





MR-Guided Focal Therapy for Prostate Cancer Management
Woodrum-MR-guided focal therapy for native and recurrent prostate cancer
Introduction
The American Cancer Society (ACS) estimates 299,010 new cases of prostate cancer in 2024 and 35,250 deaths secondary to prostate cancer¹,⁵. In 2024 prostate cancer is the most commonly diagnosed noncutaneous cancer and second-leading cause of death in men⁶. With the dramatic increase in good quality diagnostic mpMRI, organ confined prostate cancer is increasingly visible, targetable and potentially treatable with focal ablative technologies²,⁵,⁷.
Unfortunately, the time line and variability of prostate cancer progression from organ confined disease to extra-prostatic spread is unknown. However, it seems intuitive that early detection and proper characterization may play a role in preventing the development of metastatic disease⁴. In view of the significant disparity on recommendations for early detection and prostate cancer screening among various scientific organizations (i.e. American Urological Association, American Society of Clinical Oncology, National Comprehensive Cancer Network, American Cancer Society, US Preventative Task Force and the European Association of Urology), and the uncertainty of the harm/benefit of screening, this review will not delve into this controversy. Our focus will be on the current state of art of prostate imaging, biopsy, and ablation techniques for early native prostate cancer and prostate cancer recurrence after surgery or radiation.
The significance of precise image identification and biopsy is further amplified by Level 1 evidence supporting detection and subsequent aggressive treatment of intermediate and high-risk prostate cancer⁸. Therefore accurate ascription of cancer risk (i.e. grade and stage) using imaging and biopsy is critical. Advances in prostate treatment have become integrated with imaging, image identification, and image guided biopsy and therapy propelling prostate treatment solutions forward faster than ever.
1. Primary Prostate Cancer
CANCER WORK-UP
The historical workup for prostate cancer has been a combination of prostate-specific antigen (PSA) screening and digital rectal exam (DRE) followed by DRE-directed biopsy. More recently, the use of ultrasound (US) imaging has helped direct biopsies toward suspicious lesions and systematically sample the prostate; however, US imaging alone is not sensitive enough to find all the prostate cancer within the gland, despite advanced US modalities (i.e. color/power doppler, elastography and bubble contrast agents). Furthermore, while systematic (non-targeted) sampling of the entire organ has provided some answers, it runs the risk of under-sampling small-volume, high-grade but clinically-significant disease or over-sampling indolent, low-grade disease, potentially resulting in delayed diagnosis or overtreatment.
Magnetic resonance imaging (MRI) is the superior imaging modality for prostate and associated structures due to its exceptional soft tissue conspicuity, high-level spatial resolution, and cross-sectional imaging. Utilization of integrated endorectal and pelvic phased-array coils has led to continued improvement in prostatic fossa visualization. High resolution T2-weighted imaging is sensitive in depicting prostate cancer especially within the transition zone of the prostate; however, decreased T2 signal intensity is not specific for prostate cancer, especially within the peripheral zone where benign conditions can lead to imaging changes. Functional parametric imaging, including dynamic contrast-enhanced imaging (DCEI), diffusion-weighted imaging (DWI), and MR spectroscopic imaging (MRSI), complement morphologic MRI by reflecting perfusion characteristics, Brownian motion of water molecules, and metabolic profiles, respectively. Significant inverse correlation was shown between ADC value and Gleason score/highest grade⁹.
In 2013, a consensus panel endorsed utilization of mpMRI to identify patients for focal therapy¹⁰. Multiparametric MRI is capable of localizing small tumors for focal therapy. In 2015, a consensus panel agreed to Prostate Imaging Reporting and Data System (PI-RADS) version 2, which promoted standardized MR acquisition and interpretation to improve detection, localization, characterization, and risk stratification of clinically significant prostate cancer in treatment naïve prostate glands¹¹. Targeted biopsy of suspected cancer lesions detected by MRI is associated with increased detection of high-risk prostate cancer and decreased detection of low-risk prostate cancer, particularly with the aid of MRI/Ultrasound fusion platforms¹². The use of mpMRI has expanded beyond staging to detection, characterization, monitoring for active surveillance and cases of suspected local recurrence after failed definitive therapy. Though interest in the usefulness of biomarkers used in combination with mpMRI remains, emerging evidence supports its adoption as a standard of care tool in prostate cancer diagnosis at the confirmatory stage¹³,¹⁴.
While mpMRI plays an established, critical role in primary and recurrent prostate cancer, functional and metabolic imaging are playing an expanding role with a host of new agents being developed. Established positron emission tomography (PET) tracers for imaging of prostate cancer include ¹¹C and ¹⁸F choline¹⁸, F fluciclovine⁴⁸, Ga prostate-specific membrane antigen (PSMA), and ¹¹C-acetate¹¹. C-choline PET/CT has an advantage to reveal both local recurrent and distant metastatic prostate cancers¹¹. C-choline PET/CT had a sensitivity of 73%, a specificity of 88%, a positive predictive value (PPV) of 92%, a negative predictive value (NPV) of 61%, and an accuracy of 78% for the detection of clinically suspected recurrent prostate cancer in postsurgical patients¹⁵. In a study of post-prostatectomy patients with rising PSA, mpMRI is superior for the detection of local recurrence¹¹, C-choline PET/CT is superior for pelvic nodal metastasis, and both are equally excellent for pelvic bone metastasis¹¹. C-choline PET/CT and mp-MR imaging are complementary for restaging prostatectomy patients with suspected recurrent disease and exhibit diverse patterns of recurrence with implications for optimal salvage treatment strategies¹⁶,¹⁷.
⁶⁸Ga-PSMA is a promising PET tracer and indicates favorable sensitivity and specificity profiles compared to choline-based PET imaging techniques¹⁸. A recent publication demonstrated that late 3 hour imaging of⁶⁸Ga-PSMA helped to clarify activity within the prostate due to decreased activity within the bladder at this time point¹⁹. Early work with simultaneous MRI/PET imaging shows promise in capitalizing both the functional aspects of PET with the superb anatomic capabilities of MRI²⁰. Compared to mpMRI, PSMA-imaging techniques, including⁶⁸Ga-PSMA-PET/MRI¹⁸, F-PSMA-PET/CT, and⁶⁸Ga-PSMA-PET/CT, have demonstrated improved detection of dominant intraprostatic lesions²¹.
Even with improvements in US and PET/CT imaging, MRI remains preeminent for detection and staging of prostate tumors within the pelvis. MRI/PET may ultimately provide the optimal combination of diagnostic resolution in the pelvis coupled with the whole-body screening functionality of PET imaging to provide the single platform for detection and localization.
BIOPSY METHODS
Prostate Biopsy Techniques
Ultrasound guided biopsies: The transrectal ultrasound-guided (TRUS) prostate biopsy has remained the cornerstone for prostate cancer tissue diagnosis dating back to the systematic ‘sextant’ biopsy protocol with 3 cores per side²². A meta-analysis of 68 studies led to a recommendation of a more laterally directed schema with 12 cores improving prostate cancer detection rates by a factor of 1.3²³. Using this systematic 12 core TRUS sampling for men undergoing initial biopsy with elevated PSA yields cancer detection rates between 30-55%²⁴. The false negative rate for this 12-core schema is on the order of 20-24% and repeated 12 core or saturation biopsies show detection rates of 11-47%²⁵,²⁶. This is particularly true for men with anteriorly located and apex tumors²⁷. To improve the accuracy of sampling, some experts advocate the use of template, transperineal-mapping (TPP) biopsies to systematically sample all quadrants of the prostate²⁸. This has been criticized for oversampling of insignificant tumors with risk of additional morbidity and need for general anesthesia. While the comparative costs and benefits of TPP-biopsy remain under debate, a growing body of evidence suggests it offers high sensitivity of clinically significant cancer detection and more accurate anterior prostate gland sampling²⁹,³⁰.
MR-based biopsy techniques
Increasingly, evidence supports the use of pre-biopsy mpMRI for identification of clinically significant disease. The hope is to identify the significant lesions for targeted biopsy while not oversampling otherwise normal regions²⁶,³¹,³². Emerging research suggests pre-biopsy mpMRI can reduce unnecessary biopsies; however, underdetection rates associated with pre-biopsy mpMRI suggest TRUS biopsies may be necessary even if pre-biopsy mpMRI results are negative³³,³⁴. There are three main MR-based biopsy technical approaches.
Cognitive/Visual – directed MRI Targeted Biopsy:
Overall, cognitive fusion (or visually directed) biopsy techniques demonstrate the most variability between operators due to the reliance on spatial orientation of the lesion from the MR which is used to direct the US and biopsy needle by the operator. With appropriate experience, this can be readily implemented but can be very difficult with small lesions or targets well away from the US transducer, such as with anterior tumors in large glands. Although MR-directed cognitive fusion biopsy of the prostatectomy bed is still useful for the evaluation of patients with biochemical failure after surgery, no dedicated MR-TRUS fusion software biopsy system is currently available for this application. The cognitive/fusion method is prone to error in reliably mapping the MRI suspicious lesion on real time TRUS and the confirmation of TRUS guided targeted biopsy needle location over the MRI suspicious lesion is not feasible, except when needle tracks are visible. In a study of 555 patients by systematic biopsy as well as cognitive fusion guided targeted biopsy, overall 54% (302/555) of patients were found to have cancer; 82% of them were clinically significant. Systematic biopsy and cognitive fusion guided targeted biopsy detected 88% and 98% of clinically significant cancers, respectively³⁵. Cognitive fusion targeted biopsy showed 16% more high-grade cancers and higher mean cancer core lengths than standard systematic biopsy. Cognitive targeted biopsy would only avoid 13% of insignificant tumors. Valerio et al compared cognitive fusion to a software-based targeted biopsy. The software-based, targeted transperineal approach found more clinically significant disease than visually directed biopsy although this was not statistically significant (51.9% vs. 44.3%, p = 0.24)³⁶. The current diagnostic ability of visually/cognitively targeted and software-based biopsies seem to be nearly comparable with experienced operators. A recent meta-analysis found high variability between studies comparing cognitive-fusion versus image-guided fusion prostate biopsies, highlighting the need for thoughtful consideration of operator familiarity and experience when selecting a biopsy strategy³⁷.
Software-based Ultrasound – MRI fusion Targeted Biopsy³⁸,³⁹:
Software-based MRI/TRUS fusion-guided biopsy platforms seek to combine the advantage of lesion visualization from the MRI with the ease and availability of US based biopsy platforms for real-time imaging. There are three key tracking methods including 1) image organ-based tracking, 2) electromagnetic sensor-based tracking, and 3) mechanical arm, sensor-based tracking⁴⁰.
Image organ (prostate) – based tracking method fuses prior MRI with real-time 3D US using a surface-based registration and elastic organ-based deformation algorithm (Urostation, Koelis, Meylan, France). MRI-identified suspicious lesions are loaded into the system which then projects the target into the biopsy aiming mechanism on the US probe. This is relatively inexpensive and allows systematic biopsy. However, confirmation of targeted needle biopsy tracts is retrospective⁴¹.
Additional systems utilize electromagnetic sensor-based tracking using a non-rigid registration algorithm. The advantage with this approach is that it allows real-time spatial tracking of targets and needle location and is less operator-dependent allowing free hand scanning during procedures (UroNav, InVivo, Inc. Gainesville, FL, USA; Real-time Virtual Sonography [RVS], Hitachi-Aloka, Tokyo, Japan and BK Fusion, BK Medical ApS, Herlev, Denmark). Published in 2016, a prospective study of 1003 men undergoing a MR/ultrasound fusion targeted and concurrent standard biopsy found that targeted MR/ultrasound fusion biopsy was shown to diagnose 30% more high-risk prostate cancer (defined as Gleason score 4 + 3 or greater) while a combination of standard and targeted biopsies revealed 22% more prostate cancer, mostly (83%) low-risk prostate cancer (defined as Gleason score 3 + 3 and low volume 3 + 4)⁴².
A similar but slightly different approach uses a mechanical arm, sensor-based tracking system where the tracking arm is attached to a conventional US probe. Again, this allows real-time spatial tracking of targets and needle location (Artemis, Eigen Inc., Grass Valley, CA, USA). This system is also less operator-dependent but relatively expensive. In a retrospective review of 601 men who underwent both MRI-ultrasound fusion targeted biopsy and systematic biopsy, targeted MRI-ultrasound fusion biopsy detected fewer Gleason score 6 prostate cancers (75 vs. 121; p < 0.001) and more Gleason score ≥7 prostate cancers (158 vs. 117; p < 0.001) when compared with systematic biopsy⁴³. In a 2012 review of 105 patients with prior negative biopsies and elevated PSA, MRI-ultrasound fusion targeted biopsy improved detection of clinically significant prostate cancer when compared with systematic biopsy⁴⁴. A recent study further confirmed that MR/ultrasound fusion targeted biopsy had higher sensitivity, detecting clinically significant disease with less oversampling.
Recent advances in MRI have demonstrated the value and importance of good prostate imaging. These advances are actively changing the way prostate cancer is diagnosed and treated. However, even with these advances it is critical to understand that MRI still has its limitations and needs further development. A recent study of 125 surgical prostatectomy patients studied the accuracy of the pre-surgical biopsy where there had been a pre-biopsy mpMRI with subsequent MR-US fusion biopsy. They found that there was a 4% (5 of 123) MR miss rate on surgical pathologic analysis⁴⁵. Another study of 1042 men examined mpMRI targeted biopsies versus systematic biopsies. They found that the addition of systematic biopsy to targeted biopsy found 7% (60/825) more clinically significant cancers⁴⁶. These lesions would have been underdiagnosed if mpMR suspected lesions only were targeted. Supporting these findings, a recent review found that systematic biopsies should be used in combination with targeted biopsies to ensure the most robust assessment of the prostate gland in at-risk patients⁴⁷. In a recent study in 100 patients who underwent mpMRI, 162 clinically important malignant lesions were present after subsequent prostatectomy. On a per patient basis, mpMRI depicted clinically important prostate cancer in 99 (99%) of the 100 patients. However, at least one clinically important tumor was missed in 26 (26%) patients⁴⁸. Considering the state of evidence, a recent review article recommended mpMRI as the initial step in the workup of men with suspected cancer⁴⁹.
In-Bore Direct MRI Targeted Biopsy:
There are two main in-bore direct MRI targeted biopsy approaches including robot assisted, transrectal biopsy (DynaTRIM, InVivo) or a transperineal approach via template. In-bore MRI-guided biopsies have the advantage of real-time MR imaging to confirm biopsy acquisition position, thereby improving sampling accuracy. Using the direct in-bore biopsy technique one eliminates the issues of mis-registration, organ deformation and organ movement which continue to plague software-based US-fusion imaging. Additionally, transperineal biopsies using a template reduce or nearly eliminate the bacterial infection risk seen in transrectal biopsies. A study of 265 patients with rising PSA and negative TRUS biopsy found that performance of MR-guided robot-assisted transrectal biopsy (DynaTRIM, InVivo) in this population produced a detection rate of 41% (108/265) for prostate cancer and 87% (94/108) for clinically significant cancer⁴⁴. Penskofer et al showed in a prospective clinical study, that in-bore prostate biopsies with at least one MRI detected lesion in men on active surveillance monitoring and in men with suspected recurrent cancer following treatment, detected cancer in 72% under active surveillance and detected recurrent cancer in 72% with possible recurrence⁵⁰,⁵¹. The accuracy of the transperineal in-bore biopsy appears acceptable as demonstrated by analysis of biopsy and post-prostatectomy histopathology⁵². MR-detected targets located in the anterior gland had the highest cancer yield (62.5%). In a retrospective study of 223 patients, Del Monte et al found MRI in-bore targeted biopsy showed higher malignant cell percentages per-core; however, no statistically significant difference in detection rate between in-bore biopsy and MRI-TRUS fusion biopsy was found⁵³. These results were supported by Ramos et al’s study (n = 280), finding that in-bore biopsy was associated with higher detection rates of clinically significant cancer in targeted cores only⁵⁴. Exclusive to PI-RADS category 4 or 5 lesions, a recent retrospective study (n = 286) found that in-bore MRI-targeted biopsy demonstrated higher specificity compared to fusion biopsy⁵⁵. Although these advantages are attractive, this technique is underutilized due to specialized MRI compatible tools, relative cost disadvantage, difficulty obtaining access to MRI, and need for coordination between Urology and Radiology.
TREATMENTS FOR PRIMARY PROSTATE CANCER
Once prostate cancer is identified from imaging and/or biopsy, a treatment plan must be formulated for the patient. The traditional therapy options for clinically localized prostate cancer with intent for cure have been either surgical resection or radiotherapy⁵⁶. A recent meta-analysis of 19 studies suggests that surgery offers a benefit in overall and prostate cancer-specific survival compared with radiotherapy⁵⁷. This is further supported by the results of a randomized phase III trial which found that, among patients who develop metastases within 10 years of treatment, those who received prostatectomy had a lower mortality rate⁵⁸. For patients with localized high-risk prostate cancer, recent reviews suggest a benefit in radical prostatectomy over radiotherapy for overall and prostate cancer specific mortality⁵⁹,⁶⁰. Roughly about half of patients choose surgery and half choose radiotherapy⁶¹.
However, these therapies have significant risk and morbidity to the patient’s health-related quality of life with potential impact on sexual, urinary and bowel function⁶². A recent meta-analysis reported that differences in quality-of-life outcomes, such as urinary, bowel, and sexual function, between surgery and radiotherapy recipients diminished over time⁶³. Active screening programs for prostate cancer have enabled earlier identification of low-risk prostate cancer, but due to related morbidity from standard therapies, many choose active surveillance to delay treatment until cancer progression³.
EVOLVING FOCAL AND PARTIAL GLAND THERAPY TREATMENT OPTIONS
For men with newly diagnosed prostate cancer and with a life expectancy >10 years, radical prostatectomy and radiation therapy remain preferred definitive therapy of choice⁶⁴–⁶⁶. However, patients are increasingly interested in less radical, more focal, methodologies for treatment, especially in the active surveillance population. For this population of low- and intermediate-risk prostate cancer patients, they also may be uncomfortable remaining on active surveillance but don’t want surgery or radiation. This patient-driven interest for a more minimally invasive approach is driving focal therapies for prostate carcinoma in low-risk patients⁶⁷.
As a result, several minimally invasive thermal ablation methods under direct MR guidance, most prominently cryotherapy, laser ablation, and high-intensity focused ultrasound (HIFU), have been developed and are currently being evaluated⁶⁸–⁷⁰. Despite this, focal therapy is still controversial due to the potential for multifocality of prostate cancer, limitations of current biopsy strategies, variation in quality MR imaging and less than robust prediction models for indolent prostate cancers. Furthermore, prostate cancer recurrence rates after established forms of therapy range from 20-60%⁷¹. Although emerging research suggests that partial gland ablation recipients suffer fewer side effects compared to those who receive surgery or radiotherapy, little is known about long-term outcomes associated with thermal and non-thermal focal treatment options⁷².
Patient Selection for Focal and Partial Gland Therapy
Selecting the appropriate patient for focal/partial gland therapy as a primary treatment for prostate cancer is the most important element of a successful outcome. Accurately staging the prostate cancer is critical not only for the highest grade of prostate cancer but also understanding the extent of low-grade (i.e. Gleason 6) disease as well. With low-risk disease, there is level 1 evidence that implies a lack of benefit from radical/nonconservative therapy⁷³–⁷⁵. Patients are many times initially targeted for cancer workup due to rising PSA or nodule on digital rectal exam. These patients may undergo further workup with mapping biopsy and/or mpMRI with targeted biopsy. Patients are then classified to have low, intermediate, or high-risk disease. For consideration of focal therapy, the patient needs to have low or intermediate risk disease with a focal positive index lesion on mpMRI, Gleason ≤4+3, and PSA <20ng/mL. The target lesion should be confined to one lobe of the prostate⁷⁴. Furthermore, the target should be visible with the imaging modality which will be used to guide the focal ablation treatment. With MRI having exceptional soft tissue conspicuity, high spatial resolution, and multi-planar imaging capacity, this approach has clear advantage over transrectal ultrasound as an imaging guidance platform.
MODALITIES USED TO ABLATE PRIMARY PROSTATE CANCER:
MR-guided Cryoablation
MR guided percutaneous cryoablation combines excellent soft tissue resolution and ice ball monitoring without the use of MRI thermometry. Early experience combining cryoablation with MRI has shown a high degree of accuracy in defining normal and frozen tissue on all MR imaging sequences⁷⁶,⁷⁷. There is limited data using MR guided cryoablation for primary treatment of prostate cancer. Two published canine studies demonstrated feasibility and overall safety⁷⁸,⁷⁹. These studies did expose one limitation of cryoablation which is that the visualized edge of the ice (0°C) does not represent the ablation margin. The actual ablation margin is best demonstrated with contrast enhancement post-procedure and is actually at the -20°C isotherm. There are two published reports of MR guided cryoablation in native prostate glands, each with relatively small numbers (Fig. 1)⁸⁰,⁸¹. Gangi et al. performed MRI guided prostate cryoablation in eleven patients on 1.5T MRI with minor complications of hematuria, dysuria, and urine retention and one major complication of rectal fistula with spontaneous closure after 3 months⁸⁰. These studies confirm that MR-guided cryoablation is technically feasible with relative safety; however, more intermediate and long-term outcome data is needed to assess overall efficacy. A recent literature review on MR-guided cryoablation found that focal or whole gland cryoablation may be appropriate for low- and intermediate-risk cases wherein surgery is not recommended or gland salvage is required⁸².
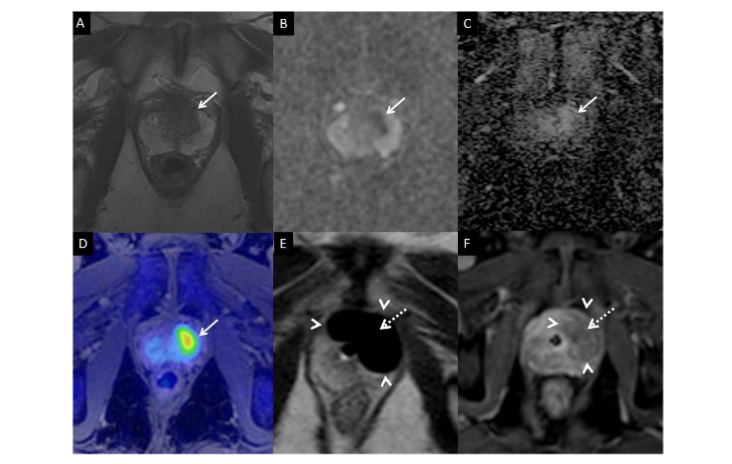
Figure 1 (Cryoablation): 70-year-old male presents with Gleason 3+3 adenocarcinoma of the left anterior prostate with a PSA of 6.2 ng/mL. Multiparametric MRI at 3 Tesla demonstrated an area of decreased signal intensity in the left anterolateral peripheral zone at the prostatic midgland (Panel A, arrow) with corresponding hypointensity on ADC map (Panel B, arrow) and early hyperenhancement (Panel C, arrow). Using a 1.5T MRI, three IceRod cryoneedles were placed via transperineal approach into the left anterior prostate and freezing was performed under imaging guidance with three freeze-thaw cycles. An iceball is clearly visible on axial T2-weighted image during the freezing phase (Panel D) tumor arrow, iceball arrowheads, urethra dashed arrow). Subsequent post-ablation dynamic gadolinium enhanced series demonstrates the corresponding ablation zone to encompass the previously demonstrated cancerous lesion (Panel E, arrow).
MR thermometry for thermal ablation
One major advantage of MR guidance for heating thermal ablations is ablation monitoring using MRI thermometry where subsequent dose estimations can be applied. The MR thermometry typically performed is a near real-time proton resonance frequency (PRF) sequence which demonstrates signaling change as a function of temperature⁸³. During delivery of ablative energy (generated by ultrasound transducer or laser applicator) a series of 2D phase sensitive T1-weighted fast spoiled gradient-recalled echo MR images are acquired on MRI scanner⁸⁴–⁸⁶. Based on temperature changes, a thermal dose can be calculated to predict a real-time tissue lethal dose⁸⁷. However, the two major limitations with this sequence are the inaccuracy in fat tissue and susceptibility to motion artifact. Additionally, PRF only measures temperature change relative to an established reference temperature⁸⁸.
MR-guided Laser Ablation
Laser-induced interstitial thermal therapy (LITT) uses a locally placed laser fiber probe to deliver targeted thermal ablation under MR guidance. LITT is inherently magnetic resonance (MR) compatible. MR guidance for laser applicator placement and ablative monitoring provides the imaging to prevent encroachment onto adjacent critical structures. Two early publications demonstrated technical feasibility of laser ablation monitoring in canine prostate and demonstrated correlation of the MR temperature map with contrast enhanced T1-weighted images⁸⁹,⁹⁰. A subsequent study in cadavers demonstrated technical feasibility in the human prostate within a 3T MRI scanner⁹¹. Lee et al. examined 23 patients treated with focal laser ablation demonstrating promising results⁶⁹. Raz et al. described using laser ablation for treatment of 2 prostate cancer patients at 1.5T with discharge 3 hours after the procedure⁹². A recent phase I trial (n = 8) found that laser ablation, though safe and feasible, may require broader treatment margins to effectively destroy tumors⁹³. These studies demonstrate the potential utility of laser ablation in the prostate. However, more clinical data is needed to determine short- and long-term efficacy.
US- and MR-guided High-intensity Focused Ultrasound (HIFU) Ablation
Treatment of the prostate with focused ultrasound ablation is not new, although MRI guided version of procedure has not, as of yet, been approved by FDA in the United States. HIFU achieves cellular death by rising the cellular temperature >60°C causing cellular necrosis. HIFU ablation technique does not require placement of a needle probe in a targeted prostate tumor via the rectum or skin (perineum) to deliver thermal energy and destroy cancerous tissue. This treatment modality has been performed with transrectal ultrasound (US) imaging guidance with success in Europe for many years⁹⁴. The major limitation of US imaging guidance for prostate ablation is that ultrasound cannot precisely visualize the focus of cancer and therefore the target of therapy. Therefore, the initial treatment strategy used with US-guided high intensity focused ultrasound (HIFU) was to ablate the entire prostate, or a relatively large region where the site of biopsy-proven cancer was found using a mapping biopsy and/or mpMRI. This often resulted in inadequate tumor control or over-ablation of unnecessary normal/neural tissue with potential subsequent morbidity. An early study, using HIFU ablation in prostate by Gelet et al, treated 82 patients who were subsequently followed up for 24-month duration. These patients also received subsequent radiation treatments⁹⁵. Among these patients, 68% were cancer free at the time of follow-up. Due to relatively high complication rates, the treatment device underwent multiple iterations and improvements. A subsequent study, by Gelet et al, demonstrated incontinence and impotency rates around 14% and 61% respectively at 19 months post-treatment. In both studies, major limitations were identified as total procedure time due to a need to cover the entire prostate and inability to monitor temperature elevations or ablation zone expansion⁹⁶. Current generation US guided HIFU has evolved into more robust treatment platforms with motion detection, improved planning modules and capacity to perform focal and partial gland therapy using US/MRI fusion⁹⁷. The largest prospective single arm study with 1,002 patients demonstrated that whole gland ablation could be performed with severe incontinence rates from 3-6% and urethral stricture rates of 6-35%⁹⁸. The 8-year biochemical free survival rates were 76% for low-risk, 63% for intermediate risk, and 57% for high risk⁹⁸. A subsequent single arm prospective clinical trial of HIFU hemiablation in 50 patients with unilateral, low-intermediate disease and 39.5 month followup demonstrated biochemical recurrence rate of 28-36% with 6% incontinence rate and 20% impotence rate⁹⁹. As the ultrasound guided technology has improved so have the results¹⁰⁰. A 2-year follow-up of 928 patients treated with 3 sequential versions of Sonablate devices demonstrated a corresponding 5 year biochemical disease free rate of 48.3%, 62.3%, and 82% respectively⁹⁷. At the current time, ultrasound guidance is challenged with the inability to see the tissue heating produced by the focused ultrasound such that there is no real-time feedback. This is one of the advantages of real-time MR imaging which does in fact see and measure the tissue heating in a real-time quantitative manner.
To address the issue of visualization and temperature monitoring, two different MR guided focused ultrasound systems were developed. With MR thermal monitoring and localization of lesions/zones within prostate, focused ultrasound could be performed with smaller treatment zones presumably resulting in improved treatment margins with decreased morbidity. Currently, there are two MRI-integrated systems using transrectal (Exablate, InSightec, Haifa, Israel) (Fig2) or transurethral (Profound Medical Inc., Toronto, Canada) transmission routes for treatment of prostate lesions with focused ultrasound technology. The system is fully integrated with the MRI console with temperature feedback control to adjust power, frequency, and rotation rate. Following the publication of results from the TULSA-PRO Ablation Clinical Trial (n = 115), which found a 93% reduction in median PSA and 96% of patients presenting with >75% PSA reduction, Profound Medical Inc.’s TULSA system received FDA approval in August 2019¹⁰⁰,¹⁰¹. A recent systematic review found that Profound Medical Inc.’s TULSA system was effective at prostate cancer ablation and reducing urinary symptoms¹⁰². The results of a phase II trial (n = 101) evaluating the Exablate approach suggest that MR-guided US ablation is effective for treating grades 2 and 3 prostate cancer without causing side effects. Specifically, in 88% of patients, no intermediate- or high-risk cancer remained in the treated area at 6 and 24 months¹⁰². Exablate Prostate received FDA approval in December 2021¹⁰³.
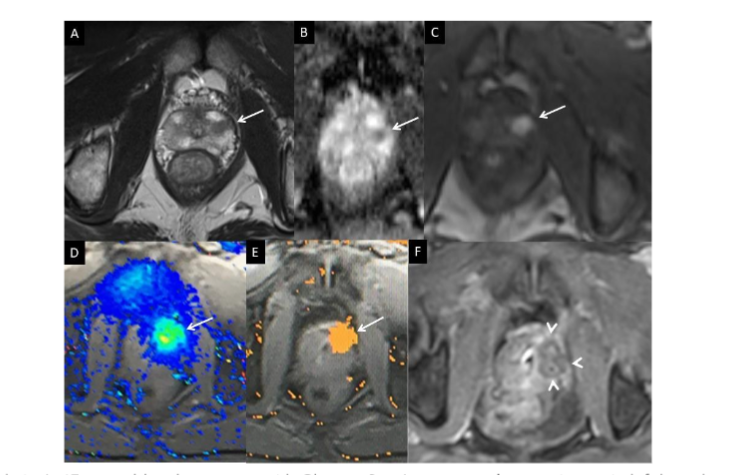
Figure 2 (Laser ablation): 67-year-old male presents with Gleason 3 + 4 prostate adenocarcinoma in left lateral peripheral zone at the apex. During MR guided laser ablation, axial T1-weighted images demonstrate a small hypointensity in left lateral peripheral zone within the lesion (Panel A, arrow) which corresponds to the change in temperature seen on phase imaging (Panel B, arrow) and calculated ablation zone on the damage map (Panel C, arrow).

Figure 3 (InSightec): 65-year-old male presents with Gleason 3+4 prostatic adenocarcinoma of the left peripheral prostate. Multiparametric MRI at 3 Tesla demonstrated an area of decreased signal intensity in the left lateral peripheral zone at the prostatic midgland (Panel A, arrow), with corresponding hypointensity on ADC map (Panel B, arrow), and early subtle hyperenhancement (Panel C, arrow). InSightec ultrasound transducer was placed in the rectum and treatment plan created (Panel D). Post-ablation dynamic gadolinium enhanced series demonstrates the corresponding ablation zone to encompass the previously demonstrated cancerous lesion (axial Panel E, arrow and sagittal, Panel F).
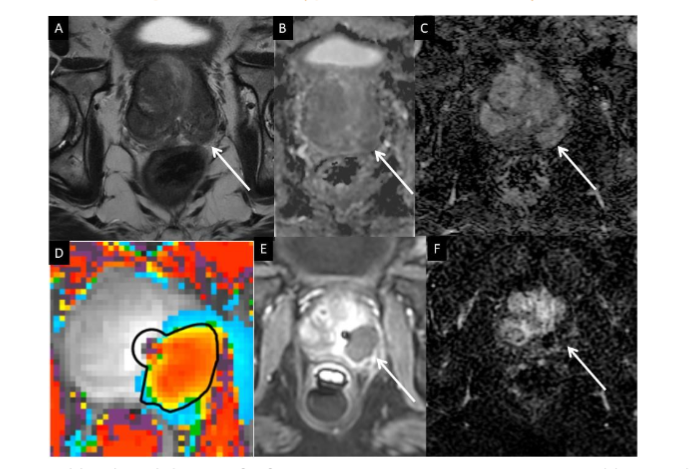
Figure 4 (TULSA): 75-year-old male with history of refractory prostate cancer status post external beam radiation therapy with subsequent salvage prostatectomy and lymphadenectomy. PSA was undetectable but started rising. Pelvic MRI demonstrated a hyperenhancing recurrence posterior to the vesicourethral (VU) anastomosis. TRUS-guided biopsy revealed Gleason 4 + 4. Axial T2-weighted images demonstrate a soft tissue nodule with hypointensity posterior to VU anastomosis (Panel A, arrows). Corresponding ADC map demonstrates restricted diffusion (Panel B, arrows). Corresponding DCE image demonstrates hyperenhancement (Panel C, arrows). CT/PET choline imaging demonstrates corresponding increased activity in the hyperenhancing nodule (Panel D, dashed arrow). Using a 1.5T MRI, six IceRod cryoneedles were placed via the transperineal approach posterior to the vesicourethral anastomosis. An iceball is clearly visible on axial T2-weighted image during the freezing phase (Panel E, iceball arrowheads). Subsequent post-ablation dynamic gadolinium enhanced series demonstrates the corresponding ablation zone to encompass the previously demonstrated cancerous lesion (Panel F, arrowheads).
Recurrent Prostate Cancer
Recurrent prostate cancer after surgery can range from 25 to 40% manifesting as a rise in PSA¹⁰⁴–¹⁰⁶. Up to one-third of all men with prostate cancer will develop biochemical recurrence (BCR) with rising PSA after radical prostatectomy¹⁰⁴. Approximately 81% of prostate cancer recurrences occur locally in the prostate bed and can be visualized with multiparametric MRI¹⁰⁷. With radiation treatment, biochemical recurrence can range widely between 33 and 63% over 10 years, and this contributes another 45,000 men/year with post-radiotherapy recurrent cancer in the USA alone¹⁰⁸,¹⁰⁹. Salvage treatments currently available for recurrent prostate cancer include salvage radical prostatectomy, salvage radiotherapy, salvage ultrasound (U/S)-guided high-intensity focused ultrasound, salvage U/S-guided cryoablation, and newly described salvage MRI-guided laser and cryoablation.
MRI FOR RECURRENT PROSTATE CANCER
After a definitive radical prostatectomy or radiation therapy, patients are followed at periodic intervals with measurement of PSA levels and DRE. However, DRE is frequently unreliable in evaluating local recurrent disease after radical prostatectomy. Following a radical prostatectomy, PSA levels are expected to be undetectable within several weeks of surgery. If there is a rise in a previously undetectable or stable postoperative PSA level (biochemical failure), a prompt search for persistent, recurrent, or metastatic disease should be pursued. However, PSA alone does not differentiate local from distant disease recurrence. There are three main categories of recurrence after radical prostatectomy for prostate cancer, including 1) local recurrence in the prostatic bed, 2) distant metastasis (e.g., bone, lymph node) and 3) a combination of local recurrence and distant metastasis. Therefore, the major objective of diagnostic imaging studies is to assess patients for the presence of distant metastatic disease or local recurrent disease, each requiring different forms of systemic or local therapy. Local recurrence may be amenable to salvage therapy. Systemic recurrence may be an indication for systemic treatment including androgen deprivation therapy and/or chemotherapy.
Transrectal ultrasound (TRUS) has been used for the evaluation of local recurrence. However, the altered anatomy of the region, the development of fibrotic tissue, the fact that 30% of recurrent tumors may be isoechoic and that some lesions are in an anterior position or extend along the bladder wall influence the accuracy of this modality. Furthermore, CT imaging can depict only local recurrences of greater than or equal to 2 cc¹¹⁰.
The use of biopsy has been questioned in the face of a rising PSA level, since the negative results are unreliable and elevated PSA levels usually precede clinical evidence of local recurrence by one or more years. Repeat TRUS with vesicourethral anastomosis (VUA) needle biopsy may be necessary to document local recurrence in one-third of cases¹¹¹. About 25% of men with post-prostatectomy PSA levels of less than 1 ng/ml have histologic confirmation of local recurrence after biopsy of the prostatic fossa¹¹². In a more contemporary study, MRI directed biopsies in 132 post-prostatectomy patients using cognitive /visual registration and TRUS guided biopsies, with a median PSA of 0.59 ng/ml and a median lesion size on MRI of 1 cm yielding a positive predictive value of 85% with positive biopsy rates of 74% with lesion sizes between 1-2cm¹¹³.
¹¹C-choline PET/CT has an advantage to reveal both locally recurrent and distant metastatic malignant lesions. ¹¹C-choline PET/CT had a sensitivity of 73%, a specificity of 88%, a positive predictive value (PPV) of 92%, a negative predictive value (NPV) of 61%, and an accuracy of 78% for the detection of clinically suspected recurrent prostate cancer in postsurgical patients¹⁵. A recent meta-analysis of 18 studies (n = 2,126) found a pooled detection rate of 62% for recurrent prostate cancer. However¹¹, C-choline PET/CT is not widely available.
With the limitations of US and CT imaging, MRI has been shown to be quite useful in detection and staging of recurrent prostate tumors¹¹⁴–¹¹⁶. MRI provides superior soft tissue contrast resolution, high spatial resolution, multiplanar imaging capabilities, and a large field of view. The use of integrated endorectal and pelvic phased-array coils has led to improved visualization of the prostatic fossa. The use of mpMRI for recurrent prostate cancer continues to evolve and has potential to evaluate both local recurrence and distant bony and nodal metastases¹⁶. Functional information from MR spectroscopic imaging and diffusion-weighted imaging may complement morphologic MRI by reflecting tissue biochemistry and Brownian motion of water molecules, respectively. These functional imaging techniques may be used to supplement conventional MR imaging in diagnostic clinical studies.
2. Salvage Therapies for Prostate Cancer
A. SURGERY
Salvage radical prostatectomy (sRP) after radiotherapy is more difficult because of local fibrosis and tissue plane changes secondary to the radiation. From this standpoint only a few centers take on these cases. However, sRP has the longest follow-up period for any of the salvage therapies with follow-up greater than 10 years. The biochemical disease-free survival (bDFS) at 10 years was 30-43% based on aggregated data from four institutions. The 10 year cancer-specific survival rates were 70-77%¹¹⁷,¹¹⁸. More recently, salvage robotic radical prostatectomy has been reported with some small patient studies demonstrating more promising results, but it is premature to report on long term follow up¹¹⁹. Due to the difficulties posed after primary radiation treatment failure, the complication rates for sRP have been higher than primary surgery with incontinence rates of 58% and major complication rates of 33%¹²⁰. The largest series to date is a multi-institutional collaboration study which reviewed 404 patients with a median follow up of 4.4 years and freedom from clinical metastasis of >75% at 10 years from surgery. This study also identified the most favorable groups to undergo sRP were in men with a PSA < 4 ng/ml and post radiation prostate biopsy Gleason score of ≤ 7¹²¹. In a recent retrospective study in patients with local recurrence after primary treatment (n = 106), functional outcomes were inferior compared to those from primary robot assisted radical prostatectomy¹²².
B. RADIATION
Salvage radiotherapy can be used for BCR following surgery or primary radiotherapy failures. Frequently, salvage brachytherapy (BT) is performed for primary radiotherapy failures. In a large study out of Mayo Clinic, 49 patients with primary external beam radiotherapy (EBRT) failure were treated with salvage low dose rate BT. They demonstrated a 3-year biochemical disease free survival (bDFS) of 48% and a 5-year bDFS of 34%¹²³. Multiple other studies demonstrate a slightly better bDFS, but neoadjuvant androgen treatment was also used in conjunction with the radiation confounding the results. Overall, the 5-year bDFS for salvage BT after primary radiotherapy is approximately 20-70%. Complications for salvage BT were either genitourinary (GU) or gastrointestinal (GI). Grade 3-4 GU toxicity was 17% as a late complication and grade 3-4 GI toxicity was around 5.6%¹²⁰,¹²³,¹²⁴. In a more contemporary series of 98 patients, the 3-year bDFS was 60.1%, and there was no difference between low-dose rate BT and high-dose rate BT. On multivariate analysis, only the prostate specific antigen doubling time (PSADT) < 12 months was significantly associated with PSA relapse¹²⁵. The results of a recent follow-up study (n = 89) found 5- and 8-year survival rates (95% CI) for salvage radiotherapy were 90.2% (78.9-95.6%) and 69.8% (46.4-84.4%), respectively. Additionally, the 5-year bDFS survival rate was 50.8% (36.7-63.3%)¹²⁶.
C. HIGH INTENSITY FOCUSED ULTRASOUND (HIFU)
Salvage high intensity focused ultrasound (HIFU) which targets focused ultrasound energy to a specific area has been used for primary prostate cancer treatment and for salvage therapy. Salvage HIFU is a relatively recent treatment modality with a growing number of studies on its efficacy. Three different studies have been published with a relatively short follow up period of 7.4-18.1 months. These studies demonstrated a highly variable bDFS of 25-71% which was confounded by variable definitions of PSA failure and variable use of hormonal therapy before treatment. The most commonly reported complications are incontinence (10-49.5%), urethral stricture with retention (17-17.6%), erectile dysfunction (66.2-100%), and recto-urethral fistula (3-16%)¹²⁰,¹²⁷–¹²⁹. In the largest multi-institutional pooled series of 418 patients treated with whole gland HIFU after failed radiotherapy, the 7-year cancer specific survival and metastasis free survival of >80% were attained at the price of significant morbidity. According to this study, salvage HIFU should be initiated early following radiation failure and by centers with significant experience¹³⁰. In a recent systematic review (n = 1,241), Maestroni et al found that salvage HIFU was effective at treating radiorecurrent prostate cancer, yielding an 85.2% 5-year survival rate¹³¹.
D. ULTRASOUND-GUIDED CRYOABLATION
Ultrasound guided cryotherapy is currently being used for primary prostate cancer treatment as well as salvage treatment after primary radiotherapy failure. Due to the relative recent development as a treatment modality, there are limited studies on its efficacy. Chin et al. reported on 118 patients treated with salvage US cryotherapy after radiotherapy failure¹³². This study showed a negative biopsy rate of 87% with a median follow up of 18.6 months. Siddiqui et al. presented 15 patients with salvage ultrasound guided cryotherapy after radical retropubic prostatectomy¹³³. Their findings demonstrated a 40% bDFS at a mean follow up of 20 months. As cryotherapy devices have evolved with mixed gas technology, smaller cryoprobe size, improved urethral preservation with warmers, better imaging, and increased operator experience, the success rates have improved, and complication rates decreased. A recent large study from the COLD cryo on-line data registry reported a 5-year bDFS to be 58.9% by the ASTRO definition of BCR and 54.5% by the Phoenix definition of BCR¹³⁴. For patients treated with salvage US guided cryotherapy after primary radiotherapy failure, the most recent reported complication rates are perineal pain (4-14%), mild-moderate incontinence (6-13%), severe incontinence (2-4%), and urethrorectal fistula (1-2%). With the use of urethral warming catheter, the rate of sloughing and urethral stricture has been reduced to near zero. Erectile dysfunction (ED) is still high with rates of 69-86.9%. In a pooled study of 396 patients who underwent salvage cryosurgery for radiation failure with a median follow up of 47.8 months, had respective 5- and 10-year DFS of 63% and 35% with disease specific survivals of 91% and 79% respectively¹³⁵. A 2022 systematic review (n = 11,228), with a follow-up period between 9.0 and 297.6 months, reported a disease-specific survival rate of 65.5-100.0% with a biochemical recurrence rate of 15.4-62.0%¹³⁶.
Selection of Patients for Focal Therapy
One of the most important aspects of assessing recurrent prostate cancer is determination of whether the recurrence is localized or metastatic¹⁰⁵. The second issue in managing patients with BCR of prostate cancer is assessing the risk of cancer treatment versus the risk of further intervention. Overall, rapid PSA rise, short-disease free interval, and high-grade disease are all poor prognostic indicators with a higher likelihood of systemic recurrence, while slow PSA rise, long disease-free interval, and low-grade disease are better prognostic indicators with a higher likelihood of local recurrence⁶⁵,¹³⁷.
Potential criteria for MR guided focal ablative treatment of recurrent prostate cancer are as follows: (1) biopsy proven local recurrent tumor that can be visualized by MRI, (2) absence of distant metastasis confirmed with chest, abdomen, pelvis CT and/or MRI plus bone scintigraphy and/or ¹¹C choline PET/CT scan¹¹⁶,¹³⁶. Although not perfect, these criteria seek to rule out patients where they have both local and systemic metastases unless local treatment is coupled with systemic treatment strategy for cancer control.
MRI guided Recurrent Prostate Cancer Focal Therapy Options
MR-guided Cryoablation
MR-guided cryoablation for recurrent prostate cancer is technically feasible and been successful in short-term follow-up. Woodrum et al. published on 18 patients treated with MR guided cryoablation for locally recurrent prostate cancer where treatment optimization parameters were assessed for two groups of 9 patients¹³⁸. Ultimately, the study demonstrated that a more aggressive tight (5mm) spacing of cryoneedles, 3 freeze-thaw cycles, and prudent adjustment of the urethral warmer temperature produced better short-term recurrence free intervals. Gangi et al. also demonstrated successful MR-guided cryoablation treatment of several patients with recurrent prostate cancer⁸⁰. This technique offers the advantage that it is not appreciably limited by the prior surgical or radiation treatment to the targeted area⁸⁰,⁸¹. Using MR guidance, cryoablation treatment can be tailored to the desired area (Fig 2). In another series, MR-guided cryoablation has been reported to successfully treat select patients with locally recurrent tumors after failed radiation therapy¹³⁹. A recent retrospective analysis (n = 47) of patients who underwent MR-guided cryoablation after primary radiotherapy found that wider ablation margins may be necessary for effective treatment¹³⁹.
MR-Guided Laser Interstitial Therapy (LITT)
Using Laser interstitial thermal therapy (LITT) for recurrent prostate cancer has been shown to be feasible with a case report using a 3T MRI with Visualase 980nm diode laser system (Medtronic, Minneapolis, MN, USA)⁸¹. A small case series was also presented by the same group which demonstrated feasibility of treating recurrent prostate cancer with laser ablation. Difficulties encountered with this ablation technique in these patients were the temperature mapping distortion secondary to the surgical clips from prior surgery. This could also be encountered with brachytherapy seed implantation as well. Therefore, recurrences within the surgical clips or brachytherapy seeds would represent a relative contraindication for this method of treatment.
MR-Guided Focused Ultrasound
Briefly describe the ongoing multicenter prospective US pivotal study for low volume Gleason 7 cancer using MR guided trans-rectal focused US. Final accrual likely to be completed by late in 2018.
Follow-up Imaging
After MR-guided salvage focal ablation, the best way to monitor the patient is by measuring serial serum PSA and MR imaging. PSA levels should decrease soon after ablation and ideally drop to undetectable within several weeks of salvage procedure if there is no remaining prostate tissue. In the setting of prior radiation, the PSA is expected to return to prior baseline PSA levels seen after radiation treatment. In either situation the PSA should decrease to a new plateau level and remain there over time. A rise in a previously undetectable or stable postoperative PSA levels during post-treatment follow up indicates recurrent or possibly metastatic disease warranting a further workup to localize viable disease.
One possible schematic for follow up is PSA every 3 months and MR imaging at 6, 12, 18, 24 months post procedure and then lengthen to yearly after the first two years post-ablation if all is negative. Cryoablation has been shown to have some residual ablation zone contrast enhancement when imaging less than 6 months post ablation which resolves at – month imaging¹⁴⁰. Multiparametric MRI can assess prostatic fossa, iliac lymph nodes and pelvic bones. Mild inflammatory enhancement about the ablation zone without a discrete mass is a common finding after procedure and usually resolves within 3 months after procedure. Persistent or new discrete enhancing nodules on MRI are suspicious for residual or recurrent cancerous lesions. These enhancing nodules, if still confined in the prostatic bed, may be amenable for repeated MR-guided salvage ablation. Post-ablative biopsies should also be entertained at one- and two-years post treatment with particular attention to the margin of the ablation zone.
Challenges of Focal Therapy
LIMITATIONS TO MRI VISUALIZATION OF ICEBALL TEMPERATURE ISOTHERMS
A limitation for MR-guided cryoablation is that the leading edge of the iceball is well visualized due to very rapid T2 relaxation of ice protons, but this corresponds to 0°C and may not be completely lethal. Therefore, it is necessary to carry the edge of the ice beyond the tumor margin by at least 5mm assuming that iceball lethal isotherms of -40°C are less than 5mm from the leading edge of the iceball¹⁴¹. Complicating factors to this assumption include heat transfer from adjacent major vessels or urethral warmers¹⁴². Studies have shown that ultra-short echo times (UTE) can be used to visualize temperature changes within the iceball; however, this technique is yet to be widely applied clinically¹⁴³–¹⁴⁵. Confounding the need for good margin coverage is the problem of very restrictive space in and around the prostate bed with close proximity to the rectum, bladder, and external striated urethral sphincter. This small margin of error presents an ongoing challenge of balancing treatment efficacy with morbidity.
LIMITATIONS OF MRI THERMOMETRY
Proton resonance temperature mapping (PRF) capitalizes on the phenomenon of linear change of resonance frequency of water protons with temperature. PRF temperature mapping is a powerful tool, but it has some major limitations such as sensitivity to motion and tissue edge artifacts. PRF relies on a baseline comparison image which all subsequent images are compared. As a consequence, motion is a large problem where the baseline image alignment is disrupted causing phase registration artifacts. A method that has been proposed to alleviate this is reference-less temperature mapping. Another potential issue is the presence of the surgical clips, which can cause metallic artifact resulting in image distortion and signal drop-out, degrading the MR images.
the native prostate, this is less of an issue, but in the post-surgical prostate bed, surgical clip artifact becomes a real problem for phase change-based temperature imaging. The final major limitation with PRF-based temperature mapping is the problem with tissue/fat interface. The resonance frequency is only dependent on temperature for water protons. The resonance frequency of protons in fat is different, producing artifact and inaccuracy for tissue fat interfaces. Some approaches attempt to resolve this issue by the use of the so-called Dixon technique to separate MRI signals from fat and water, use of the PRF method on the fat-only images, and use of phase changes of the fat signal to correct for non-temperature-dependent phase changes¹⁴⁶. This technique, however, has only been applied in a limited number of cases, as of yet¹⁴⁷.
Conclusions
Prostate cancer is the most common solid malignancy in men. As the clinical burden is significant, prostate cancer diagnosis and treatment for new or recurrent disease will demand considerable resources and effort for years to come. mpMRI is playing a pivotal role in the diagnosis and management of this disease. MRI and ultrasound fusion for prostate biopsy guidance appear to represent the next step in timely diagnosis and navigation to clinically significant cancers. mpMRI is an effective modality in the depiction of a locally recurrent tumor after failed definitive treatment. While minimally invasive MR-guided focal ablation of native or locally recurrent prostate cancer is feasible and rapidly becoming a viable treatment alternative, there is still continued work needed to determine long term efficacy. To date, all focal therapy treatment series suffer from relatively small patient numbers with short follow-up and need for comparison to established therapies. Additionally, it is critically important that good prospective clinical trials for each treatment modality be performed to assess the advantage of each and to determine long-term efficacy.
Conflict of Interest:
None.
Funding Statement:
None.
Acknowledgements:
None.
References
1. Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024. CA Cancer J Clin. Jan-Feb 2024;74 (1):12-49. doi:10.3322/caac.21820
2. Potosky AL, Davis WW, Hoffman RM, et al. Five-year outcomes after prostatectomy or radiotherapy for prostate cancer: the prostate cancer outcomes study.[see comment]. Journal of the National Cancer Institute. Sep 15 Sep 15 2004;96(18):1358-67.
3. Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2006. CA Cancer J Clin. Mar-Apr 2006;56 (2):106-30. doi:10.3322/canjclin.56.2.106
4. Vickers AJ, Ulmert D, Sjoberg DD, et al. Strategy for detection of prostate cancer based on relation between prostate specific antigen at age 40-55 and long term risk of metastasis: case-control study. BMJ. 2013;346:f2023.
5. Miller KD, Siegel RL, Lin CC, et al. Cancer treatment and survivorship statistics, 2016. CA: a Cancer Journal for Clinicians. Jul 2016;66(4):271-89. doi:10.3322/caac.21349
6. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA: a Cancer Journal for Clinicians. Jan 2015;65(1):5-29. doi:10.3322/caac.21254
7. Onik G. Rationale for a “male lumpectomy,” a prostate cancer targeted approach using cryoablation: results in 21 patients with at least 2 years of follow-up. Cardiovascular & Interventional Radiology. Jan-Feb Jan-Feb 2008;31(1):98-106.
8. Bill-Axelson A, Holmberg L, Garmo H, et al. Radical prostatectomy or watchful waiting in early prostate cancer. N Engl J Med. Mar 6 2014;370(10) :932-42. doi:10.1056/NEJMoa1311593
9. Hambrock T, Somford DM, Huisman HJ, et al. Relationship between apparent diffusion coefficients at 3.0-T MR imaging and Gleason grade in peripheral zone prostate cancer. Radiology. May 2011;259(2):453-61. doi:10.1148 /radiol.11091409
10. Muller BG, Futterer JJ, Gupta RT, et al. The role of magnetic resonance imaging (MRI) in focal therapy for prostate cancer: recommendations from a consensus panel. BJU Int. Feb 2014;113 (2):218-27. doi:10.1111/bju.12243
11. Spektor M, Mathur M, Weinreb JC. Standards for MRI reporting-the evolution to PI-RADS v 2.0. Transl Androl Urol. Jun 2017;6(3):355-367. doi:10.2 1037/tau.2017.01.02
12. Siddiqui MM, Rais-Bahrami S, Turkbey B, et al. Comparison of MR/ultrasound fusion-guided biopsy with ultrasound-guided biopsy for the diagnosis of prostate cancer. JAMA. Jan 27 2015;313(4):390-7. doi:10.1001/jama.2014.17942
13. Stabile A, Giganti F, Rosenkrantz AB, et al. Multiparametric MRI for prostate cancer diagnosis: current status and future directions. Nat Rev Urol. Jan 2020;17(1):41-61. doi:10.1038/s41585-019-0212-4
14. Chiam K, Carle C, Hughes S, et al. Use of multiparametric magnetic resonance imaging (mpMRI) in active surveillance for low-risk prostate cancer: a scoping review on the benefits and harm of mpMRI in different biopsy scenarios. Prostate Cancer Prostatic Dis. Sep 2021;24(3):662-673. doi:10.1038/s41391-021-00320-9
15. Reske SN, Blumstein NM, Glatting G. [11C]choline PET/CT imaging in occult local relapse of prostate cancer after radical prostatectomy. Eur J Nucl Med Mol Imaging. Jan 2008;35(1):9-17. doi:10.1007/s00259-007-0530-2
16. Kitajima K, Murphy RC, Nathan MA, et al. Detection of recurrent prostate cancer after radical prostatectomy: comparison of 11C-choline PET/CT with pelvic multiparametric MR imaging with endorectal coil. J Nucl Med. Feb 2014;55(2):223-32. doi:10.2967/jnumed.113.123018
17. Parker WP, Davis BJ, Park SS, et al. Identification of Site-specific Recurrence Following Primary Radiation Therapy for Prostate Cancer Using C-11 Choline Positron Emission Tomography /Computed Tomography: A Nomogram for Predicting Extrapelvic Disease. Eur Urol. Mar 2017;71(3):340-348. doi:10.1016/j.eururo.2016.08.055
18. Corfield J, Perera M, Bolton D, Lawrentschuk N. (68)Ga-prostate specific membrane antigen (PSMA) positron emission tomography (PET) for primary staging of high-risk prostate cancer: a systematic review. World J Urol. Apr 2018;36 (4):519-527. doi:10.1007/s00345-018-2182-1
19. Afshar-Oromieh A, Holland-Letz T, Giesel FL, et al. Diagnostic performance of (68)Ga-PSMA-11 (HBED-CC) PET/CT in patients with recurrent prostate cancer: evaluation in 1007 patients. Eur J Nucl Med Mol Imaging. Aug 2017;44(8):1258-1268. doi:10.1007/s00259-017-3711-7
20. Wieder H, Beer AJ, Holzapfel K, et al. 11C-choline PET/CT and whole-body MRI including diffusion-weighted imaging for patients with recurrent prostate cancer. Oncotarget. Sep 12 2017;8(39):66516-66527. doi:10.18632/oncotarget.16227
21. Scobioala S, Kittel C, Wolters H, et al. Diagnostic efficiency of hybrid imaging using PSMA ligands, PET/CT, PET/MRI and MRI in identifying malignant prostate lesions. Ann Nucl Med. May 2021;35(5):628-638. doi:10.1007/s1214 9-021-01606-7
22. Hodge KK, McNeal JE, Terris MK, Stamey TA. Random systematic versus directed ultrasound guided transrectal core biopsies of the prostate. J Urol. Jul 1989;142(1):71-4; discussion 74-5. doi:10. 1016/s0022-5347(17)38664-0
23. Eichler K, Hempel S, Wilby J, Myers L, Bachmann LM, Kleijnen J. Diagnostic value of systematic biopsy methods in the investigation of prostate cancer: a systematic review. J Urol. May 2006;175(5):1605-12. doi:10.1016/S0022-5347(05) 00957-2
24. Jones JS. Saturation biopsy for detecting and characterizing prostate cancer. BJU Int. Jun 2007 ;99(6):1340-4. doi:10.1111/j.1464-410X.2007.06868.x
25. Lane BR, Zippe CD, Abouassaly R, Schoenfield L, Magi-Galluzzi C, Jones JS. Saturation technique does not decrease cancer detection during followup after initial prostate biopsy. J Urol. May 2008;179(5):1746-50; discussion 1750. doi:10.1016 /j.juro.2008.01.049
26. Nelson AW, Harvey RC, Parker RA, Kastner C, Doble A, Gnanapragasam VJ. Repeat prostate biopsy strategies after initial negative biopsy: meta-regression comparing cancer detection of transperineal, transrectal saturation and MRI guided biopsy. PLoS One. 2013;8(2):e57480. doi:10.1371/journal.pone.0057480
27. Ahmed HU, Emberton M, Kepner G, Kepner J. A biomedical engineering approach to mitigate the errors of prostate biopsy. Nat Rev Urol. Feb 7 2012;9(4):227-31. doi:10.1038/nrurol.2012.3
28. Salami SS, Ben-Levi E, Yaskiv O, et al. In patients with a previous negative prostate biopsy and a suspicious lesion on magnetic resonance imaging, is a 12-core biopsy still necessary in addition to a targeted biopsy? BJU Int. Apr 2015;115(4):562-70. doi:10.1111/bju.12938
29. Bhanji Y, Allaway MJ, Gorin MA. Recent Advances and Current Role of Transperineal Prostate Biopsy. Urol Clin North Am. Feb 2021;48 (1):25-33. doi:10.1016/j.ucl.2020.09.010
30. Thomson A, Li M, Grummet J, Sengupta S. Transperineal prostate biopsy: a review of technique. Transl Androl Urol. Dec 2020;9(6):3009-3017. doi:10.21037/tau.2019.12.40
31. Arumainayagam N, Ahmed HU, Moore CM, et al. Multiparametric MR imaging for detection of clinically significant prostate cancer: a validation cohort study with transperineal template prostate mapping as the reference standard. Radiology. Sep 2013;268(3):761-9. doi:10.1148/radiol.13120641
32. Ahmed HU, Kirkham A, Arya M, et al. Is it time to consider a role for MRI before prostate biopsy? Nat Rev Clin Oncol. Apr 2009;6(4):197-206. doi:10. 1038/nrclinonc.2009.18
33. Kong M, Lee L, Mulcahy K, Rajesh A. A single centre service evaluation of the pre-biopsy mpMRI pathway for prostate cancer diagnosis. Journal of Clinical Urology. 2023;16(5):478-489. doi:10.1177/ 20514158211065946
34. Bryant RJ, Hobbs CP, Eyre KS, et al. Comparison of Prostate Biopsy with or without Prebiopsy Multiparametric Magnetic Resonance Imaging for Prostate Cancer Detection: An Observational Cohort Study. J Urol. Mar 2019; 201(3):510-519. doi:10.1016/j.juro.2018.09.049
35. Haffner J, Lemaitre L, Puech P, et al. Role of magnetic resonance imaging before initial biopsy: comparison of magnetic resonance imaging-targeted and systematic biopsy for significant prostate cancer detection. BJU Int. Oct 2011;108(8 Pt 2):E171-8. doi:10.1111/j.1464-410X.2011.10112.x
36. Valerio M, McCartan N, Freeman A, Punwani S, Emberton M, Ahmed HU. Visually directed vs. software-based targeted biopsy compared to transperineal template mapping biopsy in the detection of clinically significant prostate cancer. Urol Oncol. Oct 2015;33(10):424 e9-16. doi:10. 1016/j.urolonc.2015.06.012
37. Watts KL, Frechette L, Muller B, et al. Systematic review and meta-analysis comparing cognitive vs. image-guided fusion prostate biopsy for the detection of prostate cancer. Urol Oncol. Sep 2020;38(9):734 e19-734 e25. doi:10.1016/ j.urolonc.2020.03.020
38. Padhani AR, Barentsz J, Villeirs G, et al. PI-RADS Steering Committee: The PI-RADS Multiparametric MRI and MRI-directed Biopsy Pathway. Radiology. Aug 2019;292(2):464-474. doi:10.1148/radiol.2019182946
39. Drost FH, Osses DF, Nieboer D, et al. Prostate MRI, with or without MRI-targeted biopsy, and systematic biopsy for detecting prostate cancer. Cochrane Database Syst Rev. Apr 25 2019;4(4):CD 012663. doi:10.1002/14651858.CD012663.pub2
40. Tyson MD, Arora SS, Scarpato KR, Barocas D. Magnetic resonance-ultrasound fusion prostate biopsy in the diagnosis of prostate cancer. Urol Oncol. Jul 2016;34(7):326-32. doi:10.1016/j.urolo nc.2016.03.005
41. Mozer P, Roupret M, Le Cossec C, et al. First round of targeted biopsies using magnetic resonance imaging/ultrasonography fusion compared with conventional transrectal ultrasonography-guided biopsies for the diagnosis of localised prostate cancer. BJU Int. Jan 2015;115(1):50-7. doi:10.1111/bju.12690
42. Meng X, Rosenkrantz AB, Mendhiratta N, et al. Relationship Between Prebiopsy Multiparametric Magnetic Resonance Imaging (MRI), Biopsy Indication, and MRI-ultrasound Fusion-targeted Prostate Biopsy Outcomes. Eur Urol. Mar 2016;69( 3):512-7. doi:10.1016/j.eururo.2015.06.005
43. Sonn GA, Chang E, Natarajan S, et al. Value of targeted prostate biopsy using magnetic resonance-ultrasound fusion in men with prior negative biopsy and elevated prostate-specific antigen. Eur Urol. Apr 2014;65(4):809-15. doi:10.1 016/j.eururo.2013.03.025
44. Hoeks CM, Schouten MG, Bomers JG, et al. Three-Tesla magnetic resonance-guided prostate biopsy in men with increased prostate-specific antigen and repeated, negative, random, systematic, transrectal ultrasound biopsies: detection of clinically significant prostate cancers. Eur Urol. Nov 2012;62(5):902-9. doi:10.1016/j.euru ro.2012.01.047
45. Delongchamps NB, Lefevre A, Bouazza N, Beuvon F, Legman P, Cornud F. Detection of significant prostate cancer with magnetic resonance targeted biopsies–should transrectal ultrasound-magnetic resonance imaging fusion guided biopsies alone be a standard of care? J Urol. Apr 2015;193(4):1198-204. doi:10.1016/j.juro .2014.11.002
46. Filson CP, Natarajan S, Margolis DJ, et al. Prostate cancer detection with magnetic resonance-ultrasound fusion biopsy: The role of systematic and targeted biopsies. Cancer. Mar 15 2016;122(6):884-92. doi:10.1002/cncr.29874
47. Ploussard G, Borgmann H, Briganti A, et al. Positive pre-biopsy MRI: are systematic biopsies still useful in addition to targeted biopsies? World J Urol. Feb 2019;37(2):243-251. doi:10.1007/s0034 5-018-2399-z
48. Borofsky S, George AK, Gaur S, et al. What Are We Missing? False-Negative Cancers at Multiparametric MR Imaging of the Prostate. Radiology. Jan 2018;286(1):186-195. doi:10.1148/r adiol.2017152877
49. Richenberg J, Logager V, Panebianco V, Rouviere O, Villeirs G, Schoots IG. The primacy of multiparametric MRI in men with suspected prostate cancer. Eur Radiol. Dec 2019;29(12):6940-6952. doi:10.1007/s00330-019-06166-z
50. Penzkofer T, Tuncali K, Fedorov A, et al. Transperineal in-bore 3-T MR imaging-guided prostate biopsy: a prospective clinical observational study. Radiology. Jan 2015;274(1):170-80. doi:10.1 148/radiol.14140221
51. Elhawary H, Zivanovic A, Rea M, et al. The feasibility of MR-image guided prostate biopsy using piezoceramic motors inside or near to the magnet isocentre. Med Image Comput Comput Assist Interv. 2006;9(Pt 1):519-26. doi:10.1007/ 11866565_64
52. Lagerburg V, Moerland MA, van Vulpen M, Lagendijk JJ. A new robotic needle insertion method to minimise attendant prostate motion. Radiother Oncol. Jul 2006;80(1):73-7. doi:10.1016/ j.radonc.2006.06.013
53. Del Monte M, Cipollari S, Del Giudice F, et al. MRI-directed biopsy for primary detection of prostate cancer in a population of 223 men: MRI In-Bore vs MRI-transrectal ultrasound fusion-targeted techniques. Br J Radiol. Mar 1 2022;95(1131) :20210528. doi:10.1259/bjr.20210528
54. Ramos F, Korets R, Fleishman A, et al. Comparative Effectiveness of Magnetic Resonance Imaging-Ultrasound Fusion Versus In-bore Magnetic Resonance Imaging-targeted Prostate Biopsy. Urology. Jan 2023;171:164-171. doi:10.10 16/j.urology.2022.09.016
55. Prince M, Foster BR, Kaempf A, et al. In-Bore Versus Fusion MRI-Targeted Biopsy of PI-RADS Category 4 and 5 Lesions: A Retrospective Comparative Analysis Using Propensity Score Weighting. AJR Am J Roentgenol. Nov 2021;217 (5):1123-1130. doi:10.2214/AJR.20.25207
56. Heidenreich A, Bastian PJ, Bellmunt J, et al. EAU guidelines on prostate cancer. part 1: screening, diagnosis, and local treatment with curative intent-update 2013. Eur Urol. Jan 2014; 65(1):124-37. doi:10.1016/j.eururo.2013.09.046
57. Wallis CJD, Saskin R, Choo R, et al. Surgery Versus Radiotherapy for Clinically-localized Prostate Cancer: A Systematic Review and Meta-analysis. Eur Urol. Jul 2016;70(1):21-30. doi:10.1016/j.euru ro.2015.11.010
58. Hamdy FC, Donovan JL, Lane JA, et al. Fifteen-Year Outcomes after Monitoring, Surgery, or Radiotherapy for Prostate Cancer. N Engl J Med. Apr 27 2023;388(17):1547-1558. doi:10.1056/NE JMoa2214122
59. Lei JH, Liu LR, Wei Q, et al. Systematic review and meta-analysis of the survival outcomes of first-line treatment options in high-risk prostate cancer. Sci Rep. Jan 12 2015;5:7713. doi:10.1038/srep07713
60. Petrelli F, Vavassori I, Coinu A, Borgonovo K, Sarti E, Barni S. Radical prostatectomy or radiotherapy in high-risk prostate cancer: a systematic review and metaanalysis. Clin Genitourin Cancer. Aug 2014;12(4):215-24. doi:10. 1016/j.clgc.2014.01.010
61. Cooperberg MR, Broering JM, Carroll PR. Time trends and local variation in primary treatment of localized prostate cancer. J Clin Oncol. Mar 1 2010;28(7):1117-23. doi:10.1200/JC O.2009.26.0133
62. Potosky AL, Davis WW, Hoffman RM, et al. Five-year outcomes after prostatectomy or radiotherapy for prostate cancer: the prostate cancer outcomes study. J Natl Cancer Inst. Sep 15 2004;96(18):1358-67. doi:10.1093/jnci/djh259
63. Chen C, Chen Z, Wang K, Hu L, Xu R, He X. Comparisons of health-related quality of life among surgery and radiotherapy for localized prostate cancer: a systematic review and meta-analysis. Oncotarget. Nov 17 2017;8(58):99057-99065. doi:10.18632/oncotarget.21519
64. Sanda MG, Cadeddu JA, Kirkby E, et al. Clinically Localized Prostate Cancer: AUA/ ASTRO/SUO Guideline. Part II: Recommended Approaches and Details of Specific Care Options. J Urol. Apr 2018;199(4):990-997. doi:10.1016/j.juro .2018.01.002
65. Hakimi AA, Feder M, Ghavamian R. Minimally invasive approaches to prostate cancer: a review of the current literature. Urol J. Summer 2007;4(3):130-7.
66. Menon M, Tewari A, Peabody JO, et al. Vattikuti Institute prostatectomy, a technique of robotic radical prostatectomy for management of localized carcinoma of the prostate: experience of over 1100 cases. Urol Clin North Am. Nov 2004;31(4):701-17. doi:10.1016/j.ucl.2004.06.011
67. Passoni NM, Polascik TJ. How to select the right patients for focal therapy of prostate cancer? Curr Opin Urol. May 2014;24(3):203-8. doi:10.10 97/MOU.0000000000000045
68. Blana A, Rogenhofer S, Ganzer R, et al. Eight years’ experience with high-intensity focused ultrasonography for treatment of localized prostate cancer. Urology. Dec 2008;72(6):1329-33; discussion 1333-4. doi:10.1016/j.urology.2008.06.062
69. Lee T, Mendhiratta N, Sperling D, Lepor H. Focal laser ablation for localized prostate cancer: principles, clinical trials, and our initial experience. Rev Urol. 2014;16(2):55-66.
70. Ritch CR, Katz AE. Prostate cryotherapy: current status. Curr Opin Urol. Mar 2009;19(2):177-81. doi:10.1097/mou.0b013e32831e16ce
71. Punnen S, Cooperberg MR, D’Amico AV, et al. Management of biochemical recurrence after primary treatment of prostate cancer: a systematic review of the literature. Eur Urol. Dec 2013;64 (6):905-15. doi:10.1016/j.eururo.2013.05.025
72. Fainberg JS, Al Hussein Al Awamlh B, DeRosa AP, et al. A systematic review of outcomes after thermal and nonthermal partial prostate ablation. Prostate Int. Dec 2021;9(4):169-175. doi:10.1016/j. prnil.2021.04.001
73. Budaus L, Spethmann J, Isbarn H, et al. Inverse stage migration in patients undergoing radical prostatectomy: results of 8916 European patients treated within the last decade. BJU Int. Oct 2011;1 08(8):1256-61. doi:10.1111/j.1464-410X.2010.09982.x
74. Muller BG, van den Bos W, Pinto PA, de la Rosette JJ. Imaging modalities in focal therapy: patient selection, treatment guidance, and follow-up. Curr Opin Urol. May 2014;24(3):218-24. doi:10.1097/MOU.0000000000000041
75. Stephenson AJ, Scardino PT, Bianco FJ, Jr., Eastham JA. Salvage therapy for locally recurrent prostate cancer after external beam radiotherapy. Curr Treat Options Oncol. Oct 2004;5(5):357-65. doi:10.1007/s11864-004-0026-2
76. Tacke J, Adam G, Haage P, Sellhaus B, Grosskortenhaus S, Gunther RW. MR-guided percutaneous cryotherapy of the liver: in vivo evaluation with histologic correlation in an animal model. J Magn Reson Imaging. Jan 2001;13(1):50-6. doi:10.1002/1522-2586(200101)13:1<50::aid-jmri1008>3.0.co;2-a
77. Tuncali K, Morrison PR, Tatli S, Silverman SG. MRI-guided percutaneous cryoablation of renal tumors: use of external manual displacement of adjacent bowel loops. Eur J Radiol. Aug 2006;59 (2):198-202. doi:10.1016/j.ejrad.2006.04.013
78. Josan S, Bouley DM, van den Bosch M, Daniel BL, Butts Pauly K. MRI-guided cryoablation: In vivo assessment of focal canine prostate cryolesions. J Magn Reson Imaging. Jul 2009;30(1):169-76. doi:1 0.1002/jmri.21827
79. van den Bosch MA, Josan S, Bouley DM, et al. MR imaging-guided percutaneous cryoablation of the prostate in an animal model: in vivo imaging of cryoablation-induced tissue necrosis with immediate histopathologic correlation. J Vasc Interv Radiol. Feb 2009;20(2):252-8. doi:10.1016 /j.jvir.2008.10.030
80. Gangi A, Tsoumakidou G, Abdelli O, et al. Percutaneous MR-guided cryoablation of prostate cancer: initial experience. Eur Radiol. Aug 2012; 22(8):1829-35. doi:10.1007/s00330-012-2411-8
81. Woodrum DA, Kawashima A, Karnes RJ, et al. Magnetic resonance imaging-guided cryoablation of recurrent prostate cancer after radical prostatectomy: initial single institution experience. Urology. Oct 2013;82(4):870-5. doi:10.1016/j.urol ogy.2013.06.011
82. de Marini P, Cazzato RL, Garnon J, et al. Percutaneous MR-guided prostate cancer cryoablation technical updates and literature review. BJR Open. 2019;1(1):20180043. doi:10.12 59/bjro.20180043
83. McNichols RJ, Gowda A, Kangasniemi M, Bankson JA, Price RE, Hazle JD. MR thermometry-based feedback control of laser interstitial thermal therapy at 980 nm. Lasers Surg Med. 2004;34 (1):48-55. doi:10.1002/lsm.10243
84. Hynynen K, Freund WR, Cline HE, et al. A clinical, noninvasive, MR imaging-monitored ultrasound surgery method. Radiographics. Jan 1996;16(1) :185-95. doi:10.1148/radiographics.16.1.185
85. Ishihara Y, Calderon A, Watanabe H, et al. A precise and fast temperature mapping using water proton chemical shift. Magn Reson Med. Dec 1995;34(6):814-23. doi:10.1002/mrm.1910340606
86. Vitkin IA, Moriarty JA, Peters RD, et al. Magnetic resonance imaging of temperature changes during interstitial microwave heating: a phantom study. Med Phys. Feb 1997;24(2):269-77. doi:10.1118/1.598096
87. Sapareto SA, Dewey WC. Thermal dose determination in cancer therapy. Int J Radiat Oncol Biol Phys. Jun 1984;10(6):787-800. doi:10.1016/ 0360-3016(84)90379-1
88. Zhu M, Sun Z, Ng CK. Image-guided thermal ablation with MR-based thermometry. Quant Imaging Med Surg. Jun 2017;7(3):356-368. doi:10. 21037/qims.2017.06.06
89. McNichols RJ, Gowda, A., Gelnett, M. D., Stafford, R. J. Percutaneous MRI-guided laser thermal therapy in canine prostate. Progress in Biomedical Optics and Imaging – Proceedings of SPIE. 2005;5686:214-225. doi:10.1117/12.587747
90. Stafford RJ, Shetty A, Elliott AM, et al. Magnetic resonance guided, focal laser induced interstitial thermal therapy in a canine prostate model. J Urol. Oct 2010;184(4):1514-20. doi:10.10 16/j.juro.2010.05.091
91. Woodrum DA, Gorny KR, Mynderse LA, et al. Feasibility of 3.0T magnetic resonance imaging-guided laser ablation of a cadaveric prostate. Urology. Jun 2010;75(6):1514 e1-6. doi:10.1016/ j.urology.2010.01.059
92. Raz O, Haider MA, Davidson SR, et al. Real-time magnetic resonance imaging-guided focal laser therapy in patients with low-risk prostate cancer. Eur Urol. Jul 2010;58(1):173-7. doi:10.1016 /j.eururo.2010.03.006
93. Natarajan S, Raman S, Priester AM, et al. Focal Laser Ablation of Prostate Cancer: Phase I Clinical Trial. J Urol. Jul 2016;196(1):68-75. doi:10.1016 /j.juro.2015.12.083
94. Thuroff S, Chaussy C, Vallancien G, et al. High-intensity focused ultrasound and localized prostate cancer: efficacy results from the European multicentric study. J Endourol. Oct 2003;17(8):673-7. doi:10.1089/089277903322518699
95. Gelet A, Chapelon JY, Bouvier R, et al. Transrectal high-intensity focused ultrasound: minimally invasive therapy of localized prostate cancer. J Endourol. Aug 2000;14(6):519-28. doi:10 .1089/end.2000.14.519
96. Gelet A, Chapelon JY, Bouvier R, Rouviere O, Lyonnet D, Dubernard JM. Transrectal high intensity focused ultrasound for the treatment of localized prostate cancer: factors influencing the outcome. Eur Urol. Aug 2001;40(2):124-9. doi:10. 1159/000049761
97. Uchida T, Tomonaga T, Kim H, et al. Improved outcomes with advancements in high intensity focused ultrasound devices for the treatment of localized prostate cancer. J Urol. Jan 2015;193 (1):103-10. doi:10.1016/j.juro.2014.07.096
98. Crouzet S, Chapelon JY, Rouviere O, et al. Whole-gland ablation of localized prostate cancer with high-intensity focused ultrasound: oncologic outcomes and morbidity in 1002 patients. Eur Urol. May 2014;65(5):907-14. doi:10.1016/j.eururo.2013.04.039
99. van Velthoven R, Aoun F, Marcelis Q, et al. A prospective clinical trial of HIFU hemiablation for clinically localized prostate cancer. Prostate Cancer Prostatic Dis. Mar 2016;19(1):79-83. doi:10.1038 /pcan.2015.55
100. Profound Medical Receives U.S. FDA 510(k) Clearance for TULSA-PRO®. Global News Wire. https://www.globenewswire.com/news-release/2019/08/16/1903004/0/en/Profound-Medical-Receives-U-S-FDA-510-k-Clearance-for-TULSA-PRO.html
101. Klotz L PD, Chin J, Pavlovich C, Relle J, Koch M, et al. LBA20 MRI-GUIDED TRANSURETHRAL ULTRASOUND ABLATION (TULSA) IN PATIENTS WITH LOCALIZED PROSTATE CANCER: PRELIMINARY RESULTS OF TACT PIVOTAL STUDY. Journal of Urology 2018;199(4S):e1077–8. doi: https://doi.org/10.1016/j.juro.2018.03.091
102. Ehdaie B, Tempany CM, Holland F, et al. MRI-guided focused ultrasound focal therapy for patients with intermediate-risk prostate cancer: a phase 2b, multicentre study. Lancet Oncol. Jul 2022;23(7):910-918. doi:10.1016/S1470-2045(22)0 0251-0
103. INSIGHTEC ANNOUNCES FDA CLEARANCE FOR EXABLATE PROSTATE TO TREAT PROSTATE TISSUE. Insightec. https://insightec.com/news/insightec-announces-fda-clearance-for-exablate-prostate/
104. Shore ND, Moul JW, Pienta KJ, Czernin J, King MT, Freedland SJ. Biochemical recurrence in patients with prostate cancer after primary definitive therapy: treatment based on risk stratification. Prostate Cancer Prostatic Dis. Jun 2024;27(2):192-201. doi:10.1038/s41391-023-00712-z
105. Stephenson AJ, Slawin KM. The value of radiotherapy in treating recurrent prostate cancer after radical prostatectomy. Nat Clin Pract Urol. Dec 2004;1(2):90-6. doi:10.1038/ncpuro0056
106. Brandeis J, Pashos CL, Henning JM, Litwin MS. A nationwide charge comparison of the principal treatments for early stage prostate carcinoma. Cancer. Oct 15 2000;89(8):1792-9.
107. Sella T, Schwartz LH, Swindle PW, et al. Suspected local recurrence after radical prostatectomy: endorectal coil MR imaging. Radiology. May 2004;231(2):379-85. doi:10.1148/ radiol.2312030011
108. Agarwal PK, Sadetsky N, Konety BR, Resnick MI, Carroll PR, Cancer of the Prostate Strategic Urological Research E. Treatment failure after primary and salvage therapy for prostate cancer: likelihood, patterns of care, and outcomes. Cancer. Jan 15 2008;112(2):307-14. doi:10.1002/cncr.23161
109. Kuban DA, Thames HD, Levy LB, et al. Long-term multi-institutional analysis of stage T1-T2 prostate cancer treated with radiotherapy in the PSA era. Int J Radiat Oncol Biol Phys. Nov 15 2003;57(4):915-28. doi:10.1016/s0360-3016(03)00632-1
110. Kramer S, Gorich J, Gottfried HW, et al. Sensitivity of computed tomography in detecting local recurrence of prostatic carcinoma following radical prostatectomy. Br J Radiol. Oct 1997;70(83 8):995-9. doi:10.1259/bjr.70.838.9404201
111. Connolly JA, Shinohara K, Presti JC, Jr., Carroll PR. Local recurrence after radical prostatectomy: characteristics in size, location, and relationship to prostate-specific antigen and surgical margins. Urology. Feb 1996;47(2):225-31. doi:10.1016/S009 0-4295(99)80421-X
112. Leventis AK, Shariat SF, Slawin KM. Local recurrence after radical prostatectomy: correlation of US features with prostatic fossa biopsy findings. Radiology. May 2001;219(2):432-9. doi:10.1148/ radiology.219.2.r01ma20432
113. Linder BJ, Kawashima A, Woodrum DA, et al. Early localization of recurrent prostate cancer after prostatectomy by endorectal coil magnetic resonance imaging. Can J Urol. Jun 2014;21 (3):7283-9.
114. Roy C, Foudi F, Charton J, et al. Comparative sensitivities of functional MRI sequences in detection of local recurrence of prostate carcinoma after radical prostatectomy or external-beam radiotherapy. AJR Am J Roentgenol. Apr 2013; 200(4):W361-8. doi:10.2214/AJR.12.9106
115. May EJ, Viers LD, Viers BR, et al. Prostate cancer post-treatment follow-up and recurrence evaluation. Abdom Radiol (NY). May 2016;41(5): 862-76. doi:10.1007/s00261-015-0562-1
116. Kitajima K, Hartman RP, Froemming AT, Hagen CE, Takahashi N, Kawashima A. Detection of Local Recurrence of Prostate Cancer After Radical Prostatectomy Using Endorectal Coil MRI at 3 T: Addition of DWI and Dynamic Contrast Enhancement to T2-Weighted MRI. AJR Am J Roentgenol. Oct 2015;205(4):807-16. doi:10.2214/ AJR.14.14275
117. Amling CL, Blute ML, Bergstralh EJ, Seay TM, Slezak J, Zincke H. Long-term hazard of progression after radical prostatectomy for clinically localized prostate cancer: continued risk of biochemical failure after 5 years. J Urol. Jul 2000;164(1):101-5.
118. Bianco FJ, Jr., Scardino PT, Stephenson AJ, Diblasio CJ, Fearn PA, Eastham JA. Long-term oncologic results of salvage radical prostatectomy for locally recurrent prostate cancer after radiotherapy. Int J Radiat Oncol Biol Phys. Jun 1 2005;62(2):448-53. doi:10.1016/j.ijrobp.2004.09.049
119. Boris RS, Bhandari A, Krane LS, Eun D, Kaul S, Peabody JO. Salvage robotic-assisted radical prostatectomy: initial results and early report of outcomes. BJU Int. Apr 2009;103(7):952-6. doi:10.1111/j.1464-410X.2008.08245.x
120. Kimura M, Mouraviev V, Tsivian M, Mayes JM, Satoh T, Polascik TJ. Current salvage methods for recurrent prostate cancer after failure of primary radiotherapy. BJU Int. Jan 2010;105(2):191-201. doi:10.1111/j.1464-410X.2009.08715.x
121. Chade DC, Shariat SF, Cronin AM, et al. Salvage radical prostatectomy for radiation-recurrent prostate cancer: a multi-institutional collaboration. Eur Urol. Aug 2011;60(2):205-10. doi:10.1016/j.eururo.2011.03.011
122. De Groote R, Nathan A, De Bleser E, et al. Techniques and Outcomes of Salvage Robot-Assisted Radical Prostatectomy (sRARP). Eur Urol. Dec 2020;78(6):885-892. doi:10.1016/j.eururo.2020.05.003
123. Grado GL, Collins JM, Kriegshauser JS, et al. Salvage brachytherapy for localized prostate cancer after radiotherapy failure. Urology. Jan 1999;53(1):2-10. doi:Doi 10.1016/S0090-4295(98)0 0492-0
124. Koutrouvelis P, Hendricks F, Lailas N, et al. Salvage reimplantation in patient with local recurrent prostate carcinoma after brachytherapy with three dimensional computed tomography-guided permanent pararectal implant. Technol Cancer Res Treat. Aug 2003;2(4):339-44. doi:10.11 77/153303460300200409
125. Kollmeier MA, McBride S, Taggar A, et al. Salvage brachytherapy for recurrent prostate cancer after definitive radiation therapy: A comparison of low-dose-rate and high-dose-rate brachytherapy and the importance of prostate-specific antigen doubling time. Brachytherapy. Nov-Dec 2017;16(6):1091-1098. doi:10.1016/j.bra chy.2017.07.013
126. Zaine H, Vandendorpe B, Bataille B, et al. Salvage Radiotherapy for Macroscopic Local Recurrence Following Radical Prostatectomy. Front Oncol. 2021;11:669261. doi:10.3389/fonc.2021.669261
127. Murat FJ, Poissonnier L, Rabilloud M, et al. Mid-term results demonstrate salvage high-intensity focused ultrasound (HIFU) as an effective and acceptably morbid salvage treatment option for locally radiorecurrent prostate cancer. Eur Urol. Mar 2009;55(3):640-7. doi:10.1016/j.eururo.2008.04.091
128. Zacharakis E, Ahmed HU, Ishaq A, et al. The feasibility and safety of high-intensity focused ultrasound as salvage therapy for recurrent prostate cancer following external beam radiotherapy. BJU Int. Sep 2008;102(7):786-92. doi:10.1111/j.1464-410X.2008.07775.x
129. Gelet A, Chapelon JY, Poissonnier L, et al. Local recurrence of prostate cancer after external beam radiotherapy: early experience of salvage therapy using high-intensity focused ultrasonography. Urology. Apr 2004;63(4):625-9. doi:10.1016/j.urolo gy.2004.01.002
130. Crouzet S, Blana A, Murat FJ, et al. Salvage high-intensity focused ultrasound (HIFU) for locally recurrent prostate cancer after failed radiation therapy: Multi-institutional analysis of 418 patients. BJU Int. Jun 2017;119(6):896-904. doi:10.1111/bju .13766
131. Maestroni U, Tafuri A, Dinale F, Campobasso D, Antonelli A, Ziglioli F. Oncologic outcome of salvage high-intensity focused ultrasound (HIFU) in radiorecurrent prostate cancer. A systematic review. Acta Biomed. Sep 2 2021;92(4):e2021191. doi:10.23750/abm.v92i3.11475
132. Chin JL, Pautler SE, Mouraviev V, Touma N, Moore K, Downey DB. Results of salvage cryoablation of the prostate after radiation: identifying predictors of treatment failure and complications. J Urol. Jun 2001;165(6 Pt 1):1937-41; discussion 1941-2. doi:10.1097/00005392-200 106000-00022
133. Siddiqui SA ML, Zincke H, Hoffmann NE, Lobo JR, Wilson TM. Treatment of prostate cancer local recurrence after radical retropubic prostatectomy with 17-guage interstitial transperineal cryoablation: initial experience. Urology. 2007;70(117)
134. Pisters LL, Rewcastle JC, Donnelly BJ, Lugnani FM, Katz AE, Jones JS. Salvage prostate cryoablation: initial results from the cryo on-line data registry. J Urol. Aug 2008;180(2):559-63; discussion 563-4. doi:10.1016/j.juro.2008.04.005
135. Wenske S, Quarrier S, Katz AE. Salvage cryosurgery of the prostate for failure after primary radiotherapy or cryosurgery: long-term clinical, functional, and oncologic outcomes in a large cohort at a tertiary referral centre. Eur Urol. Jul 2013;64(1):1-7. doi:10.1016/j.eururo.2012.07.008
136. Chin YF, Lynn N. Systematic Review of Focal and Salvage Cryotherapy for Prostate Cancer. Cureus. Jun 2022;14(6):e26400. doi:10.7759/cureus.26400
137. Uchida T, Shoji S, Nakano M, et al. High-intensity focused ultrasound as salvage therapy for patients with recurrent prostate cancer after external beam radiation, brachytherapy or proton therapy. BJU Int. Feb 2011;107(3):378-82. doi:10.1 111/j.1464-410X.2010.09518.x
138. Bomers JG, Yakar D, Overduin CG, et al. MR imaging-guided focal cryoablation in patients with recurrent prostate cancer. Radiology. Aug 2013;268(2):451-60. doi:10.1148/radiol.13121291
139. Overduin CG, Jenniskens SFM, Sedelaar JPM, Bomers JGR, Futterer JJ. Percutaneous MR-guided focal cryoablation for recurrent prostate cancer following radiation therapy: retrospective analysis of iceball margins and outcomes. Eur Radiol. Nov 2017;27(11):4828-4836. doi:10.1007/s00330-017-4833-9
140. Porter CAt, Woodrum DA, Callstrom MR, et al. MRI after technically successful renal cryoablation: early contrast enhancement as a common finding. AJR Am J Roentgenol. Mar 2010;194(3):790-3. doi:10.2214/AJR.09.2518
141. Gage AA, Baust J. Mechanisms of tissue injury in cryosurgery. Cryobiology. Nov 1998;37(3):171-86. doi:10.1006/cryo.1998.2115
142. Favazza CP, Gorny KR, King DM, et al. An investigation of the effects from a urethral warming system on temperature distributions during cryoablation treatment of the prostate: a phantom study. Cryobiology. Aug 2014;69(1):128-33. doi:10 .1016/j.cryobiol.2014.06.004
143. Butts K, Sinclair J, Daniel BL, Wansapura J, Pauly JM. Temperature quantitation and mapping of frozen tissue. J Magn Reson Imaging. Jan 2001;13(1):99-104. doi:10.1002/1522-2586(20010 1)13:1<99::aid-jmri1015>3.0.co;2-o
144. Wansapura JP, Daniel BL, Vigen KK, Butts K. In vivo MR thermometry of frozen tissue using R2* and signal intensity. Acad Radiol. Sep 2005; 12(9):1080-4. doi:10.1016/j.acra.2005.06.006
145. Lu A, Daniel BL, Pauly JM, Pauly KB. Improved slice selection for R2* mapping during cryoablation with eddy current compensation. J Magn Reson Imaging. Jul 2008;28(1):190-8. doi:10.1002/jmri.21396
146. Soher BJ, Wyatt C, Reeder SB, MacFall JR. Noninvasive temperature mapping with MRI using chemical shift water-fat separation. Magn Reson Med. May 2010;63(5):1238-46. doi:10.1002/mrm.22310
147. Alabousi M, Ghai S, Haider MA. MRI-guided Minimally Invasive Focal Therapies for Prostate Cancer. Radiology. Dec 2023;309(3):e230431. doi: 10.1148/radiol.230431