

Multidisciplinary Approach to Apical Dehiscence Management
Multidisciplinary Management of Apical Dehiscence and Mucosal Fenestration on a Mandibular Incisor Using Cone-Beam Computed Tomography-Guided Periodontal Regenerative Therapy: A Case Report
Ahmad Soolari, DMD, MS1
- Adjunct Professor, West Virginia University, Depart of Periodontics, School of Dentistry; Morgantown, WV 26506.
Email: [email protected]
OPEN ACCESS
PUBLISHED 31 December 2025
CITATION: Soolari, A., 2025. Multidisciplinary Management of Apical Dehiscence and Mucosal Fenestration on a Mandibular Incisor Using Cone- Beam Computed Tomography- Guided Periodontal Regenerative Therapy: A Case Report. Medical Research Archives, [online] 13(12). https://doi.org/10.18103/mra.v 13i12.7122
COPYRIGHT: © 2025 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v 13i12.7122
ISSN 2375-1924
ABSTRACT
Apical dehiscence is a bony defect on the buccal root surface that exposes the root without involving the marginal alveolar bone, often resulting from adverse tooth position, trauma, or orthodontic movement. This report details the multidisciplinary management of a combined endo-perio lesion presenting as a persistent mucosal fenestration at the apex of an endodontically treated mandibular incisor, tooth #24, in a 51-year-old female patient. A two-dimensional (2D) radiograph failed to reveal the extent of the defect, but a Cone-Beam Computed Tomography scan provided a definitive three-dimensional (3D) diagnosis: the root apex was positioned outside the labial cortical plate, exhibiting severe apical dehiscence. Given the thin bone and severe depression defect, the option of extraction and implant placement was ruled out. The case was successfully resolved through endodontic microsurgery, root end refinement, combined with Periodontal Regenerative Therapy, utilizing a bone graft for hard tissue augmentation and a Subepithelial Connective Tissue Graft for stable soft tissue repair. This report illustrates the critical role of advanced imaging for accurate diagnosis and treatment planning in managing complex apical fenestrations and affirms the long-term value of tooth preservation.
Keywords:
- Mucosal Fenestration
- Apical Dehiscence
- Cone-Beam Computed Tomography (CBCT)
- Periodontal Regenerative Therapy (PRT)
- Combined Endo-Perio Lesion
- Tooth Preservation
- 3D Imaging
- Subepithelial Connective Tissue Graft (SCTG)
CASE REPORT
Introduction
The diagnosis and treatment of lesions involving both the endodontium and periodontium—classified as combined endo-perio lesions—represent a complex clinical challenge. An apical dehiscence or fenestration is a specific anatomical defect of the alveolar bone, typically on the labial aspect, resulting in an area of denuded root surface. When this defect occurs on an endodontically compromised tooth, the associated chronic inflammation can lead to the breakdown of overlying soft tissue, manifesting as a mucosal fenestration—a visible breach in the mucosa at the root apex.
Anatomical factors, particularly the severe buccolingual inclination of the root, have been significantly correlated with the presence of these dehiscence and fenestration defects. Traditional 2D periapical radiography is inherently limited by geometric distortion and superimposition, often masking the true three-dimensional morphology and extent of these osseous defects. Therefore, the enhanced resolution and minimal artifacts offered by Cone-Beam Computed Tomography (CBCT) technology are becoming increasingly indispensable for diagnosis and predictable treatment planning in modern periodontology.
The long-term prognosis for preserving a periodontally and endodontically compromised tooth must be critically weighed against the option of extraction and implant replacement. Literature supports that when a favorable prognosis can be achieved through intervention, tooth preservation is often the more biologically and cost-effective approach. This case report details the successful treatment of a chronic combined lesion presenting as a mucosal fenestration on a mandibular incisor, emphasizing the decisive role of CBCT-guided diagnosis and subsequent Periodontal Regenerative Therapy (PRT) using connective tissue graft.
Case Presentation
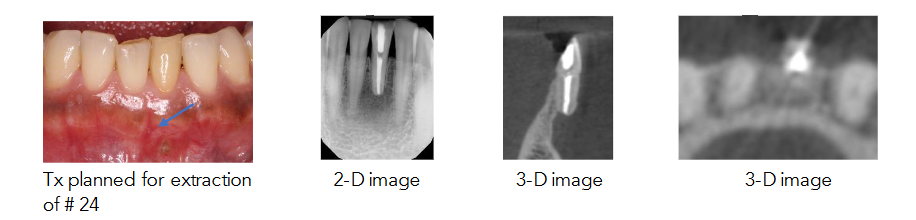
A 51-year-old Asian American female was referred to the office for evaluation and treatment of an apical dehiscence at tooth #24, mandibular left central incisor. The patient presented with a persistent, unhealed region and heavy hard deposits at the exposed apex. Pre-operative clinical examination revealed a localized mucosal fenestration at the apex of the tooth, indicated by an arrowhead in the clinical photo.
A CBCT scan was performed to facilitate diagnosis. The 3D imaging confirmed that the tooth, which had previously undergone endodontic treatment, exhibited a root length shorter than the adjacent tooth #25, suggestive of prior apical surgery. Crucially, the axial and cross-sectional views disclosed that the long axis of the tooth was tilted lingually at the incisal, resulting in the apical root segment being completely outside of the labial cortical plate—a severe apical dehiscence/fenestration defect. The labial bone surface displayed a deep, localized depression outlined by a thin, well-defined layer of cortical bone.
Based on the CBCT findings—specifically the extremely thin bone in the buccolingual dimension and the severe apical depression defect—the initial treatment plan considered by the referring dentist, which involved extraction and immediate implant placement, was determined to be contraindicated. The absence of sufficient hard tissue necessitated a reconstructive approach.
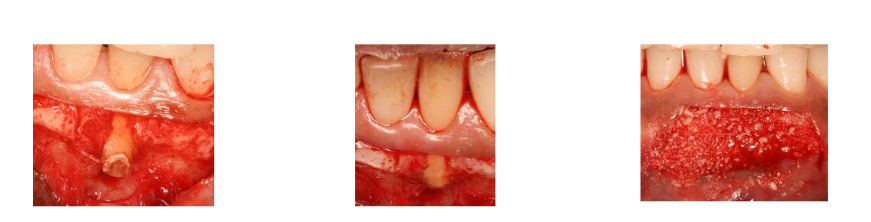
The patient accepted a revised treatment plan focused on tooth preservation using PRT. The surgical procedure involved a full-thickness flap elevation, which exposed the root end. The exposed root end was carefully flattened and smoothed to remove irritants and create a favorable recipient site for regeneration, as described in literature for managing similar defects.
After reflection of the full-thickness flap, the labial concavity was filled with bone graft (FDBA) followed by a Subepithelial Connective Tissue Graft (SCTG), which was obtained from the tuberosity. To achieve predictable root coverage, increase the width of keratinized tissue, and enhance esthetics, SCTG was utilized. SCTG is considered the gold standard technique for increasing the width and thickness of keratinized tissue (KT) and achieving predictable long-term complete root coverage (CRC). The autogenous graft was harvested from the tuberosity region, providing a rich source of cells, growth factors, and extracellular matrix that promote superior healing and tissue regeneration. The graft and flap were stabilized using fine non-resorbable sutures, 6-0 PTFE (polytetrafluoroethylene), which ensures meticulous, tension-free flap closure and stabilization of the regenerative materials, critical for healing and primary intention closure.
Post-operative recovery was uneventful, and clinical follow-up demonstrated complete root coverage and resolution of the mucosal fenestration.
Discussion and Analysis
The successful management of this persistent mucosal fenestration hinged on three key analytical pillars: accurate diagnosis, evidenced-based treatment selection, and meticulous surgical execution.
- Diagnostic Imperative: The Role of Cone-Beam Computed Tomography
The fundamental challenge in this case was the inadequate two-dimensional (2D) depiction of the osseous defect. Conventional periapical radiography failed to characterize the buccolingual extent of the lesion, a known limitation due to anatomical superimposition. The CBCT scan was, therefore, not merely a supplementary tool but a critical diagnostic necessity. The cross-sectional and axial views definitively revealed the severe apical dehiscence of tooth #24, with the apex positioned entirely outside the labial cortical plate. This visualization was essential for quantifying the minimal remaining bone width and accurately delineating the surrounding deep depression defect. Without this precise three-dimensional (3D) roadmap, the true complexity of the hard tissue deficiency would have remained masked, potentially leading to a flawed treatment strategy. - Etiological Correlation and Defect Classification
The CBCT findings allowed for a precise etiological and morphological analysis. The image confirmed a lingual tilt of the tooth’s long axis, a key contributing factor highly correlated with the formation of labial dehiscence and fenestration defects in the anterior mandible. This anatomical predisposition, exacerbated by the chronic inflammatory process of the combined endo-perio lesion, led to the breakdown of the already thin labial cortical plate and the resultant mucosal fenestration. The defect was confirmed as a true apical fenestration requiring both endodontic stabilization, root end refinement, and aggressive periodontal reconstruction. - Treatment Rationale: Preservation versus Replacement
The detailed CT analysis was pivotal in the critical decision to pursue tooth preservation rather than extraction and replacement. Given the severe lack of native labial bone and the depth of the apical depression, immediate implant placement was technically infeasible. Even delayed placement would have necessitated significant, multi-stage bone augmentation with an inherently less predictable outcome. Our approach aligns with the current evidence favoring the retention of periodontally and endodontically compromised teeth when a predictable prognosis can be achieved. Furthermore, systematic reviews confirm that the long-term maintenance costs and biological complications associated with dental implants can often surpass the expenses of maintaining a successfully treated natural tooth, supporting the rationale for preservation from a biological and cost-effectiveness perspective. - Surgical and Regenerative Analysis: The SCTG Gold Standard
The successful reconstruction of both the hard and soft tissue deficiencies necessitated a rigorous, two-pronged regenerative strategy:- Hard Tissue Regeneration (GBR): Following flap reflection and root end refinement, the apical bony concavity was treated with Guided Bone Regeneration (GBR), utilizing FDBA (freeze-dried bone allograft) bone graft. This step provided the necessary scaffolding to correct the apical dehiscence defect and recreate the lost alveolar bone structure.
- Soft Tissue Augmentation (SCTG): The most critical step for predictable, stable, and aesthetic long-term soft tissue repair was the use of the Subepithelial Connective Tissue Graft (SCTG), harvested from the maxillary tuberosity. SCTG remains the gold standard technique for soft tissue augmentation due to its high predictability for increasing gingival thickness and achieving complete root coverage. In the thin periodontal biotype of the mandibular anterior region, the SCTG was vital to:
- Protect the Underlying Graft: The SCTG provided a robust, vascularized covering to shield the bone graft material, promoting undisturbed healing of the hard tissue.
- Augment Tissue Thickness: SCTG increased the gingival thickness, which is crucial for long-term stability and resistance to future recession, ensuring the final restorative result is durable.
- Enhance Esthetics: The biotype augmentation provided by the SCTG optimizes the final aesthetic outcome by achieving harmonious color and contour matching.
The meticulous surgical technique, involving the stabilization of the graft and flap using fine non-resorbable PTFE sutures, ensured tension-free primary closure. This is a fundamental requirement for the biological success of both GBR and SCTG integration. The favorable clinical outcome validates the efficacy of this combined CBCT-guided regenerative approach in managing complex apical dehiscence defects.
Conclusion
This case report demonstrates the successful diagnosis and treatment of a severe apical dehiscence and mucosal fenestration on an endodontically treated tooth, which was managed through Cone-Beam Computed Tomography-guided Periodontal Regenerative Therapy. CBCT proved essential as a diagnostic tool, facilitating a definitive 3D diagnosis of the osseous defect and preventing an unnecessary and complicated extraction and implant procedure. The utilization of a Subepithelial Connective Tissue Graft (SCTG) combined with bone grafting was key to reconstructing both the hard and soft tissue deficiencies. The successful outcome, characterized by complete root coverage and patient satisfaction, confirms that for complex anatomical defects such as apical fenestrations, combining precise diagnostics with established periodontal regenerative techniques provides a predictable and valuable alternative for tooth preservation.
Conflict of Interest Statement:
None.
Funding Statement:
None.
Acknowledgements:
None.

References:
- Rajesh KS, Chaurasia K, Apoorva K, Srivastava S. Treating apical fenestration in a previously endodontically treated tooth. J Conserv Dent Endo. 2024;27(11):1193-1195.
- Ferrari CH, Silva M, Ribeiro R. Correlation between Tooth Position Parameters and Apical Fenestration: A Cone-Beam Computed Tomography Study. Methodos Protoc. 2024;7(1):14.
- Coskun I, Kaya B. Appraisal of the relationship between tooth inclination, dehiscence, fenestration, and sagittal skeletal pattern with cone beam computed tomography. Angle Orthod. 2019;89(4):544-551.
- Adam M. ‘Combined endo-perio lesions’ – what is the best treatment? Evid Based Dent. 2021;22(4):158-159.
- Shikha T, Narendranath A, Jayashankar K, Sharma P, Guptha M. Management of isolated labial mucosal fenestration by endodontic microsurgery along with platelet-rich fibrin and connective tissue graft: a series of four cases. Clin Adv Periodontics. 2022;12(3):194-203.
- Walter C, Weiger R, Zitzmann NU. Cone beam computed tomography (CBCT) for diagnosis and treatment planning in periodontology: systematic review update. Clin Oral Investig. 2020;24(9):2943-2958.
- Eshraghi VT, Malloy KA, Tahmasebi M. Role of Cone-Beam Computed Tomography in the Management of Periodontal Disease. Dent J (Basel). 2019;7(2):57.
- Verykokou C, Theoharatos C, Tsalikis L. CBCT-Based Design of Patient-Specific 3D Bone Grafts for Periodontal Regeneration. J Clin Med. 2023;12(15):5023.
- Nagpal D, Garlapati D, Chhabra V, Chhabra A. The cost-effectiveness of tooth preservation vs implant placement in severe periodontal disease patients: a systematic review. Quintessence Int. 2024;55(1):76-85.
- Bentour E, etal. The Decision Between Tooth Retention or Replacement with Implants: A Continuing Dilemma. Dentistry Journal. 2025;13(3):99.
- Park W, Park W, Lim S, Han J. Periodontal Phenotype Modification Using Subepithelial Connective Tissue Graft and Bone Graft in the Mandibular Anterior Teeth with Mucogingival Problems Following Orthodontic Treatment. Medicina (Kaunas). 2023;59(3):584.
- Bharti, Ramesh, Etal. Management of mucosal fenestration with external root resorption by multidisciplinary approach. BMJ Case Rep. 2014 Oct 9:2014:bcr2014206259.
- Rajula MPB, Etal. Gingival Fenestration Management: A Rarefied Case Entity and Literature Review. J Pharm Bioallied Sci. 2020 Aug;12(Suppl 1):S648-S651.