





Multidisciplinary Management of Renal Angiomyolipoma
Multidisciplinary Approach to a Complicated Renal Angiomyolipoma: A Case Report Review
Aisha K. Kawafie1, Zeina H. Kalaji2, Ahmed M. Ibrahim3, Efria M. Emtair4, and Talal F. Al-Rabadi5
- Department of Nephrology, Royal Bahrain Hospital, Bahrain.
- Department of Medicine, University of Jordan, Amman, Jordan.
- Department of Interventional Radiology, Royal Bahrain Hospital, Bahrain.
- Department of Urology, Royal Bahrain Hospital, Bahrain.
- Department of Nephrology, University of Utah Hospital, UT, USA.
OPEN ACCESS
PUBLISHED: 31 October 2024
CITATION: Kawalti, I.A., Kalaji, Z.H., et al., 2024. Multidisciplinary Approach to a Complicated Renal Angiomyolipoma: A Case Report Review. Medical Research Archives, [online] 12(10).
https://doi.org/10.18103/mra.v12i10.5880
COPYRIGHT: © 2024 European Society of Medicine. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI https://doi.org/10.18103/mra.v12i10.5880
ISSN 2375-1924
ABSTRACT
Angiomyolipoma (AML) is a benign kidney tumor composed of fat tissue, smooth muscle cells, and significant neovascularization, which can lead to spontaneous hemorrhage, causing hematuria and/or retroperitoneal hematoma with back pain. While nephrectomy can be a first-line treatment, embolization is an effective, less invasive alternative. We present a 41-year-old male admitted with left flank pain. Initial ultrasound revealed a heterogeneous hyperechoic mass in the right kidney, and subsequent CT showed a right renal AML with an arterial aneurysm and perirenal fat hematoma. Despite initial hemodynamic stability, a drop in hemoglobin levels necessitated urgent intervention. Interventional radiology performed endovascular embolization with microparticles and coils, resulting in successful devascularization. This case report discusses the clinical presentation, diagnostic workup, treatment strategy, and successful outcome of this complex case.
Keywords: Angiomyolipoma, kidney, embolization.
Introduction
Renal angiomyolipoma (AML) is a benign tumor composed of varying proportions of adipose tissue, blood vessels, and smooth muscle cells. Recognized as one of the most common solid benign renal tumors and the most common mesenchymal renal tumor, angiomyolipoma often presents asymptomatically¹. The primary clinical concerns include the risk of hemorrhage associated with the mass’ vascular component as well as ruling out renal cell carcinoma in select cases².
Recent studies indicate that renal angiomyolipoma are more prevalent than previously noted. A study in 1998 noted the prevalence to be 13 per 10,000 adults, while a study published in 2014 found the prevalence among a larger patient pool to be 0.44%²,³. Moreover, there seems to be convincing evidence to suggest a predilection in female patients over males. The majority of cases appear to be unilateral and single masses. The mean age of diagnosis is well above puberty except for cases associated with Tuberous Sclerosis Complex and other syndromes⁴.
Most angiomyolipoma are asymptomatic and detected incidentally; however, complications such as bleeding and rupture can pose significant clinical challenges³⁻⁵. Hence, attempts to characterize and classify them to delineate treatment regimens have been undertaken. Attributes such as size and clinical presentation have been used to stratify renal angiomyolipoma for treatment selection⁵. Moreover, it has also been classified as Tuberous Sclerosis Complex-associated type and a sporadic type. Efforts to histologically and radiologically categorize angiomyolipoma as classic, fat-poor, or epithelioid have also assisted in predicting the natural history of the mass and guiding management.
Due to the fat content, renal AMLs can usually be detected easily on CT imaging⁶. However, the fat-poor variant presents a diagnostic challenge, necessitating the consideration of a differential diagnosis, including renal cell carcinoma⁷.
The case discussed herein involves a 41-year-old male diagnosed with a combination of an AML with an arterial aneurysm and perirenal fat hematoma. The co-existence of this combination is an uncommon and intricate scenario that requires a multifaceted treatment approach. This highlights the importance of offering a tailored management plan based on the individual characteristics of each AML, while being aware of the potential complications that can arise.
Case Presentation
A 41-year-old male with an unremarkable medical and surgical history presented with acute left flank pain accompanied by a positive Murphy sign. Ultrasonography of the abdomen revealed a heterogeneous lower hyperechoic mass within the right kidney. Subsequent CT imaging demonstrated a lower right renal angiomyolipoma, alongside an associated upper interlobar artery aneurysm feeding the angiomyolipoma and perirenal fat hematoma⁶,⁷. During admission, the patient’s hemoglobin level was 14 g/dl, and he remained hemodynamically stable. As a result, a conservative management approach was initially pursued.
Diagnostic Workup
The diagnostic approach included a combination of imaging modalities. Ultrasonography provided preliminary insights into the renal mass, while CT imaging enabled detailed visualization of the angiomyolipoma, arterial aneurysm, and perirenal fat hematoma. The integration of these diagnostic tools facilitated accurate assessment and risk stratification of the complex clinical presentation.(Figures 1 & 2)

Figure 1A

Figure 1B
FIGURE 1: Abdominal CT scan;
Non contrast CT scan showing an Angiomyolipoma at the lower pole of the left kidney with retroperitoneal hematoma (Figure 1A). Contrast CT scan (Figure 1B).
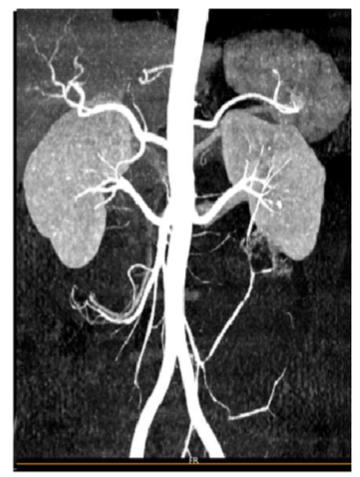
Figure 2A
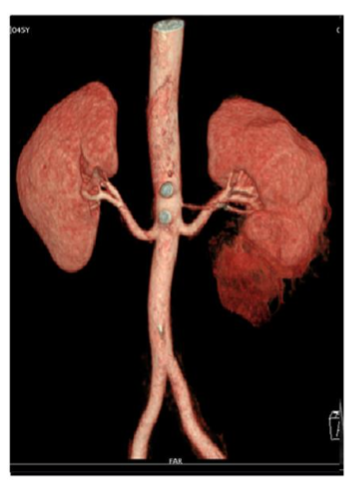
Figure 2B
FIGURE 2: CT Angiography
Angiomyolipoma at the lower pole of the left kidney (Figures 2A, 2B)
Conservative Management and Subsequent Intervention
Given the patient’s hemodynamic stability, conservative management was initially selected. Close monitoring and bed rest were implemented to mitigate the risk of bleeding or further complications. However, a follow-up hemoglobin assessment revealed a drop to 11 g/dl, prompting concern for ongoing hemorrhage. Urgent intervention by interventional radiology was deemed necessary.
Endovascular Approach and Embolization
To address the complex pathology, an endovascular approach was chosen. The procedure involved embolization with microparticles (300-500µm) to occlude distal intratumoral vessels, coupled with the placement of coils to target the feeding arteries. This combined approach aimed to achieve effective devascularization of the angiomyolipoma, prevent ongoing hemorrhage, and mitigate the risk of rupture⁸⁻¹¹. (Figure 3)
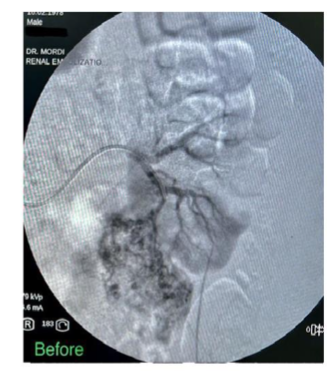
Figure 3A
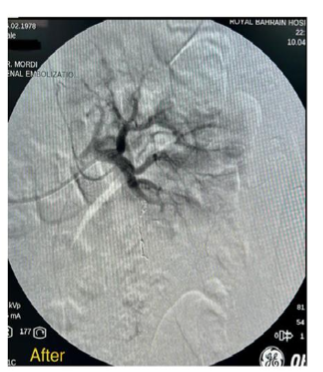
Figure 3B
FIGURE 3: Trans-catheter superselective angiogram
Figure 3A shows classic pathological arteries within the lower polar angiomyolipoma with free active extravasation. Figure 3B shows trans-catheter superselective coil embolization of the feeding arterial branch shows cessation of bleeding from the ruptured angiomyolipoma of the lower pole
Successful Outcome and Follow-up
The endovascular procedure was executed without complications. Post-procedural care encompassed vigilant monitoring for any signs of bleeding, infection, or renal dysfunction. A follow-up CT scan performed after one month demonstrated satisfactory devascularization of the angiomyolipoma. The patient’s clinical symptoms significantly improved, and no evidence of active bleeding or rupture was evident on imaging²,⁸,¹²,¹³. (Figure 4)

Figure 4A
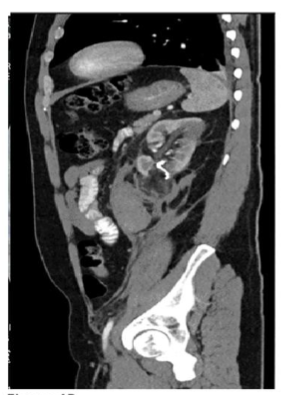
Figure 4B
FIGURE 4: Abdominal CT scan
Post super selective arterial embolization of angiomyolipoma (hematoma reduced)
Discussion
Being a benign renal tumor of varying components, angiomyolipoma treatment should be tailored. The concurrent presence of an angiomyolipoma, arterial aneurysm, and perirenal fat hematoma is a rare clinical entity that demands a multidisciplinary approach involving urologists, nephrologists, and interventional radiologists. The successful outcome achieved in this case underscores the significance of timely intervention and the feasibility of an endovascular approach using embolization materials.
In the case presented, the patient with a diagnosis of angiomyolipoma with associated arterial aneurysm and perirenal fat hematoma posed both diagnostic and therapeutic challenges that were catered to by a multidisciplinary team of clinicians. The importance of early recognition and diagnosis is highlighted by Omran et al., whereby a patient presenting with an angiomyolipoma with an intratumoral aneurysm was diagnosed after rupture, necessitating surgical intervention¹⁴. Factors pertaining to the risk of rupture were undertaken in several studies that showed that tumor size (greater than 4 cm) and aneurysm size (greater than 5 mm) were leading predictors¹⁵,¹⁶.
Other diagnostic challenges arise when the tumor presents with a reduced fat component, such as in epithelioid angiomyolipoma. A differential diagnosis including renal cell carcinoma should thus be carefully considered. Although usually associated with Tuberous Sclerosis, angiomyolipoma not uncommonly presents with an associated aneurysm. However, the presence of an additional perirenal fat hematoma was striking in the patient. Significant perinephric bleeding was first described by Wunderlich in 1856 using the classic triad: hypovolemic shock, abdominal pain, and a palpable mass. The patient mentioned herein did not develop Wunderlich syndrome but was carefully diagnosed with a series of imaging that delineated the case as well as the extent of involvement¹⁷,¹⁸.
Conclusion
This case report highlights the diagnostic and therapeutic challenges associated with a rare clinical scenario involving a renal angiomyolipoma, arterial aneurysm, and perirenal fat hematoma. Through the application of an endovascular approach encompassing embolization with microparticles and coils, successful management was achieved, and complications were averted. This article underscores the importance of tailored treatment strategies and collaborative efforts among medical specialties to effectively address intricate renal cases.
Disclosures
CONFLICT OF INTEREST:
The authors declare no conflict of interest. The case presentation was approved by the Royal Bahrain Hospital Reviewer Board.
HUMAN SUBJECTS:
Informed consent was obtained from the patient.
CONFLICTS OF INTEREST:
All authors declare the following:
• Payment/Services: All authors declared that no financial support was received from any entity for the above work.
• Financial Relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work.
○ Other Relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
References
1. Bissler JJ, Kingswood JC. Renal angiomyolipomata. Kidney Int. 2004; 66:924–934.
2. Dabbeche C, Chaker M, Chemali R. Role of embolization in renal angiomyolipomas. J Radiol. 2006; 87:1859–1867.
3. Eble JN. Angiomyolipoma of kidney. Semin Diagn Pathol. 1998;15(1):21-40. PMID: 9503504.
4. Fittschen A, Wendlik I, Oeztuerk S, et al. Prevalence of sporadic renal angiomyolipoma: a retrospective analysis of 61,389 in- and out-patients. Abdom Imaging. 2014; 39:1009–1013. doi:10.1007/s0026 1-014-0129-6.
5. Dickinson M, Ruckle H, Beaghler M, Hadley HR. Renal angiomyolipoma: optimal treatment based on size and symptoms. Clin Nephrol. 1998;49(5): 281-286. PMID: 9617489.
6. Hatano T, Egawa S. Renal angiomyolipoma with tuberous sclerosis complex: How it differs from sporadic angiomyolipoma in both management and care. Asian J Surg. 2020;43(10):967-972. doi: 10.1016/j.asjsur.2019.12.008. PMID: 31959574.
7. Kurosaki Y, Tanaka Y, Kuramoto K. Improved C.T. fat detection in small kidney angiomyolipomas using thin sections and single voxel measurements. J Comput Assist Tomogr. 1993; 17:745–748.
8. Lemaitre L, Claudon M, Dubrulle F. Imaging of angiomyolipomas. Seminars in ultrasound, C.T. and M.R.I.
9. Khaitan A, Hemal AK, Seth A. Management of renal angiomyoplipoma in complex clinical situations. Urol Int. 2001; 67:28–33.
10. Radeleff BA, Heye T, Lopez-Benitez R. Interventional management of acute bleeding giant renal angiomyolipoma: Report of three cases and review of the literature. Euro J Radiol Extra. 2007; 61:119–128.
11. Sung CK, Hwang SS, Park BK. Management of renal angiomyolipoma: current status and future direction. J Korean Med Sci. 2012;27(9):1105-1115.
12. Teichgraber KMU, Bucourt DM. Massive retroperitoneal hemorrhage from a giant renal angiomyolipoma treated by selective arterial embolization with an Amplatzer Vascular Plug II. Acta Radiol Short Rep. 2012; 1:8.
13. Rosenov A, Schindewolf M, Baumgartner I. Selective arterial embolizations of renal angiomyolipomas using 96% ethanol: a case series of 5 patients. Clinical Medicine Insights: Case Reports. 2020; 13:1–7.
14. Wang C, Yang M, Tong X. Transarterial embolization for renal angiomyolipomas: a single center experience in 79 patients. J Int Med Res. 2017; 45:706–713.
15. Patil AR, Chandra R, Gupta A, Thukral BB. Giant aneurysm formation in sporadic renal angiomyolipoma. J Radiol Case Rep 2010;4(6):21-27. 10.3941/jrcr.v4i6.439
16. Al Omran B, Ansari N. Aneurysm in a large sporadic renal angiomyolipoma. Oman Med J. 2016;31(3):223-226. doi:10.5001/omj.2016.42. PMID: 27162594; PMCID: PMC4852083.
17. Yamakado K, Tanaka N, Nakagawa T, et al. Renal angiomyolipoma: relationships between tumor size, aneurysm formation, and rupture. Radiology. 2002;225(1):78-82. doi:10.1148/radiol. 2251011477. PMID: 12354988.
18. Parameswaran B, Khalid M, Malik N. Wunderlich syndrome following rupture of a renal angiomyolipoma. Ann Saudi Med. 2006;26(4):310-312. doi:10.5144/0256-4947.2006.310. PMID: 168 85633; PMCID: PMC6074510
Most read articles by the same author(s)
- Issa Afif Kawalit, Abdulraqeeb Hasan Al-Omari, Zeina H. Kalaji, Asad Ibrahim Al-Tirawi, Muhand Salama Eltwal, Abbas Y. El-Khatib, Renal outcomes with sodium-glucose cotransporters 2 inhibitors in Patients with Type 2 Diabetes Mellitus with Chronic Kidney Disease Stages 3b-4. , Medical Research Archives: Vol 12 No 11 (2024): November Issue, Issue 11, VOl.12