, the measurement of procalcitonin has been very important and applied in most ICU settings. However, the response of blood concentrations of procalcitonin to successful treatment is rather slow and takes 3–4 days before significant changes are seen²³˒³⁴. It was therefore of great interest that we could show in our previous study on patients with sepsis a faster decline in concentrations of the neutrophil specific HNL Dimer as a response to adequate treatment i.e. within 24–48 hours³⁵.
To follow up on these findings we conducted a larger study on 277 patients admitted to the ICU and measured the biomarkers HNL Dimer, HNL Total (pab/765), Heparin-binding protein and Procalcitonin on 3 occasions and on three consecutive days⁴. Also to discriminate between the faster response among signs of sepsis and those fulfilling the Sepsis3 criteria HNL Total (pab/765) showed an AUC (Area Under the Curve) in the ROC-analysis of 0.86 (Sensitivity 81% and specificity 85%). Positive predictive value 93% and negative predictive value 64%) and with a similar AUC of 0.84 (Sensitivity 77% and specificity 77%). Positive predictive value 92% and negative predictive value 48%) for procalcitonin. The other two biomarkers less efficiently identified patients with sepsis. At follow up we saw a significant overall decline in the concentrations of HNL Dimer at the day after admission (Day 2) and a further decline the next day (Day 3). This pattern was not discernible for the other three biomarkers. When calculated on the sepsis patients separately a significant decline was also seen in the concentrations of HNL Total on these days following admission when only paired observations were calculated on, whereas no such pattern was seen for heparin-binding protein or procalcitonin. However, a highly significant decline in the concentrations of HNL Dimer was observed already at the day after admission in the sepsis group whether calculated as paired observations or not.
The HNL Dimer pattern was strikingly different from the other biomarkers. Importantly, the decline in HNL Dimer was most obvious and significant in those who survived the 30 days observation period, whereas no significant decline in HNL Dimer plasma concentrations was observed in the non-surviving group of patients. This finding was true for the whole cohort of ICU patients as well as for the sepsis cohort. In the patients with the very high concentrations of HNL Dimer the reduction was 5–10 fold after one day of successful antibiotics treatment. The object of the Östersund study was to examine whether the fast decline of HNL Dimer in plasma as a response to successful antibiotics treatment could be confirmed³⁵. As shown in the figure (Figure 3) in which the results of the two studies are compared, the decline in plasma concentrations of HNL Dimer was conspicuous in both studies in contrast to the absence of an early response by the concentrations of PCT. These findings should be challenged and confirmed in other studies.
Conclusion
Given the fact that we were able to confirm the potential of plasma HNL Dimer as a clinically useful biomarker for antibiotics stewardship in two independent studies encourages us to suggest that this biomarker should be implemented in intensive care units and in the care of seriously ill and infected patients.
Figure 3 Successful antibiotics monitoring in sepsis
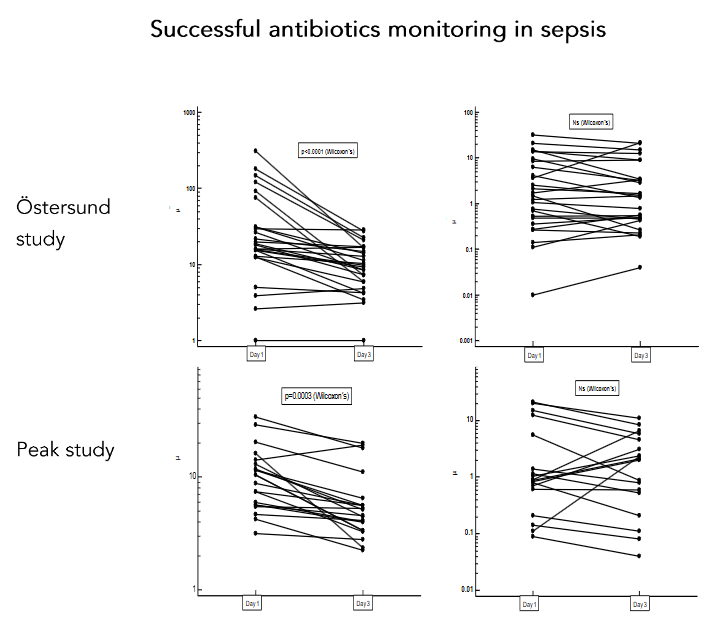
Figure 3. The HNL Dimer was measured by the HNL ELISA (mab 763/765) in EDTA plasma of patients with sepsis at admission (day 1) and after 2 days of successful antibiotics treatment (day 3). Procalcitonin was measured for comparison. We show the results from two different cohorts with sepsis — the Östersund study⁴ and the Peak study³⁵. The statistics is shown on the figure. The results adopted from references ⁴˒³⁵.
References
(1) Singer M, Deutschman CS, Seymour CW et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016; 315(8):801-810.
(2) Saxena J, Das S, Kumar A et al. Biomarkers in sepsis. Clin Chim Acta 2024;562:119891.
(3) Xie Y, Huang P, Zhang J et al. Biomarkers for the diagnosis of sepsis-associated acute kidney injury: systematic review and meta-analysis. Ann Palliat Med 2021.
(4) Venge P, Peterson C, Xu S, Larsson A, Johansson J, Tydén J. HNL Dimer in plasma is a unique and useful biomarker for the monitoring of antibiotic treatment in sepsis. PLOS ONE 2024;In Press.
(5) Venge P, Xu S, Mårtensson J. HNL Dimer-A specific biomarker of neutrophil activity – in sepsis and antibiotic monitoring. A mini-review. Arch Clin Biomed Res 2022;6 (1):145-152.
(6) Albert C, Haase M, Albert A, Zapf A, Braun-Dullaeus RC, Haase-Fielitz A. Biomarker-Guided Risk Assessment for Acute Kidney Injury: Time for Clinical Implementation? Ann Lab Med 2021;41(1):1-15.
(7) Bellos I, Fitrou G, Daskalakis G, Perrea DN, Pergialiotis V. Neutrophil gelatinase-associated lipocalin as predictor of acute kidney injury in neonates with perinatal asphyxia: a systematic review and meta-analysis. Eur J Pediatr 2018;177(10):1425-1434.
(8) Cai L, Borowiec J, Xu S, Han W, Venge P. Assays of urine levels of HNL/NGAL in patients undergoing cardiac surgery and the impact of antibody configuration on their clinical performances. Clin Chim Acta 2009;403(1-2):121-125.
(9) Cai L, Rubin J, Han W, Venge P, Xu S. The Origin of Multiple Molecular Forms in Urine of HNL/NGAL. Clin J Am Soc Nephrol 2010.
(10) Claudel SE, Waikar SS. Systematic Review of Kidney Injury Biomarkers for the Evaluation of CKD of Uncertain Etiology. Kidney Int Rep 2024;9(6): 1614-1632.
(11) Ferreira GS, Frota ML, Gonzaga MJD, Vattimo MFF, Lima C. The Role of Biomarkers in Diagnosis of Sepsis and Acute Kidney Injury. Biomedicines 2024;12(5).
(12) Jaberi SA, Cohen A, D’Souza C et al. Lipocalin-2: Structure, function, distribution and role in metabolic disorders. Biomed Pharmacother 2021;142:112002.
(13) Khawaja S, Jafri L, Siddiqui I, Hashmi M, Ghani F. The utility of neutrophil gelatinase-associated Lipocalin (NGAL) as a marker of acute kidney injury (AKI) in critically ill patients. Biomark Res 2019;7:4.
(14) Marakala V. Neutrophil gelatinase-associated lipocalin (NGAL) in kidney injury – A systematic review. Clin Chim Acta 2022;536:135-141.
(15) Nguyen MT, Devarajan P. Biomarkers for the early detection of acute kidney injury. Pediatr Nephrol 2008;23(12):2151-2157.
(16) Romejko K, Markowska M, Niemczyk S. The Review of Current Knowledge on Neutrophil Gelatinase-Associated Lipocalin (NGAL). Int J Mol Sci 2023;24(13).
(17) Shi K, Jiang W, Song L et al. Persistent acute kidney injury biomarkers: A systematic review and meta-analysis. Clin Chim Acta 2025;564:119907.
(18) Xu S, Venge P. Lipocalins as biochemical markers of disease. Biochim Biophys Acta 2000;1482(1-2): 298-307.
(19) Xu SY, Carlson M, Engstrom A, Garcia R, Peterson CG, Venge P. Purification and characterization of a human neutrophil lipocalin (HNL) from the secondary granules of human neutrophils. Scand J Clin Lab Invest 1994;54:365-376.
(20) Bartsch S, Tschesche H. Cloning and expression of human neutrophil lipocalin cDNA derived from bone marrow and ovarian cancer cells. FEBS Lett 1995;357:255-259.
(21) Kjeldsen L, Bainton DF, Sengelov H, Borregaard N. Identification of neutrophil gelatinase-associated lipocalin as a novel matrix protein of specific granules in human neutrophils. Blood 1994;83 No.3:799-807.
(22) Xu SY, Höglund M, Venge P. The effect of granulocyte colony-stimulating factor (G-CSF) on the degranulation of secondary granule proteins from human neutrophils in vivo may be indirect. Br J Haematol 1996;93(3):558-568.
(23) Schmekel B, Seveus L, Xu SY, Venge P. Human neutrophil lipocalin (HNL) and myeloperoxidase (MPO). Studies of lung lavage fluid and lung tissue. Respir Med 2000;94(6):564-568.
(24) Albert C, Zapf A, Haase M et al. Neutrophil Gelatinase-Associated Lipocalin Measured on Clinical Laboratory Platforms for the Prediction of Acute Kidney Injury and the Associated Need for Dialysis Therapy: A Systematic Review and Meta-analysis. Am J Kidney Dis 2020;76(6):826-841.
(25) Glassford NJ, Schneider AG, Xu S et al. The nature and discriminatory value of urinary neutrophil gelatinase-associated lipocalin in critically ill patients at risk of acute kidney injury. Intensive Care Med 2013;39(10):1714-1724.
(26) Venge P, Xu S, Peterson C et al. Plasma biomarkers associated to outcome in patients with Sars-Cov-2 infection. J Clin Lab Med 2022;7(1):1-8.
(27) Xu SY, Pauksen K, Venge P. Serum measurements of human neutrophil lipocalin (HNL) discriminate between acute bacterial and viral infections. Scand J Clin Lab Invest 1995;55(2):125-131.
(28) Yu Z, Jing H, Hongtao P et al. Distinction between bacterial and viral infections by serum measurement of human neutrophil lipocalin (HNL) and the impact of antibody selection. J Immunol Methods 2016;432:82-86.
(29) Fang C, Wang Z, Dai Y, Chang W, Sun L, Ma X. Serum human neutrophil lipocalin: An effective biomarker for diagnosing bacterial infections. Clin Biochem 2020;75:23-29.
(30) Venge P, Douhan-Hakansson L, Garwicz D, Peterson C, Xu S, Pauksen K. Human Neutrophil Lipocalin as a Superior Diagnostic Means To Distinguish between Acute Bacterial and Viral Infections. Clin Vaccine Immunol 2015;22(9):1025-1032.
(31) Venge P, Hakansson LD, Garwicz D, Peterson C, Xu S, Pauksen K. Human neutrophil lipocalin in fMLP-activated whole blood as a diagnostic means to distinguish between acute bacterial and viral infections. J Immunol Methods 2015;424:85-90.
(32) Assarsson J, Korner U, Lundholm K. Evaluation of procalcitonin as a marker to predict antibiotic response in adult patients with acute appendicitis: a prospective observational study. Surg Infect (Larchmt ) 2014;15(5):601-605.
(33) Prkno A, Wacker C, Brunkhorst FM, Schlattmann P. Procalcitonin-guided therapy in intensive care unit patients with severe sepsis and septic shock–a systematic review and meta-analysis. Crit Care 2013;17(6):R291.
(34) Shehabi Y, Sterba M, Garrett PM et al. Procalcitonin algorithm in critically ill adults with undifferentiated infection or suspected sepsis. A randomized controlled trial. Am J Respir Crit Care Med 2014;190(10):1102-1110.
(35) Jonsson N, Gille-Johnson P, Martling CR, Xu S, Venge P, Martensson J. Performance of plasma measurement of neutrophil gelatinase-associated lipocalin as a biomarker of bacterial infections in the intensive care unit. J Crit Care 2019;53:264-270.